
Abstract
Background
Whole-body (WB) magnetic resonance imaging (MRI) is increasingly being used in children and often includes the paranasal sinuses.
Purpose
To examine the prevalence of paranasal sinus opacifications by age and over time, as seen on WB-MRI.
Material and Methods
Prospective, population-based, bi-center study including healthy volunteers aged 6-18 years, undergoing WB-MRI (1.5 T) for research purposes only during 2018–2020, of whom 88 had a follow-up after a mean of 88 days. Paranasal sinuses and mastoid complexes were assessed separately for symmetry, presence of a nasal septal spur, bullous or inverted conchae, mucosal thickness, and presence/thickness of fluid levels. Opacification was graded on a scale of 0–3, as none/<2 mm, <33%, 33%–65%, and 66%–100% and according to the Lund–Mackay scoring system.
Results
A total of 171 volunteers (85 boys; mean age=11.9 ± 3.3 years) were included. On a 0–3 scale, 120/171 (70.2%) participants had opacification grade ≥1 in at least one paranasal sinus (67.8%) or mastoid air cell (6.4%). Corresponding findings for each sinus pair separately were 51.4% of the maxillary, 39.2% of the ethmoid, 23.4% of the sphenoid, and 4.7% of the frontal sinuses. Mean Lund–Mackay score for the initial scans was 2.85, with 47/171 (27.5%) scoring ≥4; 40.9% had a score of 0 or 1. In the majority, the grade of opacification remained stable over time.
Conclusion
The prevalence of paranasal sinus opacifications in healthy 6–18-year-olds is high, with nearly one-third having a Lund–Mackay score ≥4, which, in a clinical setting, supports a diagnosis of rhinosinusitis.
Introduction
Whole-body magnetic resonance imaging (WB-MRI) is increasingly being used in children; however, few studies have addressed its precision, accuracy and clinical validity (1). Indications range from screening in cancer predisposition syndromes, assessment of multifocal inflammatory conditions, and screening and staging of known malignant disease (2).
The paranasal sinuses are complex anatomical structures which are often included in WB-MRI and should be evaluated as part of the examination. Accurate knowledge of growth patterns and normal appearances are essential for a correct diagnosis. Several studies on development and growth of paranasal sinuses have been published (3). Mucosal swelling has been reported in up to 60% of children and adolescents undergoing computed tomography (CT) or MRI for reasons other than sinusitis or mastoiditis, and even more frequently in the younger age groups. However, these studies have a high risk of bias as most are retrospective and based on clinical populations (4–8). Moreover, few studies describe mucosal changes over time. Knowing the prevalence and extent of sinus opacifications in a general pediatric population, as well as the expected natural course of these findings, is helpful in differentiating incidental findings from disease such as chronic rhinosinusitis (CRS). This is particularly important in children, as they are less able to communicate the severity and presence of any symptoms. The aim of the present study was to examine the prevalence of paranasal sinus opacifications as seen on WB-MRI, by age and over time, in healthy volunteers aged 6–18 years.
Material and methods
This is a Regional Ethics Committee (REK-SØR ref.2016/1696) approved, prospective, population-based, bi-center WB-MRI (1,5 T) study, including healthy volunteers aged 6–18 years. The study was conducted for research purposes only, and the examinations were performed between November 2018 and February 2020. Volunteers residing in Tromsø
Sample size was estimated based on results from previous MRI studies on hands and feet in healthy individuals (9). To secure a balanced dataset for establishing normative MRI data, we stratified data sampling by sex and age. Participants were recruited via clipboard notes, announcements on social media, or by a written invitation letter by mail. Inclusion criteria were age 6–18 years and the ability to undergo a WB-MRI scan without sedation. Children with a history of systemic infectious or inflammatory disorders, cancer, metabolic diseases, ongoing infection (including upper respiratory infections such as common colds and sinus infection), medication, or trauma within the past 4 weeks or were excluded.
Image acquisition
WB-MRI was performed on a 1.5-T scanner (Philips Medical Systems, Best, the Netherlands; Intera model release 2.3 or a Magnetom Siemens Area, Siemens Healthineers Erlangen Germany, software e11c), including the following sequences: coronal T1 TSE (TR = 500 ms, TE = 5 ms, acquired voxel size = 0.9 × 0.9 × 3.5 mm), coronal T2 Dixon (TR = 5000 ms, TE = 100 ms, acquired voxel size = 0.9 × 0.9 × 3.5 mm), and coronal diffusion-weighted imaging with background suppression (DWIBS) b50 and b1000 (TR = 3000 ms, TE = 80 ms, acquired voxel size = 3 × 3 × 3.5 mm). Multiplanar reconstructions were made when deemed necessary for scoring. To examine changes over time, a follow-up WB-MRI was performed in 81 participants from Tromsø
Image analysis, paranasal sinuses
The images, including the follow-up scans, were analyzed by one out of two radiologists with more than 10 years of experience, following thorough discussions and standardization of imaging features before scoring. Equivocal findings were resolved by consensus between the two radiologists. If initial scans did not include the frontal sinuses, their development was assessed on the follow-up scan. All sinuses and mastoid complexes were evaluated separately. Symmetry was assessed on coronal images, and asymmetry was recorded as a visual estimation of >10% difference in size. Absence, presence of a nasal septal spur or bullous or inverted conchae, mucosal thickness, and/or presence and maximum thickness of fluid collections and levels (in mm) were recorded. Furthermore, the degree of sinus opacification was scored by visual assessment on a scale of 0–3 (0 = none/<2 mm, 1 = less than 33%, 2 = 33%–65%, and 3 = 66%–100%) (Figure 1). The rationale behind using this scoring system was based on previous research, demonstrating good to excellent agreement both within and between readers, for assessment of changes within a volume (9–11). In addition, cases of complete opacification were registered. Mucosal thickening, fluid, and retention cysts were scored together due to the varying signal intensities of mucus and fluid on T2-weighted (T2W) images, and difficulties in accurately separating these features on coronal images alone.
