
Abstract
Background
Imaging is crucial for the detection of pancreatic diseases. Photon-counting computed tomography (PCCT) is a recent improvement in CT detector technology that may improve pancreatic imaging quality.
Purpose
To compare the image quality in pancreatic imaging with PCCT versus conventional CT (EIDCT) both subjectively and quantitatively.
Material and Methods
We retrospectively identified 35 patients scanned with both EIDCT and PCCT in multiple contrast phases. Image quality over 11 peripancreatic areas was rated on a 5-point Likert scale. One reader made quantitative measurements of density and noise. Data analysis was performed using R Studio. Continuous data were compared using a paired t-test and ordinal data with a Wilcoxon signed-rank test.
Results
Image quality was rated significantly higher on PCCT for the pancreatic parenchyma in the late arterial phase (3.87 vs. 2.77; P <0.01), the pancreatic parenchyma in the portal venous phase (3.31 vs. 2.53; P <0.01), pancreatic ducts (2.88 vs. 2.62; P <0.01), superior mesenteric artery (4.10 vs. 2.74; P <0.01), coeliac axis (4.04 vs. 2.70; P <0.01), and portal vein (3.29 vs. 2.52; P <0.01). Noise levels were significantly lower with PCCT with a mean reduction of 5.8 HU across all areas. Dose-length-product was significantly reduced in both the late arterial phase (31.8%; P <0.01) and the portal venous phase (21.5%; P <0.01).
Conclusion
Image quality was subjectively and quantitatively significantly improved for all evaluated pancreatic and peripancreatic structures with PCCT compared to EIDCT. In addition, radiation dose was significantly reduced.
Introduction
Computed tomography (CT) is the preferred imaging modality for the visualization of many pancreatic diseases such as cancer (1). Radiologists struggle to detect small pancreatic cancer lesions before they have progressed to invasion into nearby vessels, organs, or metastatic disease (2). Suboptimal image quality is very likely one of the reasons for this. A historical systematic review from 2006 even found that conventional CT to be universally inferior to endoscopic ultrasound in detecting pancreatic cancer (3). However, the standard of care/diagnosis for a patient suspected of having pancreatic cancer remains a CT scan with multiple contrast phases: typically, a late-arterial contrast-enhanced phase (LA) of the upper abdomen and a portal-venous phase (PV) of the thorax and abdomen.
Since 2006, CT technology has undergone substantial improvements, reducing both scan time and dose while increasing spatial resolution. However, conventional CT approaches its technological limits regarding improving spatial resolution without a considerable dose penalty and potential reductions in the dose of ionizing radiation without severely affecting image quality (4). Conventional CT, including both single-energy and dual-energy CT, uses a scintillator layer to convert X-ray photons into visible light that can be measured by a photodiode. This two-step detector procedure leads to unavoidable signal loss and integration of the various energy levels of the detected X-ray photons (4,5). Hence conventional CT is also called energy-integrating detector CT (EIDCT). The newest generation of CT scanners, called photon-counting detector CT (PCCT), incorporates a semi-conductor layer that can directly convert X-ray photons into electric signals. This method has several advantages and has the potential to further elevate the role of CT in the imaging of pancreatic lesions. A recently published paper has shown the extent to which the previously unseen details of pancreatic microanatomy can be visualized with an optimized PCCT protocol (6). Several groups have demonstrated an increased conspicuity of pancreatic lesions (7–9), and the new detector design also leads to lowered dose of ionizing radiation (10,11). Several reports showed significant reductions in image noise within the thoracic and abdominal areas; however, none have focused on comparing PCCT with EIDCT in the pancreatic area of the same patient.
The aim of the present study was to comprehensively compare the subjective and quantitative image quality between PCCT and EIDCT for the pancreas and important peripancreatic structures.
Material and Methods
General design
The study was approved by the national ethical committee NVK-2530757. We conducted a retrospective study to compare the diagnostic quality difference between PCCT and EIDCT in pancreatic imaging. During the experiment and blinded to the type of CT, four board-certified radiologists read both PCCT and EIDCT images of 35 patients scanned twice. The diagnostic image quality was assessed both subjectively and quantitatively.
Patient population
We analyzed patient records between 1 June 2021 and 1 December 2023 and identified 103 patients who underwent both high-end EIDCT and PCCT scans, imaged with both an LA and PV contrast phase. This included patients under suspicion/follow-up of suspected/confirmed pancreatic cancer or renal cell carcinoma (RCC). From the 103 eligible patients, we excluded 17 patients with obvious pathology in the pancreas, six patients with previous surgery of the pancreas, and 45 patients with insufficient pancreatic enhancement in the arterial phase (i.e. an early pancreatic phase, defined in our setting as a pancreatic attenuation <100 HU) (12). The final study population comprised 35 patients scanned twice in the context of follow-up of cancer or suspected cancer (Fig. 1 and Table 1 for demographics and scan characteristics).
