
Abstract
Background
Hepatic cystic echinococcosis (CE) is a major health concern, particularly in endemic regions. The modified catheterization technique (MoCaT) offers an effective option for the percutaneous treatment of hepatic CE.
Purpose
To evaluate the effectiveness of MoCaT in the percutaneous treatment of all types of hepatic CE in 183 patients.
Material and Methods
Data from 183 patients who underwent percutaneous treatment using the MoCaT between February 2010 and April 2024 were retrospectively analyzed. Demographic data, cyst types, initial and final cyst volumes, complications, lengths of hospitalization, catheterization, and follow-up periods were documented for each patient.
Results
This study included 183 patients with 211 hepatic hydatid cysts who were treated percutaneously with MoCaT. Among the 211 cysts, 20 (9.5%) were CE1, 37 (18%) were CE2, 23 (11%) were CE3a, 98 (46%) were CE3b, 16 (7.6%) were CE4, and 2 (0.9%) were CE5. In total, 15 (7%) patients presented with infected cyst cavities. No mortality was seen. A total of 29 (14%) major complications were observed. Recurrence was observed in 6 (3.85%) patients, and residual daughter vesicles remained in 1 (0.64%) patient. The mean follow-up period was 48.35 ± 36.42 months (range = 3–133 months). Mean volume reduction was 92.69%.
Conclusion
The MoCaT is an effective, minimally invasive method with low morbidity and recurrence rates. In addition to its reported success in treating CE2 and CE3b cysts, we report that the MoCaT is also safe, reliable, and effective for the treatment of all types of hepatic CE.
Introduction
Cystic echinococcosis (CE) is a helminthic infectious disease caused by the larvae of the Echinococcus granulosus tapeworm. Despite a low mortality rate, the morbidity associated with hydatid disease is significant, making it a major public health problem in endemic areas, primarily affecting the liver (50%–77%) (1–6). The percutaneous approach to treatment of the hepatic CE has become a promising method to avoid complications associated with surgery and prolonged hospitalization (7–9). The modified catheterization technique (MoCaT), aimed at the complete evacuation of cyst contents through a catheter, was first introduced by Akhan et al. (10). Its use in treating CE2 and CE3b cysts (Table 1) has expanded over the last two decades with reported successful outcomes (10–13). The aim of the present study was to evaluate the effectiveness of MoCaT in the percutaneous treatment of all types of hepatic CE by presenting the outcomes of 183 patients with 211 cysts.
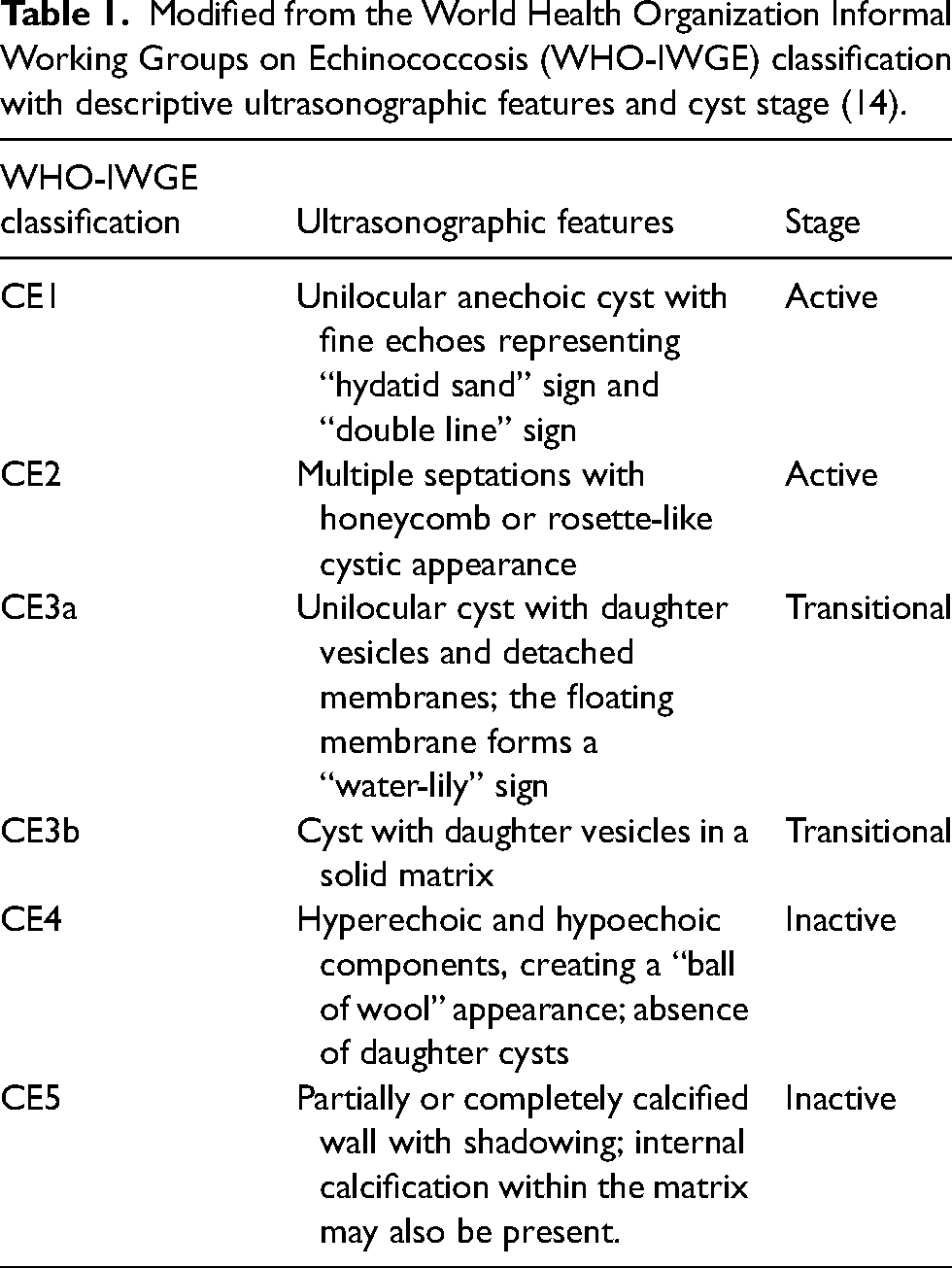
Modified from the World Health Organization Informal Working Groups on Echinococcosis (WHO-IWGE) classification with descriptive ultrasonographic features and cyst stage (14).