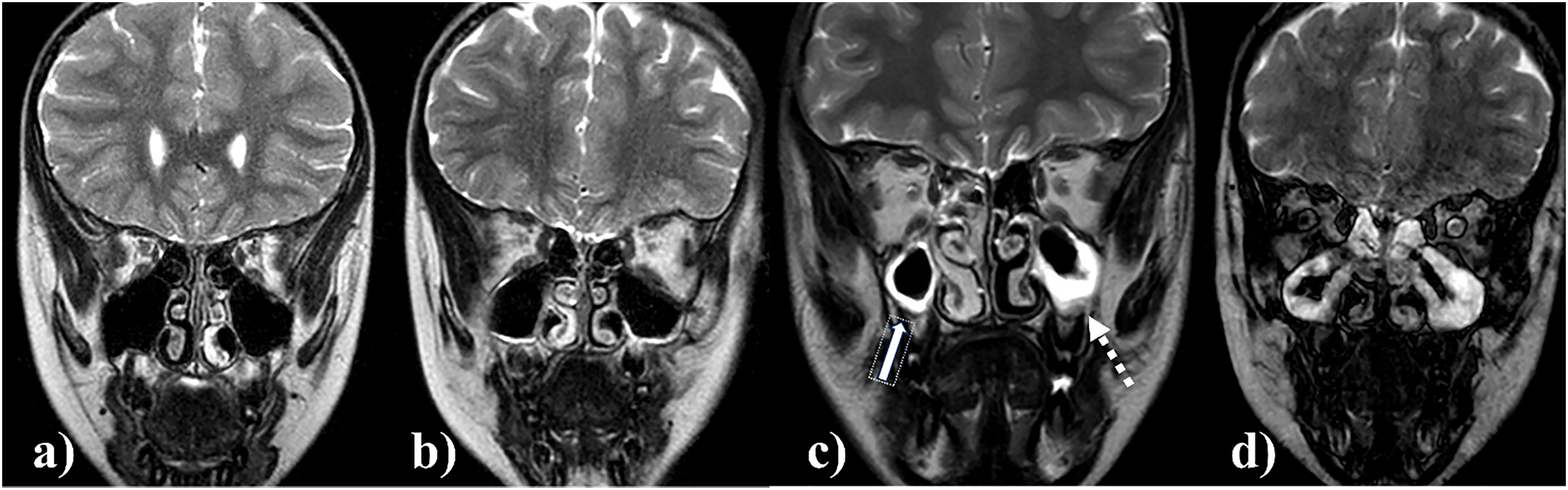
Coronal T2 Dixon in-phase images, showing maxillary opacifications on a 0–3 scale: (a, b) grade 0 = none/<2 mm; (c) grade 1 = <33% (arrow) and grade 2 = 33%–65% (dotted arrow); (d) grade 3 = 66%–100% bilaterally.
To allow for comparison with others, we also classified the sinus opacifications according to the Lund–Mackay scoring system (12). This simple, numeric scoring system was originally developed for staging rhinosinusitis on CT, and assigns each of the maxillary, frontal, sphenoid, anterior ethmoidal, and posterior ethmoidal sinuses a score: 0 = no abnormality, 1 = partial opacification, and 2 = total opacification. Moreover, the osteomeatal complex is scored as 0 (not obstructed) or 2 (obstructed). The maximum score is 24 (12). In clinical practice, the Lund–Mackay score is used to assess disease severity and treatment response in CRS and in the quantification of inflammatory disease before surgical intervention, and correlates with preoperative symptom severity (13).
Statistical analysis
Demographic characteristics are reported as count (%), mean ± SD, or range as appropriate. Change in degree of sinus opacification (category) from initial to follow-up scans are reported as count (%). Differences in the degree of opacification between cohorts from Tromsø
Results
A total of 171 volunteers (86 boys; mean age = 11.9 ± 3.3 years) were included, of whom 73 (42.7%) resided in Oslo
Development of the sinuses
In 171 (100.0%) participants, the maxillary and ethmoid sinuses, and the mastoid air cells were developed bilaterally, while 167 (100%) right and 165 (98.8%) left sphenoid sinuses were seen. Frontal sinuses were assessable in 132 participants, of which 5/132 (3.8%) were right (four aged 5–9 years and one aged 10–12 years) and 6/132 (4.6%) were left (all aged 5–9 years). Asymmetry of size was found in 81/171 (47.4%), 26/130 (20.0%), 19/171 (5.3%), and 1/171 (0.6%) of the sphenoid, frontal, maxillary, and ethmoidal sinuses, respectively.
