
Abstract
Background
The widespread use of high-resolution ultrasonography (US) imaging has led to an increased detection of thyroid nodules, which are common in the general population.
Purpose
To evaluate the correlation between ultrasonographic and pathological findings of thyroid nodules undergoing US-guided fine-needle aspiration (FNA) and assess the contribution of US features to malignancy prediction.
Material and Methods
A total of 573 patients (137 men, 436 women; age range = 20–88 years) who underwent US-guided FNA were included. Nodule characteristics were recorded using the British Thyroid Association (BTA) U classification, and cytological results were assessed according to the Bethesda system. Logistic regression analysis (LRA) was performed to determine the relationship between US features and malignancy.
Results
The distribution of nodules in U2, U3, U4, and U5 categories was 212, 171, 84, and 36, respectively, with corresponding Bethesda (2–6) classifications of 287, 159, 18, 27, and 12. Malignancy rates (Bethesda 4–6) were 0%, 10%, 28.6%, and 44.5%, respectively. Hypoechogenicity (relative to muscle), internal vascularization, and microcalcifications were significantly associated with malignancy (P <0.05). LRA achieved an 85.5% accuracy in malignancy prediction.
Conclusion
US features in the BTA U classification align with pathological findings. Hypoechoic solid nodules, central vascularization, and microcalcifications should raise suspicion for malignancy in the differential diagnosis of thyroid nodules. These study findings highlight the strong association between vascularity in the BTA classification and malignancy, suggesting its potential role in risk stratification.
Introduction
Thyroid nodules, detected as a result of the increased use of high-resolution sensitive imaging in recent years, are quite common in the population (1–4). There has been a 15-fold increase in the incidence of thyroid cancer worldwide in proportion to the increase in its diagnosis (3). Since thyroid cancers are asymptomatic in the early stages, it is essential to identify nodules rapidly as benign or malignant. It is crucial that thyroid nodules are correctly diagnosed early and managed appropriately with optimal therapeutic approaches (5). Equally important is the need to avoid overdiagnosis and intervention of incidental thyroid (6).
Ultrasonography (US), computed tomography (CT), and magnetic resonance imaging (MRI), which are non-invasive methods for imaging thyroid nodules, are used as diagnostic tests (5). US is preferred as the primary diagnostic tool in clinical practice, especially in thyroid nodules, due to its ease of use, high accuracy, and low cost (2,5,7). Furthermore, a meta-analysis reported that US has a combined sensitivity of 88% (95% confidence interval [CI] = 83%–91%) and specificity of 86% (95% CI = 79%–90%) in the diagnosis of thyroid nodules (8).
Fine-needle aspiration (FNA), the standard procedure for pathologic diagnosis of thyroid nodules, is a cost-effective, sensitive, safe, minimally invasive procedure performed under US guidance (9,10). Several classification systems have been developed to minimize patient anxiety, healthcare burden, surgical resection, and unnecessary biopsies due to thyroid nodules and standardize diagnostic terminology for reporting thyroid cytopathology results (1,11). The Bethesda classification is the most generally accepted system for determining thyroid cytology (10). FNA analysis with Bethesda is used to decide whether to proceed with a US follow-up, perform a thyroidectomy, or repeat a biopsy (1,12,13).
The British Thyroid Association (BTA) published clinical guidelines for managing thyroid cancer in 2014. These clinical guidelines recommended using a grading system from U1 to U5 to assess the risk of malignancy and guide FNA cytology (3,11). Thus, a correlation has been established between the pathology results and the U grading system (3,14). The aim of the present study was to evaluate the performance of the BTA U classification, focusing on radiology-pathology correlation with current classifications of thyroid nodules undergoing FNA in our center, and determine the importance of ultrasonographic findings of nodules in diagnosing malignancy.
Material and Methods
This retrospective cross-sectional study included 503 patients (age range = 20–86 years) who underwent US-guided FNA of thyroid nodules between January 2018 and March 2020. Patient selection was performed consecutively. Patients were recruited from a tertiary care hospital. Approval for the study was obtained from the local ethics committee with decision number 2021/538 dated 07.04.2021.
Biopsies of all patients admitted to the radiology unit for FNA were performed by a radiologist with at least 10 years of experience in interventional procedures using a US System (Aplio 500; Canon Medical Systems, Netherlands) equipped with a 7.5 MHz frequency probe. The device was appropriately preset to “thyroid” for assessment. Color Doppler gain was adjusted as high as possible just before detecting excessive noise artifacts. Wall filter was low. Each nodule was imaged in at least two planes using a colored frame large enough to encompass the entire nodule. The ultrasonographic characteristics of the target nodule for FNA were reported in detail, and appropriate images were recorded on the device. In the reporting, the localization of the nodule, nodule structure (solid/cystic/heterogeneous), maximum diameter, anteroposterior (AP)/transverse (TRV) diameter, volume (AP diameter × TRV diameter × craniocaudal diameter × 0.52), multinodularity, presence of halo (partial/full), contour (smooth/irregular or lobulated), echogenicity relative to the overlying strap muscle and thyroid, vascularity of the nodule (absent/peripheral/central), presence of calcification (macro/micro), and BTA U classification were noted. BTA U grading was performed prospectively on the US reports and images of patients with these criteria. BTA U grades were categorized as follows: U1 = normal; U2 = benign; U3 = indeterminate; U4 = suspicious; and U5 = malignant. In the study, U2 was included in the benign group, U3 in the indeterminate group, and U4 and U5 were included in the malignant group for radiologic-pathologic comparison.
FNA procedures were performed by a single radiologist without the support of rapid on-site evaluation (ROSE), as this technique is not available in our hospital. Routine FNA was performed by taking at least two aspirations per nodule with a 20-mL syringe using a 22–25 gauge, 1-1.5-inch-long needle. Most commonly, 2–3 passes were taken (range = 2–6). The needle contents spread on slides were fixed in 95% alcohol and Papanicolaou stain. In each biopsy, 4–6 preparations were spread. At least 10 experienced pathologists reported pathology findings and Bethesda classification was performed. Bethesda categories were as follows: I = non-diagnostic or unsatisfactory; II = benign; III = atypia of uncertain significance/follicular lesion of uncertain significance; IV = follicular neoplasm (FN) or suspicious for follicular neoplasm (SFN); V = suspicious for malignancy and category; and VI = malignant. Category II is included in the benign group; category III is included in the indeterminate group, and categories IV, V, and VI were included in the malignant group.