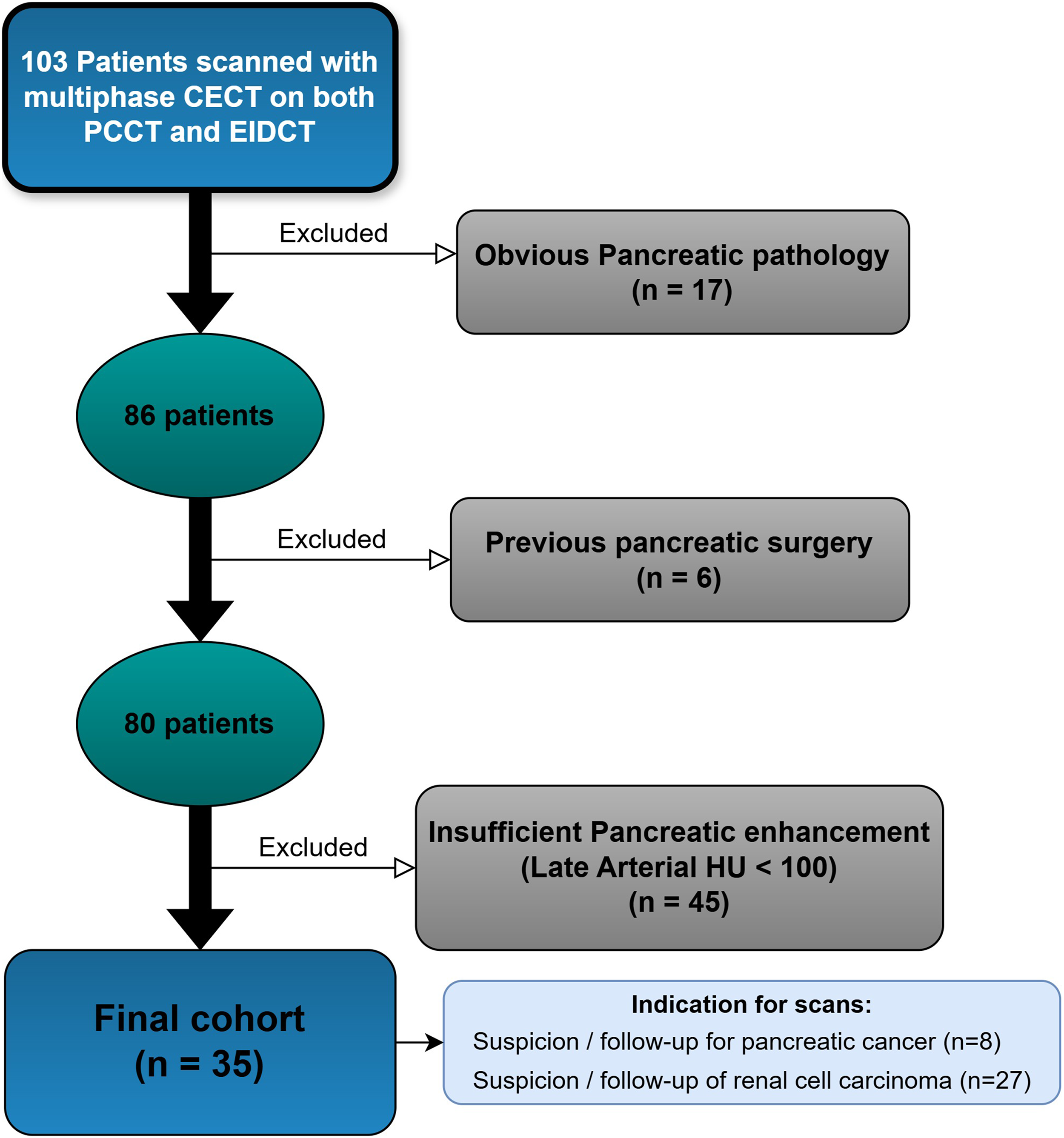
Flowchart of patient inclusion and exclusion.
Patient demographics and scan characteristics.
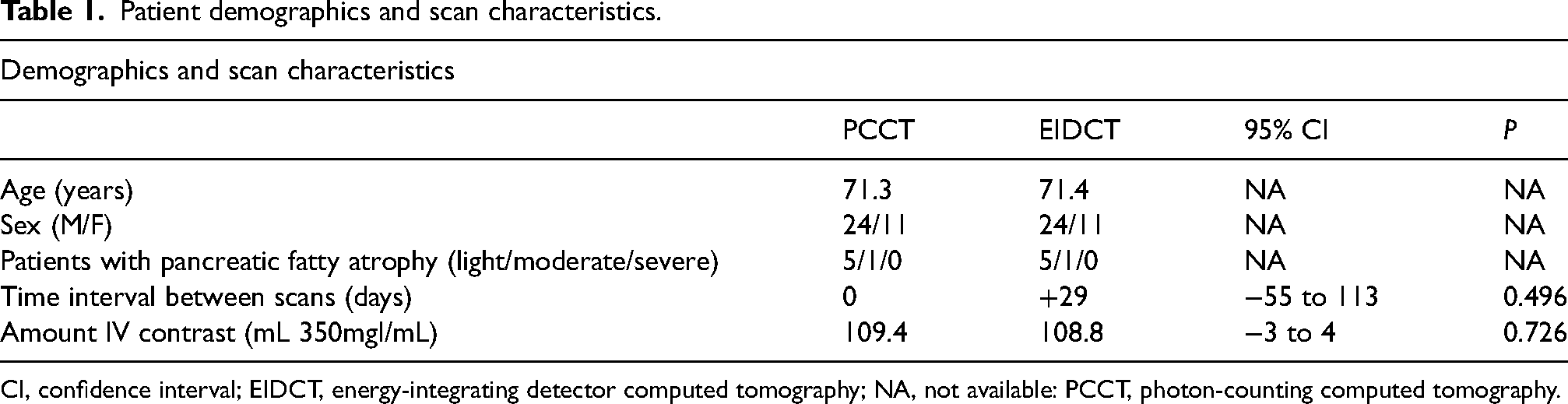
CI, confidence interval; EIDCT, energy-integrating detector computed tomography; NA, not available: PCCT, photon-counting computed tomography.
CT protocol
Standard CT protocols for a multiphase contrast-enhanced scan of the upper abdomen were used for all scanners (Table 2). Intravenous contrast (350 mg I/mL) was administered based on the patient's body weight (1.5 mL/kg). Region of interest (ROI) tracking was used for all scanners. However, an unintended difference in the timing of the contrast between the EIDCT and PCCT protocols was discovered. This difference was likely caused by a human error in lack of homogenization between CT scanners from different vendors after merging similar CT protocols. The EIDCT protocols had the intended 18-s delay after a ROI of 100 HU in the abdominal aorta, whereas PCCT had an unintendedly early 15-s delay. This led to a relatively high number of excluded patients due to insufficient pancreatic enhancement.
Table of CT protocol specifications.
