
Abstract
Background
Superior capsular folds and fold-like structures in the glenohumeral joint are potential sources of superior shoulder POS=12ptpain.
Purpose
To obtain detailed information about the arthrographic anatomy and morphology of superior capsular folds and fold-like structures.
Material and Methods
This study followed a retrospective design and involved 300 consecutive shoulder magnetic resonance (MR) images and MR arthrograms in two centers. The origins and insertions of the superior capsular folds and fold-like structures in the glenohumeral joints were carefully examined and documented. Four subtypes of extensions in the sagittal-oblique plane of the posterior synovial fold were identified from the MR arthrograms, according to their associations with the biceps tendon long head, superior glenoid notch, and supraspinatus tendon. Further, two morphological subtypes of superior synovial folds were identified: cord-shaped and fan-shaped.
Results
Superior capsular folds and fold-like structures in the shoulder joint were identified in 11 (4%) patients. Of these 11 superior capsular folds, 6 (54.5%) were then confirmed upon arthroscopy. The cord-shaped type was the most common MR arthrographic superior synovial fold and was detected in 8/11 (72.7%) patients. Type B was the most common form according to the course and insertion of the superior capsular fold (4/11 [37%] patients).
Conclusion
Superior capsular folds, probably normal capsular anatomical variants, tend to be present in the posterior portions of the superior shoulder joint capsule and are rarely seen in MR arthrograms. These anatomical variations tend to be symptomatic, especially in young individuals.
Introduction
The shoulder is the joint with the greatest range of movement in the human body. The rotator interval, which is located in the superior of the shoulder joint, contains fundamental anatomical structures such as the coracohumeral ligament, superior glenohumeral ligament, and biceps tendon long head. Rotator intervals and contents have been examined in detail in radiological cross-sectional studies, and the pathologies of these structures and the associated clinical outcomes are widely discussed in the literature (1–5).
Synovial folds of the shoulder joint are accepted as remnants of embryological development. Although radiological and arthroscopic series of posterior synovial folds are covered in the literature, very few studies have focused on superior folds (6). It is emphasized in the literature that synovial folds can mimic some pathologies. Superior synovial folds can also be confused with other anatomical variations (such as superior glenohumeral ligament multiplication, biceps vincula, and rotator cable) of the rotator interval in cross-sectional imaging.
Magnetic resonance imaging (MRI) is frequently used for joint imaging because of its high soft-tissue resolution. However, local capsule thickenings, such as ligaments and folds, may not be optimally evaluated with MRI, especially when there is not enough fluid in the joint (7). Direct MR arthrography is an imaging method that facilitates the optimal evaluation of capsuloligamentous structures. Accurate and timely diagnoses in experienced hands are critical. Correct descriptions of synovial folds on MR arthrograms decrease the possibility of misdiagnosis, preventing patient exposure to unnecessary surgical interventions (8,9).
To the best of our knowledge, the literature does not contain detailed reports on the radiological definition of superior folds in the shoulder joint. Therefore, the aim of this study was to obtain a detailed MR arthrographic definition of superior synovial folds that would facilitate differential diagnoses and to determine whether there are any clinical outcomes of these anatomical variations.
Material and Methods
A total of 300 shoulder MR arthrograms of 292 patients who were referred to our clinic for different pathologies, such as labral lesions, capsuloligamentous injuries, rotator cuff tears, and internal/external impingement syndromes, were evaluated retrospectively for superior capsular fold anomalies by two musculoskeletal radiologists with 18 and 5 years of arthrography experience. The shoulder MR arthrograms were obtained between January 2021 and December 2024 (Fig. 1). The study was conducted in accordance with the principles of the Declaration of Helsinki. Institutional review board approval for this study was made by the local ethics committee of the Istanbul Medipol University (14/11/2024 = E-10840098-202.3.02-7002). Signed informed consent forms were obtained from all participants.
