
Abstract
Background
Cementoplasty is widely used for spinal and weight-bearing extraspinal lesions, but its application in extraspinal thoracic bones (sternum, ribs, clavicles, and scapulae) remains poorly documented.
Purpose
To evaluate the feasibility, safety and pain outcomes of cementoplasty for extraspinal thoracic bone lesions.
Material and Methods
All consecutive patients who underwent cementoplasty of an extraspinal thoracic bone between March 2012 and December 2024 were retrospectively included. The following data were systematically assessed: degree of lesion filling, fracture stabilization, cement leakage, adverse events, and pain outcome at 3 months postoperatively, assessed from follow-up consultations using a four-level semi-quantitative scale (worsening pain, stable pain, pain improvement, or complete pain resolution).
Results
A total of 59 extraspinal thoracic bones were treated by cementoplasty during 51 procedures among 43 consecutive patients (27 women [63%] and 16 men [37%]; median age = 60 years). Most lesions were metastases or multiple myeloma lesions. Among patients with available follow-up, pain improvement or complete pain resolution was observed in 29/33 (88%) patients. Cement filling of more than 60% of the lesion volume was achieved in 40/45 (89%) focal lesions. Fracture stabilization was successful in 20/23 (87%) cases. Major cement leakage occurred in 5/56 (9%) treated bones with available postoperative imaging and was asymptomatic in all cases. One infectious complication was recorded.
Conclusion
Cementoplasty of extraspinal thoracic bone lesions appears technically feasible and may represent a valuable palliative option for pain relief with an acceptable safety profile.
Introduction
Cementoplasty is a minimally invasive treatment used primarily for spinal lesions, providing bone strengthening and pain relief (1,2). Vertebral cementoplasty is known to be highly effective for pain relief in patients with cancer and is a therapeutic option recommended by the European Society for Medical Oncology in the treatment of spinal metastases (level of evidence I, grade of recommendation B) (3,4). Cementoplasty has also been described for the treatment of extraspinal lesions, most of which involve weight-bearing bones such as the pelvis or long bones (5–9). Pelvic cementoplasty seems efficient to provide pain relief and long-term bone stability (10). It can be improved by associating an internal fixation using either dedicated spindles (11) or screws (12). Long bone cementoplasty is feasible but a significant number of secondary fractures have been reported, some occurring within the cement cast itself (13).
Treatment by cementoplasty of extraspinal thoracic bones (ESTB: sternum, ribs, clavicles, and scapulae), which are not weight-bearing bones, has only been described in a few case reports (5,14–18). Polymethyl methacrylate (PMMA) cement provides adequate resistance to compressive forces but limited resistance to bending and rotational forces, making percutaneous cementoplasty less effective in long bones exposed to significant mechanical stress. Consequently, its use in long bones is generally reserved for the end-of-life/palliative setting or patients unfit for surgical fixation (13). Although ESTB experience bending forces, their magnitudes are lower than those in long bones, rendering the strength of cement in ESTB unknown. Moreover, ESTB appears more challenging to treat due to specific technical difficulties: these bones are thin, mobile with respiration, close to the pleura, mediastinum, and vascular-nerve structures.
The aim of the present study was to evaluate the feasibility, safety, and pain outcomes of cementoplasty in a heterogeneous population of patients with ESTB lesions and to describe the main technical considerations associated with this procedure.
Material and Methods
Research ethics standards compliance
The study protocol was approved by the Comité d’éthique de la recherche en imagerie médicale (CERIM; Ethics Committee for Research in Medical Imaging) (CRM-2310-385, 22/12/2023). All data, including imaging data, were retrospectively collected and anonymized in accordance with national data protection regulations. The requirement for informed consent for participation in the study was waived due to the retrospective nature of the study, including permission for publication of anonymized clinical images.
All patients had provided informed consent for the therapeutic procedure itself. Each procedure was performed following either the recommendation of a multidisciplinary team meeting for patients with bone tumors or a consultation with the operator for patients with bone fractures.
Design of the study
This is a single-center, retrospective, observational study performed according to the STROBE guidelines (19).
Patient selection
All patients who underwent an ESTB cementoplasty attempt at a single tertiary care teaching hospital between March 2012 and December 2024 were included in a prospectively filled database. Inclusion criteria were patients with an ESTB tumor lesion or fracture who underwent cementoplasty for pain relief or stabilization. Patients who underwent concurrent percutaneous thermal ablation were excluded, as the objectives of that procedure were different. Demographics, site of the lesion (sternum, rib, scapula, and clavicle) and lesion characteristics (pathological origin, osteolytic/mixed, or osteoblastic pattern) were systematically recorded. Clinical, technical, and safety endpoints were evaluated retrospectively by screening the medical records, the postoperative computed tomography (CT) scan and the last follow-up CT scan when available. The flow chart of inclusions is provided in Fig. 1.