Material and Methods
Patients
Between February 2010 and April 2024, a total of 407 patients with hepatic hydatid cysts were treated percutaneously in our department. Of them, all patients treated percutaneously with MoCaT were included in the study, totaling 183 patients (211 cysts). Inclusion criteria consisted of CE1 and CE3a cysts >6 cm, CE2 and CE3b cysts, CE4 and CE5 cysts presenting with cholestasis or pain due to mass effect on adjacent biliary or vascular structures, infected cysts, and all types of cysts with cystobiliary fistulas (CBF). Exclusion criteria included asymptomatic patients with incidentally detected CE4–CE5 cysts, and patients with CE1 and CE3a cysts treated with (Puncture, Aspiration, Injection, Reaspiration (PAIR) or modified PAIR (PAID; Puncture, Aspiration, Injection, Drainage) (n = 224). Table 1 presents the CE classification based on the WHO-IWGE (14).
Unfortunately, we do not have access to the exact number of patients who underwent surgical treatment, as these cases were managed in other departments with separate records. However, in recent years, percutaneous treatment has largely replaced surgery for hepatic CE in our institution, and most patients are now referred to our interventional radiology unit by the surgeons.
The demographic information, cyst types, initial and final cyst volumes, complications, lengths of hospitalization, and catheterization periods were documented for each patient. Information on all available treatment methods, along with their advantages, disadvantages, and potential outcomes, was given, and informed consent was obtained from the patients or their legal guardians. This study received approval from our institutional research ethics committee (reference no. 191/2024).
Patient preparation
Patients with viable cysts were given albendazole (Andazol; Biofarma, Turkey) at a dose of 10 mg/kg/day, starting 1 week before the procedure and continuing for 4 weeks afterward, as prophylaxis to reduce the risk of abdominal dissemination (15). Liver function tests (LFTs) were evaluated during this period.
Coagulation parameters and a complete blood count were assessed. Patients with viable cysts received premedication containing a steroid and an antihistamine for anaphylaxis prophylaxis, along with a prophylactic antibiotic.
Technique
The procedures were performed with intravenous sedation. A laryngeal mask airway (LMA) was used in procedures anticipated to be prolonged. All patients were monitored for potential anaphylaxis.
To reduce the risk of cyst content leakage that could cause peritoneal dissemination, the puncture site was selected using ultrasound (US) to ensure that the tract would, if possible, pass through the liver parenchyma. Local anesthesia was administered. After a puncture with an 18-G Chiba needle (Egemen International, Izmir, Turkey), under US guidance, a cavitography was obtained using non-ionic contrast media (Opaxol, Opakim, Turkey). A 0.035-inch Amplatz extra stiff wire guide (Cook Medical, Bloomington, IN, USA) was advanced into the cyst cavity, and then a peel-away sheath introducer (MAHURKAR; COVIDIEN, Mansfield, MA, USA) was used to insert a 14-F drainage catheter (SKATER; Argon Medical Devices, Athens, TX, USA). Catheter holes were manually enlarged to prevent early blockage caused by cyst contents. The cyst contents, including daughter cysts, germinative membranes, and solid matrix, were evacuated through the effective irrigation technique with saline under fluoroscopy. Irrigation was initiated with isotonic saline, and in the presence of viable cysts, hypertonic saline was used as a scolicidal agent after confirming the absence of CBF. Once the contents were fully evacuated, the 14-F catheter was exchanged over the guidewire with a 12-F drainage catheter. To minimize the risk of hemorrhage, the puncture site was chosen at a safe distance from vascular structures, and aggressive aspirations and catheter manipulations were avoided as the cavity decreased in size during the final part of the procedure.