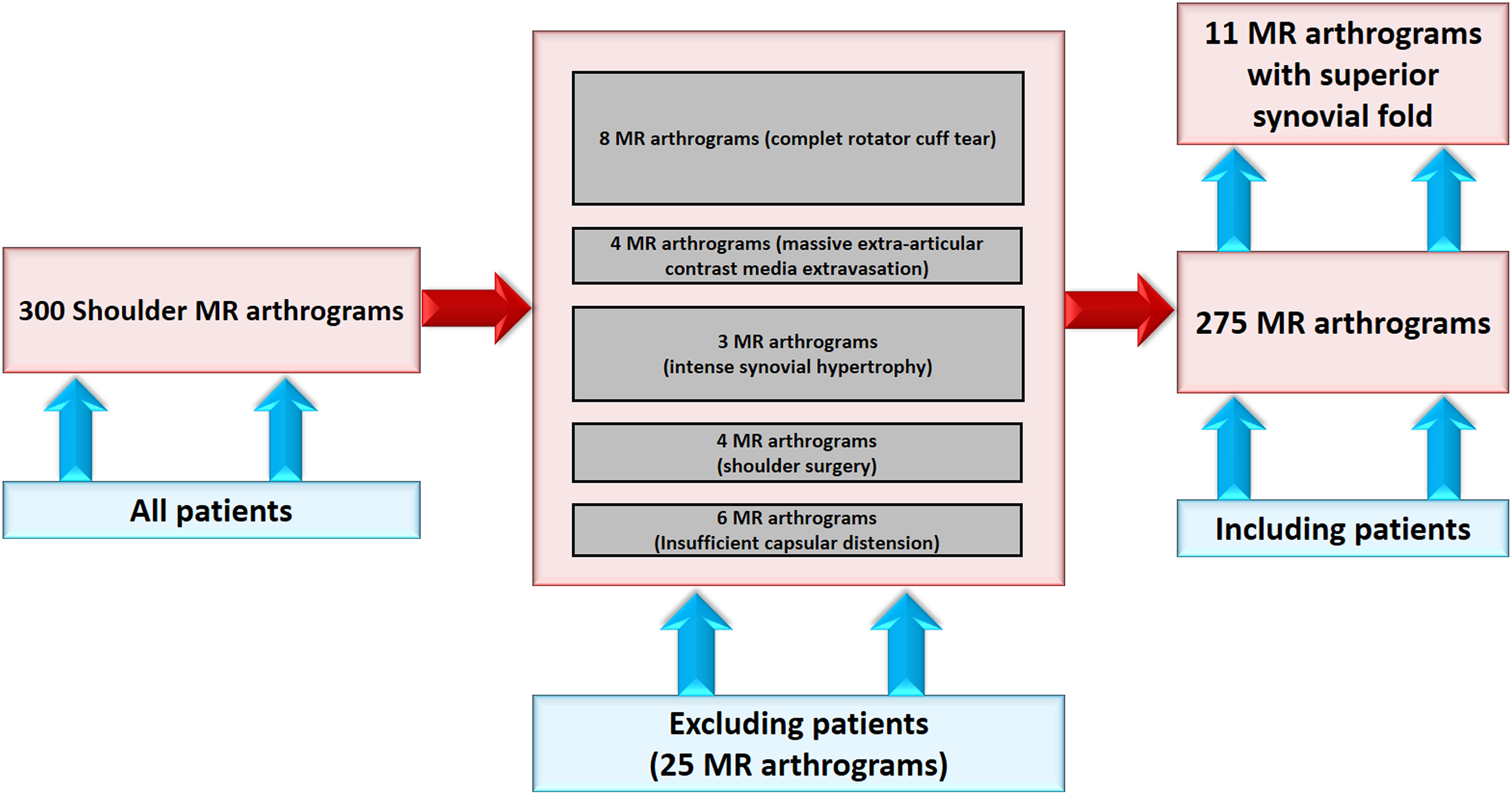
Schematic view of the inclusion and exclusion criteria.
All injections for shoulder MR arthrography were performed using a 20-G needle and an ultrasound-guided posterior approach on an outpatient basis, without any premedication. Diluted 1:200 gadolinium chelate at a volume of 12–20 mL was slowly injected into the shoulder until the joint was sufficiently distended. Joint capacity was determined according to each patient's comfort level and resistance to the injection volume.
All MR arthrograms were evaluated 15–30 min after the intra-articular injection procedure, using a 3 T MR device with a superficial shoulder coil. The protocol included the following MR arthrography sequences: transverse, oblique sagittal, and oblique coronal planes; T1-weighted (T1W) fat-suppressed turbo spin-echo; T2-weighted (T2W) oblique coronal plane; and T1W fat-suppressed 3D volumetric interpolated breath-hold examination (VIBE). The MR arthrography sequence parameters are summarized in Table 1.