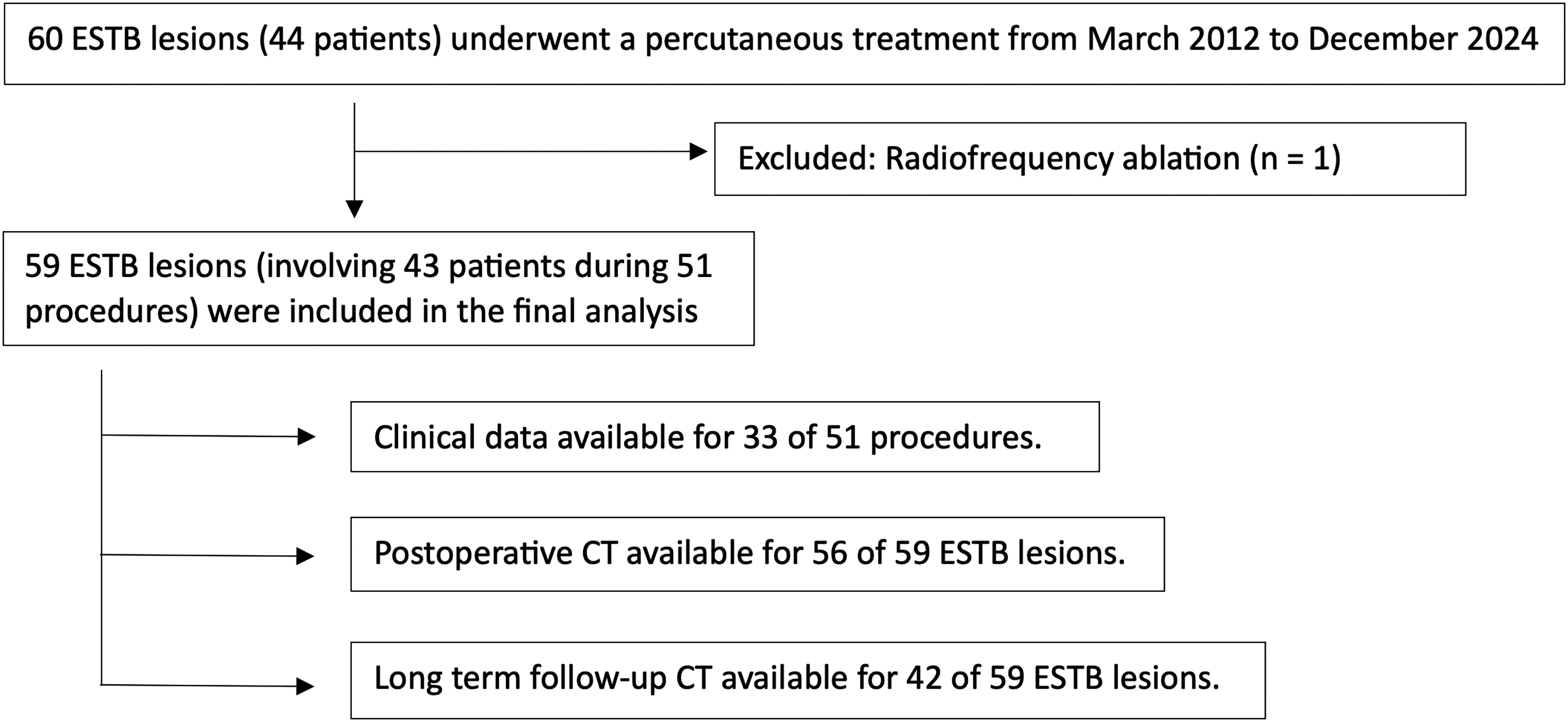
Flow chart diagram.
Technical endpoints
For tumoral lesions, the percentage of lesion filling was estimated visually on the control CT using five classes (0%–20%, 20%–40%, 40%–60%, 60%–80%, and 80%–100%).
For fractures, the result was considered technically successful if the cement filled the fracture site and the bone on both sides of the fracture site.
Bone cement leakages were also systematically recorded and were divided into absent, negligible (thin linear leakage on the bone needle's path), minor (leakage <50% of the volume in the target lesion), intermediate (leakage of 50%–100% of the volume in the target lesion) and major (leakage >100% of the volume in the target lesion).
Clinical endpoints
Clinical follow-up was performed by consultation or teleconsultation 3 months after each procedure. Pain outcomes were evaluated using a semi-quantitative scale based on changes in pain reported during follow-up consultations: (i) pain worsening; (ii) stable pain; (iii) pain improvement; and (iv) complete resolution of pain. Standardized numeric pain intensity scales were not consistently available in the retrospective clinical records.
Safety
Adverse events were systematically collected and graded using the Society of Interventional Radiology (SIR) adverse event classification (20).
Imaging follow-up
When available, the last CT available was systematically assessed. This allowed us to evaluate the radiological evolution of the treated bone and to assess progression of the lesion, a fracture, or an adverse event.
Technical aspects
Patients were treated either under general anesthesia (49%) or conscious sedation (51%). For antibiotic prophylaxis, 2 g of cefazoline was administered intravenously at the beginning of the procedure. Out of the 59 lesions, 57 (97%) were treated in a hybrid angiosuite, combining a flat panel C-arm (Artis Zee; Siemens Healthcare, Erlangen, Germany) and a 16-row CT scanner (Miyabi Emotion 16; Siemens Healthcare, Erlangen, Germany) with fluoroscopy guidance for 11 (17%) patients and fluoroscopy associated to CT guidance for 46 (80%) patients. The remaining 2 (3%) patients were treated using biplane fluoroscopic guidance and cone-beam CT (CBCT) (Artis Q Biplane; Siemens Healthcare, Erlangen, Germany) with an integrated real-time navigation system (Syngo Needle Guidance; Siemens Healthcare, Erlangen, Germany). In two cases of rib fractures, the bone needle was inserted using an electromagnetic navigation system (EMNS) (Imactis; GE Healthcare, Chicago, IL, USA). Cementoplasty was performed with one (n = 22/59), two (n = 29/59), or three (n = 8/59) 11-G bone needles with a length of 100, 125, or 150 mm (T’CD II; Strim Healthcare, Margencel, France). A bone biopsy was systematically performed. Low viscosity PMMA bone cement (V-FAST; Strim Healthcare, Margencel, France) was injected under fluoroscopic guidance. All patients underwent control CT at the end of the procedure. The technique is illustrated in Figs. 2 and 3, with the real-time navigation system Syngo Needle Guidance for the sternum, Fig. 4 for the ribs, and Fig. 5 for the clavicle.