In the presence of a CBF, when germinative membranes were observed in the bile ducts, percutaneous transhepatic removal of the germinative membranes was achieved by aspiration via a 12-F drainage catheter or by pushing into the duodenum via Fogarty balloon catheter. Then a 8/10-F external biliary drainage catheter was inserted. The catheter removal time was determined based on follow-up imaging. If germinative membranes were not observed in the bile ducts, closure of the fistula was aimed through catheterization of the cyst cavity.
In the treatment of CE1 cysts, standard protocol required modifications due to challenges in evacuation compared to other cyst types. To facilitate evacuation, either hypertonic saline was administered at the beginning of the procedure with an additional 10–15 min wait for inactivation after confirming the absence of CBF, or MoCaT was performed 3–4 days after an initial modified PAIR procedure.
Patients were called in on the second day after the procedure, and a saline solution was administered into the cavity via the catheter and then aspirated. This process was repeated several times to evacuate any potential small remnants of cyst contents and continued every 2 days until the aspirated fluid was clear of solid particles. The catheter was left in the cavity until the daily drainage decreased to below 10 mL. In cases with exophytic cysts and no bile content in the drainage fluid, ethanol (95%) was administered as a sclerosing agent under fluoroscopic guidance to rule out CBF, before catheter removal.
Follow-up
Monitoring continued for 3–6 h after the procedure, and the patients were hospitalized. Routine follow-up was conducted every 3 months during the first year, twice in the second year, and once in the subsequent years. Ultrasound was used to evaluate changes in cyst morphology and volume at each follow-up. The absence of the cyst cavity or the presence of a shrunken, anechoic cavity without content was considered a sign of complete recovery (Figs. 1 and 2). The absence of changes in cyst morphology or an increase in size was considered a sign of treatment failure. Recurrence was defined as the reappearance of an active cyst containing daughter vesicle(s). Out of 183 patients, 140 maintained their follow-ups, and the final volumes of the cysts and lengths of the follow-up period were documented.
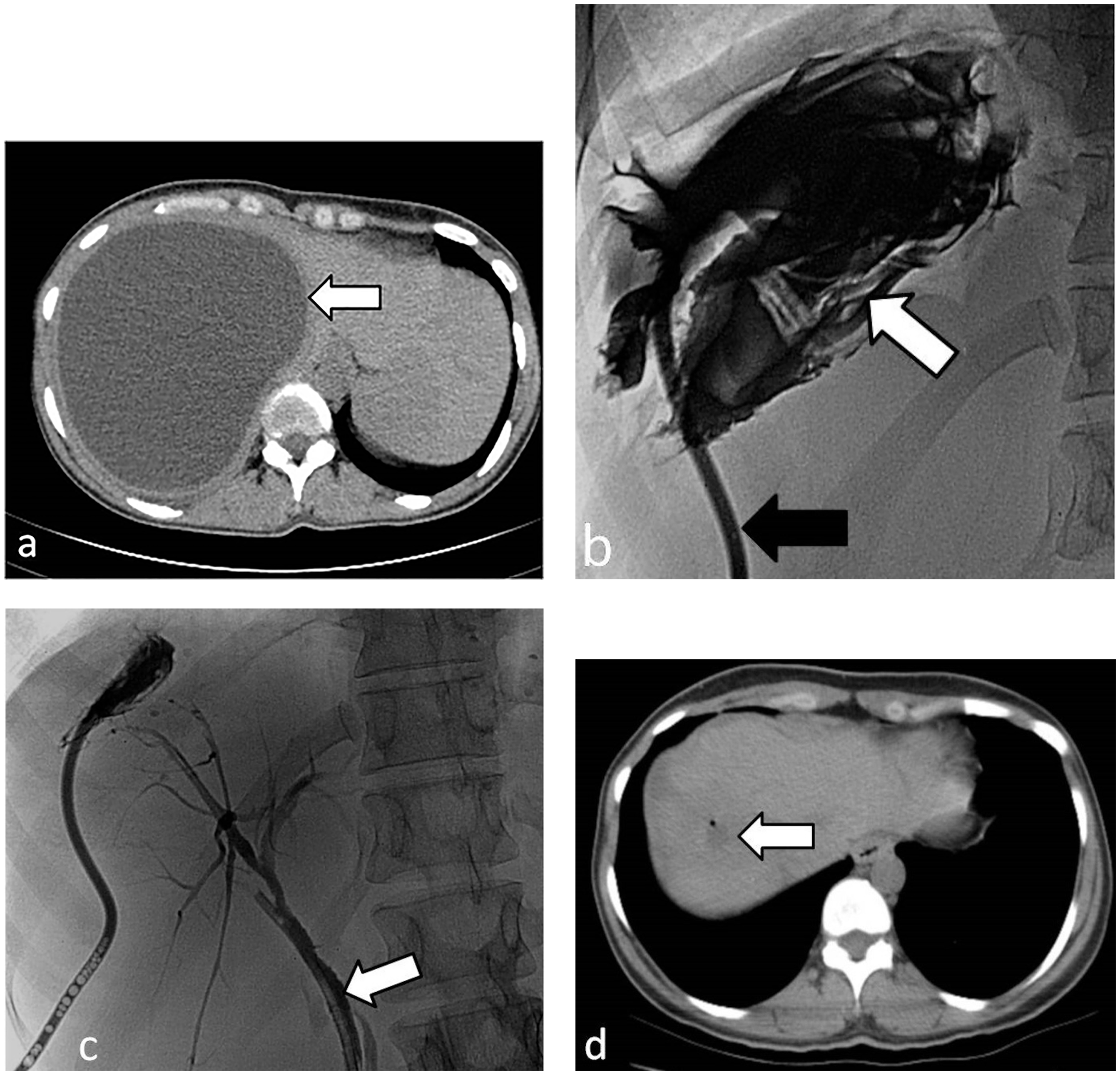
A 37-year-old woman presented with right upper quadrant pain and a palpable mass. (a) An axial CT image demonstrates a CE1 cyst (arrow), measuring 16 × 14.3 × 13 cm (volume 1547 mL) in the right lobe of the liver, (b) The fluoroscopic image shows part of the evacuation of germinative membranes (white arrow) via a 14 F catheter (black arrow), (c) The figure shows a shrunken cyst cavity after the evacuation of germinative membranes and cysto-biliary fistula; note the endoscopic plastic stent that was inserted to biliary diversion (arrow), The catheterization period was 7 days. A CT image obtained 9 months after the MoCaT procedure shows a shrunken residual cyst cavity measuring 1 cm in diameter without cyst content (arrow). The patient remained asymptomatic during the follow-up period. CT, computed tomography; MoCaT, modified catheterization technique.