Degree of opacification on a scale of 0–3, by location
The degree of opacification by location is listed in Table 1. Of the 171 participants, 120 (70.2%) had a grade 1 or more in at least one of the paranasal sinuses (67.8%) or mastoid air cells (6.4%). The corresponding findings when evaluating each sinus pair separately were 51.4% of the maxillary, 39.2% of the ethmoid, 23.4% of the sphenoid, and 4.7% of the frontal sinuses (Table 1).
Degree of opacification of the different sinuses and mastoid complexes in 171 children aged 6–18 years undergoing WB-MRI for research purposes only.
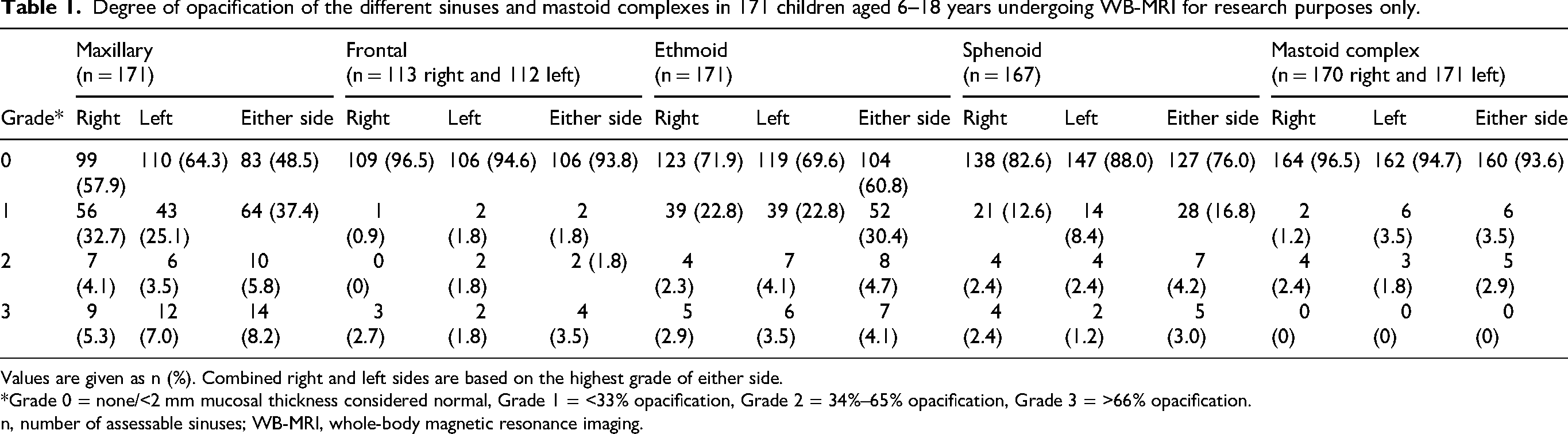
Values are given as n (%). Combined right and left sides are based on the highest grade of either side.
*Grade 0 = none/<2 mm mucosal thickness considered normal, Grade 1 = <33% opacification, Grade 2 = 34%–65% opacification, Grade 3 = >66% opacification.
n, number of assessable sinuses; WB-MRI, whole-body magnetic resonance imaging.
There were no statistically significant differences in the presence of grade ≥1 opacification between sinuses, according to sex, age group, season, or study site (latitude), with one exception; the odds for having opacified left ethmoids were higher among participants from Tromsø
Degree of opacification using the Lund–Mackay score, by location
The mean Lund–Mackay score for the initial scans was 2.85 ± 3.36, with 47 (27.5%) participants scoring ≥4. Of the 171 participants, 70 (40.9%) had a score of 1 or 0 (range = 0–19). When subgrouping the participants based on mucosal thickness according to previously suggested thresholds, 51.4% of participants would be considered to have at least one pathological maxillary sinus when using ≥2 mm as threshold, 35.0% when using ≥3 mm, and 28.7% when using ≥4 mm (Table 2).
A total of 171 children aged 6–18 years undergoing WB-MRI for research purposes only.