Statistical analysis
Statistical analysis was performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). Continuous variables were compared using the Kruskal–Wallis test, and median (range) values were given. Categorical variables were expressed as numbers and compared using the chi-square and Monte-Carlo tests. Cohen’s Kappa analysis was performed for radiology pathology concordance. Logistic regression analysis (LRA) evaluated ultrasonographic findings for malignancy prediction. Multivariate analyses were performed by including predictor variables in the same model. P <0.05 was considered statistically significant. The diagnostic performance of FNA and ultrasonographic findings were compared to pathological results.
Results
During the examination of the study, a total of 572 cases of thyroid nodules were encountered. Of these cases, 18 thyroid nodules were determined to be cystic and were excluded from study. Of the remaining 554 solid nodules, 51 were non-diagnostic (Bethesda class 1) on pathology. Bethesda class 1 cases were excluded so as not to affect the radiology-pathology evaluation result. The final number of cases in the study was 503 thyroid nodules (112 men [22.27%], 391 women [77.73%]).
There were 51 (9.2%) nodules in the Bethesda class 1 group, representing non-diagnostic or unsatisfactory findings. The distribution of nodules in Bethesda class 1, according to ultrasonographic findings, was as follows: U2 = 20 (39%) nodules; U3 = 16 (31%) nodules; U4 = 9 (18%) nodules; and U5 = 6 (12%) nodules.
According to US findings, 212 nodules belonged to U2, 171 to U3, 84 to U4, and 36 to U5. According to pathologic evaluation, 287 nodules were classified as Bethesda class 2, 159 nodules as Bethesda class 3, 18 as Bethesda class 4, 27 as Bethesda class 5, and 12 as Bethesda class 6 (Table 1).
BTA U and Bethesda distribution of nodules.
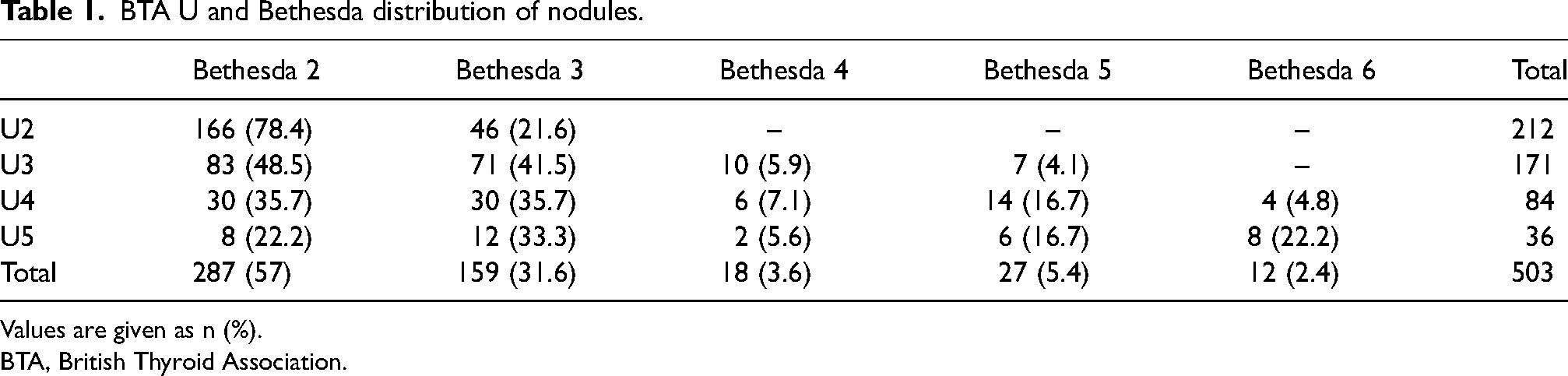