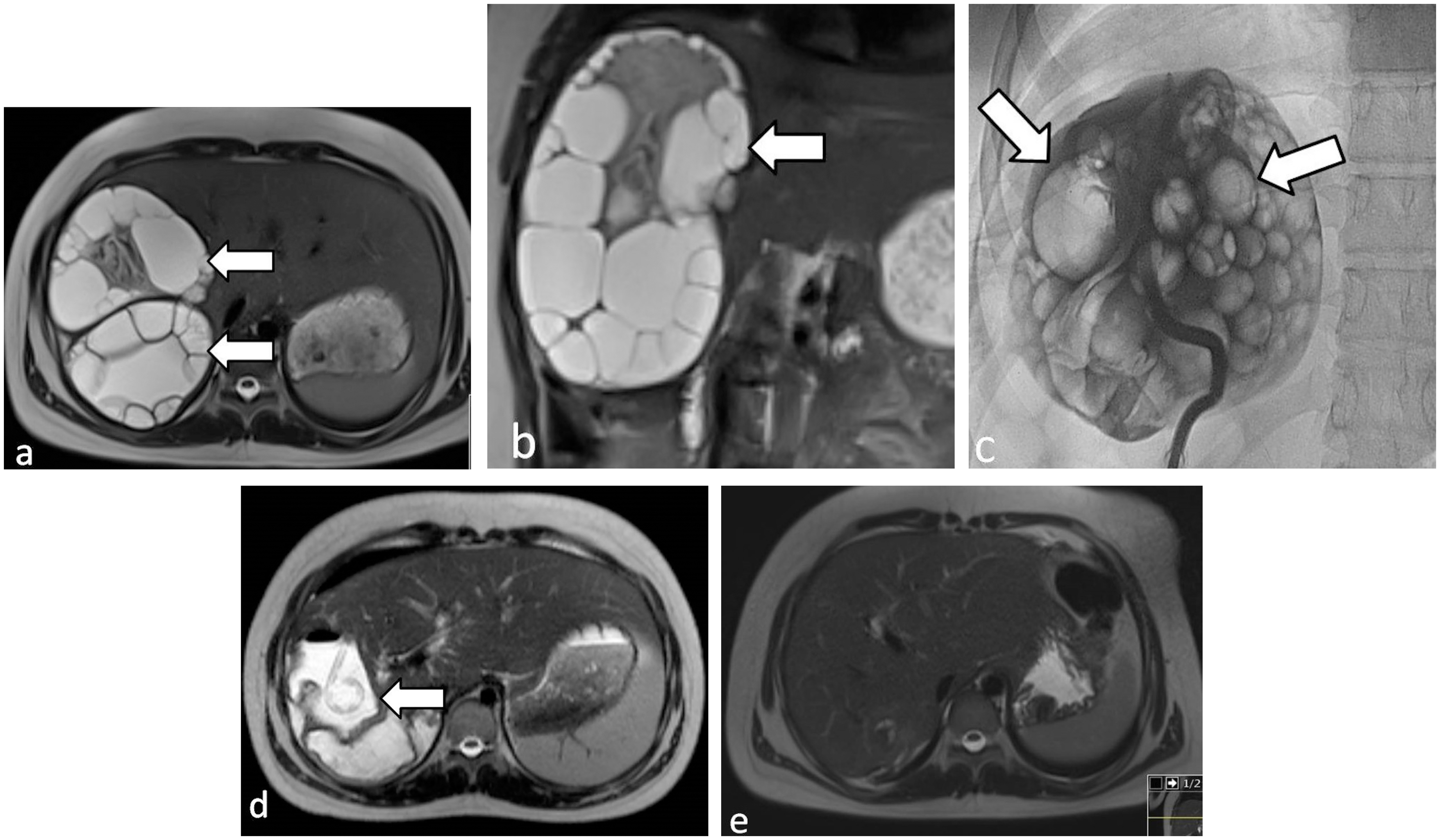
A 16 year-old girl presented with right upper quadrant pain. (a, b) Axial and coronal T2-weighted MR images demonstrate CE3b liver hydatid cysts (arrows), invading the whole right lobe of the liver, (c) The fluoroscopic image obtained during the procedure clearly demonstrates the daughter cysts (arrows), Axial T2-weighted MR image obtained 1 day later, shows a shrunken cyst cavity without daughter cysts. The catheterization period was 38 days for anteriorly located cyst and 24 days for the other one. Axial T2-weighted MR image obtained 15 months after the procedure clearly demonstrated complete resolution of the cyst cavity. The patient remained asymptomatic during the follow-up period. MR, magnetic resonance.