3 T MR scanner routine MR arthrography sequence parameters.
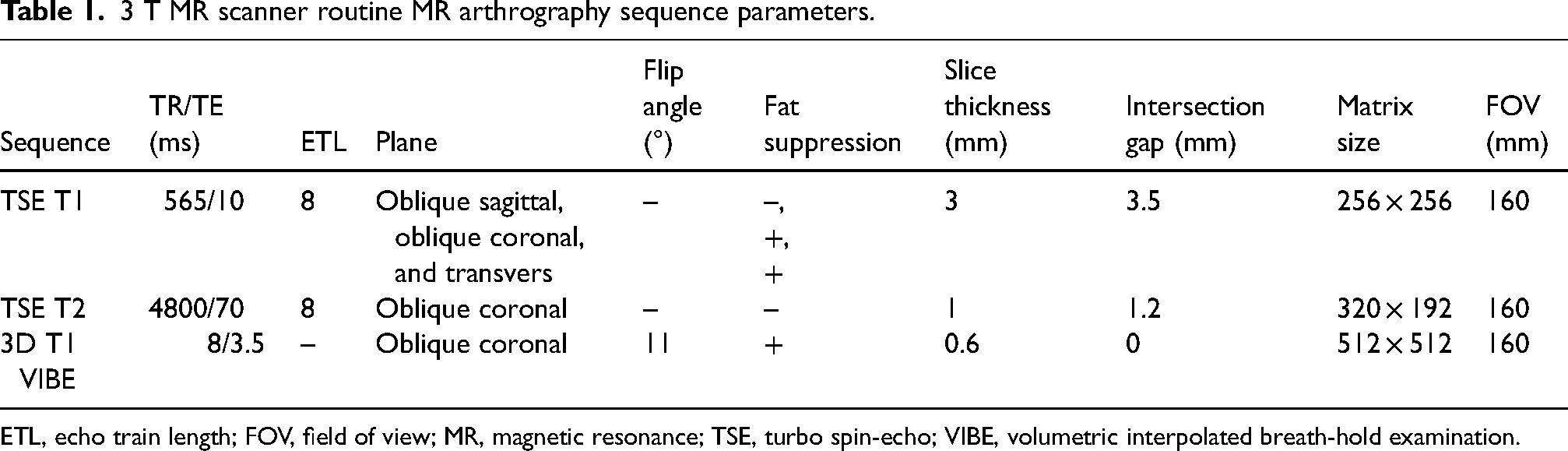
ETL, echo train length; FOV, field of view; MR, magnetic resonance; TSE, turbo spin-echo; VIBE, volumetric interpolated breath-hold examination.
Superior synovial folds were diagnosed by consensus between the examiners for each case. A total of 25 shoulder MR arthrograms obtained from 24 patients were excluded from the study. Fig. 1 shows the exclusion criteria and a patient selection flow chart. The following MR arthrography criteria were used to diagnose superior synovial folds: (i) rounded or flattened or cord-like thickening of the superior shoulder joint capsule, with a thickness of at least 2 mm that is detectable on least two planes upon volumetric MR arthrography examination; and (ii) separately defined intra-articular anatomical structures, such as the biceps tendon long head, superior glenohumeral ligament and middle glenohumeral ligament.
The presence of a superior capsular fold and its insertion level, course, and shape were examined using the 3D VIBE arthrography sequence. Extension in the vertical-oblique planes of the superior synovial folds was identified in the MR arthrograms according to the rotator interval structures and was of four subtypes (Fig. 2). The superior synovial folds were of two morphological subtypes: fan-shaped and cord-shaped.