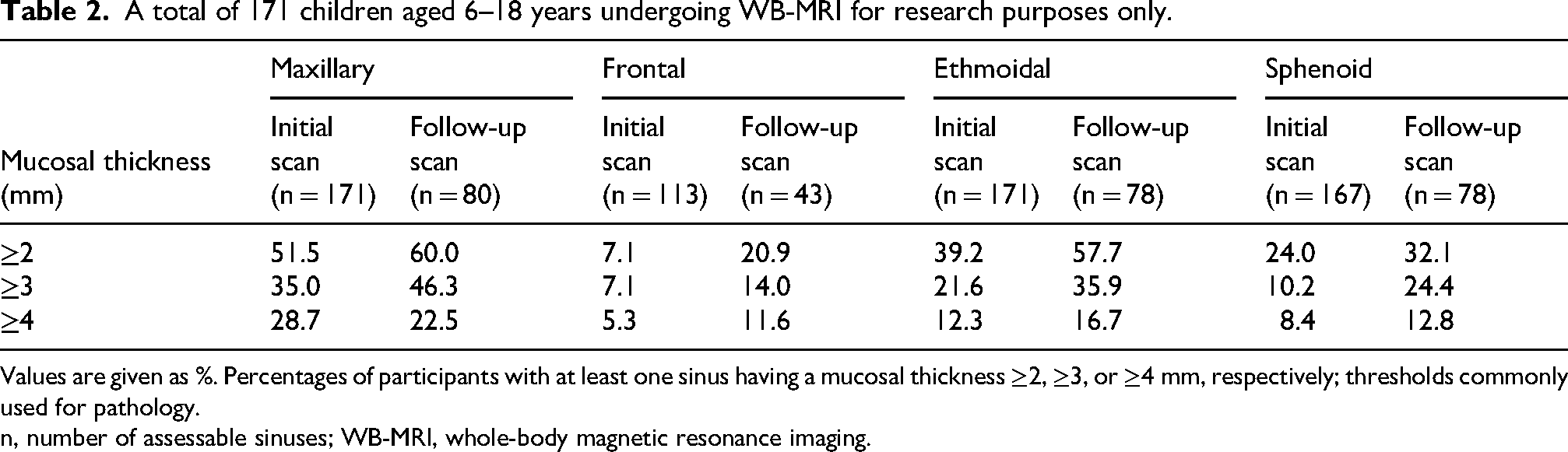
Values are given as %. Percentages of participants with at least one sinus having a mucosal thickness ≥2, ≥3, or ≥4 mm, respectively; thresholds commonly used for pathology.
n, number of assessable sinuses; WB-MRI, whole-body magnetic resonance imaging.
Degree of opacification on a scale of 0–3, on follow-up, by location
Follow-up was performed after a mean of 88 days (range = 9–182 days). The degree of opacification remained unchanged in 61.3% of the right maxillary and 63.7% of the left maxillary sinuses, whereas an increase was seen in 21.3% of right and 22.5% of left maxillary sinuses (Table 3, Figures 2–4).
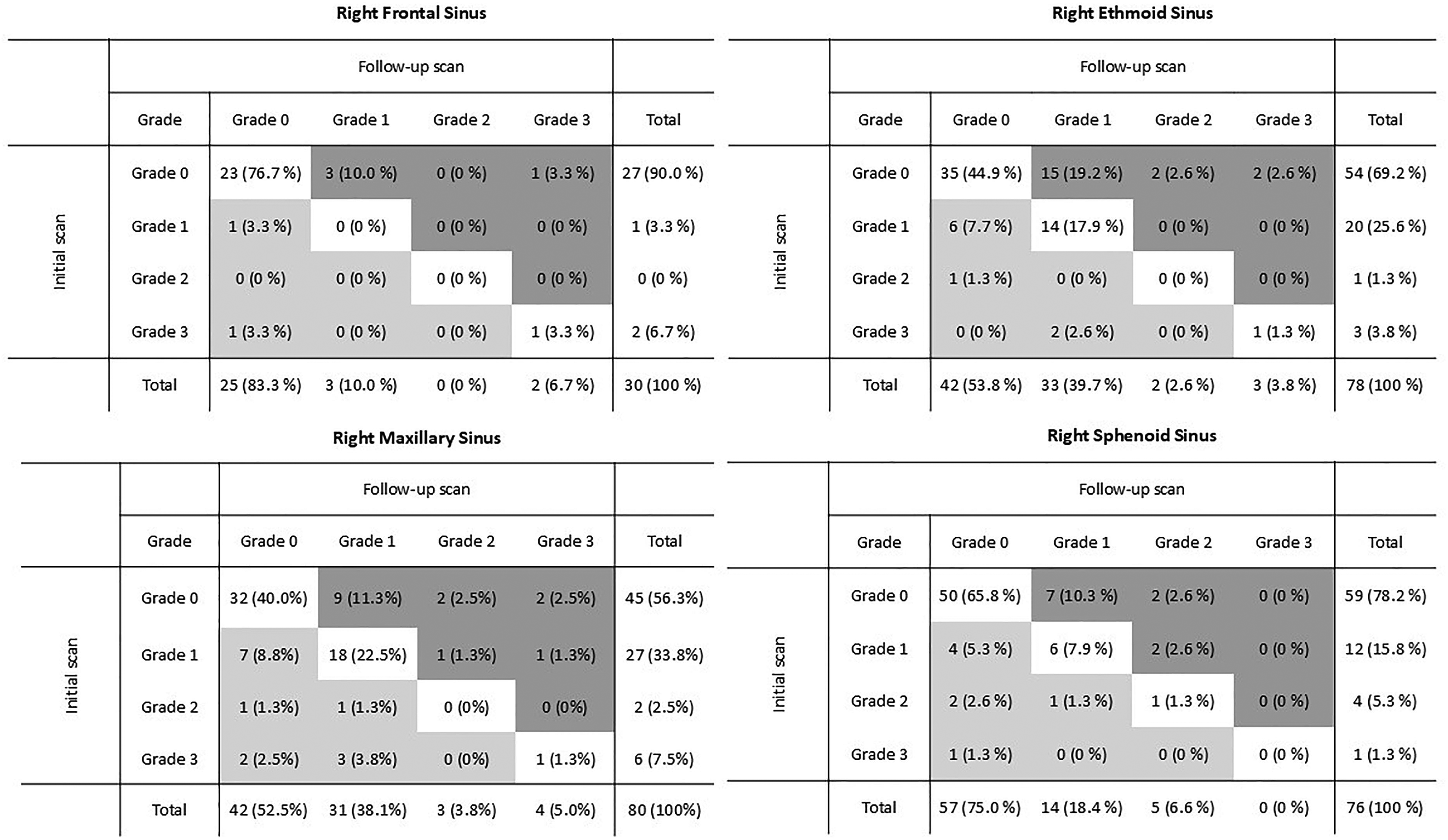
