
Abstract
Background
Cystic adventitial disease is rare and often causes stenosis or even occlusion of the corresponding blood vessels.
Purpose
To investigate the diagnostic value of color Doppler ultrasound in cystic adventitial disease.
Material and Methods
A total of 40 patients with clinically suspected cystic adventitial disease were consecutively enrolled at Shandong Provincial Hospital Affiliated to Shandong First Medical University between May 2015 and October 2023. The ultrasonographic images of cystic adventitial disease were analyzed and the ultrasonographic features were summarized. All patients underwent both ultrasound and magnetic resonance imaging (MRI). MRI findings served as a reference standard and Kappa statistic was adopted to assess the level of agreement. The sensitivity, specificity, positive and negative predictive values, accuracy, and Youden index of color Doppler ultrasound as a diagnostic tool for the diagnosis of cystic adventitial disease were assessed.
Results
Ultrasonography findings were positive in 19 patients with clinical suspicion of cystic adventitial disease. The diagnosis was confirmed by MRI in 20 patients. There was one false-positive and two false-negative by ultrasonography. The κ level of agreement between color Doppler ultrasound and MRI for the diagnosis of cystic adventitial disease was high. The κ value was 0.85. The sensitivity, specificity, positive predictive value, negative predictive value, accuracy, and Youden Index of ultrasonography were 90%, 95%, 94.7%, 90.5%, 92.5%, and 0.85, respectively.
Conclusion
Color Doppler ultrasound can effectively evaluate the ultrasound characteristic of cystic adventitial disease and provide a reliable imaging basis for its early diagnosis and treatment.
Introduction
Cystic adventitial disease (CAD) is a rare condition characterized by the formation of mucinous cyst within the adventitial layer of the blood vessels ((1–3)), typically presenting with affected limb swelling and intermittent claudication. The popliteal artery and common femoral vein are the most commonly involved arterial and venous vessels in CAD ((4,5)). CAD is usually unilateral, and predominantly occurs in young and middle-aged individuals, with a male:female ratio of approximately 5:1 ((6)). CAD often causes stenosis or even occlusion of the corresponding blood vessels, which is often misdiagnosed as atherosclerosis by computed tomography angiography (CTA) and digital subtraction angiography (DSA) when only luminal compromise is evaluated. Indeed, plain balloon angioplasty or even stent implantation may be performed with poor results compared to proper treatment of the cystic lesion. Color Doppler ultrasound and magnetic resonance imaging (MRI) not only showed the compression of blood vessels but also showed the anatomical structures surrounding these vessels, which have become the common imaging methods for diagnosing CAD. In this study, we retrospectively analyzed the clinical presentation and imaging examination data of CAD to investigate the consistency of color Doppler ultrasound and MRI in the evaluation of CAD.
Material and Methods
Between May 2015 and October 2023, 40 consecutive patients (33 males and 7 females, age range = 20–68 years; mean age = 34.6 ± 10.3years) with a clinical suspicion of CAD were retrospectively enrolled at Shandong Provincial Hospital Affiliated to Shandong First Medical University. The study was approved by the ethics committee of Shandong Provincial Hospital Affiliated to Shandong First Medical University (SWYX: NO.2023–348) with a waiver of informed consent as this was a retrospective analysis of existing clinical data. All methods were performed in accordance with the relevant guidelines and regulations. All 40 patients had no history of trauma or surgery, and all lesions were unilateral. The duration of the disease was in the range of 7 days to 4 months. Among the 40 patients, 28 experienced intermittent claudication in the affected limb, which was relieved by rest. Of these 28 patients, 12 had a claudication distance of less than 100 m and 16 had a claudication distance of approximately 200 m. Nine patients presented with swelling and pain in the affected limb, symptoms that intensified during physical activity and prolonged standing. Three patients exhibited palpable masses at the affected site.
All patients in this study underwent both color Doppler ultrasound and MRI.