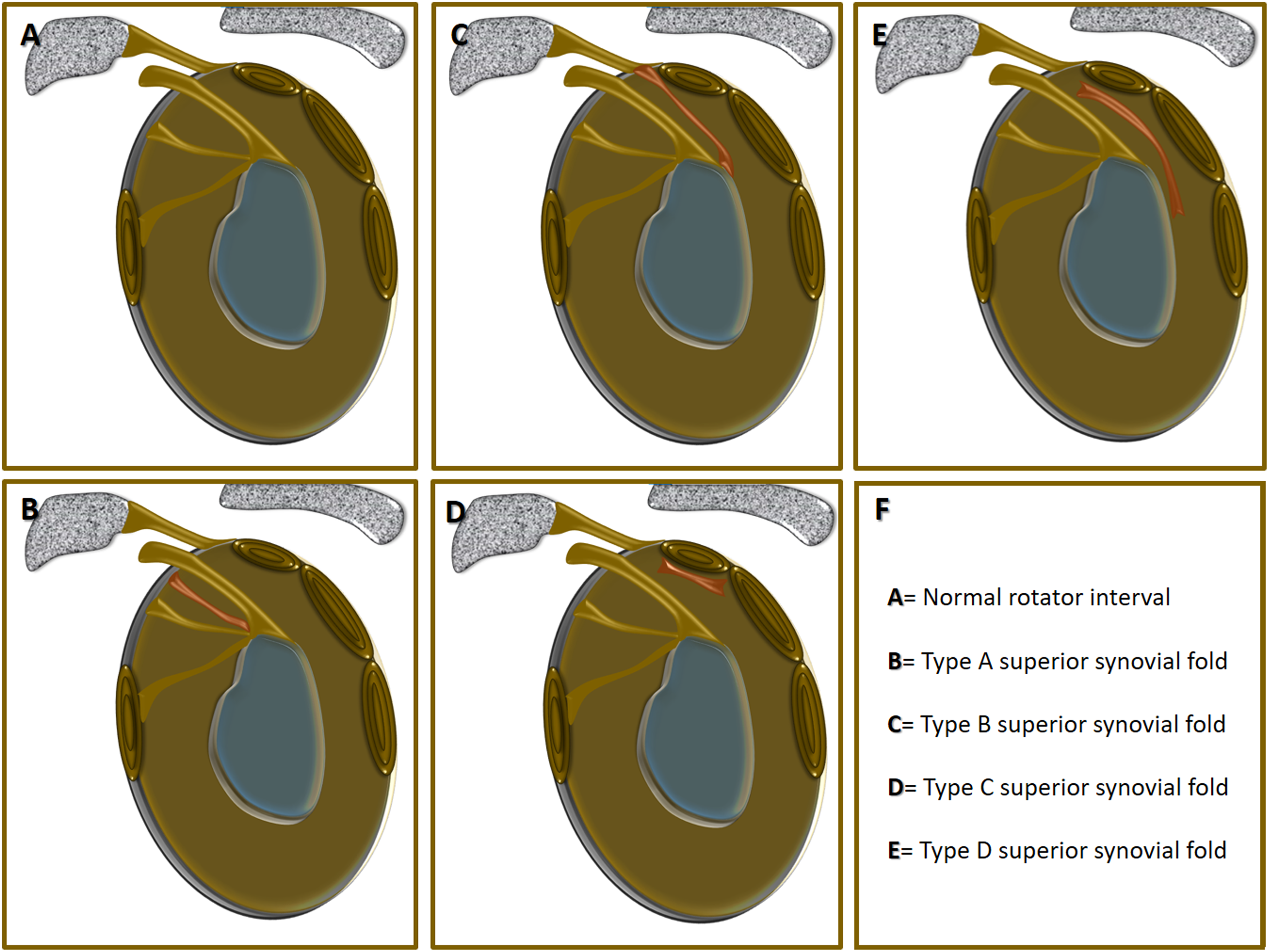
Illustration demonstrating the types of superior synovial folds in the coronal oblique plane.
All arthroscopic examinations were performed by an experienced shoulder surgeon. An arthroscopy-imaging correlation was found in 6/11 MR arthrograms. All the superior labroligamentous tears and capsular abnormalities detected on the MR arthrograms were carefully examined by the arthroscopic surgeon. The average time interval between an MR arthrographic examination and an arthroscopy was 2–6 weeks.
Complex statistical analyses were not performed in this study. The data were evaluated using SPSS 20 (IBM Corp., Armonk, NY, USA). Descriptive statistics were expressed as median (range) and mean ± SD values.
Results
The frequency of superior synovial folds on the MR arthrograms of the shoulder joints was 4% (11/275 arthrograms). The 11 patients with superior synovial folds (6 [54.5%] women and 5 [45.5%] men) had a mean age of 30.55 ± 14.13 years (age range = 18–54 years). MR arthrography was conducted for the right shoulders of 6 (54.5%) patients and the left shoulders of 5 (45.5%) patients.
Of the 11 patients with superior synovial folds, 6 (54.5%) underwent arthroscopic examinations. The findings revealed superior labrum anterior to posterior (SLAP) tears in three patients, Bankart lesion in two patients, and an anterior labroligamentous periosteal sleeve avulsion (ALPSA) lesion in one patient. The patients were all treated arthroscopically.