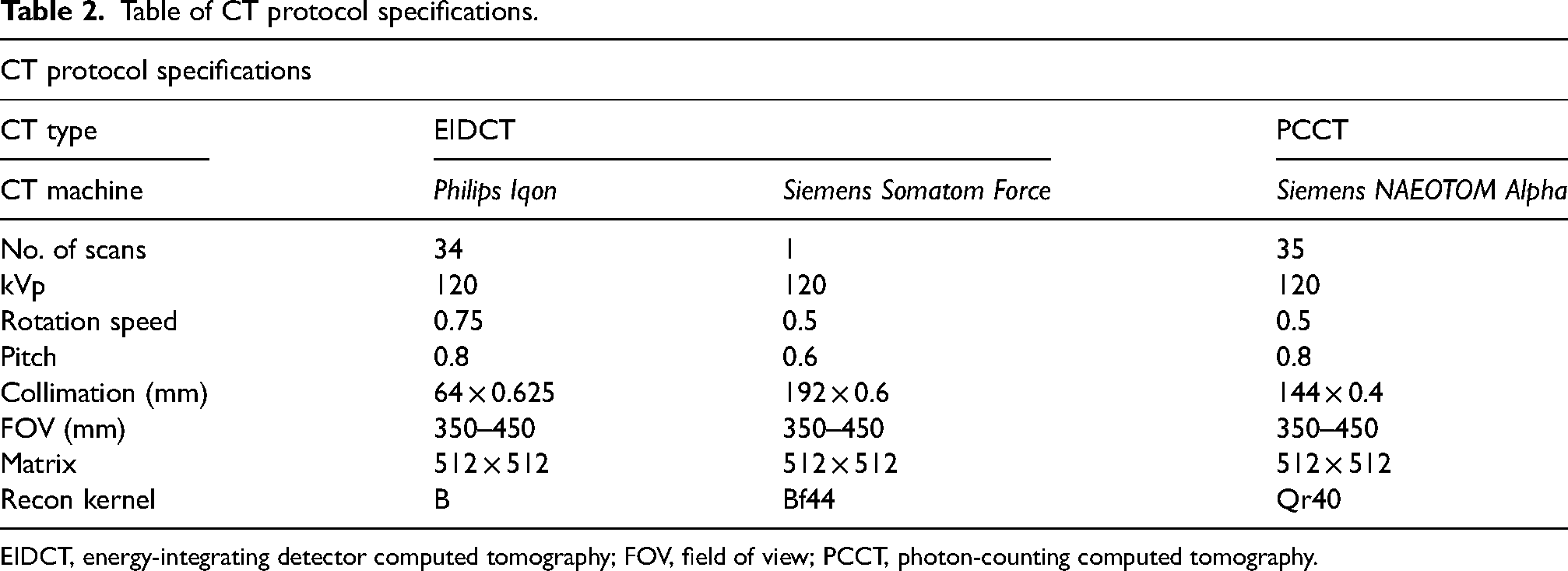
EIDCT, energy-integrating detector computed tomography; FOV, field of view; PCCT, photon-counting computed tomography.
Image analysis
Three abdominal radiology consultants and one oncological radiology consultant reviewed the CT scans (with experience in the range of 16–30 years). Each reader independently reviewed all PCCT and EIDCT scans, while blinded to the type of CT scan. Readings were arranged in two sessions with 35 readings in each. In each reading, half of the scans were PCCT and the other half were EIDCT. These were presented to the readers in a random order. Readers had a minimum of a 4-week washout period between readings. The readers independently evaluated 11 different pancreatic or peripancreatic structures. The evaluated structures were as follows: the pancreatic parenchyma (both for LA and PV), the main pancreatic duct (MPD) in the head (both for LA and PV), body (both LA and PV), tail (both LA and PV), the coeliac axis (LA), the superior mesenteric artery (LA), and the portal vein/superior mesenteric vein (PV). Readers were instructed to zoom in on the area to be assessed and evaluate image quality on a 5-point Likert scale (1 = non-diagnostic/insufficient, 2 = suboptimal, 3 = acceptable, 4 = good, 5 = excellent). The readers were given a chart of the Likert scale with text and image examples of each step of the scale for each of the 11 parameters (see supplementary material).
In addition, one reader performed quantitative measurements of density and noise in nine different pancreatic and peripancreatic areas (Fig. 2). These were performed by placing ROIs as large as possible in homogenous areas. The Hounsfield value and the standard deviation (SD) were then registered. We opted to use SD as a measurement of noise (instead of signal:noise ratio or contrast:noise ratio [CNR]) since we wished to get one universal measurement of noise in the image. The dose length product for the LA and PV and the amount of IV contrast was recorded.
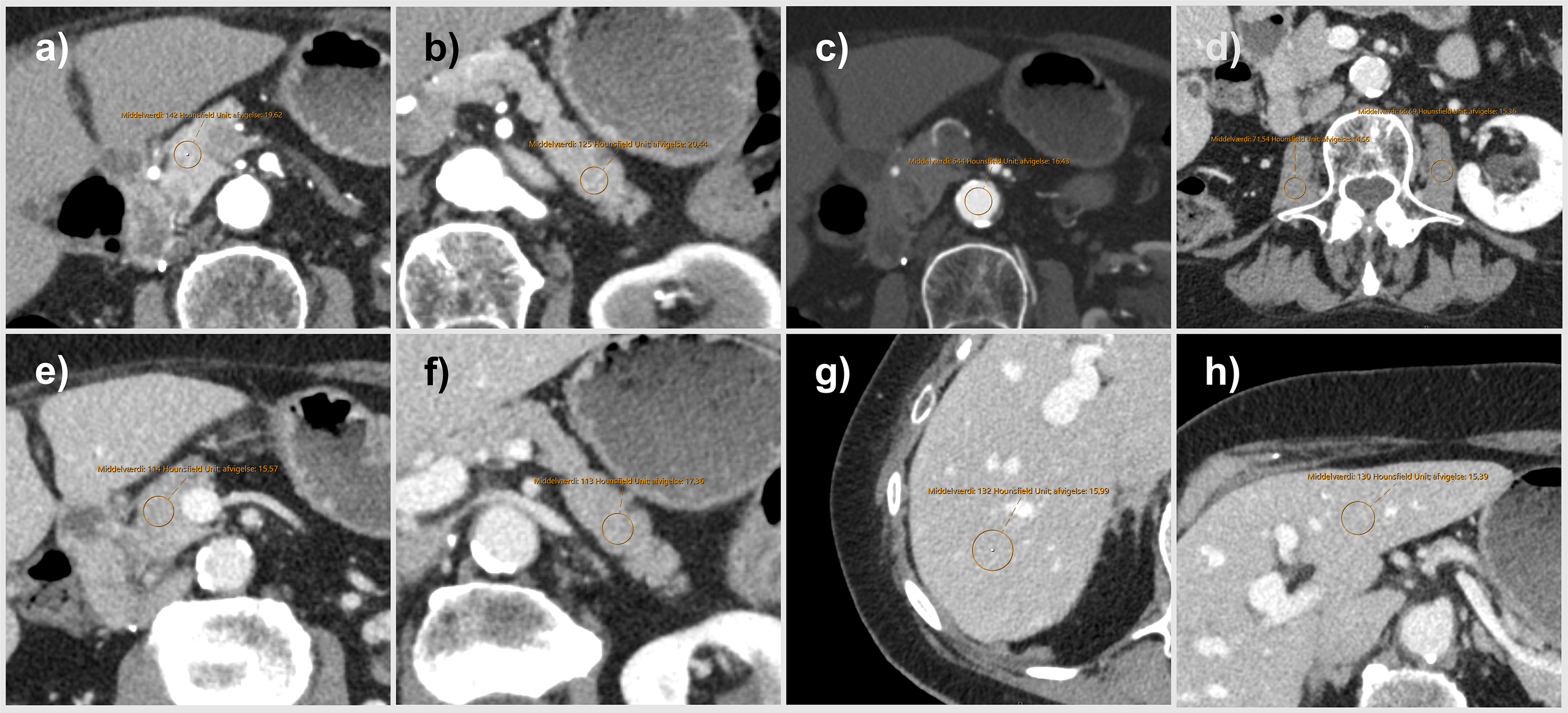
Depiction of the nine different measured for the quantitative analysis with a region of interest. (a–c) Images in the late arterial phase, while the remaining are measurements in the portal venous phase. (a, e) The head of the pancreas. (b, f) The tail of the pancreas. (c) Measurement of the aorta at the L3 level. (d) The psoas muscles at the L3 level. (g, h) Measurements in the right and left hepatic lobes.