The Philips Epiq7 and Canon i800 ultrasound systems with a 3–12-MHz or 4–11-MHz broadband linear array transducer were used in ultrasonography examination. A 1–5-MHz convex array probe was used for pelvic vessel (iliac artery or iliac vein) examination. Initially, the line array probe was placed on the surface of the lower extremity, and the scanning was performed from the level of the inguinal ligament to the level of the ankle joint. Continuous scanning was performed on the common femoral artery and vein, femoral artery and vein, popliteal artery and vein, and anterior and posterior tibial artery and vein to observe the course, diameter, internal echo, and blood flow signals of the vessels. Subsequently, a convex array probe was used for abdominal vascular examination. The scanning range was from the level of the abdominal aorta to the level of the groin. Continuous scanning of the iliac arteries and veins was conducted, focusing on vessel course, diameter, internal echo, and blood flow signals. When the blood vessel was narrowed by compression, the flow velocity of the vessel at the stenosis was measured and compared with the contralateral side. The angle between the acoustic beam and the direction of blood flow during spectral measurement was as low as possible (<60°). When perivascular lesions were identified, their location, size, shape, and relationship to adjacent blood vessels were assessed. Particular attention was also given to whether the lesions communicated with the adjacent joints. Surface localization was performed in patients requiring surgery.
T1-weighted (T1W), T2-weighted (T2W), fat-suppressed T1-weighted (FS-T1W), and FS-T2-weighted image (FS-T2W) imaging sequences in the coronal, sagittal, and transverse planes were obtained to visualize the location, signal, and involvement of perivascular lesions using a GE 3.0 T magnetic resonance system with a dedicated surface coil placed in the lesion location (GE Healthcare, GE Signa EXCITE HD 3.0 T, USA. Ten patients in this study received gadolinium contrast agent during the examination. Particular attention was given to the extent of CAD, the surrounding anatomic relationships, and the degree of vascular compression caused by the cyst.
All ultrasound examinations were performed by a certified ultrasound specialist with more than 10 years of experience in cardiovascular ultrasound. MRI examinations were carried out by an experienced vascular radiologist with 8 years of experience.
Ultrasound and MRI scans of the cases in the picture archiving and communication systems were all independently assessed by two radiologists with over 10 years of imaging diagnostic experience in interpreting results of ultrasonography and MRI. The original reports were shielded to avoid bias.
Statistical analysis
The SPSS program (version 25.0; IBM Corp., Armonk, NY, USA) was used for statistical analysis. The level of agreement between ultrasonography and MRI was determined by the kappa test. Sensitivity, specificity, positive and negative predictive values, accuracy, and Youden index were obtained. A P value less than 0.05 was considered statistically significant.
Results
Among 40 patients with clinically suspected CAD, MRI results were positive in 20 cases (17 men, 3 women) and negative in 20 cases. The ultrasonography diagnosis was positive in 19 patients and negative in 21 patients. In the 19 patients with a positive ultrasound diagnosis, the popliteal artery was involved in 10 cases, the common femoral artery in four cases, the external iliac artery in two cases, and the common femoral vein in three cases. Of the three cases with common femoral vein involvement, one was complicated by lower extremity venous thrombosis. MRI was used as the diagnostic criterion, there was one false-positive result and two false-negative results by ultrasonography. Two cases were diagnosed as popliteal artery entrapment syndrome by ultrasound, whereas MRI diagnosed CAD of the popliteal artery. One case was diagnosed as common femoral vein adventitial cyst by ultrasound, whereas MRI diagnosed hip synovial cyst squeezing the common femoral vein. CAD was excluded in 19 cases analyzed by ultrasound and MRI, including popliteal artery entrapment syndrome in seven cases, atherosclerotic occlusive disease in eight cases, and lower extremity venous thrombosis in four cases. Results of the comparison between MRI and ultrasonography are shown in Table 1.
Comparison of results: ultrasonography and MRI.
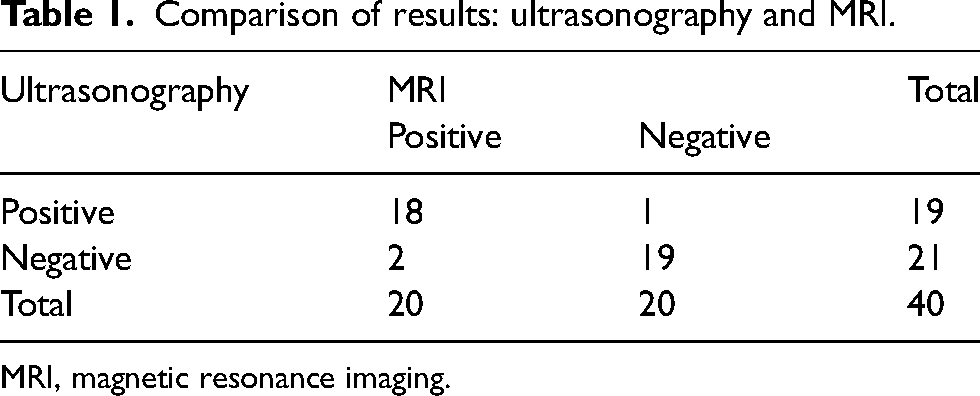
MRI, magnetic resonance imaging.