Adjacent structures and other organs were also evaluated during follow-ups. A renal CE3b cyst in one patient was treated with the MoCaT, while another patient with a hydatid cyst in the left lower quadrant was treated using the PAIR procedure. Inactive splenic hydatid cysts were detected in two patients. Four patients had a history of surgery for pulmonary hydatid cysts.
Definitions and statistics
Technical success was defined as the completion of all stages of the procedure. Clinical success was defined as the complete evacuation of the cyst cavity and the absence of recurrence during the follow-up period.
Statistical analysis was conducted using SPSS software version 26.0 (IBM Corp., Armonk, NY, USA). The Kolmogorov–Smirnov test was used to assess the normality of continuous variables. Quantitative data were expressed as mean ± standard deviation (SD), and categorical variables were presented as frequencies and percentages. Qualitative parameters between groups were compared using the chi-square and Fisher's exact tests, and P values <0.05 were considered statistically significant.
Results
A total of 183 patients (81 male patients, 102 female patients; age range = 6–83 years; mean age = 38.76 ± 19.25 years) with 211 hepatic CEs, who were treated percutaneously using the MoCaT, were included in the study. In total, 12 patients had a history of surgery and 17 had previously undergone a PAIR procedure. Abdominal pain was the most common presenting symptom. Symptoms of infection, cholangitis, cholestasis, and allergic rashes were observed. Out of 183 patients, 158 had a single cyst, while 25 had multiple cysts. Of the 211 cysts, 20 (9.5%) were CE1, 37 (18%) were CE2, 23 (11%) were CE3a, 98 (46%) were CE3b, 16 (7.6%) were CE4, and 2 (0.9%) were CE5. In total, 15 (7%) patients presented with infected cyst cavities. The mean initial volume of the cysts was 409.4 ± 384.5 mL (range = 16–1998 mL). The mean catheterization duration was 13.21 ± 9.74 days (range = 2–65 days). The mean hospitalization duration was 5.72 ± 4.29 days (range = 1–25 days). No mortality was observed. The mean follow-up period was 48.35 ± 36.42 months (range = 3–133 months), and the mean volume reduction was 92.69%.
Hypertonic saline (30% NaCl) was used for irrigation and as a scolicidal agent for patients with viable cysts, as its effectiveness has been reported in the literature (13,16–20). A 14-F drainage catheter was generally sufficient for evacuating the cyst contents. In cases of difficulty, the catheter was switched to a 16-F. The technical success rate was 100%. The clinical success rate was 96.2% after the first procedures, with six recurrences and one patient with residual daughter vesicles. Five of the six recurrences were managed with a second MoCaT procedure, while one patient underwent surgery. The clinical success rate after the second procedures was 98.9%.
Cystobiliary fistula was detected in 32/211 (15.17%) cysts. Of these, 30 were identified on preoperative imaging or during cavitography within the initial procedure, and two were detected during follow-up cavitographies. Germinative membranes were observed in the bile ducts during cavitography in 13 of these patients and percutaneous transhepatic removal of the germinative membranes was performed (Fig. 3). In 19 patients, germinative membranes were not detected in the bile ducts, and closure of the fistula was attempted through catheterization of the cyst cavity. In 10 patients, follow-up cavitographies confirmed spontaneous closure of the fistula with catheterization, while in nine patients, endoscopic papillotomy was performed by gastroenterologists due to persistent bile-containing drainage that did not decrease as expected after the procedure. The mean time to endoscopic papillotomy after initial catheterization was 19.11 ± 13.6 days (range = 7–54 days). The cases detected during follow-up cavitographies may have been procedure-related and were classified as procedure-related complications. The catheterization period and hospitalization duration were significantly longer in patients with cysts presented with CBF and infected cyst cavities as expected (16.93 ± 13.41 and 11.33 ± 6.43 days for those presenting with CBF, 16.46 ± 10.65 and 8.91 ± 5.59 days for infected cysts).