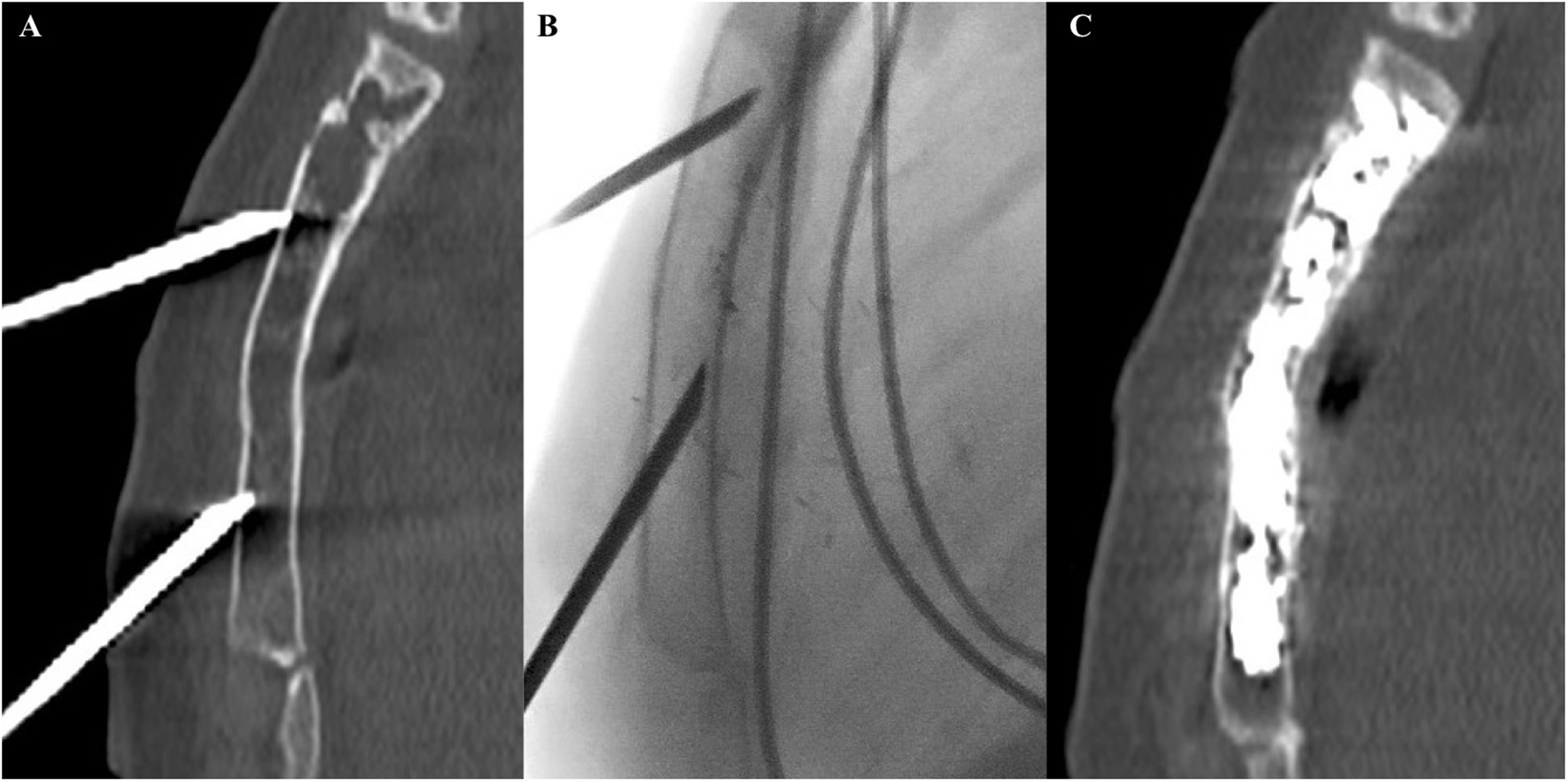
A 40-year-old woman with a painful sternal body lytic bone metastasis from breast cancer treated with cementoplasty. (a) Two bone needles were inserted using an ascending median approach under CT guidance to ensure midline placement. (b) The bone needles were advanced to the target lesion under lateral fluoroscopic guidance. (c) Cement was injected under lateral fluoroscopic visualization to monitor the integrity of the posterior and anterior sternal walls. The postoperative CT scan demonstrates satisfactory filling without leakage. CT, computed tomography.