Values are given as n (%).
BTA, British Thyroid Association.
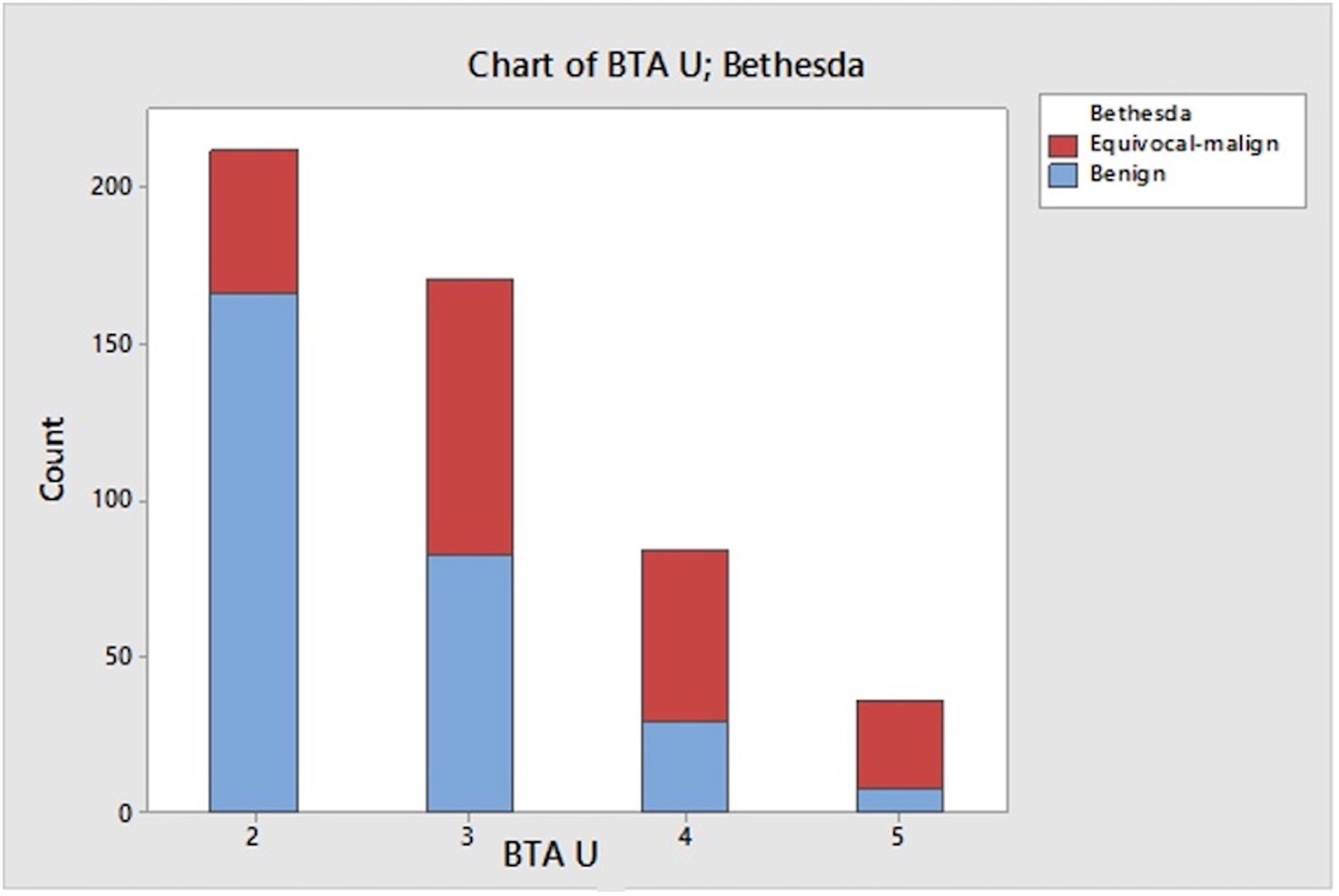
Bethesda classes 4, 5, and 6 were not detected in any of the U2 nodules but Bethesda class 6 was detected in U3 nodules. The total malignancy (Bethesda class 4–5) rate in U3 nodules was 10% (Fig. 1a–d, Table 1). In U4 and U5 nodules (Fig. 2a–d), malignancy (Bethesda classes 4–6) rates were 28.6% and 44.5%, respectively (Fig. 3). According to cytopathology, of the 503 nodules, 287 (57.1%) were benign, 159 (31.6%) were indeterminate, and 57 (11.3%) were malignant. The rate of malignant nodules was found to be significantly higher at younger ages (P = 0.039). The nodule diameter, nodule volume, and AP/TRV diameter ratio were not significantly different between the groups (Table 2).
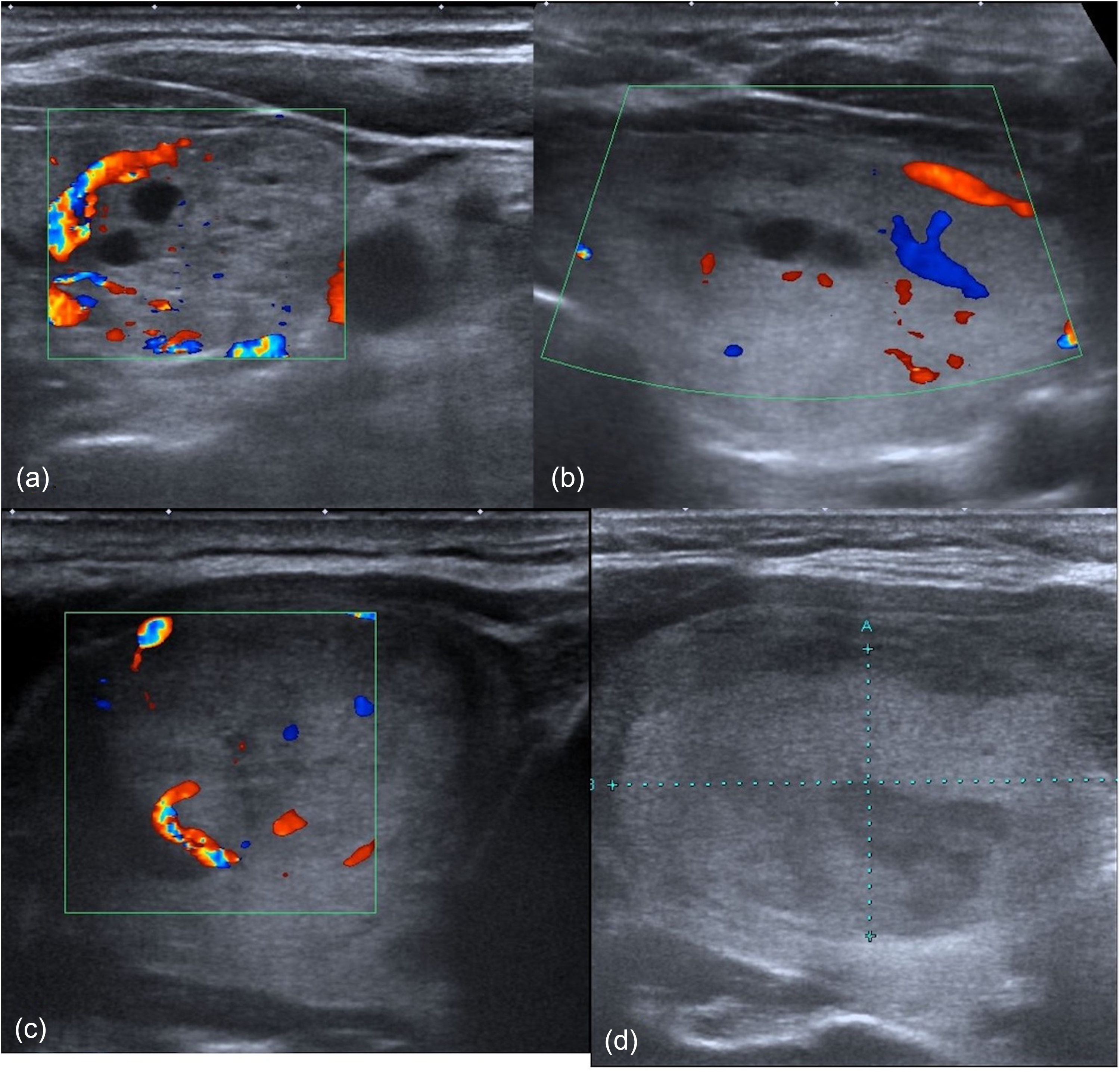
(a) A 48-year-old female patient with a 21-mm diameter isoechoic nodule (U2) in the left lobe of the thyroid was reported as Bethesda class II. The nodule has a complete halo, peripheral vascularization, and cystic components. (b) A 46-year-old female patient with a 43-mm diameter isoechoic nodule (U3) in the left lobe of the thyroid was reported as Bethesda class II. The nodule has a complete halo, cystic components, and peripheral and central vascularization. (c) A 46-year-old male patient with a 35-mm diameter isoechoic nodule (U3) in the right lobe of the thyroid was reported as Bethesda class IV. The nodule has a complete halo, cystic components, and peripheral and central vascularization. This case was confirmed by the result of the operation. (d) A 44-year-old female patient with a 37-mm diameter hyperechoic nodule (U3) in the right lobe of the thyroid was reported as Bethesda class V. The nodule has a complete halo, cystic and hypoechoic components, and peripheral vascularization. This case was confirmed by the result of the operation.