The degree of opacification of the right sinuses and its category change at follow-up. Grade 0 = none or <2 mm mucosal thickness. Grade 1 = <33% opacification. Grade 2 = 33%–65% opacification. Grade 3 = 66%–100% opacification. The darker shade indicates increase of category, while the lighter indicates decrease of category. No shading indicates no change of category.
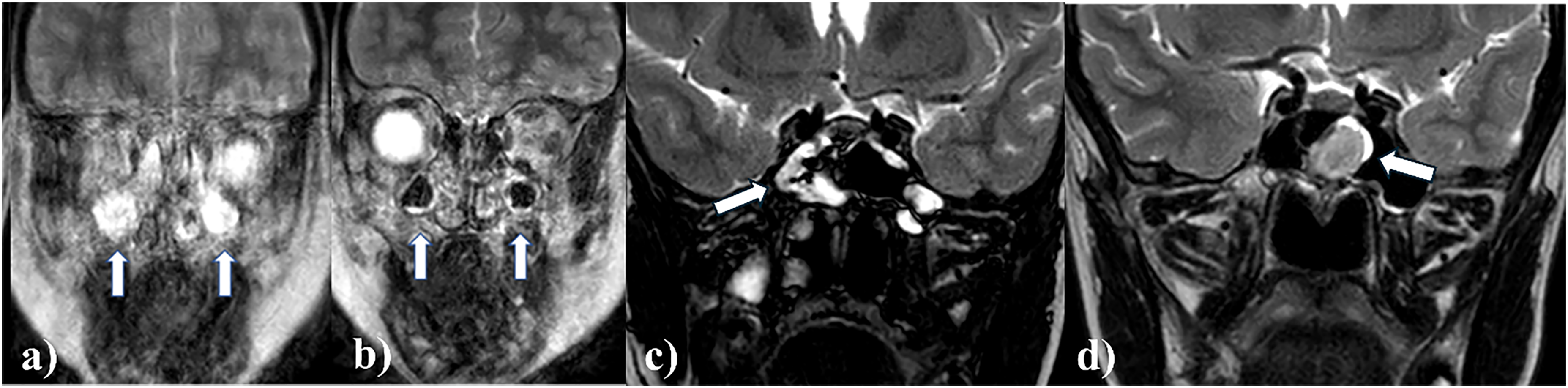
Coronal T2 Dixon in-phase images showing two examples of change between scans. (a) A 6-year-old boy with complete opacification of the maxillary sinuses (arrows), with (b) almost complete resolution at follow-up 9 days later (arrows). (c) A 13-year-old boy with irregular mucosal thickening and fluid pockets in the sphenoid sinuses on the initial scan, most prominent on the right side (arrow) and (d) showing a shift of opacification to the left side (arrow) on the follow-up scan 4 months later.