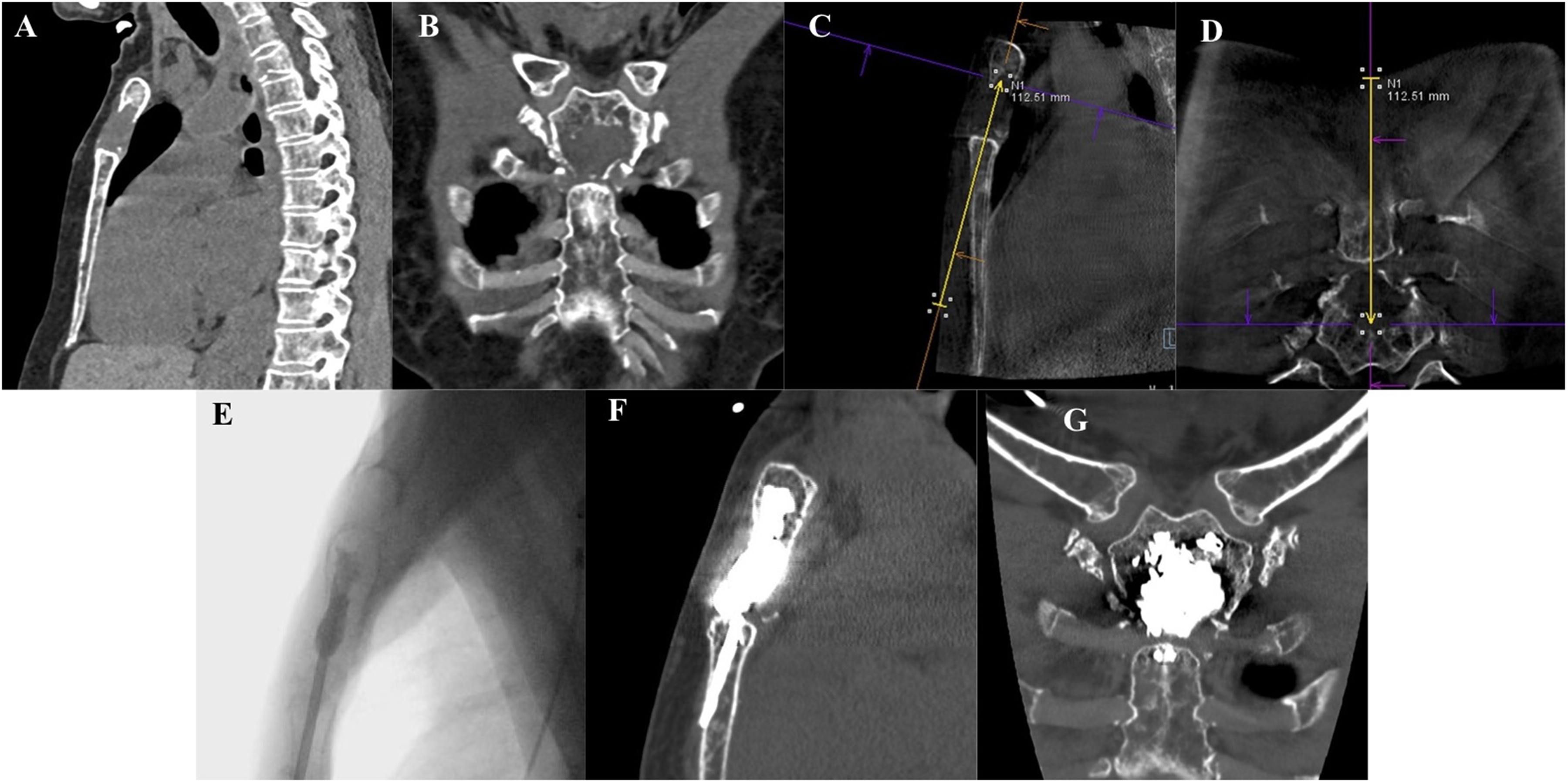
A 55-year-old woman with a painful lytic lesion of the sternal manubrium caused by multiple myeloma, treated with cementoplasty using biplane fluoroscopy and CBCT with an integrated real-time navigation system (Syngo Needle Guidance; Siemens). (a, b) Preoperative CT images showing an osteolytic lesion involving the sternal manubrium. Orthogonal multiplanar CBCT images depict the planned needle trajectory to the target lesion. (c, d) Real-time needle trajectory projection on fluoroscopic images. (e) Lateral fluoroscopic view showing the needle within the sternal manubrium and cement being injected into the lesion. (f, g) Postoperative CT images showing satisfactory lesion filling. The cylindrical cement along the needle path in the sternal body represents cement released during needle withdrawal. To prevent cement leakage into soft tissue, the needle was angulated to bend and break the cement column during withdrawal, ensuring the cement remained within the bone. CBCT, cone-beam computed tomography; CT, computed tomography.