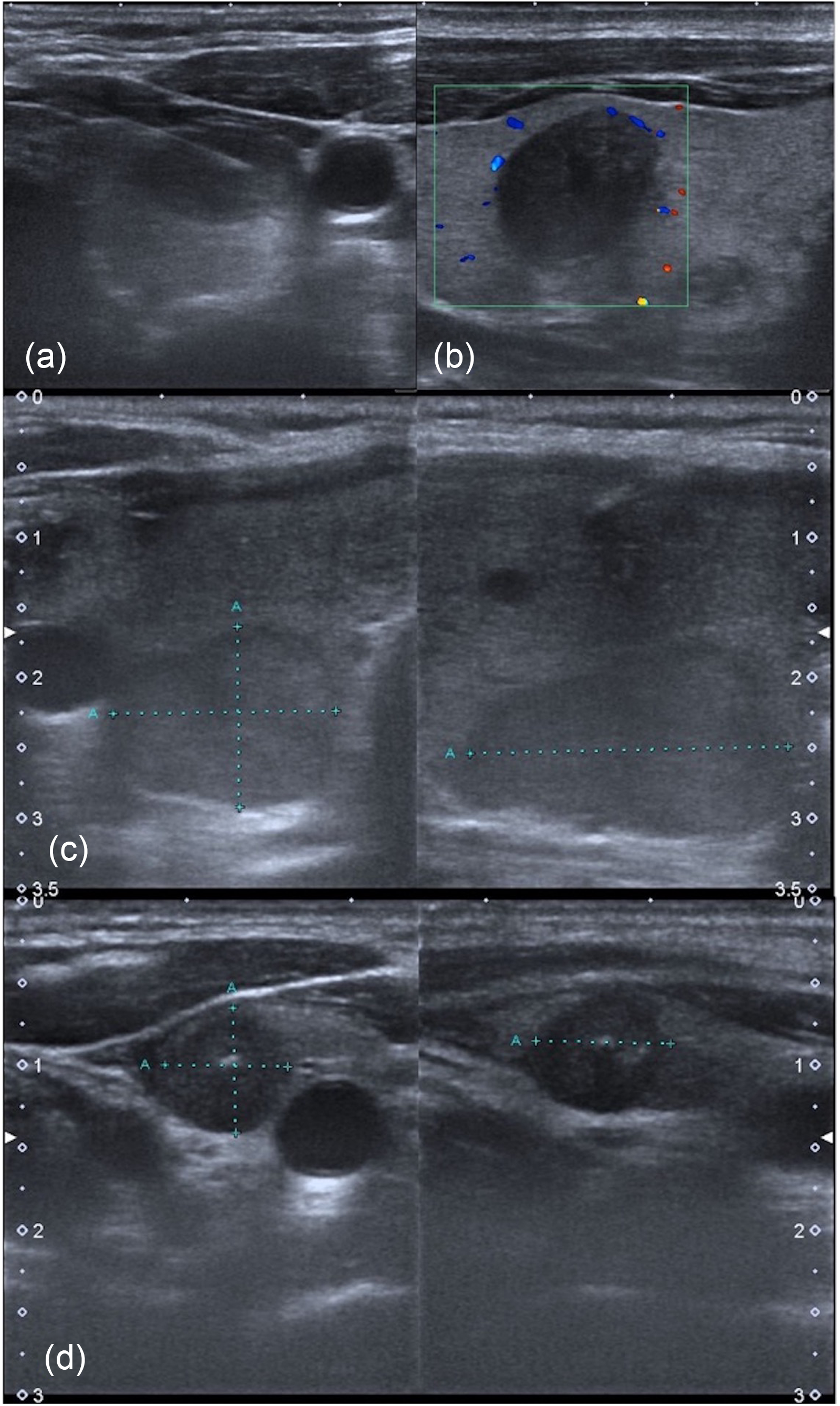
(a) A 60-year-old female patient with a 23-mm diameter hypoechoic nodule (U4) in the left lobe of the thyroid was reported as Bethesda II class. (b) A 55-year-old male patient with a 15-mm diameter hypoechoic nodule (U5) in the left lobe of the thyroid was reported as Bethesda class II. The anteroposterior/transverse diameter ratio of the nodule was measured as 1.17 mm. No obvious vascularization is observed in the nodule. (c) A 46-year-old female patient with a 22-mm diameter hypoechoic nodule (U4) in the right lobe of the thyroid was reported as Bethesda class VI. Diameter measurement of the nodule in three planes is shown. (d) A 30-year-old female patient with an 8-mm diameter hypoechoic nodule (U5) in the left lobe of the thyroid was reported as Bethesda class VI. The anteroposterior/transverse diameter ratio of the nodule was measured as 1.02 mm. Microcalcifications are seen within the nodule.