The ultrasonographic features of CAD were the cystic mass closely related to the blood vessel, with the boundary between the cystic mass and the blood vessel wall not clear. The cystic masses were generally anechoic, some of which were poorly translucent and had multiple septations. Color Doppler showed that no obvious blood flow signals in the masses (Figs. 1 and 2). The large cystic mass can squeeze the peripheral blood vessels, causing them to become narrowed by compression and the blood flow velocity to increase. MRI showed that all lesions presented low signal intensity on T1W images and high signal intensity on T2W images (Figs. 3 and 4), with enhancement of the cyst wall observed on enhanced scans.
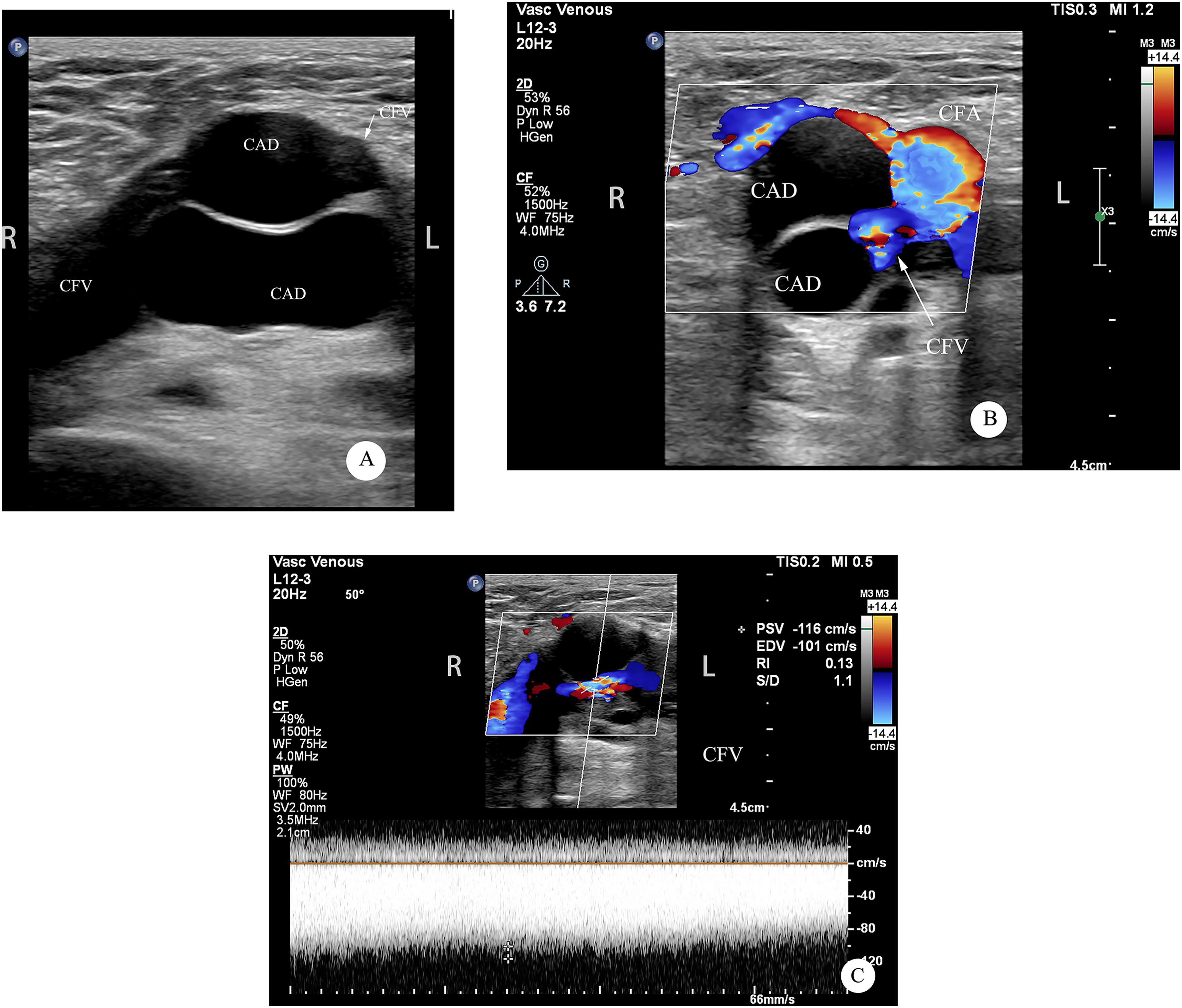