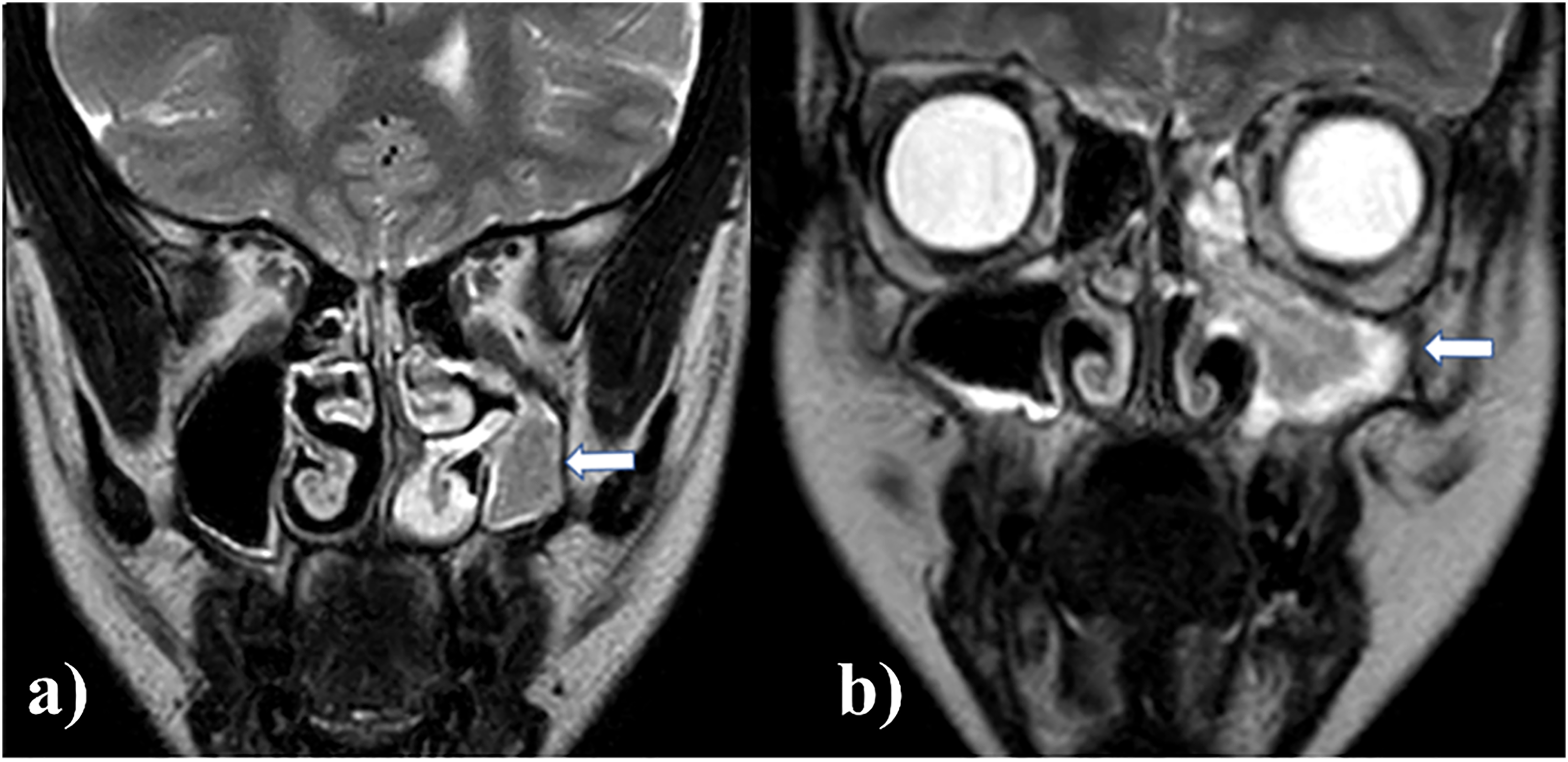
Coronal T2 Dixon in-phase images of (a) marked asymmetrical development of the maxillary sinuses with opacification of the underdeveloped left side (arrow) in a 13-year-old girl, and (b) complete opacification of the left maxillary sinus (arrow) with remodeling and widening of the osteomeatal complex and protrusion of fluid in the nasal cavity in a 9-year-old girl.
Summary of change in opacification grade category at follow-up (data from 81/171 children aged 6–18 years, undergoing WB-MRI for research purposes only).
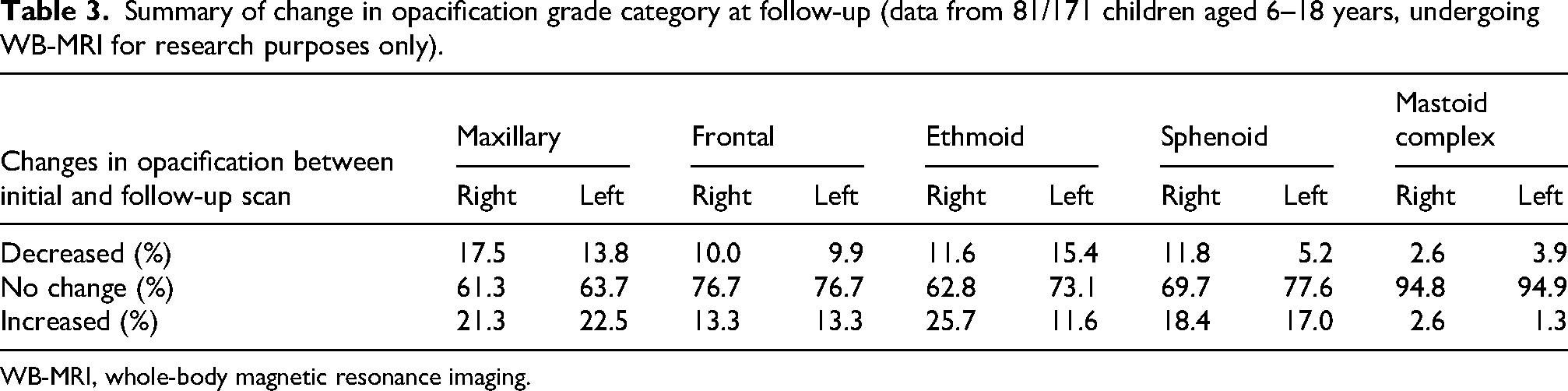
WB-MRI, whole-body magnetic resonance imaging.