The cord-shaped morphological type was the most common MR arthrographic form of the superior synovial fold; it was detected in 8/11 (72.7%) patients (Fig. 3). The remaining 3 (27.3%) patients had fan-shaped superior synovial folds (Fig. 4). Furthermore, type B was the most common form based on the course and insertion of the superior synovial fold and was found in 4/11 (37%) patients. Only 2 (18%) patients had a superior extension of the posterior synovial fold (type D). The remaining patients had type A (3/11 [27%] patients) and type C (2/11 [18%] patients) superior synovial folds.
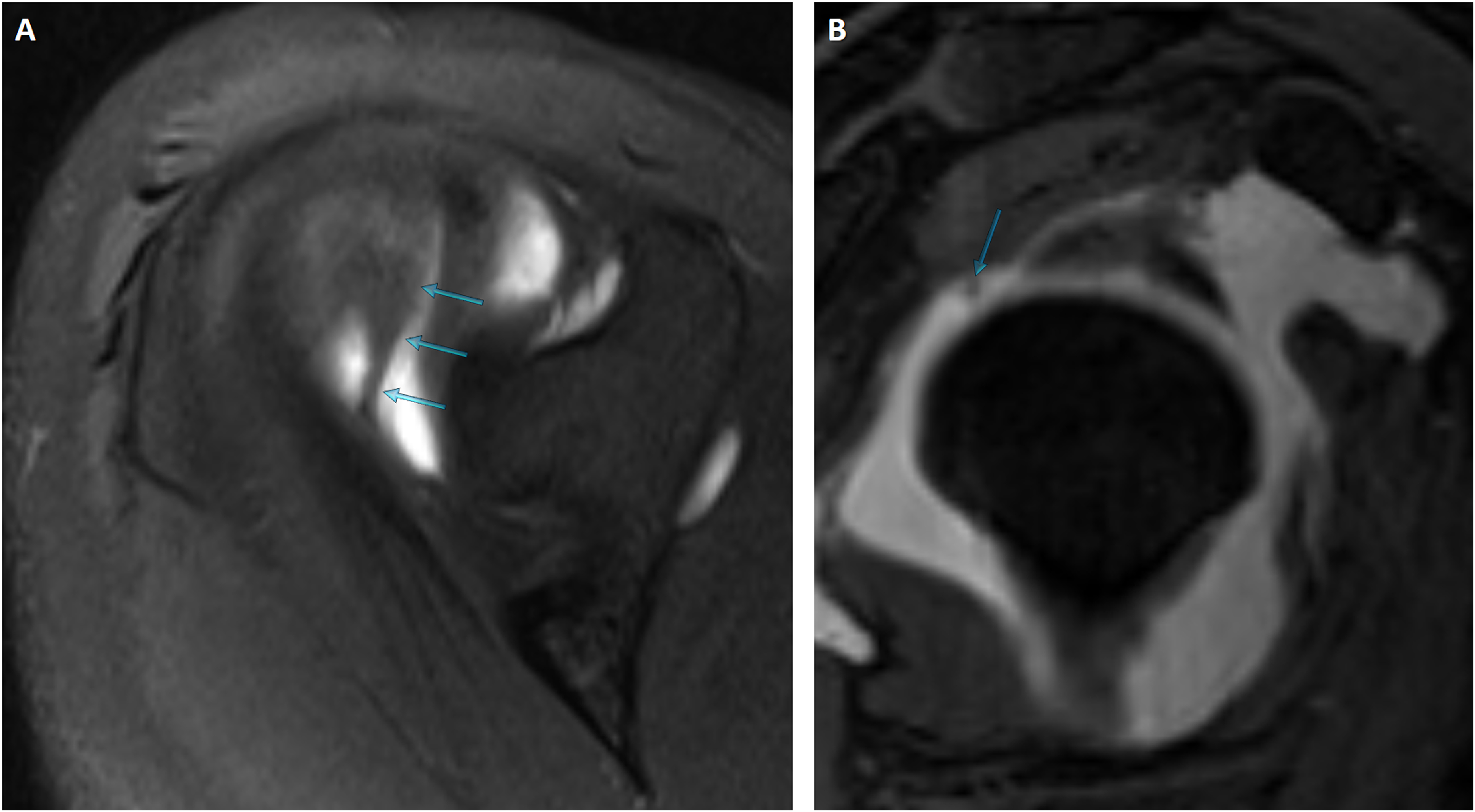
(a)#Axial and (b) sagittal oblique plane T1-weighted MR arthrograms demonstrating cord-shaped type C superior synovial folds (blue arrows).