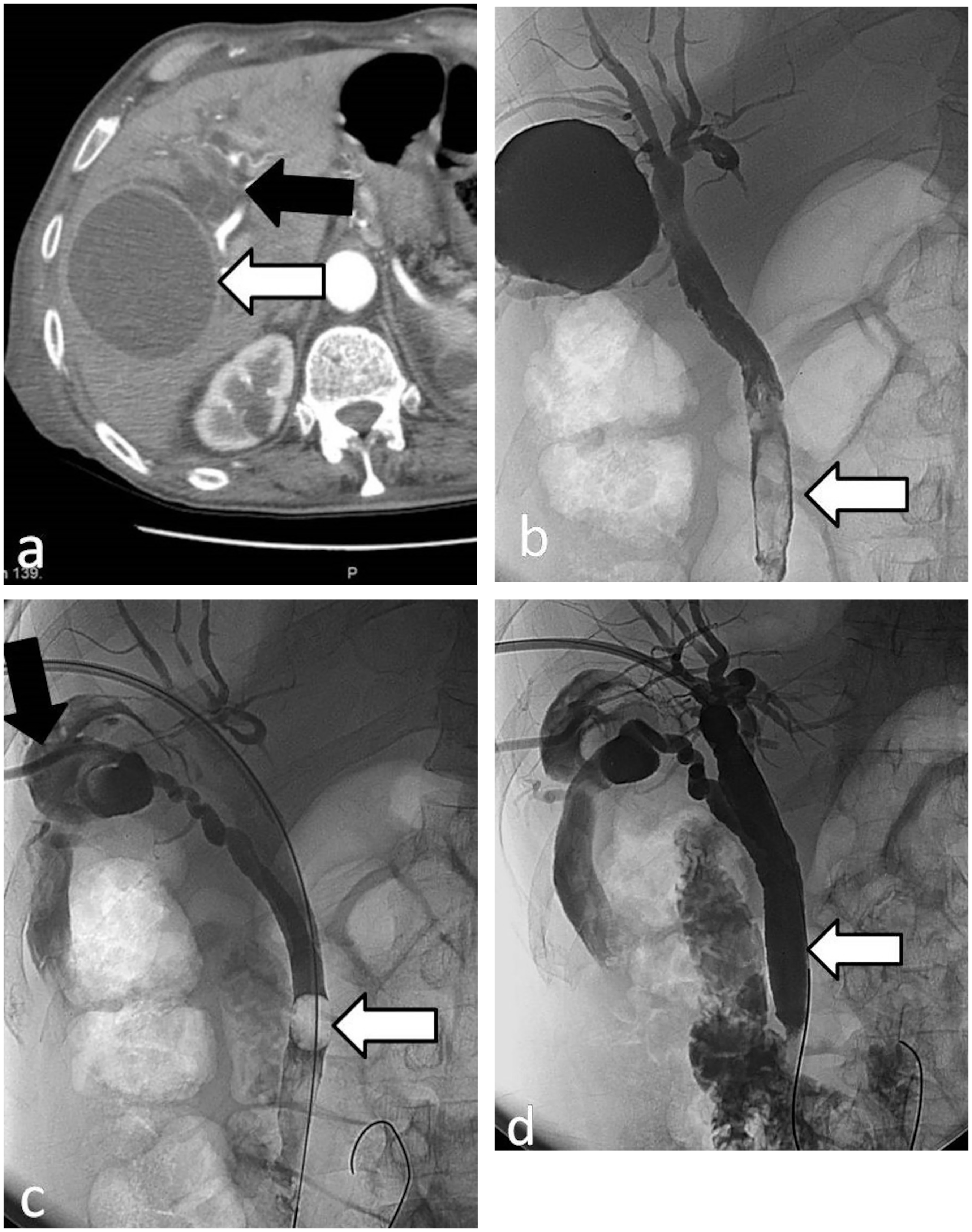
A 75-year-old male patient presented with jaundice and upper abdominal pain. (a) Blood tests indicated elevated bilirubin levels. Axial contrast-enhanced computed tomography (CT) image shows a CE IV hydatid cyst (8 × 7 × 8 cm) in the right lobe of the liver (white arrow) and bile duct dilatation (black arrow), (b) A fluoroscopic image obtained during cavitography shows cystobiliary fistula and germinative membranes in the common bile duct causing obstruction (arrow), (c) Cyst contents were removed via 14-F catheter (black arrow), and percutaneous transhepatic removal of germinative membranes was achieved by pushing them into the duodenum using a Fogarty balloon catheter (white arrow), (d) Final fluoroscopic image demonstrates the complete clearance of common bile duct (arrow) and cyst cavity, The drainage catheter was kept in place for 2 days in the common bile duct. Bilirubin levels quickly returned to the normal range after the procedure and the patient remained asymptomatic during the 12-month follow-up period.
Table 2, and outcomes, categorized by cyst type. After the procedure, an abscess developed in the cyst cavity of 12/211 (5.7%) cysts, which resulted in an extended catheterization period for two patients. A total of 10 patients who developed abscesses after the catheterization period were treated with percutaneous drainage. All received appropriate antibiotic therapy. Mean time to development of abscess formation was 3.1 weeks.
Clinical characteristics, major and minor complications based on the Society of Interventional Radiology's classification system (21), and outcomes, categorized by cyst type.