Statistical analysis
All data analysis was performed with R Studio, version 2022.07.1. A power analysis was based on a test reading of 15 initial patients by a single reader and set the power level at 0.80 and the significance level at 0.05. We used a boot-strapping method of a Wilcoxon ranked-sum test and the necessary sample size was estimated to be approximately 30 patients to prove a difference of 0.5 points on the Likert scale. From the initial test reading we expected a difference of 0.5 points in favor of PCCT on all our Likert scales. Continuous parameters were compared using a paired t-test, and mean image quality ratings were compared using a Wilcoxon signed-rank test. Inter-reader agreement was analyzed using Cohen's kappa with a squared weighting scheme for ordinal data. Subgroup analysis was performed for the most frequent type of EIDCT by excluding results from the other type of EIDCT. The significance level was set at P <0.05.
Results
Subjective parameters
Image ratings are presented as the mean of all four readers (see Table 3 for all mean and individual reader ratings). Image quality was rated significantly higher on PCCT for the pancreatic parenchyma in the LA
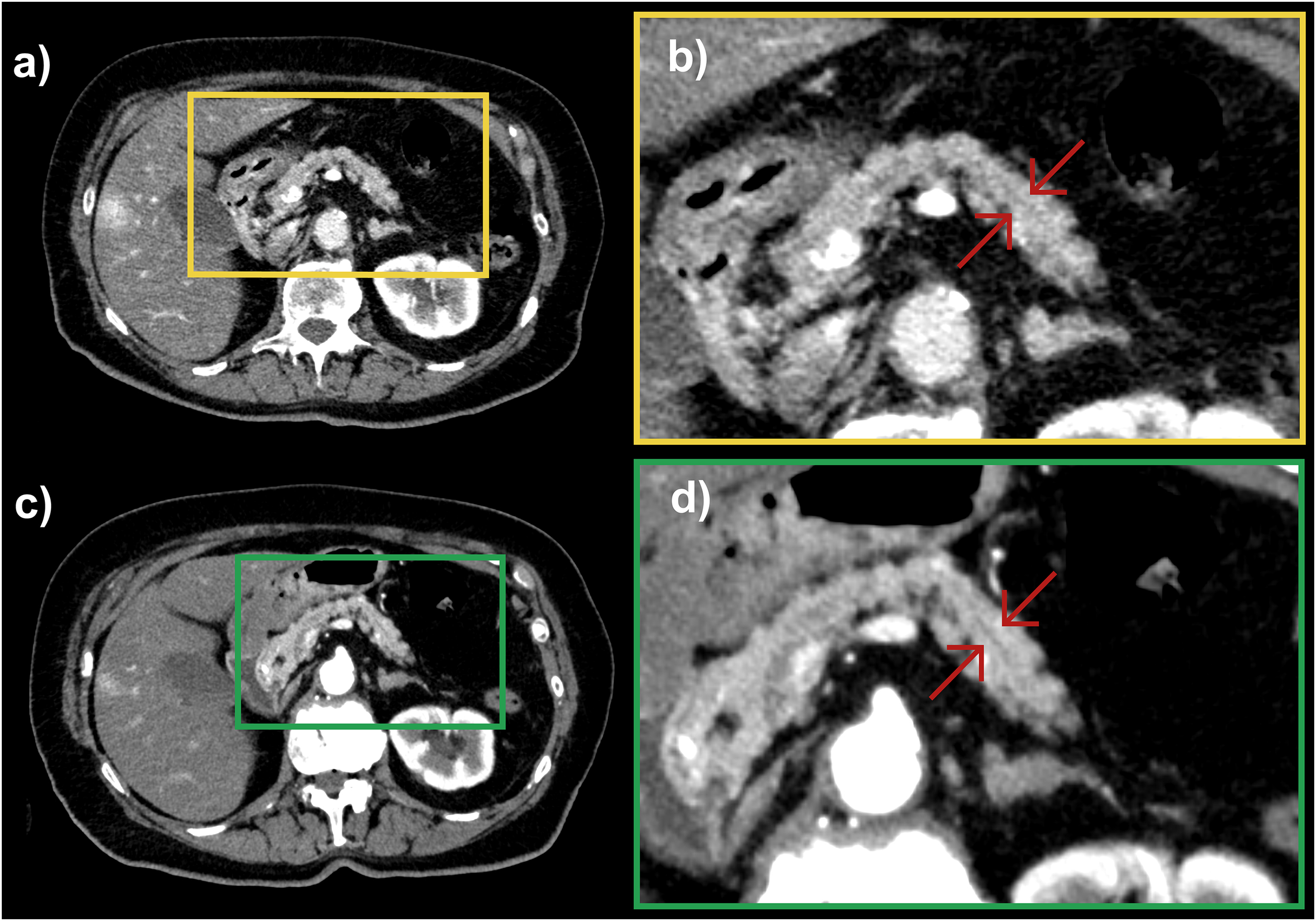
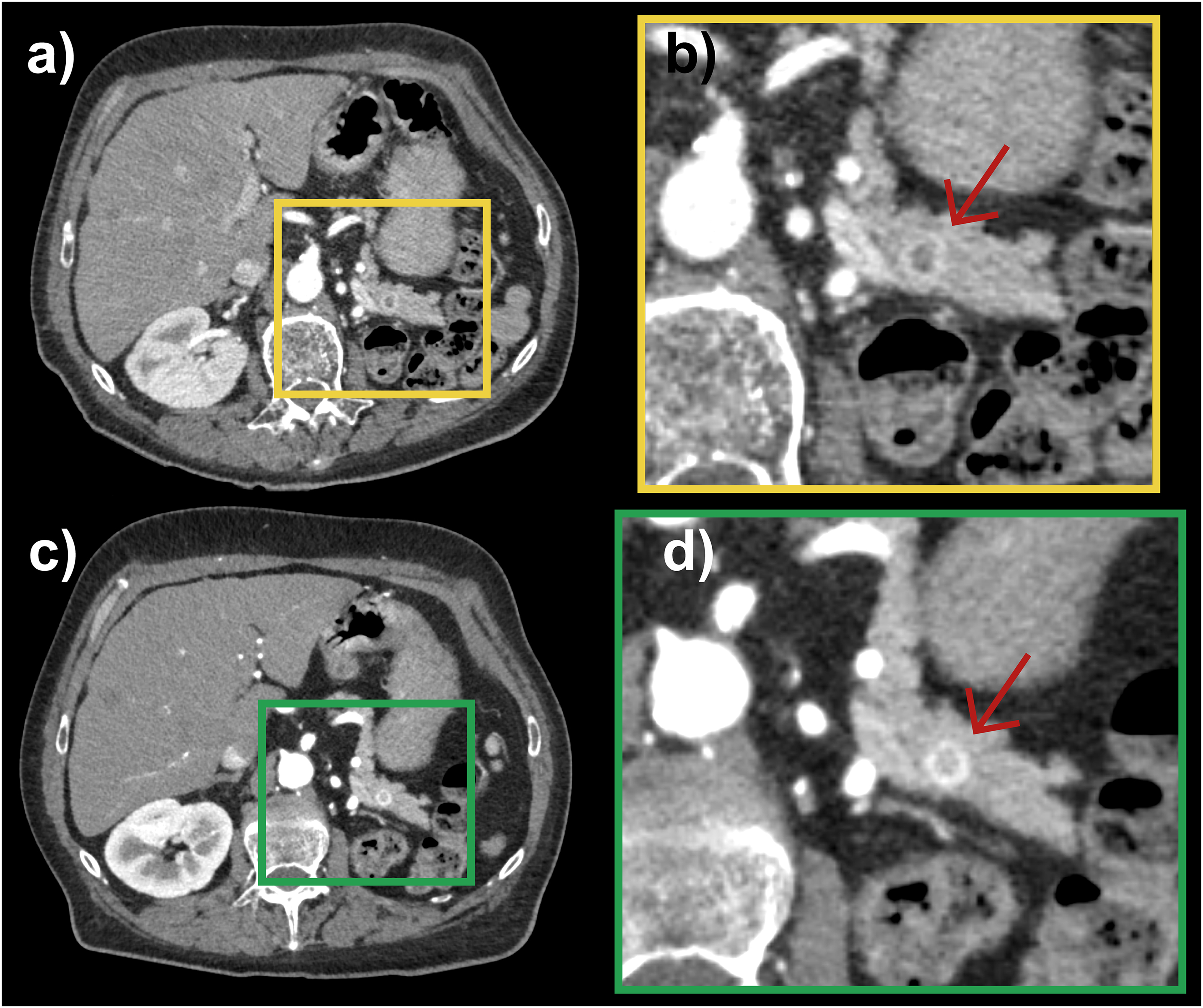
Comparison of (a, b) EIDCT with (c, d) PCCT. (a, c) The full field of view; (b, d) zoomed images to illustrate the difference of image quality (as done by the readers). The red arrows point to the main pancreatic duct in the tail of the pancreas. EIDCT, energy-integrating detector computed tomography; PCCT, photon-counting computed tomography.
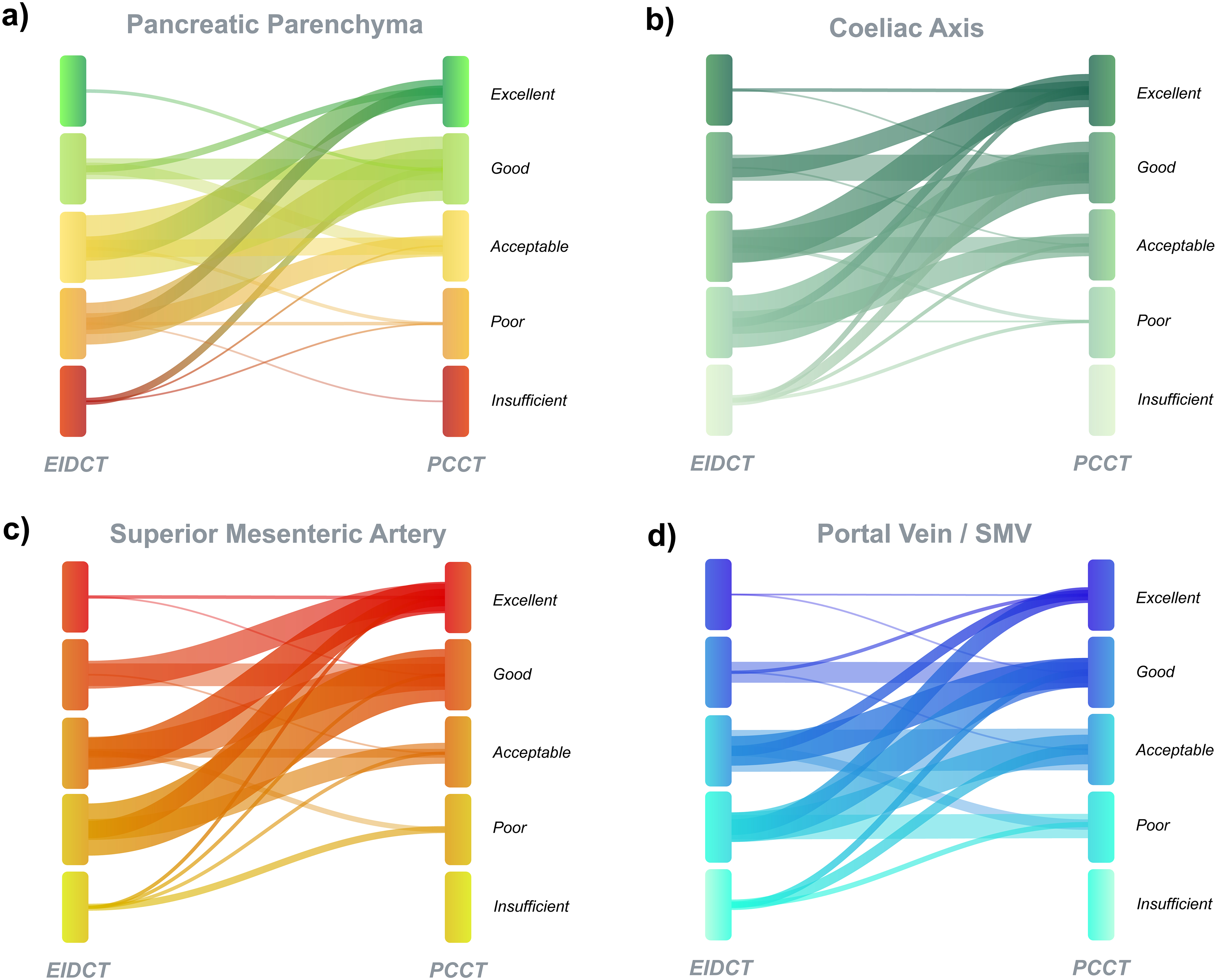
Modified alluvial plots of four of the 11 subjectively evaluated areas on a 5-point Likert scale regarding image quality. (a) Pancreatic parenchyma, (b) coeliac axis, (c) superior mesenteric artery, and (d) portal vein/superior mesenteric vein (SMV). The thickness of the individual alluvia reflects the frequency of the image quality grading, whereas the y-axis (stratum layer) does not reflect the frequency of gradings in contrary to a normal alluvial plot.