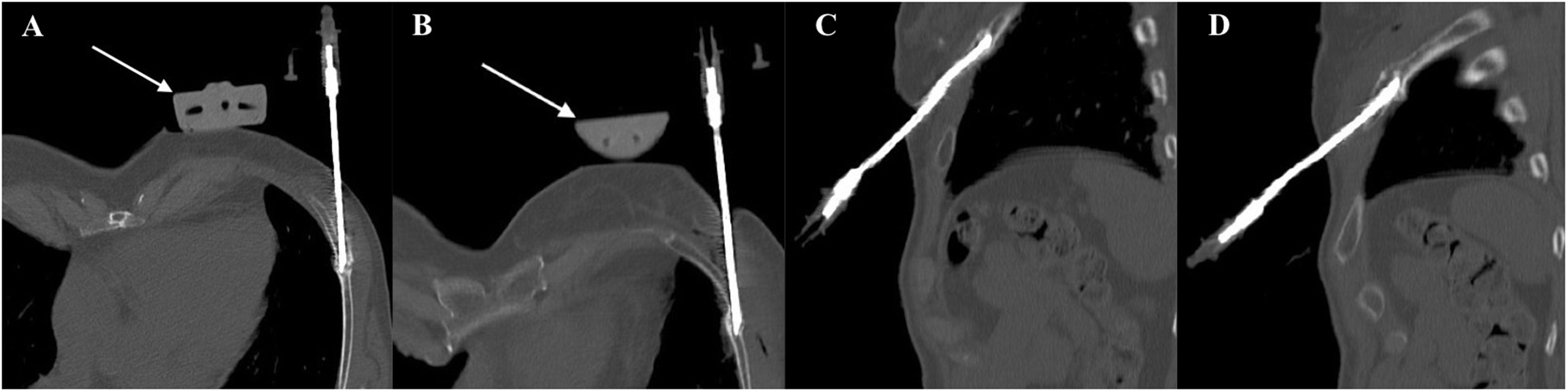
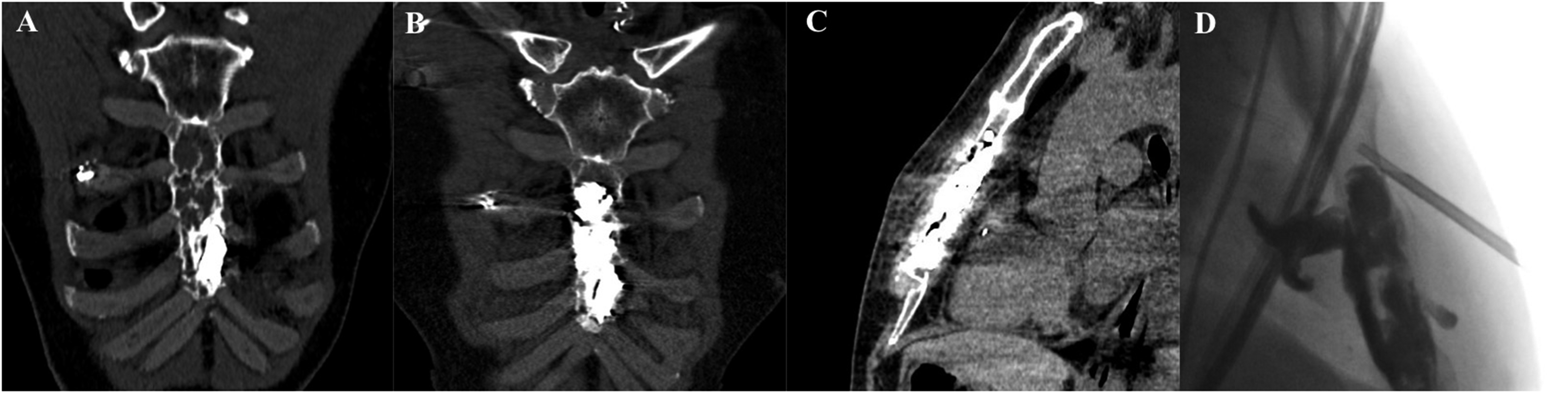
A 59-year-old woman who underwent radiotherapy for breast cancer, resulting in radiotherapy-induced osteoporosis. The patient sustained a left rib injury with fractures of four ribs. Two ribs consolidated successfully, while the other two remained painful due to incomplete healing. Cementoplasty was performed on the middle arches of the fifth and sixth left ribs. (a, b) Axial oblique multiplanar reconstruction showing the posterior tangential needle approach for the fifth and sixth ribs. (c, d) The electromagnetic navigation system reference marker is visible on the skin surface (arrows). Sagittal oblique multiplanar reconstruction shows the needle paths for the fifth and sixth ribs, respectively.
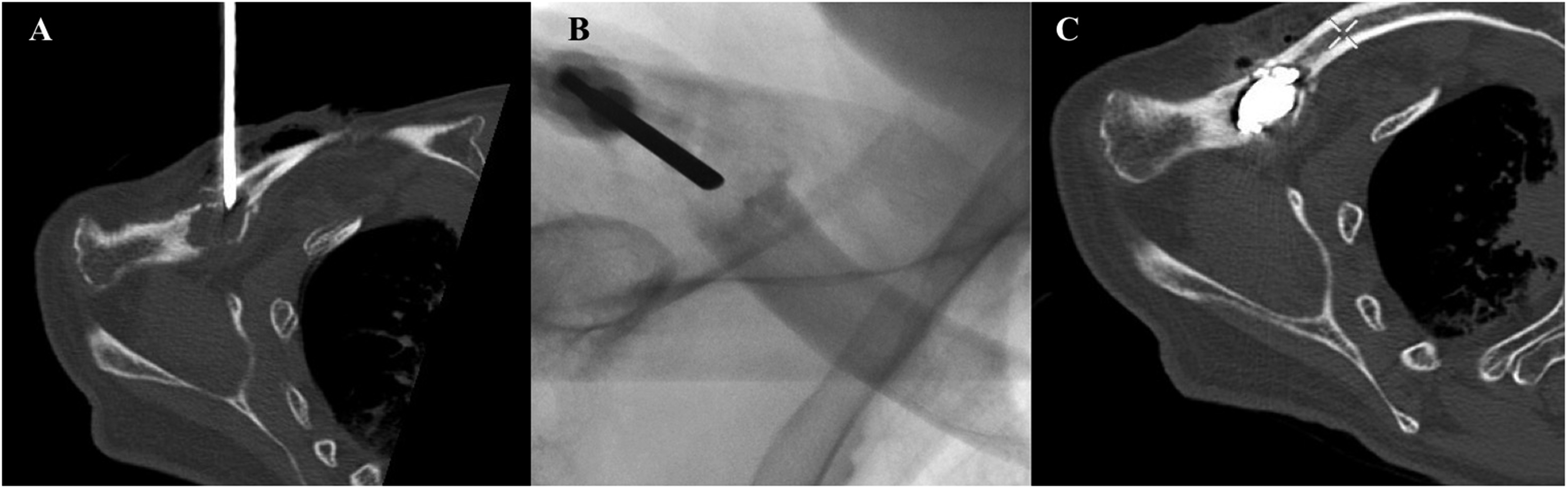
A 73-year-old man with a painful right clavicle lytic bone metastasis from renal cancer treated with cementoplasty. (a) A bone needle was inserted using an anterior perpendicular approach under CT guidance. (b) Cement was injected under oblique fluoroscopic guidance to monitor lesion filling and detect leaks. (c) The postoperative CT scan shows satisfactory filling without evidence of leakage. CT, computed tomography.