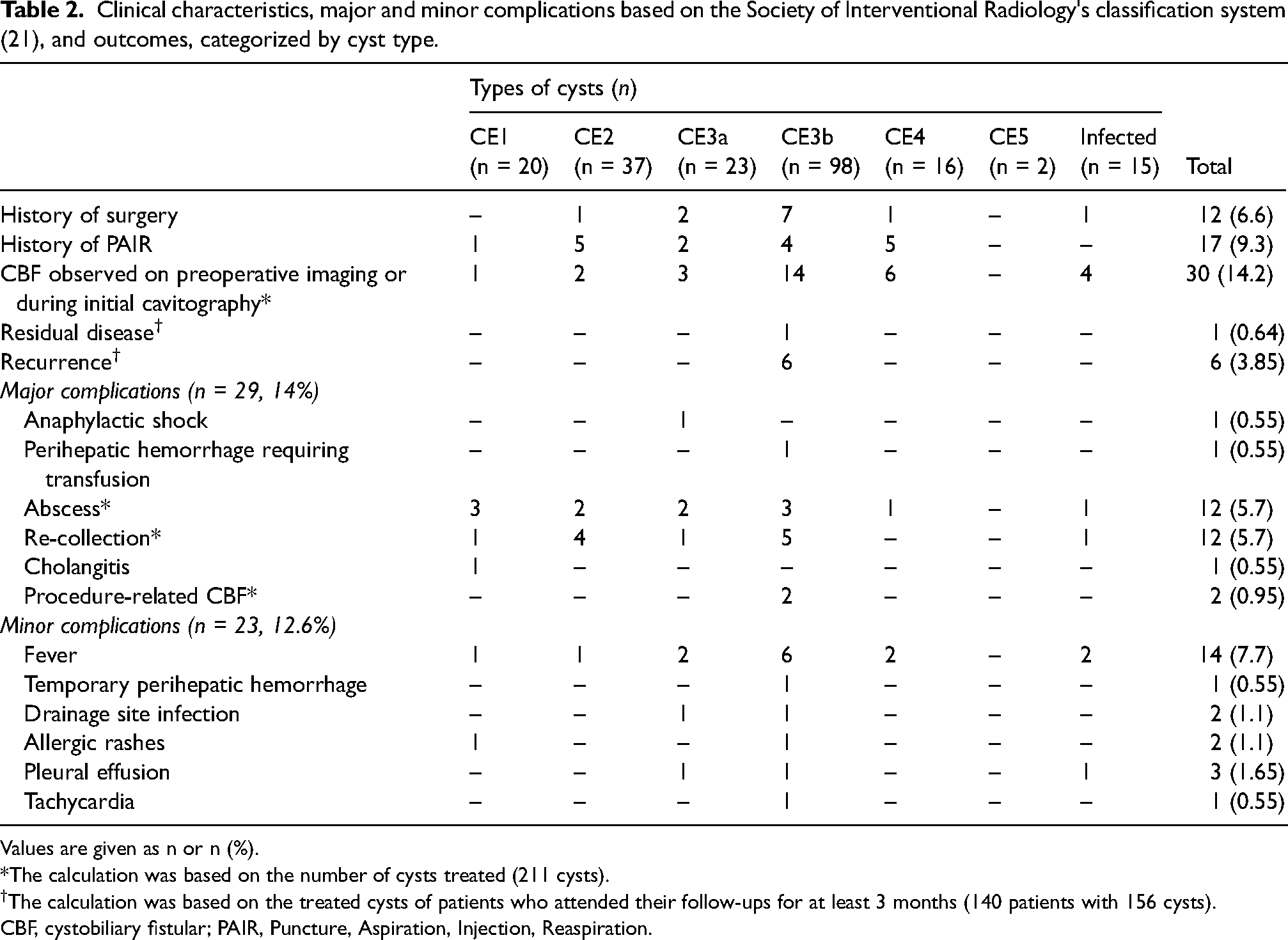
Values are given as n or n (%).
*The calculation was based on the number of cysts treated (211 cysts).
The calculation was based on the treated cysts of patients who attended their follow-ups for at least 3 months (140 patients with 156 cysts).
CBF, cystobiliary fistular; PAIR, Puncture, Aspiration, Injection, Reaspiration.
Re-collection was defined as an enlargement of the cyst cavity due to fluid accumulation, with no signs of viability. It was detected in 12/211 (5.7%) cysts in our study and was managed by catheterization. The mean time to re-collection was 7.4 months.
Allergic reactions were managed with steroids or antihistamines. In the patient who developed anaphylaxis, tracheal intubation was performed, and medical therapy was administered. The procedure was completed after stabilization. In one patient, hypotension occurred due to perihepatic hemorrhage, requiring admission to the intensive care unit and a blood transfusion. The patient with symptoms of cholangitis was managed with endoscopic papillotomy and medical treatment. Intravenous antibiotic treatment was required for three patients who developed a fever, resulting in prolonged hospitalization.