Table of mean and individual readers subjective grading for the 11 evaluated structures.
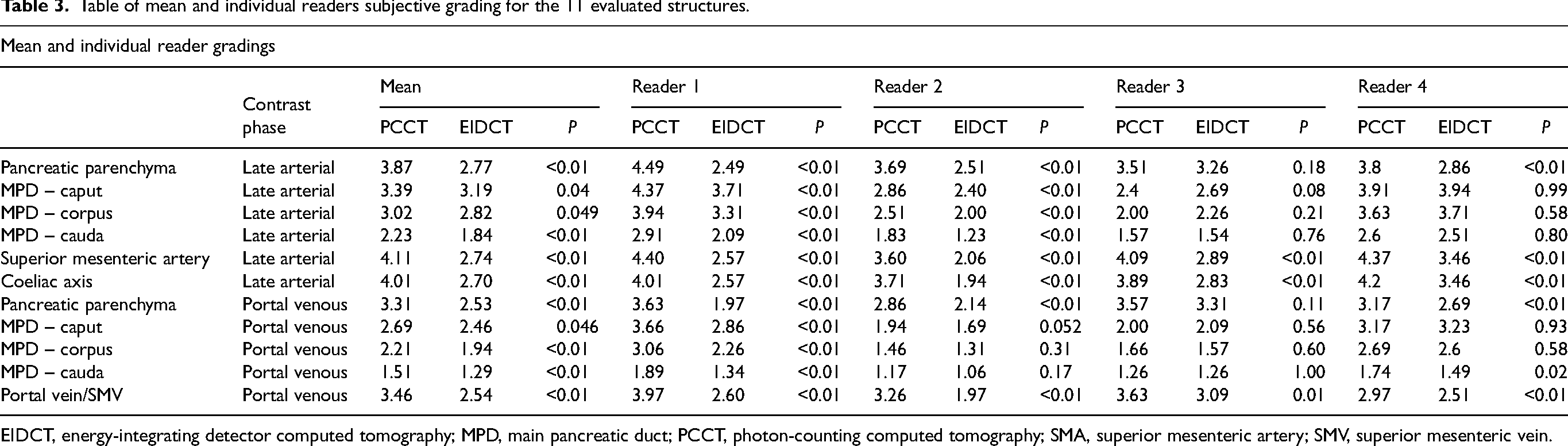
EIDCT, energy-integrating detector computed tomography; MPD, main pancreatic duct; PCCT, photon-counting computed tomography; SMA, superior mesenteric artery; SMV, superior mesenteric vein.
Image quality was rated considerably better on PCCT than on EIDCT for the superior mesenteric artery (4.11 vs. 2.74; P <0.01), the coeliac axis (4.01 vs. 2.70; P <0.01) (Fig. 5), and the portal vein/superior mesenteric vein (3.46 vs. 2.54; P <0.01). Fig. 5a and b are EIDCT images and were graded as “acceptable image quality” (i.e. 3 on our scale), while Fig. 5c and d are PCCT images of the same patient and were graded as “good image quality” (i.e. 4 on our scale).
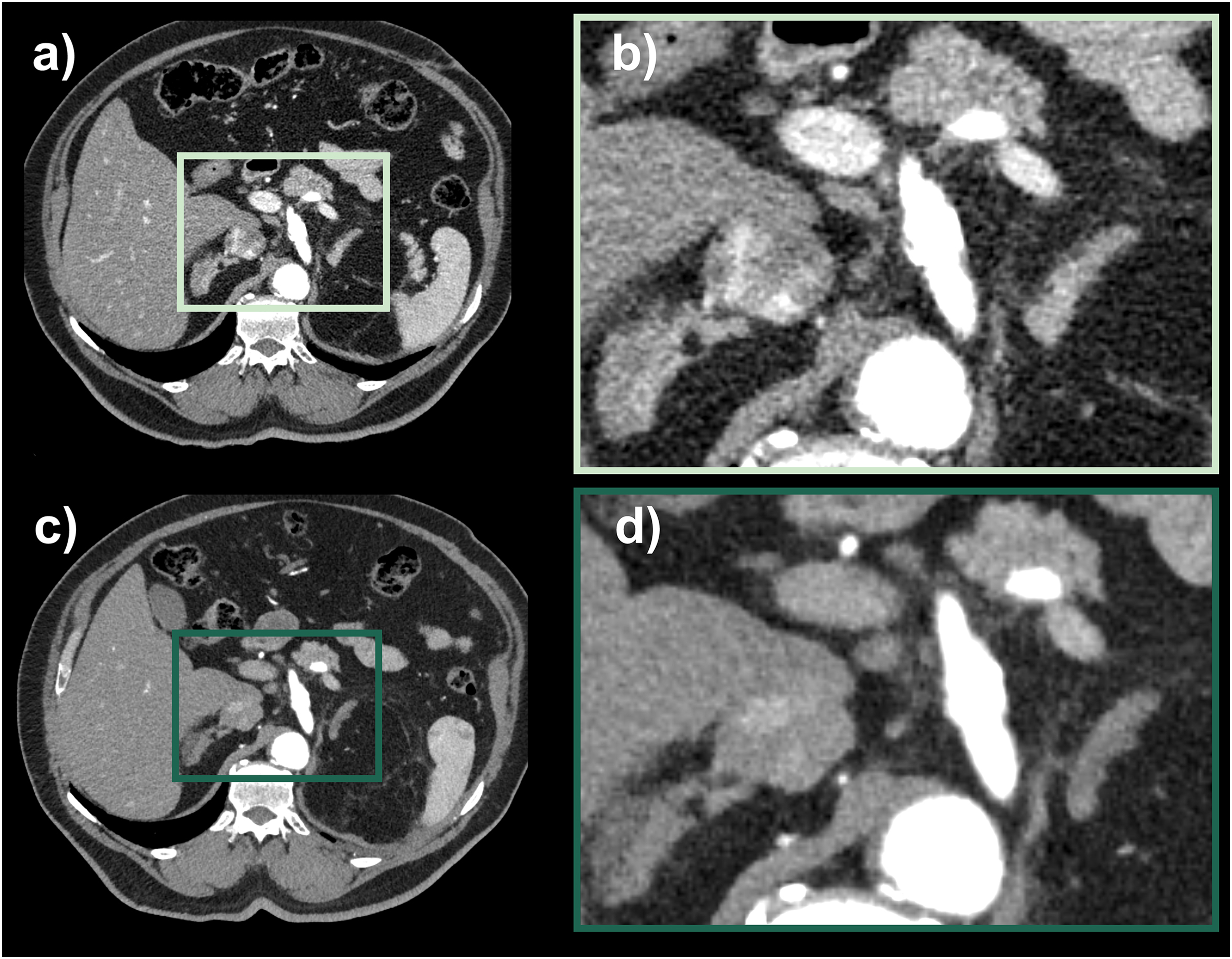
Example of the subjective image quality grading surrounding the coeliac axis. (a, b) EIDCT, (c, d) PCCT. EIDCT, energy-integrating detector computed tomography; PCCT, photon-counting computed tomography.