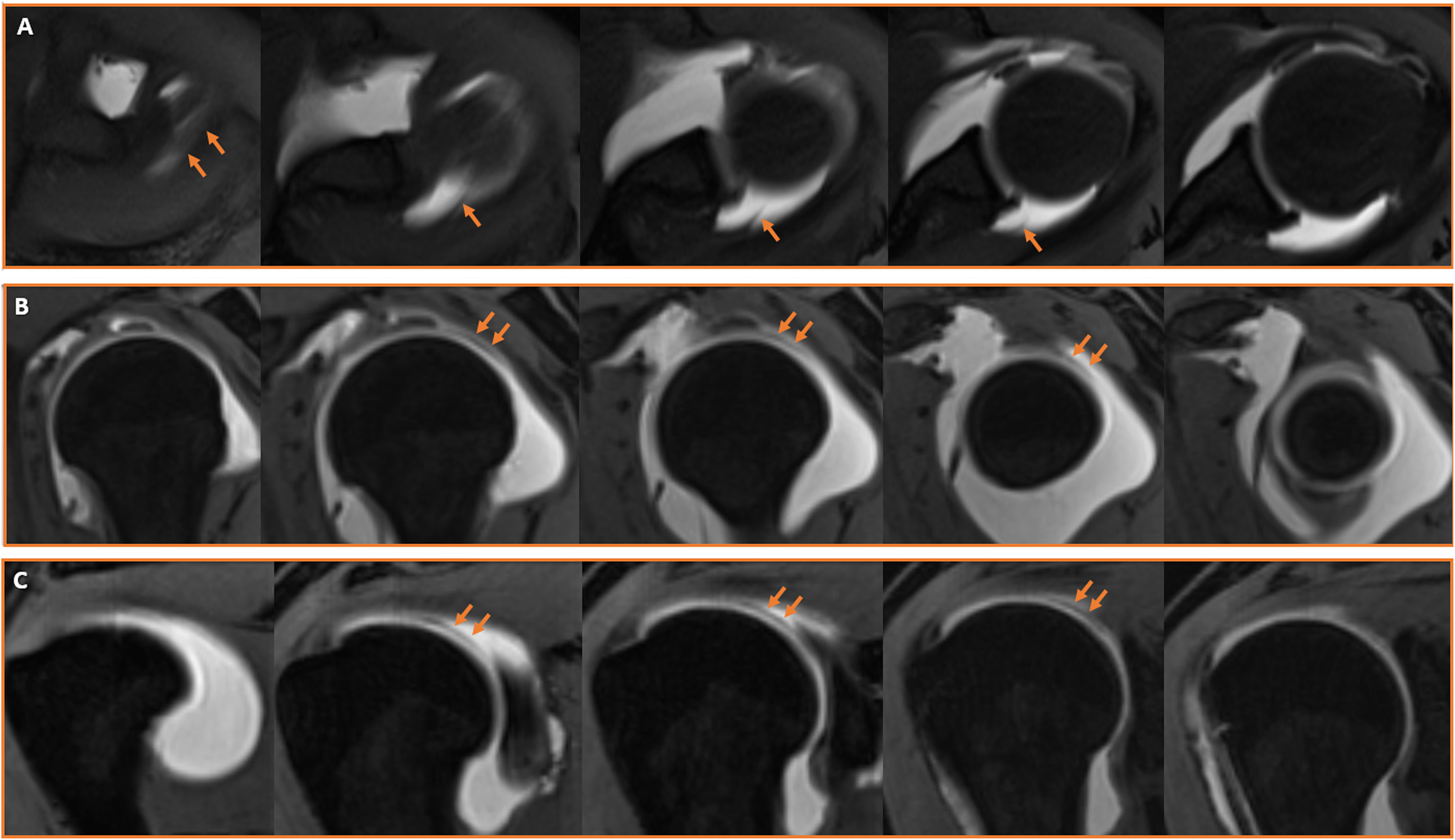
Consecutive (a) axial, (b) sagittal oblique, and (c) coronal oblique 3D VIBE T1-weighted MR arthrograms showing fan-shaped type D superior synovial folds (orange arrows).