Miscellaneous findings
A nasal septal spur was present in 23/169 (13.6%) participants, of which 9/169 (5.3%) were right-sided and 14/169 (8.3%) were left-sided. Aeration of the turbinates was seen in 38/169 (22.5%) right and 27/169 (16.0%) left conchae media. One concha bullosa (left, superior) was seen (Figure 5).
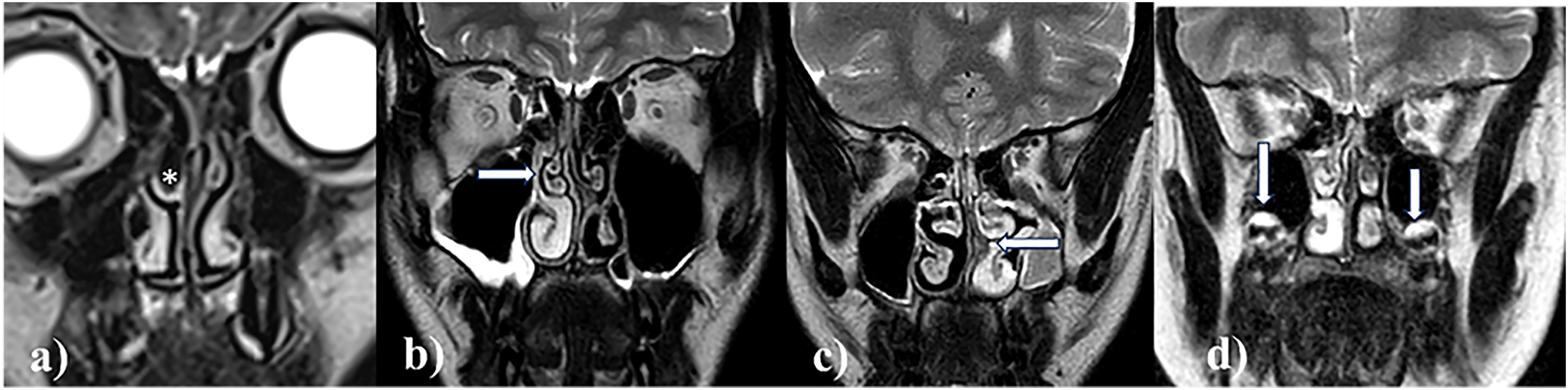
Coronal T2 Dixon in-phase images, showing (a) a right middle concha bullosa (asterisk) in a 10-year-old girl, (b) right maxillary mucosal thickening (grade 1) and an inverted right concha media (arrow) in a 15-year-old boy, (c) asymmetrically developed maxillary sinuses with complete opacification of the underdeveloped left side and a nasal septal spur (arrow) in a 13-year-old girl, and (d) high signal intensity adjacent to the floor of both maxillary sinuses (arrows) representing cartilage of developing molars in a 10-year-old girl.
Discussion
We have shown, in a large, population-based cohort of healthy children and adolescents, that nearly one in ten has a high degree of maxillary sinus opacification and this was stable over time. The degree of opacification did not differ significantly according to age group, sex, season, or latitude, with one exception; opacification of the ethmoids was more common among those residing in the northern part of the country compared to the southerners. The mean Lund–Mackay score was 2.85, with nearly one-third of participants having a score ≥4, which, in a clinical setting is suggestive of rhinosinusitis (16). Of the 171 participants, only 40.0% had a score considered normal according to commonly used threshold values.
To the best of our knowledge, this is the largest population-based study of healthy volunteers evaluating mucosal changes of the paranasal sinuses over time. Our findings are in line with those of Kristo et al. in a smaller study of 24 children aged 8–9 years, of whom 19 were asymptomatic and 18 had a follow-up examination after 6–7 months (6). Half of their participants, including 42% of those without symptoms, had some “abnormality,” 42% involving the maxillary sinuses and 38% the ethmoids (6). At follow-up, 63% of the maxillary and 42% of ethmoid sinuses had resolved (6), in contrast to our results where the majority of findings remained after a mean interval of 88 days. The use of different cutoff values (>3 mm vs. ≥2 mm) may explain this discrepancy, as well as the inclusion of symptomatic participants in the study by Kristo et al.
In another MRI-based study of 147 patients aged under 22 years undergoing MRI of the head for reasons other than sinusitis or mastoiditis, von Kalle et al. found that >60% of the children had at least one salient finding in the paranasal sinuses or mastoid cells, nearly half had mucosal swelling of the paranasal sinuses, and one-fourth of the mastoid cells (7). For comparison, we found that approximately 70% had a noteworthy finding in at least one of the paranasal sinuses or mastoid complexes, with nearly 68% having paranasal sinus opacifications and 6% having mastoid air cell findings. The differences may be due to different cohorts and definitions used for significant findings. Contrasting our results, von Kalle et al. reported a higher prevalence of salient findings in children aged under 10 years, with no associations to place of residence (7). In our study, ethmoidal opacifications were four times more common among participants residing up north, at 69°F, compared to those residing within a temperate climate zone. Colder climate in itself might cause mucosal swelling of the nasal cavity and ethmoids, explaining part of the difference. Underreporting of allergies is another potential explanation, although no seasonal variation was seen to support this. Further, none of the participants used medication, including antihistamines.