Pathological correlation of nodules according to British Thyroid Association U classification.
The comparison of the mean values of the parameters that did not exhibit normal distribution.
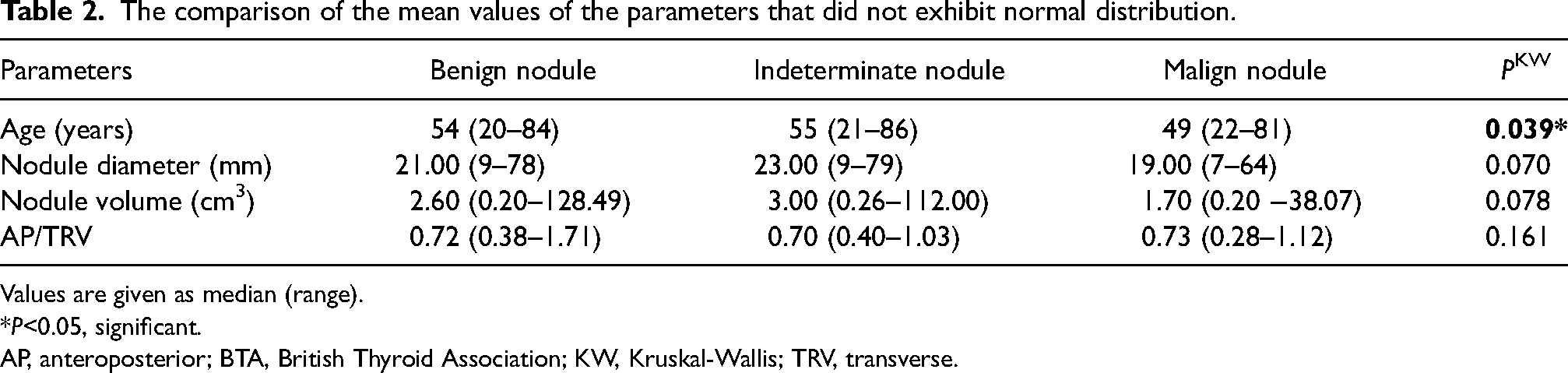
Values are given as median (range).
*P<0.05, significant.
AP, anteroposterior; BTA, British Thyroid Association; KW, Kruskal-Wallis; TRV, transverse.
In this study, no significant association was found between nodule localization and sex in differentiating among groups. Heterogeneous echotexture was significantly associated with benign nodules, whereas a pure solid nodule was strongly correlated with malignant nodules (P <0.001). Irregular margins were significantly more frequent in malignant nodules (P = 0.001). The absence of a halo was significantly associated with malignancy (P <0.05). Central vascularization was a strong predictor of malignancy (P <0.001), and solitary nodules were significantly more likely to be malignant (P = 0.002) (Table 3).
Distribution of nodules according to sex and ultrasound characteristics among benign, indeterminate, and malignant groups.
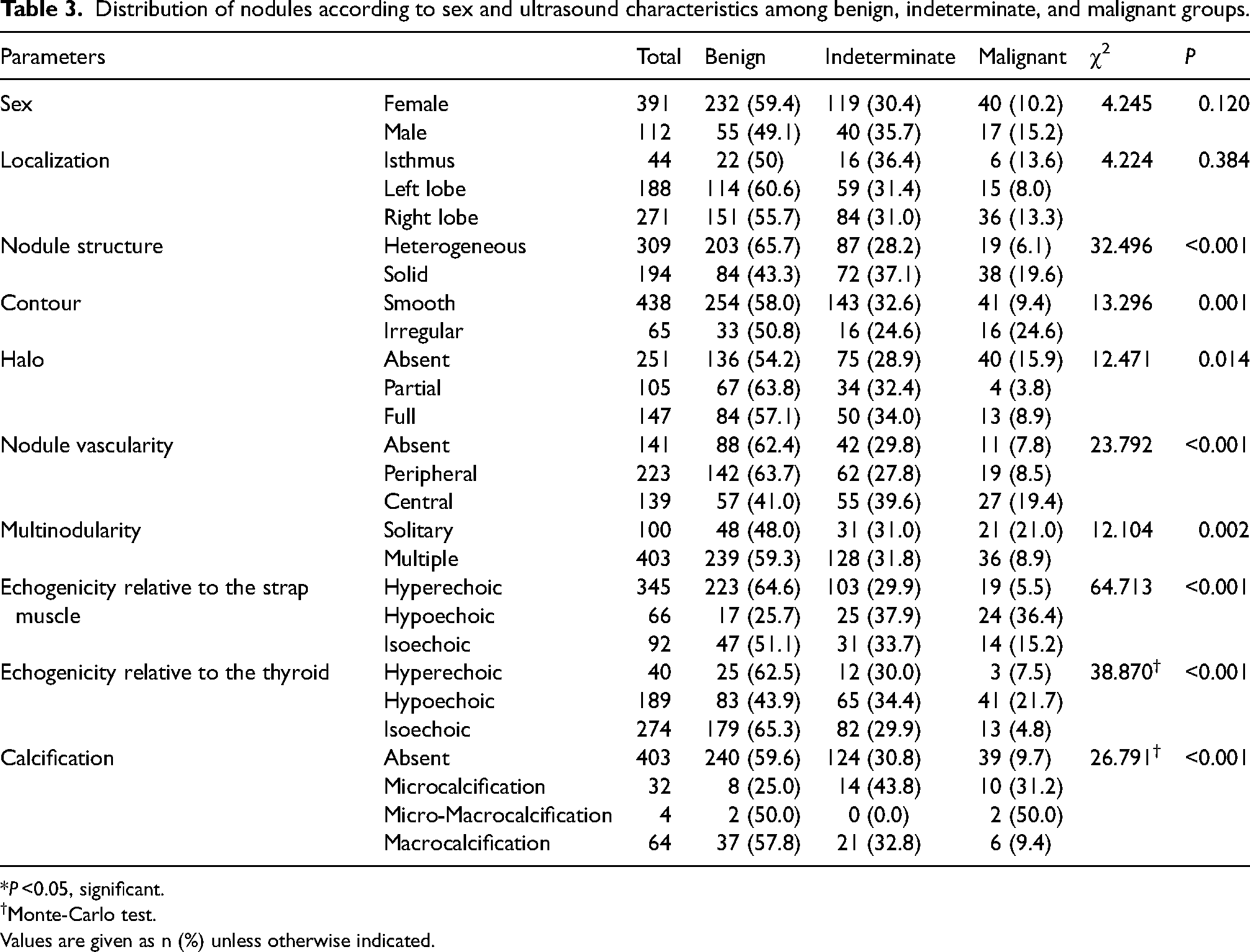
*P <0.05, significant.