A 52-year-old male patient with a common femoral vein adventitial cyst. (a) Separation was seen in the adventitial cyst and the common femoral vein was significantly narrowed by compression. (b) The color Doppler image reveals that the common femoral vein was compressed by the adventitial cyst with a colorful mosaic change in blood flow. (c) Spectral Doppler reveals the peak systolic velocity in the common femoral vein was approximately 116 cm/s. CAD, cystic adventitial disease; CFA, common femoral artery; CFV, common femoral vein.
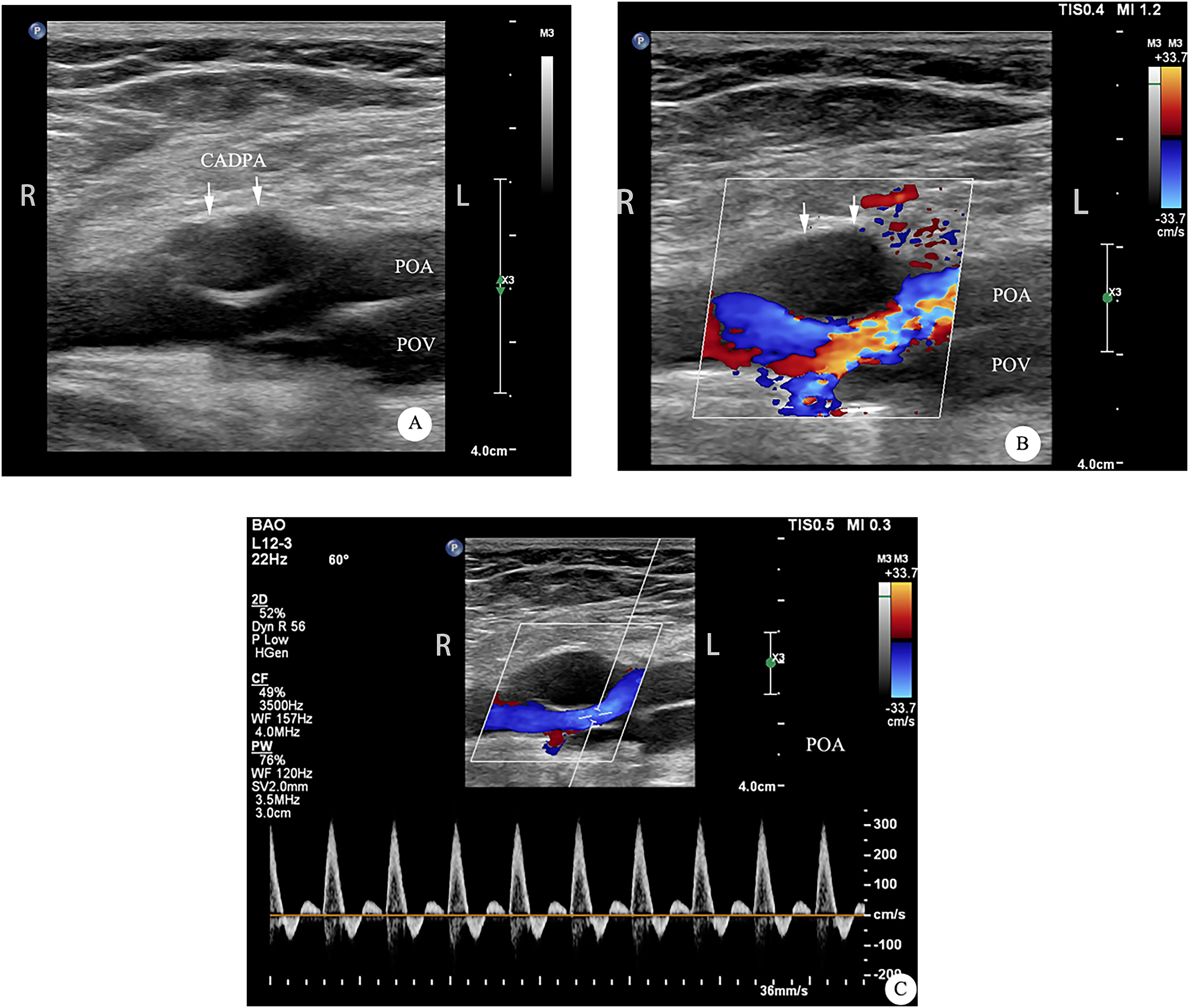
A 55-year-old male patient with a popliteal artery adventitial cyst. (a) Two-dimensional image of CADPA (white arrow). (b) The color Doppler image reveals that the popliteal artery was compressed by an adventitial cyst with a colorful mosaic change in blood flow. (c) Spectral Doppler reveals the peak systolic velocity in the popliteal artery was approximately 300 cm/s. CADPA, cystic adventitial disease of the popliteal artery; POA, popliteal artery; POV, popliteal vein.