Lack of established thresholds for normal and most likely pathological mucosal thickness in children and adults has been addressed by several authors (4–7,15–18). A study by Gordts et al. on CRS including 100 children aged 1 month to 15 years suggested a threshold of 3 mm based on MRI (4). Others have suggested a 2-mm threshold (15), which, if applied to our cohort, would have resulted in a high total of 51.4% having at least one pathological maxillary sinus, decreasing to 35% and 28.7% when using a threshold of ≥3 mm and ≥4 mm, respectively. This is intriguing, as all our participants were healthy, without any history of systemic infectious or inflammatory disorders, cancer, or metabolic diseases, nor any ongoing infections, including common colds or sinusitis, or trauma in the 4 weeks before WB-MRI, which was undertaken for research purposes only.
In clinical practice, rhinosinusitis is diagnosed based on history, symptoms, and clinical and imaging findings. Most studies addressing the paranasal sinuses are CT-based, providing high-resolution images of bony structures such as the mastoid complex and the thin bones separating the dental structures and the sinuses (19). With MRI, these structures are not as clearly visualized. However, soft tissues are better delineated, as is cartilage and the developing tooth buds of permanent dentition, shown with high intensity on T2W images, and not to be mistaken for mucosal thickening or fluid in the maxillary sinuses.
The CT-based Lund–Mackay scoring system has been used for decades to evaluate disease severity and treatment response of CRS before surgical intervention (13). Bhattacharyya et al. have previously suggested that a Lund–Mackay score of 0 or 1 is unlikely to represent CRS and should be considered normal or “negative” (16). They considered scores ≥4 to be indicative of CRS, while a score of 2 or 3 was equivocal (16, 17). In 2004, Hill et al. reported a mean incidental Lund–Mackay score of 2.8, based on 324 CT scans of the brain, sinuses, or temporal bones in patients aged 1–18 years (17). This is consistent with our findings. We acknowledge that the Lund–Mackay scoring system was originally designed for CT. However, research indicates that MRI staging, using the same CT-based system, correlates well with CT findings for sinonasal disease (20,21). In contrast to a dedicated, multiplane MR examination and a CRS MRI score, the present WB-MRI study provided coronal images only. We therefore considered the relatively simple Lund–Mackay score the best fit for comparative analysis.
As for MRI-based studies, a report by Lim et al., including 122 patients aged ≤16 years visiting the clinic for other reasons than upper airway infection, found a mean Lund–Mackay score of 1.28, using a cutoff of 2 mm between normal and “pathological” mucosal thickness (5).
Finally, a systematic review and meta-analysis from 2021 by Razi et al. including both CT- and MRI-based studies using the Lund–Mackay scoring system found a mean score of 1.74 in an asymptomatic pediatric subgroup. In three studies not included in the meta-analysis, the mean score was 1.23. The most commonly used definition of maxillary sinus thickening in the literature was ≥2 mm (mixed adult and pediatric population) (15).
Based on this threshold, only 40% of our healthy cohort had a Lund–Mackay score considered true negative or normal (score of 0 or 1), while nearly 30% had a score of ≥4, which, in a clinical setting, would have indicated rhinosinusitis. This underscores the importance of combining history and clinical and imaging findings when assessing patients for potential rhinosinusitis and not relying solely on imaging.
The strengths of our study are the prospective, population-based design, the large number of healthy volunteers, and the thorough scoring of the images. Moreover, efforts were made to ensure that there were no underlying pathological conditions, both in terms of follow-up interviews and imaging.
The present study has some limitations. First, there is an inherent subjective nature of the scoring process, although the scale of 0–3 (scale of thirds) used for visual estimation of volumes has performed well in similar studies (9), thus, intra- and inter-observer variation was not performed. Second, the MRI protocol was not designed to evaluate the paranasal sinuses specifically, thus, a targeted examination might have altered the results to some extent, particularly for the ethmoids and osteomeatal complexes. Third, the follow-up interval varied, with a mean of 88 days according to MRI availability, which is relatively short for assessing stability of sinus findings. Lastly, screening of participants consisted of a self-reporting questionnaire and did not include any clinical examination.
In conclusion, the prevalence of paranasal sinus opacification is high in healthy children and adolescents with no history or symptoms of an upper airway infection, with no differences according to sex or age group. Our findings underscore the importance of symptoms and clinical findings for the diagnosis of acute rhinosinusitis.
Footnotes
Acknowledgments
We want to thank the participants and their care givers for their contribution.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has received funding by the Northern Norway Regional Health Authority (grant no. HNF 1666-23).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.