Statistical analysis
Descriptive statistics were used to report the results. No inferential statistical tests were performed, as the study was primarily observational/descriptive in nature.
A 48-year-old man treated for the second time for a painful sternal body metastasis from thyroid cancer. (a) Preoperative CT images show an osteolytic lesion involving the entire body of the sternum and a previous cementoplasty performed 5 years earlier. (b) Postoperative CT images show satisfactory lesion filling. (c) The patient developed skin inflammation a few days after the procedure. (d) CT images demonstrate subcutaneous fat thickening and densification in front of the sternal body without evidence of abscess formation. Biopsy confirmed methicillin-resistant Staphylococcus epidermidis. The patient was successfully treated with antibiotics for 3 months, with complete resolution of the infection and no sequelae. CT, computed tomography.
Results
Patient demographics and lesion characteristics
Between March 2012 and December 2024, 59 ESTB were treated by cementoplasty in 51 procedures and 43 patients(16 men, 27 women; median age = 60 years; age range = 21–92 years). Patient demographics are summarized in Table 1.
Baseline characteristics of the population.
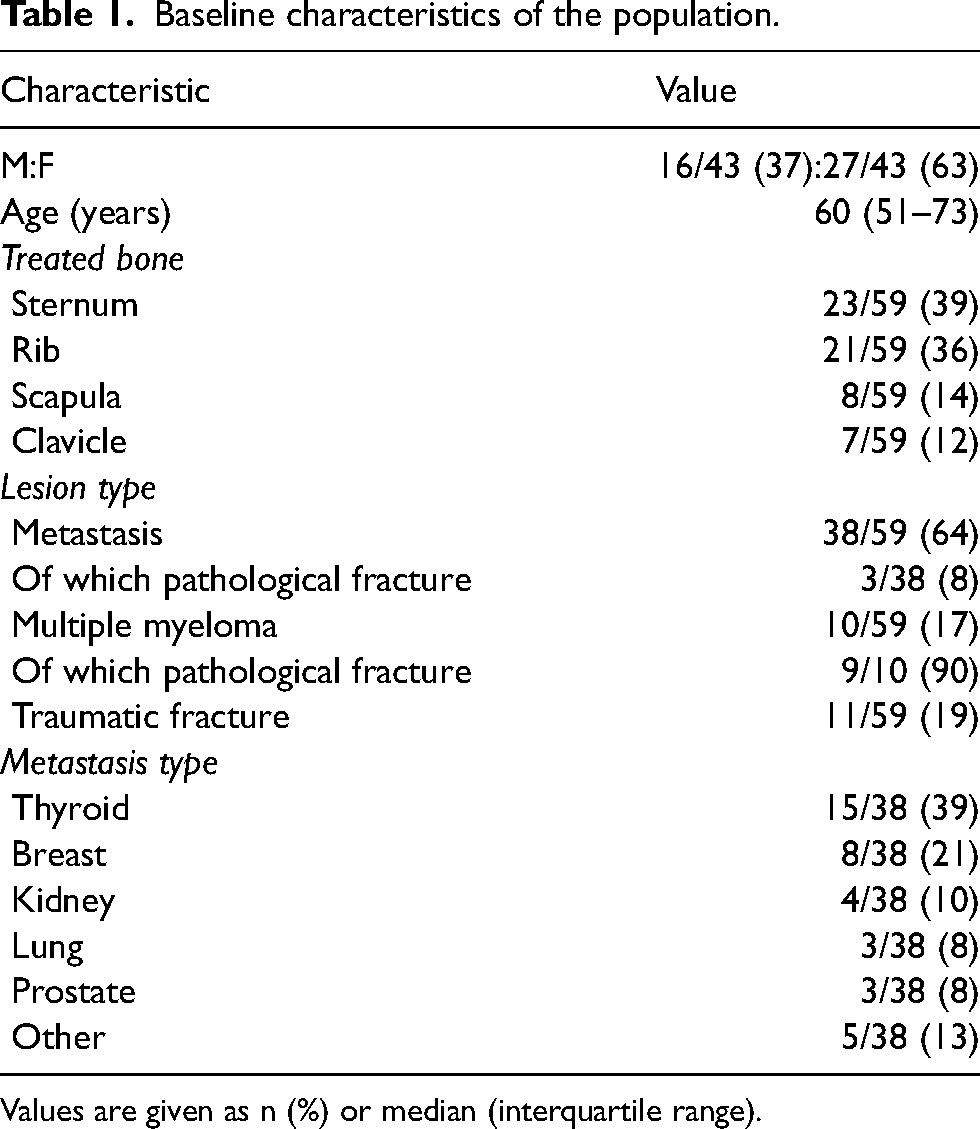
Values are given as n (%) or median (interquartile range).