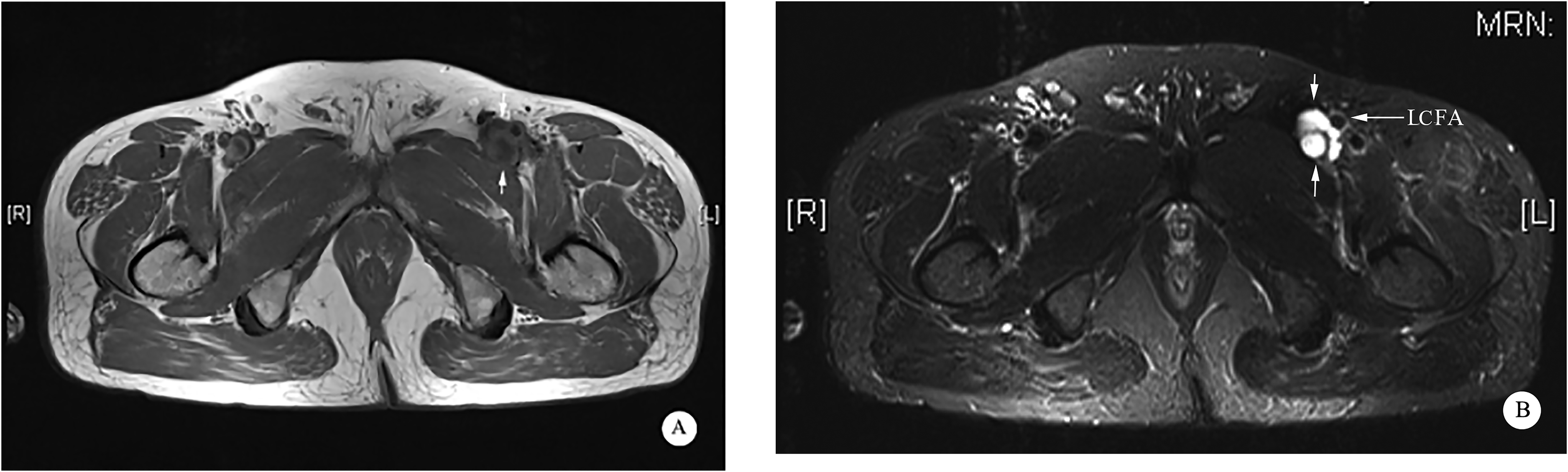
MRI of cystic adventitial disease of the common femoral vein in the same patient as Fig. 1. MRI showed that the common femoral vein adventitial cyst had low signal intensity on T1W images and high signal intensity on T2W images. There was no communication with the hip joint, no clear demarcation from the common femoral vein, and the locally compressed lumen of the common femoral vein was not clearly shown. (a) T1W images reveal the common femoral vein adventitial cyst (short arrow). (b) Fat-suppressed T2W images reveals the common femoral artery (long arrow) and the common femoral vein adventitial cyst (short arrow). MRI, magnetic resonance imaging; T1W, T1-weighted; T2W, T2-weighted.