†Monte-Carlo test.
Values are given as n (%) unless otherwise indicated.
Echogenicity patterns also differed between benign and malignant nodules: malignant nodules were predominantly hypoechoic relative to strap muscle, whereas benign nodules were hyperechoic (P <0.001). Similarly, malignant nodules were hypoechoic relative to thyroid parenchyma, while benign nodules tended to be isoechoic (P <0.001). The presence of microcalcifications was significantly associated with malignancy, while the absence of calcifications was more frequent in benign nodules (P <0.001) (Table 3).
Comparison of ultrasonographic findings with pathological results is given in Table 4 according to the chi-square test. Accordingly, a positive correlation was found between U2 nodules and pathological benignity, and U4, U5 nodules and pathological malignancy (P < 0.001). Indeterminate nodules in ultrasonography did not show a distinct correlation with pathological results.
BTA U and Bethesda comparison analysis results.

BTA, British Thyroid Association.
The result of the Cohen's Kappa coefficient for the agreement between the BTA U classification and Bethesda findings is 0.28, indicating a fair level of agreement (sensitivity = 0.70, specificity = 0.57, positive predictive value = 0.33, negative predictive value = 0.78) (Table 4). Table 5 shows the contribution of ultrasonographic variables to the model in logistic regression analysis by removing the suspicious group in pathological results (Bethesda). The main effect module was selected, and the reference category was generated by SPSS as nodule structure (heterogeneous), contour (smooth), halo (absent), nodule vascularity (absent), multinodularity (solitary), echogenicity relative to the muscle (hyperechoic), and calcification (absent). In multivariate logistic regression, nodule vascularity, and echogenicity referring to strap muscle, ultrasonographic variables that showed significant association with malignancy. Age, AP/TRV diameter, nodule structure, contour, halo, nodule vascularity multinodularity, echogenicity referring to strap muscle, and calcification parameters were entered and P <0.05 and an accuracy rate of 85.5% were obtained (Table 6). The analysis was conducted at the level of the main parameters. Subcategories were not entered into SPSS as independent variables and thus were not analyzed separately.
Individual contribution of BTA ultrasound morphological characteristics to the logistic regression model for predicting malignancy.
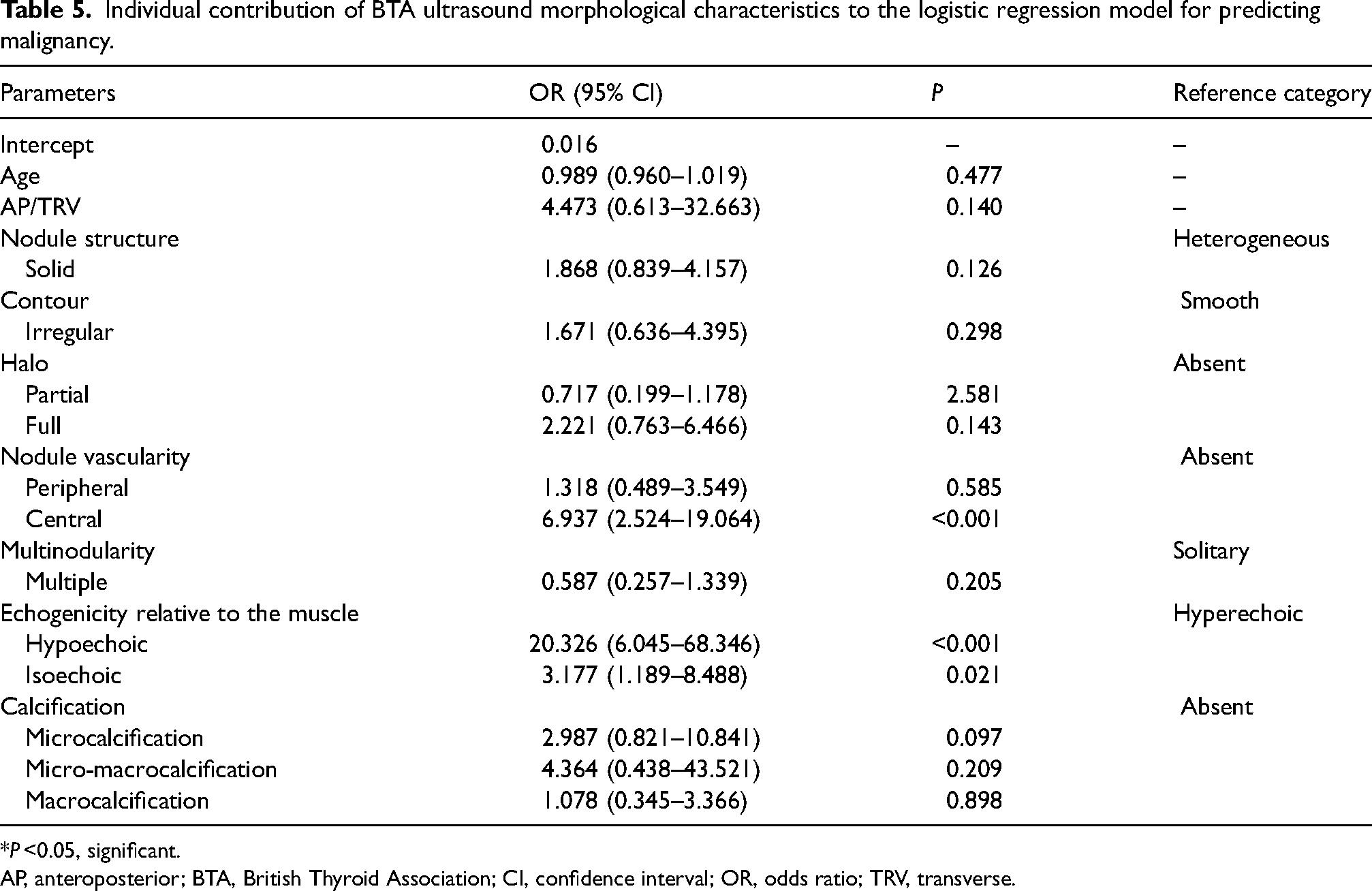
*P <0.05, significant.