Our readers detected three small hypervascular pancreatic metastases from RCC in two different patients on PCCT scans in this study in the late arterial phase (Fig. 6). These findings had not been reported in the original imaging reports in our RIS system. The patients’ records and all available imaging were reviewed and none of these additional findings had any clinical consequence for the patients (since they both had other simultaneous metastases from RCC). The paired EIDCT scans were also evaluated. One scan was 3 months earlier (Fig. 6a and b) to PCCT (Fig. 6c and d), while the other scan was 6 months after the PCCT. All three lesions could retrospectively be detected on EIDCT in the late arterial phase. Two of the metastases had an unchanged size but were less conspicuous (Fig. 6), and one metastasis was smaller on EIDCT and less enhancing.
Comparison of (a, b) EIDCT images and (c, d) PCCT images of the tail of the pancreas in the same patient. The red arrows point to the detected renal cell cancer metastasis. EIDCT, energy-integrating detector computed tomography; PCCT, photon-counting computed tomography.
Quantitative parameters
The noise levels were significantly lower with PCCT, with a mean reduction of 5.8 HU across all parameters (SD of 15.6 HU vs. 21.4 HU; P <0.01). The MPD could be measured in more cases on PCCT than on EIDCT in the head (35/35 on PCCT; 32/35 cases on EIDCT) and especially in the tail of the pancreas (27/35 on PCCT; 16/35 on EIDCT). DLP was significantly reduced n both phases, with a 31.8% reduction (266.2 mg*cm vs. 390.4 mGy*cm: P <0.01) for the LA phase and 21.5% (735.5 mGy*cm vs. 936.8 mGy*cm; P <0.01) for the PV phase (Table 1). There was no significant difference in the amount of IV contrast from PCCT to EIDCT (1094 mL vs. 108.8 mL; P = 0.73). The time interval between EIDCT and PCCT was in the range of −23 months to +19 months. There was no systematic difference in the time interval from EIDCT to PCCT (mean difference of the scan dates of 29 days; P = 0.496) (Table 1). However, we found a small but significant difference in the mean attenuation of the pancreatic parenchyma in the LA phase with a lower enhancement on PCCT than EIDCT (120.2 HU vs. 135.4 HU; P <0.01).
Inter-reader agreement
There was a fair to moderate mean inter-reader agreement between readers for image quality grading of the pancreatic parenchyma in the LA phase, PV phase, MPD, superior mesenteric artery, and portal vein/superior mesenteric vein. The subjective grading of the coeliac axis showed poor inter-reader agreement (Table 4).
Table of inter-reader agreement (κ) for the evaluated structures.
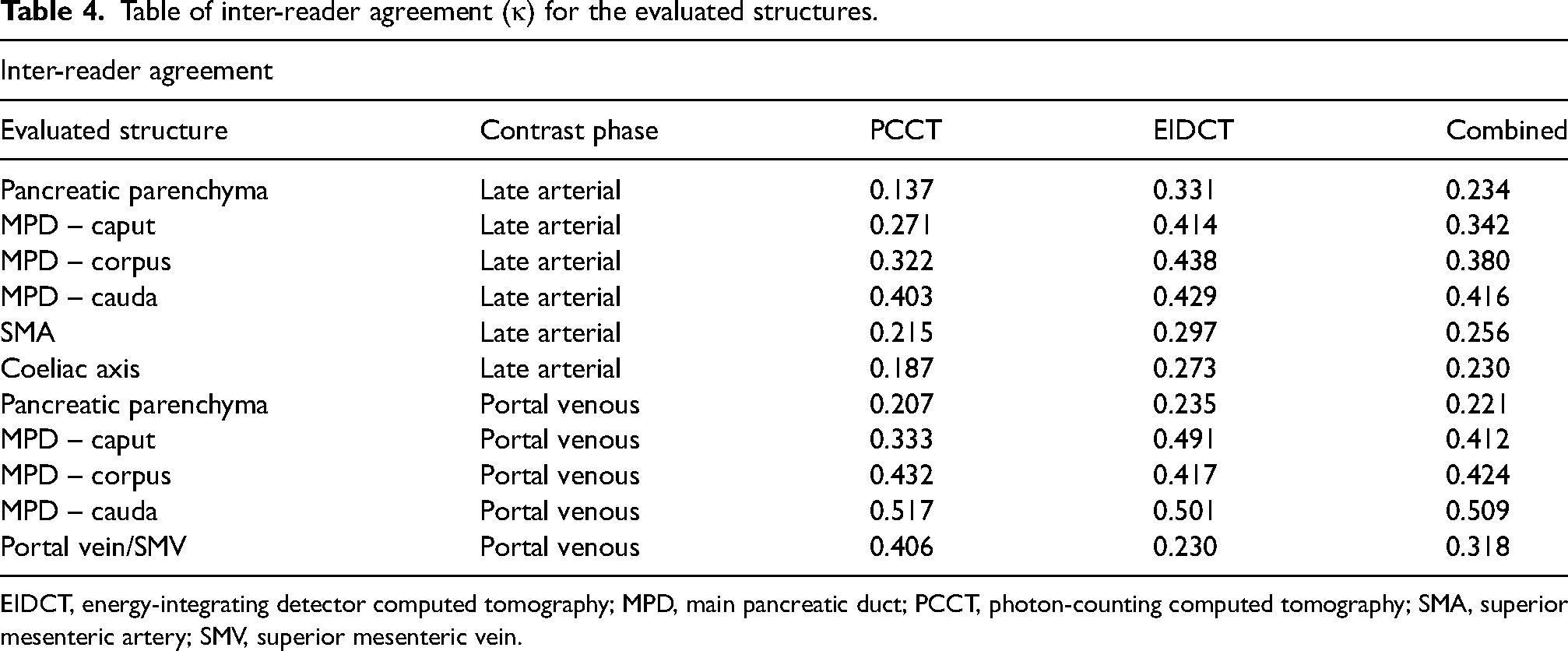
EIDCT, energy-integrating detector computed tomography; MPD, main pancreatic duct; PCCT, photon-counting computed tomography; SMA, superior mesenteric artery; SMV, superior mesenteric vein.