Three patients who did not accept arthroscopic examinations had no MR arthrography results that could explain their clinical conditions. These patients were young (aged 18, 19, and 21 years) and experienced anterosuperior shoulder pain. Arthroscopy did not confirm the conditions of three patients in whom superior synovial folds were suspected upon MR arthrography. The first of these patients was diagnosed with a subtle partial thickness delaminated tear of the supraspinatus tendon at the time of arthroscopy (Fig. 5). The second patient had synovial hemosiderosis. The last patient was arthroscopically completely negative. The examiners re-evaluated the MR arthrography of this patient. A superior capsular image in the MR arthrogram was interpreted by them as a double synovial line that occurred due to a delayed MR examination.
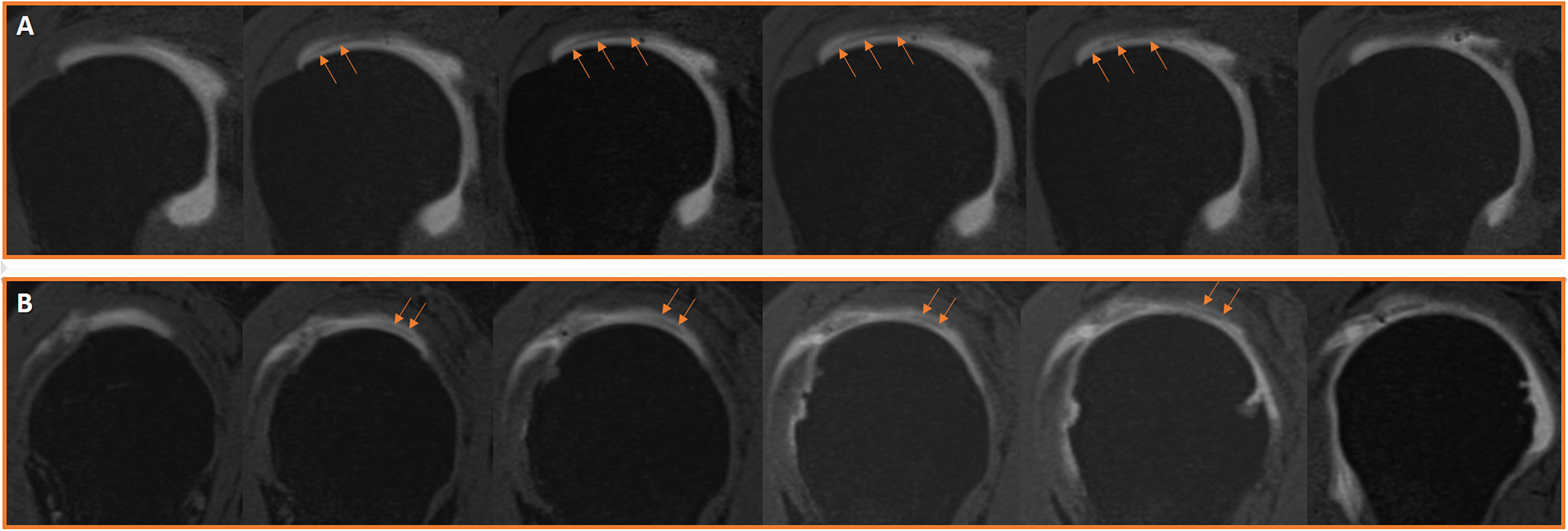
Consecutive (a) coronal oblique and (b) sagittal oblique 3D VIBE T1-weighted MR arthrograms showing a subtle partial thickness delamination tear of the supraspinatus tendon (orange arrows), which mimics a superior synovial fold.
Discussion
The study findings revealed that 4% of the patients who underwent shoulder MR arthrography had superior synovial folds. Some young patients who, based on their MR arthrograms, did not have other shoulder pathologies but had superior synovial folds experienced isolated superior shoulder pain. In addition, the MR arthrogram of a patient with a subtle partial delamination tear on the under surface of the supraspinatus tendon was reported to be a fold-like structure of the superior shoulder joint capsule.
Apart from the superior glenohumeral and coracohumeral ligaments, the other ligamentous structures located in the upper part of the shoulder joint are the accessory superior glenohumeral ligament, biceps vincula, rotator cable, and superior synovial fold. These anatomical structures may not be easily distinguished from each other on MR images. MR arthrography is a very sensitive imaging method that enables the examination of synovial folds or fold-like structures in the shoulder joint (7–9).