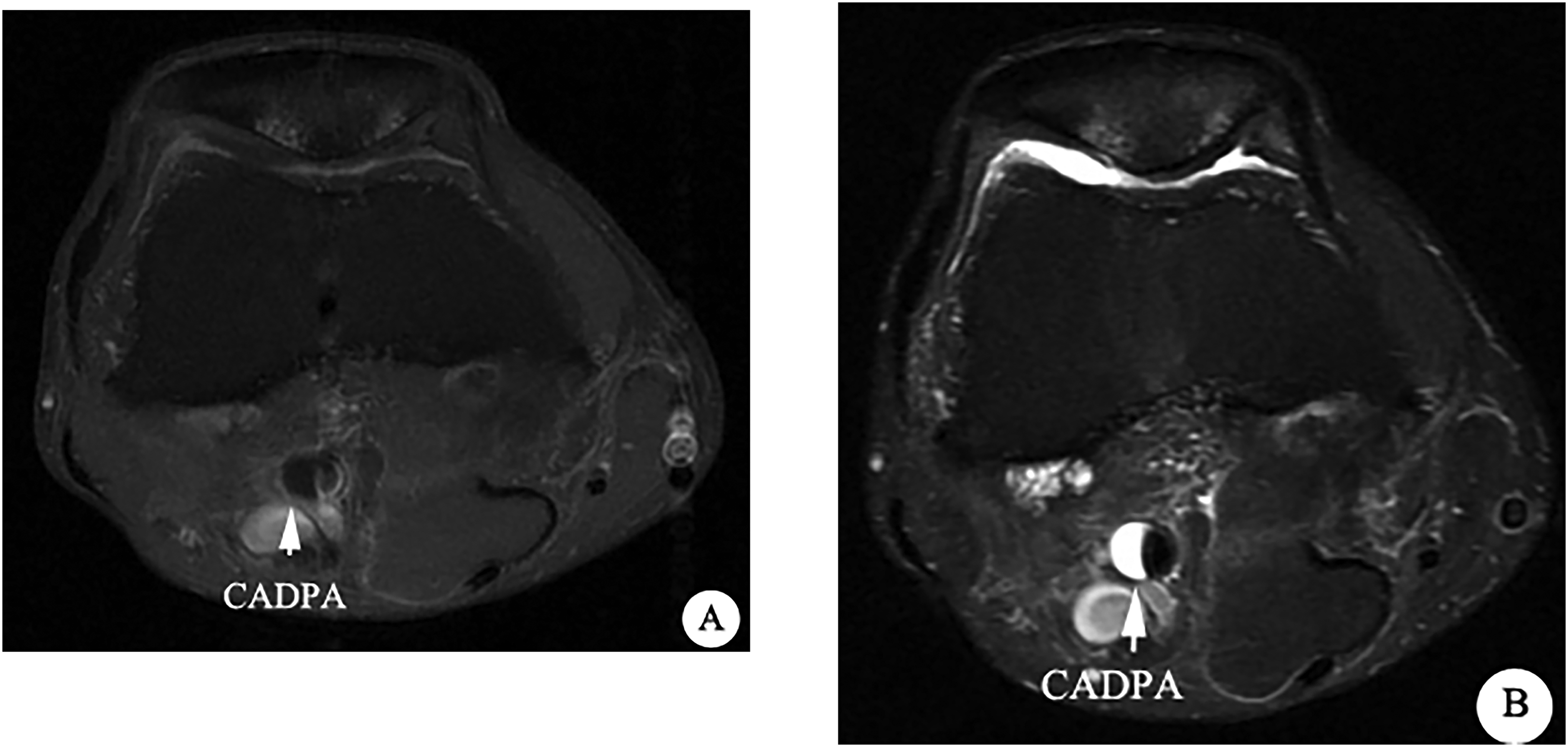
MRI of CADPA in the same patient as Fig. 2. (a) Fat-suppressed T1-weighted image; (b) fat-suppressed T2-weighted image. CADPA, cystic adventitial disease of the popliteal artery (white arrow).