Discussion
We found significantly improved image quality of all evaluated pancreatic and peripancreatic structures when scanning patients with PCCT compared to EIDCT for all readers and for each reader individually. The MPD was measurable on considerably more PCCT scans than on EIDCT. In addition, image noise was quantitatively significantly reduced at reduced patient dose levels in both the LA and PV phases. As the pancreas is a difficult organ to visualize with imaging, pancreatic cancers are often not detected on initial imaging (2). Evaluation of pancreatic vessels is essential for determining whether pancreatic cancer is resectable or locally advanced (13). EIDCT has a high, but far from perfect sensitivity for the determination of vascular invasion (14). Improvements from the PCCT image quality could improve this outcome. Several studies on PCCT have demonstrated an increase in image quality over a wide range of anatomical areas (10,15). For pancreatic imaging, PCCT has been shown to make pancreatic cancers more conspicuous using monoenergetic images (16,17). Kim et al. recently showed an improved inter-reader agreement for the evaluation of vessel ingrowth and detection of metastases in the setting of pancreatic cancer on PCCT compared to EIDCT (18). They speculated that this was due to the higher spatial resolution and improved CNR. However, they did not measure the CNR or noise levels. Their findings are in line with ours, with improved image quality subjectively and quantitatively. Several other studies have reported improvements in image quality in the abdomen with a lower dose of ionizing radiation (15,19–22). However, a direct comparison of subjective and quantitative image quality parameters for PCCT and EIDCT for the evaluation of the pancreas, pancreatic duct, and pancreatic vessels has not been performed. Our findings confirm the improved pancreatic imaging seen with PCCT, which could lead to improved diagnosis and staging of pancreatic cancer, in addition to improvements in the diagnoses of other pancreatic diseases.
We excluded patients with reported pancreatic pathology or obvious gross pancreatic abnormalities (patients with fatty atrophy were not excluded). Despite this, our readers identified several small hypervascular pancreatic lesions on PCCT (Fig. 6). Whether these findings indicate a potential diagnostic advantage of PCCT is purely coincidental, or a consequence of the unintended contrast timing-difference is uncertain. However, this should be examined in future and properly powered clinical studies.
The direct comparison between PCCT and EIDCT in both the late arterial and portal venous phases was a definite strength of our study. In addition, the combination of subjective and quantitative grading of the image quality makes our results comprehensible and applicable to daily radiological routines. As mentioned in the introduction, PCCT has several advantages over EIDCT. This includes an improved spatial resolution in the x-, y-, and z-planes (including a lower collimation, as seen in Table 1). The observed differences between PCCT and EIDCT reflect the difference in image quality that were the focus of this study and therefore are not considered a limitation.
The present study has some limitations. We studied a relatively small number of patients, and this increased the risk of a selection bias. Out of 35 EIDCT scans, 34 were performed on one type of EIDCT scanner (Table 2), limiting the generalizability of our study to this type of EIDCT. We created overall subjective grading scales over several smaller anatomical peripancreatic areas instead of individually evaluating noise, sharpness, and presence of artefacts. This was an intentional methodological decision to closer simulate daily radiological image quality evaluation. The readers were introduced to the grading scales during a 60-min training session. However, inter-reader agreement for the subjective assessments was only fair to moderate, reflecting the inherent subjectivity of the grading scales. This could have been minimized by more extensive training in the use of the scales. However, as the scales were not intended for future clinical use and intra-reader comparisons between PCCT and EIDCT were highly consistent, we consider this a minor limitation. We evaluated patients without pancreatic tumors to enable assessment of the entire pancreatic parenchyma, MPD, and peripancreatic structures in all patients in a comparable manner. This was an intentional study design choice and is therefore considered a strength rather than a limitation. We observed a small but statistically significant increase in attenuation of the pancreatic parenchyma during the late arterial phase on EIDCT. This was due to an unintended difference in scan timing between the two scanners (i.e. 18 s post-bolus for EIDCT and 15 s post-bolus for PCCT). Because patients with insufficient pancreatic enhancement were excluded, this difference is unlikely to have had a substantial influence on the results. Any resulting selection bias would likely have reduced the subjective grading scores for the pancreatic parenchyma on PCCT and consequently diminished the observed difference between EIDCT and PCCT (i.e. acting in the opposite direction to our results).
Because the study was retrospective, the PCCT protocol was the standard protocol for a late arterial series. Studies have reported considerably enhanced visualization of anatomical features with an optimized pancreatic protocol and ultra-high-resolution imaging (6). Further studies with an optimized PCCT pancreatic protocol and studies of pancreatic tumors and their staging are warranted and might lead to further improvements in the diagnosis of pancreatic diseases.
In conclusion, PCCT provides consistently improved subjective and quantitative image quality compared with conventional CT for the evaluation of pancreatic and peripancreatic structures. These improvements may contribute to enhanced detection and staging of pancreatic cancer, particularly in early disease.
Supplemental Material
sj-pdf-1-acr-10.1177_02841851261458363 - Supplemental material for Improved pancreatic imaging with photon-counting CT: a retrospective comparison with conventional CT
Supplemental material, sj-pdf-1-acr-10.1177_02841851261458363 for Improved pancreatic imaging with photon-counting CT: a retrospective comparison with conventional CT by Erik Gudmann Steuble Brandt, Felix Christoph Müller, Yousef JW Nielsen, Anne Marie Ewald, Bulat Ibragimov, Henrik Thomsen, Anders Rodell and Michael Brun Andersen in Acta Radiologica
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EGSB has previously received a shared PhD research grant from Siemens Healthcare A/S along with the Innovation Fund Denmark A/S; ABR is a full-time employee of Siemens Healthineers; MBA has performed lectures/presentations with a salary from Siemens Heathineers, Philips Healthcare, and GE Healthcare. CFMüller has previously received a shared PhD research grant from Siemens Healthcare A/S along with the Innovation Fund Denmark A/S, and has been given a salary for lectures for Siemens Healthcare A/S and Sectra A/S. The remaining authors have no potential conflicts of interests.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Innovationsfonden, Novo Nordisk Fonden (grant no. 1044-00015B, NFF20OC0062056). Bulat Ibragimov was supported by the Novo Nordisk Foundation, Denmark (grant no. NFF20OC0062056).
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.