Correct diagnoses of fold or fold-like anatomic structures in the superior shoulder joint capsule are crucial for avoiding unnecessary surgical procedures. Although their clinical importance remains unclear, the present study's findings highlight the need to take these anatomical structures into account when treating symptomatic patients with no other known underlying medical condition.
Shoulder synovial folds are rest synovial septations that arise from the joint capsule's differentiation and formation of the joint cavity during embryonic development (10). In adulthood, these folds remain integral components of the joint capsule, contributing to passive joint stability. They are active and functional during joint movements; they fold inward and respond to joint dynamics in the form of hypertrophied focal capsular thicknesses. From a biomechanical perspective, synovial folds help distribute capsular stress during joint movements, thereby reinforcing the joint capsule and limiting excessive humeral head movements. Compared to glenohumeral ligaments, which offer static stability, these folds are adaptable and flexible and contribute to dynamic stability by lowering the friction between the joint surfaces and adjusting to movement (7,8,11).
The identification and morphological assessment of superior synovial folds in the shoulder joint are heavily dependent on imaging modalities and protocols. Conventional MRI is an effective modality that offers soft-tissue contrast, but it has limitations in accurately assessing small intracapsular anatomic structures, particularly when insufficient joint fluid is present. Computed tomography (CT) scanning is a very useful imaging technique for evaluating bone structure. However, this modality is inadequate for identifying soft tissues such as capsules, ligaments, and capsular folds (12). CT arthrography provides high spatial resolution, enabling the detailed visualization of fine intra-articular structures. However, this technique has a relatively low soft-tissue contrast resolution and exposes patients to radiation. Ultrasonography, with its portability and ease of use, offers several benefits, but it is insufficient for assessing complex anatomical structures, such as shoulder joint capsules and ligaments (7–9). After intra-articular injection, sonoarthrographic imaging of the glenohumeral joint can be performed in the same manner as conventional ultrasonography (13). In a sonoarthrographic examination, joint capsule distention allows for the separation and visualization of posterior capsular folds (13). However, no sonoarthrographic studies of superior synovial folds have been conducted.
Considering the above, MR arthrography is suitable for obtaining clear visualizations of superior synovial folds, specifically by inflating the joint capsule with intra-articular contrast agents. Notably, volumetric MR arthrography protocols with high-resolution 3D sequences enable accurate assessments of the morphology of these folds and their interactions with adjacent structures (7–9,14). The present study demonstrated that volumetric MR arthrography has high accuracy in identifying superior synovial folds and allows for the reliable differentiation of anatomical variations. Nevertheless, previous researchers have reported that arthroscopy is the gold standard for definitive diagnoses. It plays a critical role in confirming a diagnosis and distinguishing synovial folds from other pathologies through direct visual and physical evaluations (7–8,13,15).
When synovial folds become symptomatic, they manifest as “fold syndromes” and are characterized by clinical features such as pain, restricted movement, and recurrent inflammation due to mechanical irritation or impingement. Medial plica syndrome of the knee joint is the most frequently described fold syndrome in the literature. It has also been reported that plica structures in the ankle, elbow and hip joints can become pathological (7,16). The present study's findings indicate that superior synovial folds can be symptomatic in certain cases and may cause anterosuperior shoulder pain in young patients. Although conservative treatment is often preferred in such cases, arthroscopic excision is an effective treatment option when symptoms persist (16).
The present study has some limitations. One of them is its retrospective design. Retrospective studies frequently encounter difficulties in generalizability and replicability due to unmanageable factors related to the patient selection and data gathering procedures. The lack of arthroscopic confirmation for all patient cases was another significant factor that limited the accuracy of the radiological findings in this study. The absence of established anatomical validation techniques, including cadaver dissection, limited the investigation of the histological properties and biomechanical functions of superior synovial folds, affecting thoroughness. Sophisticated designs and anatomical verification techniques are necessary to further comprehend the clinical and biomechanical functions of these structures.
In conclusion, this study identified the incidence and morphological characteristics of superior synovial folds in the glenohumeral joint and revealed that certain types may be mistaken for pathologies. It was determined that these structures can cause anterosuperior shoulder pain, particularly in younger patients, and their accurate identification is crucial in clinical evaluations. Future research should incorporate advanced anatomical verification methods to better understand the clinical and biomechanical roles of these structures.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data that support the findings of this study are not openly available due to reasons of sensitivity of human data and are available from the corresponding author upon reasonable request.