Analysis of internal validity parameters of ultrasonography as a diagnostic tool for CAD showed a sensitivity of 90%, specificity of 95%, a positive predictive value of 94.7%, and a negative predictive value of 90.5%. The overall accuracy was 92.5%. The Youden index of ultrasonography was 0.85. The κ level of agreement between MRI and ultrasonography for diagnosing CAD was 0.85 (high level). A total of 16 patients underwent surgical treatment and were confirmed with adventitial cysts by postoperative pathology. Four patients were followed up because of mild symptoms.
Discussion
CAD is a rare vascular lesion. The earliest report, by Atkins and Key ((7)) in 1947, reported the first case of adventitial cyst involving the external iliac artery. The pathogenesis of CAD is not completely clear, and most scholars believe that mucin-secreting mesenchymal cells of adjacent joints enter the adventitia of blood vessels during embryonic development, leading to the formation of cysts ((8,9)). Middle-aged men were more common in this study, which is basically consistent with the literature ((10)). The general clinical manifestations of CAD are pain, swelling, and intermittent claudication of the lower limbs. Because of its atypical clinical symptoms and rarity, it is easy to be misdiagnosed and underdiagnosed. Two patients in this study were diagnosed with popliteal artery entrapment syndrome via ultrasound but confirmed as CAD of the popliteal artery by MRI. MRI accurately identified the two cases of CAD confirmed by surgery. The results demonstrated that MRI exhibited higher sensitivity than ultrasound. Therefore, in cases where ultrasound diagnosis remains inconclusive, further evaluation with MRI is recommended, particularly for the confirmation of popliteal artery entrapment syndrome. CAD is mainly differentiated from popliteal artery entrapment syndrome, para-vascular synovial cyst, and lower extremity venous thrombosis. Popliteal artery entrapment syndrome was characterized by separation between popliteal artery and vein, with abnormal muscle bundles observed in the intervening space. Notably, during plantar flexion, there was significant compression of the popliteal artery ((11)). The para-vascular synovial cyst presented as cystic masses adjacent to the blood vessel with a clear demarcation between the mass and the vessel wall; sometimes the mass was seen to communicate with the joint cavity. Lower extremity venous thrombosis manifests as solid hypoechoic filling in the venous lumen, no obvious blood flow signal was displayed, and the vessel was basically unchanged by probe compression.
At present, the diagnosis of CAD mainly depends on color Doppler ultrasound, CTA, and MRI. CTA can clearly show the relationship between blood vessels and surrounding tissues and the degree of lumen stenosis, but its application is limited by high radiation exposure and the need for contrast medium. Although MRI can clearly show the connection between adventitial cysts and adjacent joint capsules ((12,13)), its long scanning time and high cost impose certain limitations on the follow-up of CAD. Ultrasonography is an economical, non-invasive, and radiation-free examination that provides real-time dynamic visualization of vessel wall structure and perivascular anatomical relationships in multiple sections and angles, and also provides critical hemodynamic information that is not available from other examinations, which is of great clinical value for the diagnosis and follow-up of CAD.
The present study has demonstrated that ultrasound is useful in diagnosing CAD, showing high diagnostic accuracy (92.5%) compared with MRI, with a high level of agreement between the two examinations (k = 0.85). Therefore, a reliable diagnosis can be achieved in patients with typical clinical symptoms and positive ultrasound manifestations.
The present study also has some limitations. First, the ultrasound examination is unavoidably operator-dependent, which may affect the consistency of results. Second, the relationship between certain deeper vessels and the joint capsule is not clearly shown. Third, this study is a single-center retrospective study with a small sample size, which should be expanded in order to obtain more specific conclusions. The treatment of CAD should generally be selected based on the shape and location of the lesion, the degree of stenosis, and the relationship to the surrounding vessels ((14)). Excision of the cyst, ultrasound or CT-guided puncture and aspiration can relieve symptoms but are prone to recurrence. For larger cysts, multilocular cysts and severe vascular stenosis or occlusion, cyst resection and vascular reconstruction may be the best choice for the treatment of CAD ((15–17)).
In conclusion, CAD has a relatively low incidence. When a young patient has intermittent claudication or swelling of the lower limbs, the possibility of CAD should be considered. Ultrasonography could be a simple, reliable, and convenient examination method, which provides important imaging evidence for the diagnosis, treatment, and follow-up of CAD.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Shandong Province (grant no. ZR2022MH043).