Technical endpoints
Lesion filling volume was greater than 80% in 32/45 (71%) focal lesions. Among the 23 traumatic and pathological fractures, the treatment successfully filled the fracture site and the adjacent bone in 20/23 (87%) cases. Intermediate or major leaks (>50% of the target lesion volume) were observed in 16/56 (28%) cases and had no clinical consequences. Technical endpoints are summarized in Table 2.
Clinical and technical results.
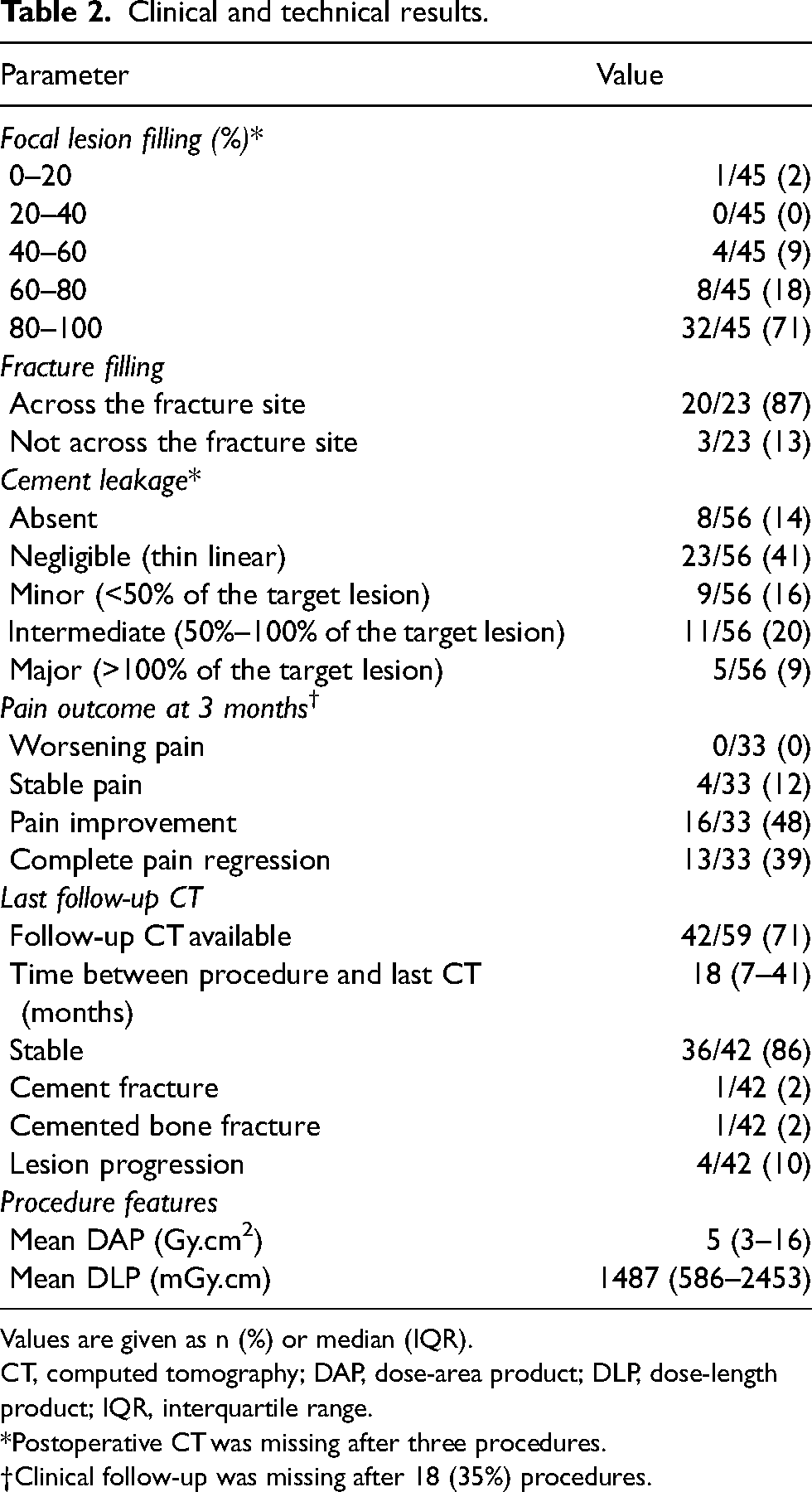
Values are given as n (%) or median (IQR).
CT, computed tomography; DAP, dose-area product; DLP, dose-length product; IQR, interquartile range.
*Postoperative CT was missing after three procedures.
Clinical follow-up was missing after 18 (35%) procedures.
Clinical endpoints
Follow-up data were unavailable for 18/51 (35%) procedures, either due to patients being lost to follow-up, patients dying before follow-up, or missing data in the medical records. Among the 33 patients with available clinical follow-up data, 13 (39%) experienced complete pain resolution, 16 (48%) demonstrated pain improvement, 4 (12%) had stable pain, and no patients reported pain worsening. The median time from treatment to clinical follow-up was 60 days. A summary of the clinical endpoints is provided in Table 2.