AP, anteroposterior; BTA, British Thyroid Association; CI, confidence interval; OR, odds ratio; TRV, transverse.
Bethesda outcomes after logistic regression analysis of individual BTA ultrasound morphological characteristics.
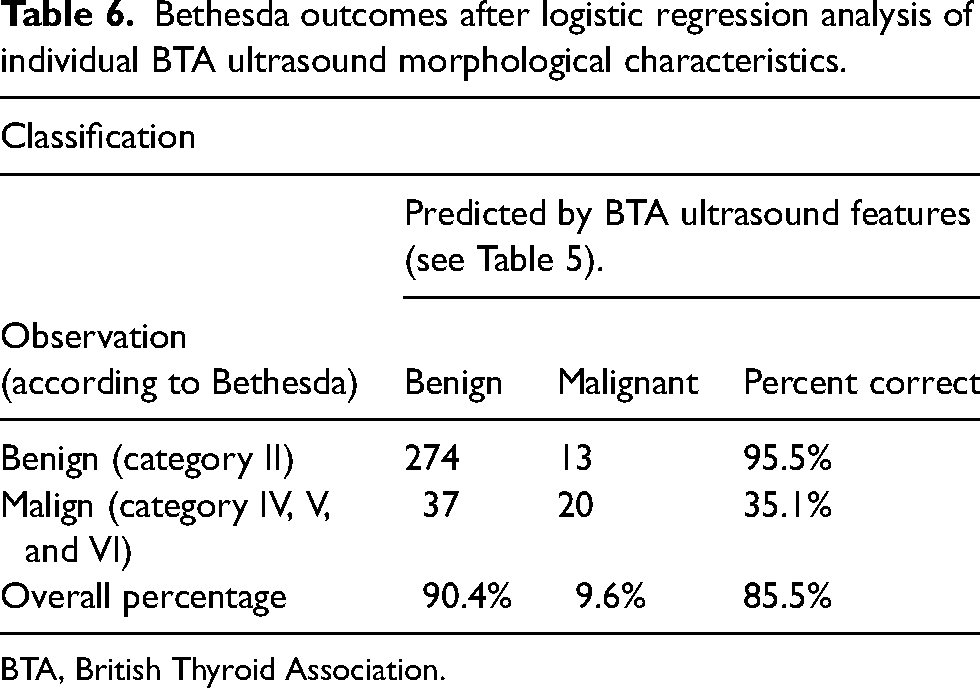
BTA, British Thyroid Association.
Discussion
This study performed FNA on 503 solid nodules, and malignant nodules were reported pathologically at 11.3% and indeterminate nodules at 31.6%. US features of benign thyroid nodules were heterogeneous internal structure, hyperechogenicity referring to strap muscle, and isoechogenicity referring to the thyroid. It was observed that prominent hypoechoic nodules, nodules containing microcalcification, solid nodules, and nodules with central vascularization were highly correlated with malignancy, whereas solitary nodules, irregularly contoured nodules, and nodules without halo were less significantly associated with malignancy. An accuracy rate of 85.5% was obtained using US findings, showing a significant or marginal relationship with the malignant nodule result.
When we look at radiology and pathology correlation rates, a study in the literature on 987 nodules recorded a malignancy rate of 2.1% in U2, 10% in U3, 51.3% in U4, and 80.9% in U5 (15). In a study of 129 nodules, Arambewela et al. reported the malignancy rate in patients undergoing thyroid surgery as 13.6% in U2, 30.4% in U3, 40% in U4, and 100% in U5 (16). In another study of 308 thyroid nodules, malignancy was 18.2% in U2, 39.4% in U3, 65.9% in U4, and 85.1% in U5 (17). Persichetti et al. (15), BTA thyroid cancer guidelines, American Thyroid Association (ATA) (86%), and the American Association of Clinical Endocrinologists (AACE/ACE/AME) (86%) compared different US modalities using US grading of thyroid lesions for high risk of malignancy and low and intermediate risk categories and found a higher accuracy rate of 89% for BTA. In one study, the accuracy rate was stated as 79% with TIRADS and 97% with Bethesda (18). Accordingly, in the current BTA U classification study, 0% malignant nodules were detected in U2, 10% in U3, 28.6% in U4, and 44.5% in U5. In fact, although FNA is generally not recommended in U2 nodules, FNA procedures were performed in cases of clinical suspicion and incompatibility predicted by the clinician. The relatively low agreement rates between Bethesda and U4 and U5 classes may be explained by the fact that hypoechoic-complicated cystic nodules gave a solidified appearance on US and were included in the high BTA U category. The absence of vascularization in these nodules on Doppler examination supports this idea. In addition, in some patients with a history of surgery, residual thyroid tissue was included in the high U category due to hypoechoic, high AP/TRV diameter, and irregular contour features, which may contribute to this discordance.
Damião et al. noted in their study of 147 nodules that individuals in the malignant group were younger (19). Xu et al. reported no association between age and benign or malignant groups (5). Another study of 1290 nodules explained that the incidence of malignant nodules in the younger group was significantly higher than in the older group (20). A study of 400 nodules noted that age had no effect on the risk of malignancy (21). In this study, thyroid malignancy rates were higher in the younger age group. Differences between studies are seen due to different populations and patient selection. Similarly, in correlation with the literature, no effect of sex on thyroid malignancy was shown (5,10,21). Again, in correlation with the literature (2,22), thyroid nodules were more common in women (77% in the present study).