Complications and recurrences were analyzed by classifying patients into five groups according to CE stages: (i) CE1 and CE3a, (ii) CE2 and CE3b, (iii) CE4 and CE5, (iv) infected cysts, and (v) CE cysts with CBF diagnosed before the procedure. No statistically significant difference was found among the groups (P >0.05).
Recurrence
A total of 140 patients with 156 treated cysts continued their follow-ups for at least 3 months. Recurrence was observed in 6 (3.85%) patients, as reappearance of daughter vesicle(s) in the cyst cavity. In 1 (0.64%) patient with a large cyst, residual daughter vesicles remained in the posterior wall of the cyst cavity despite repeated evacuation attempts. It has persisted similarly throughout the 34-month follow-up period and routine follow-up continues.
Discussion
Treatment is recommended for patients with viable cysts due to the risk of potential complications that can lead to mortality and morbidity (e.g. anaphylactic reaction, intrabiliary rupture, and rupture into the peritoneal or pleural cavity) (2,15–17,22).
There is no consensus on the best treatment approach (8,9,15,23–26). However, as presented in our study, treatment may be required for inactive cysts due to mass effect or when CBF is present.
The effectiveness of the MoCaT procedure in treating CE2 and CE3b cysts is well documented in the literature (10,11,13,27). All decisions were made after discussing alternative treatment options with the patients.
Ethanol has been reported as a safe and effective sclerosing agent in studies (10,11,13,28), and its use is generally preferred when the absence of CBF is confirmed. In the early 2010s, ethanol was routinely used for sclerosis among patients included in this study; however, considering that a significant portion of cysts might present with CBF (15% in this study), and given that the absence of contrast passage into the bile ducts on cavitography after the initial intervention does not entirely rule out a biliary connection, routine use was discontinued. Since then, ethanol has been selectively administered as a sclerosing agent in cases with an exophytic cyst location or absence of bile content in the drainage fluid, provided there was evidence of cyst viability and no detectable CBF. The use of ethanol might have helped reduce the rate of re-collection. Cavity size reduction and prevention of re-collection were targeted by extending the catheterization period. In cases where re-collection occurred, catheterization alone was sufficient for management.
The risk of hemorrhage was one of the major concerns during the MoCaT procedure. Adjacent vascular structures should be evaluated before the puncture. Catheter manipulations and aspirations should be performed more gently, as the cavity reduces during the final part of the procedure. To reduce the risk of hemorrhage and complications associated with the procedure, we used a peel-away sheath, which removes the need for tract dilatation and makes repeated catheter manipulations easier and safer. Manually enlarging the catheter holes helped prevent early blockage caused by cyst contents, indirectly reducing the need for aggressive aspirations; however, it also reduced catheter stability, making catheter insertion and exchange over the guidewire more challenging. The use of a peel-away sheath helped overcome this difficulty by allowing easier catheter placement and exchange.
Based on our experience, evacuating the cyst contents was easier in inactive cysts, while it was most challenging in active cysts, particularly in CE1 cysts, requiring technical modifications as detailed in the “Material and Methods” section. No additional difficulty was encountered during the evacuation of CE3a cysts compared to CE2 and CE3b cysts. Compared to PAIR, we believe that evacuating the cyst contents through the MoCaT procedure reduces the mass effect in large CE1 and CE3a cysts and may potentially decrease recurrence rates. In this study, no recurrence was observed in CE1 and CE3a cysts treated with MoCaT; head-to-head comparative studies are needed to draw more definitive conclusions.
We believe that extending the catheterization period and evaluating the cavity for any potential solid remnants on the second day after the procedure may reduce the risk of recurrence and re-collection. However, extending the catheterization period may increase the risk of infection, which makes standardization difficult. We suggest that this period may be extended until fluid drainage stops completely, depending on patient tolerance.
In this study, the major complication rate was 14% and the minor complication rate was 12.6%, based on the SIR guidelines (7,11,13,17–21,29–31).
In this study, 6 (3.85%) recurrences were observed and the recurrence rate was consistent with those reported in the literature (9–11,20,24). Recurrences are typically seen as a few daughter vesicles within the cavity, and relatively easy to treat with MoCaT.
The differences in the present study are the inclusion of all types of hydatid cysts, the use of a peel-away sheath, the selective use of ethanol for sclerosis, and our approach to evacuating germinative membranes or daughter vesicles present in the bile ducts in cases with CBF.
The present study has some limitations. These are the inability to compare it with other percutaneous methods and its retrospective design. Data on complications were collected from the archive, and minor complications may have been underreported. In addition, the lack of randomized controlled trials (RCTs) in hydatid disease remains a major limitation in the field. Future prospective studies with standardized outcome measures are essential to strengthen the evidence base and enable better comparison between treatment modalities.
In conclusion, our results confirm the reported success of MoCaT in treating CE2 and CE3b cysts in the literature. We also report that the MoCaT is safe, reliable, and effective for the treatment of large CE1 and CE3a cysts, as well as complicated hydatid cysts, including CE4 and CE5 cysts (e.g. those presenting with CBF or infection) and recurrent cysts after surgical or percutaneous procedures. Given the low recurrence rates and manageable complications, we suggest that the MoCaT could be the first-line treatment option for all types of hepatic CE in the mentioned indications.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.