Safety
One patient underwent a grade 2 SIR adverse event: a 48-year-old man treated for a sternum body metastasis from a thyroid cancer (Fig. 6). He had been treated with lenvatinib (a vascular endothelial growth factor receptor tyrosine kinase inhibitor) for 2 weeks before the procedure. He developed skin inflammation a few days after treatment. He was hospitalized for infectious sampling, which showed methicillin-resistant Staphylococcus epidermidis. In agreement with the infectiology team at our center, he was treated with daptomycin for 1 week then rifampicin and levofloxacin for 3 months. There were no sequelae and the infection completely resolved.
Imaging follow-up endpoints
CT follow-up was available in 42/59 (71%) ESTB cementoplasties, with a median time interval of 18 months. Two cases of treated bone fracture occurred: one fracture of the treated sternum body through the cement cast and one fracture of the sternum body after manubrium cementoplasty away from the cement. Four cases of lesion local progression occurred. Follow-up endpoints are summarized in Table 2.
Discussion
The present study evaluated the feasibility, safety, and pain outcomes of cementoplasty for ESTB lesions in a heterogeneous population of patients with painful bone lesions. Patients with painful ESTB lesions are usually managed using multimodal palliative strategies including analgesics and radiation therapy. The present study was not designed to compare cementoplasty with these treatment options, but rather to evaluate its role as a complementary minimally invasive option for the management of ESTB-related pain. The high technical success rate and limited number of complications support the safety of cementoplasty in this setting. Most patients with available clinical follow-up reported pain relief after the procedure, supporting the potential palliative role of cementoplasty for ESTB lesions.
Only a limited number of reports have previously described cementoplasty for ESTB lesions, with most published data limited to isolated sternal case reports (14–18,21). To our knowledge, the present series represents the largest reported cohort of ESTB cementoplasty to date. The pain relief observed in our study is consistent with the favorable clinical outcomes previously reported in these isolated cases.
Previous reports of sternal cementoplasty mainly described perpendicular or anterolateral approaches requiring multiple needle trajectories (14–16,18). In contrast, the ascending tangent approach used in our study appeared to provide satisfactory cement distribution while maintaining a safe distance from mediastinal structures, with a limited number of clinically significant cement leakages.
Percutaneous ablation techniques may be combined with cementoplasty for the treatment of ESTB lesions, particularly for local tumor control of bone metastases (22–24). The present study primarily focused on the palliative role of cementoplasty for pain relief and stabilization of ESTB lesions. The superficial location of thoracic bones may also increase the risk of cutaneous injury during thermal ablation procedures.
Some teams combine cementoplasty with screw fixation or osteosynthesis, particularly for lesions involving the shoulder girdle, sternum, or clavicle (25–27). In the present series, isolated cementoplasty provided satisfactory stabilization in most patients, with only one reported intracement fracture occurring in a patient with extensive sternal cortical destruction and incomplete cement filling. Nevertheless, the choice between isolated cementoplasty and additional stabilization likely depends on lesion size, cortical integrity, and expected mechanical stress (28).
Intermediate or major cement leakage occurred in 28% of procedures but was not associated with clinically significant consequences. Major leakage occurred in 9% of treated bones with available postoperative imaging. Comparable leakage rates have previously been reported during percutaneous bone interventions, with only rare cases requiring extraction of leaked cement (29).
One infectious complication occurred after sternal cementoplasty despite perioperative antibiotic prophylaxis. The patient had recently started lenvatinib treatment, which may have contributed to impaired wound healing and increased susceptibility to infection (30). The superficial location of thoracic bones may theoretically increase exposure to cutaneous contamination. These observations support careful preventive measures, including perioperative antibiotic prophylaxis.
The present study has some limitations. First, its retrospective single-center design and long inclusion period expose the analysis to potential selection, reporting, and procedural heterogeneity biases. Second, the study population was heterogeneous and included metastatic lesions, hematological malignancies, and fractures involving multiple thoracic bone locations. Subgroup analyses according to lesion location were not performed because of the limited sample size within each anatomical subgroup. Many patients received concomitant therapies, including analgesics and radiation therapy, which may have contributed to pain relief and limit attribution of clinical benefit exclusively to cementoplasty. Pain assessment relied primarily on patient-reported changes in pain documented in follow-up consultations rather than on standardized pain or quality-of-life scales. Although this pragmatic approach reflects routine clinical practice, it provides a less standardized assessment of treatment response. Pain related to ESTB lesions is often heterogeneous, fluctuating, and position-dependent, which may be only partially reflected by single time point pain intensity scales. In addition, the degree of lesion filling was subjectively assessed and may have been overestimated (31). Finally, clinical follow-up data were incomplete for a substantial proportion of patients.
In conclusion, cementoplasty for extraspinal thoracic bone lesions appears technically feasible and may represent a valuable palliative option for pain relief with an acceptable safety profile. However, these findings should be interpreted cautiously given the retrospective design, heterogeneous population and absence of comparative data.
Footnotes
Consent for publication
Consent for publication was obtained for every individual person’s data included in the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required. Our local institutional review board (IRB), the “Comité d'éthique de la recherche en imagerie médicale” (CERIM) approved the study protocol (IRB approval CRM-2310-385).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from all individual participants included in the study.