In some studies, conducted on different case series, it was reported that there was no correlation between nodule size and malignancy (3,5,10,19). In contrast, a study noted that increasing nodule size carries a higher risk of malignancy (21). The present study showed no difference between benign and malignant nodules in maximum diameter, volume, and AP/TRV diameter ratios. Similarly, according to the thyroid lobe localization of the nodule, there was no difference between benign and malignant nodules (23), and no association with malignancy was found. Ramundo et al. reported that malignancy was detected more frequently in nodules with middle localization when examined at the upper, middle, and lower poles. However, there was no difference according to the lobe (24).
In the present study, solidity was significantly higher in malignant nodules when the internal structure of thyroid nodules was evaluated. Heterogeneous nodules containing solid and cystic components were significant for benignity. Heterogeneous texture in benign nodules may be due to the presence of colloid, cystic degeneration, or fibrosis, whereas solid structure in malignant nodules is often attributed to the dense cellularity of malignant tissue. These results are consistent with the literature (25–27). Regarding contour features, previous studies have shown that irregular margins are among the ultrasonographic findings of malignant nodules (25,26,28), and smooth contour was significant in benignity (27). In this study, although nodules with smooth contours were more frequently associated with benign pathology, irregular contours showed a significant correlation with malignancy. In their study of 170 thyroid nodules, Mohebbi et al. showed that a thin halo is among the features of benign nodules, and the absence of a halo is an important criterion for recommending FNA (29). Jinadu et al. reported that a thin peripheral halo was found in benign nodules (27). In the present study, nodules with a partial or complete halo gave more benign pathologic results and absence of halo showed low association with malignancy. When literature is examined, there are studies that associate the absence of a halo with malignancy and those that do not (30–33). We think these results may be due to the high number of complicated cystic nodules without halo and hypoechoic-heterogeneous internal texture due to dense content.
Vinayak and Sande reported that central vascularity is important in differentiating benign-malignant nodules (34). Similarly, Majstrov reported that central vascularization is more commonly an ultrasonographic finding of malignant nodules (2). Chng et al. did not find significant results in differentiating benign and malignant nodules in a study evaluating intranodular vascularity (25). In the study of 107 nodules by Jinadu et al., peripheral vascularization was significant for benignity (27). The present study revealed central vascularization as a significant ultrasonographic finding for malignant nodules. Furthermore, these study findings indicate that vascularity assessment in the BTA classification is associated with a significantly high odds ratio (OR = 6.9) for malignancy, suggesting its potential importance in risk stratification. This feature, which is not included in TIRADS, may provide additional diagnostic value and warrants further investigation.
In a study of 219 nodules by Zhang et al., multinodularity was not associated with malignancy (23). Multinodular thyroid gland was more common in this study and solitary nodules were found to have association with malignancy. In addition, the presence of microcalcification in the nodule was associated with malignancy in accordance with the literature (25,34–36).
Many studies in the literature show that hypoechoic nodules in the thyroid are significant for malignancy (2,25,29,35,36). Since some pathologies, such as thyroiditis, may reduce the echogenicity of the gland, the detected nodules may appear with relatively different echogenicities and may lead to discordance in the Bethesda-BTA U comparison (37). Therefore, in the present study, thyroid nodule echogenicity was also evaluated according to the surrounding strap muscles. Accordingly, it was found significant that malignant nodules were hypoechoic, referring to both the thyroid and muscle, and benign nodules were hyperechoic, referring to muscle, and isoechoic, referring to the thyroid.
Alam et al. (28) obtained an overall accuracy of 82% in differentiating benign and malignant nodules according to ultrasonographic features. Majstrov obtained 76.2% accuracy in multivariate LRA by entering ultrasonographic variables that showed significance or marginal association with malignancy (2). In this study, an accuracy rate of 85.5% was obtained by entering ultrasonographic parameters that showed a significant association with malignancy in the multivariate LRA.
In the present study, it was observed that U2 nodules were the most common in the Bethesda 1 group. The reason is that since there are more complicated cystic nodules in the U2 class, such nodules can be predicted as FNA insufficiency (15,38,39).
Bethesda 3 is described in the Bethesda System as atypia of undetermined significance or follicular lesion of undetermined significance. Since it does not provide a differential diagnosis between malignant and benign lesions, re-biopsy is recommended for nodules detected in this class for malignancy risk and management recommendation (40). Actual malignancy rates for Bethesda class 3 are in the range of 10%–30% in patients undergoing surgery (41–43). In this study, 31.6% of Bethesda class 3 nodules were detected and the BTA U class distribution was 21.6% U2, 41.5% U3, 35.7% U4, and 33.3% U5. In this study, the long-term results of the patients could not be followed up and the current status of the nodules was evaluated. Therefore, the outcome of Bethesda class 3 nodules was not included in the study and further categorization was not performed. This can be considered as a limitation due to the retrospective design of the current single-center study.
Further categorization could not be made because the study was retrospective. In addition, comparison with operative results could not be made for each nodule. Biopsies were repeated twice in 23 patients and three times in one patient. A surgical history of 14 patients was obtained. Non-diagnostic biopsy results (Bethesda class 1) were 9.2%. Despite the lack of ROSE, this rate is comparable to studies where on-site cytology assessment was available.
In conclusion, this study revealed that ultrasonographic features such as hypoechoic solid nodules, central vascularization, solitary nodules, and microcalcifications are important for differentiating malignant thyroid nodules. According to BTA U categorization, high pathological correlation was obtained, especially in the U2 and U5 classes. Although U3 nodules are considered low risk for malignancy, FNA should be recommended in suspicious cases. US and ultrasonography-guided FNA can be used effectively in the diagnosis, follow-up, and surgical planning of thyroid nodules.
Footnotes
Acknowledgments
The study was presented orally at the 9th International Hippocrates Congress on Medical and Health Sciences on 10 October 2022.
Authorship contribution statement
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.