
Abstract
This study aimed to characterize the clinical presentation, ophthalmologic findings, and final diagnoses of patients with primary intracranial mass lesions who initially presented with visual symptoms. We conducted a retrospective observational case series at the Neuro-ophthalmology Department of Chi Mei Medical Center, Taiwan, analyzing adult patients who presented with visual disturbances between January 2021 and August 2023 and were subsequently diagnosed with intracranial mass lesions. Demographic characteristics, ophthalmologic findings, imaging results, treatment modalities, and visual outcomes were analyzed. Thirteen patients were included (six men; mean age: 45.2 ± 13.1 years). Blurred vision (61.5%) was the most frequent presenting symptom. Visual field defects (76.9%) and optic disc pallor (53.9%) were common findings. Pituitary adenoma was the most predominant tumor type (38.5%). The results indicate that visual symptomatology may represent an early manifestation of primary intracranial mass lesions. Prompt neuroimaging and multidisciplinary management are essential for achieving timely diagnosis and optimal clinical outcomes.
Keywords
Introduction
Primary intracranial lesions represent a significant health challenge, ranking as the seventh most prevalent intracranial lesion in adults in many developed countries and acting as a leading cause of neurological disease-related deaths, surpassed only by stroke in several demographic regions. 1 Due to their anatomical location and mass effect, these lesions frequently disrupt afferent and efferent pathways, resulting in a broad spectrum of neurological and ophthalmic complaints.
The clinical presentation of a brain tumor is highly variable and is influenced by factors such as the tumor location, size, growth rate, and the extent of surrounding mass effect or edema. Common initial symptoms—which reflect generalized cerebral irritation or increased intracranial pressure—include seizures, persistent headaches, and varying degrees of cognitive impairment.
Crucially, visual disturbances also frequently serve as an initial presenting symptom in a notable proportion of cases, with both their occurrence and severity often increasing as the tumor progresses. These visual deficits may result from direct tumor compression of the optic nerve, optic chiasm, or visual pathways in the brain or indirectly from hydrocephalus and papilledema due to elevated intracranial pressure. Of particular diagnostic concern, visual disturbances associated with low-grade or slow-growing tumors are frequently implicated in delayed diagnosis, as subtle or intermittent visual changes may be misattributed to other causes. 2 Understanding the exact nature and frequency of these initial visual presentations is crucial for enhancing diagnostic vigilance across multiple clinical specialties.
Review of existing literature and research gap
Despite the neurological burden of brain tumors, the existing literature addressing the full spectrum of initial visual disturbances across a broad cohort of intracranial mass lesions remains comparatively scarce and fragmented. Most existing research has focused on the visual impact of specific tumor types (e.g. pituitary adenomas or optic pathway gliomas), often in very small series, rather than providing a comprehensive, generalized analysis across all primary intracranial mass lesions. 3 Systematic studies detailing the clinical characteristics of initial visual symptoms across diverse patient populations remain notably limited. For example, foundational research includes reports constrained by very small sample sizes, such as studies by Lee et al. 3 involving 11 patients and by Sefi-Yurdakul 2 involving 18 patients. Although a larger-scale analysis in 2020 by Alther et al. 4 provided valuable data from a cohort of 85 patients, the overall evidence base remains constrained by limited sample sizes and narrow diagnostic focus, hindering the generation of robust, population-level insights.
Furthermore, contemporary, population-based data on this topic within the Taiwanese clinical setting remain distinctly scarce. This geographical and clinical gap underscores the urgent need for a large-scale, locally relevant investigation to enhance diagnostic algorithms, identify high-risk visual symptoms, improve early intervention, and ultimately refine treatment strategies for patients presenting with primary intracranial mass lesions in this region.
Methods
Study design and patient selection
This study was designed as a single-center, retrospective observational case series conducted at the Neuro-ophthalmology Department of Chi Mei Medical Center in Tainan, Taiwan. The study conducted a review of electronic medical records for all eligible patients who presented with visual disturbances between January 2021 and August 2023. The study cohort comprised 13 consecutive patients who met the eligibility criteria. Inclusion criteria included patients aged 18 years or older, those who have initially presented to the ophthalmology clinic with a primary visual or ocular complaint, and those who have subsequently received a definitive diagnosis of a primary intracranial mass lesion confirmed by neuroimaging and/or histopathology. Furthermore, the availability of complete medical records and follow-up data was required for study enrollment. Patients were consecutively enrolled to minimize potential selection bias. Exclusion criteria included patients younger than 18 years, those diagnosed with secondary or metastatic intracranial lesions, or those with incomplete ophthalmologic data.
Ethical considerations
The study protocol strictly adhered to the principles of the Declaration of Helsinki (1975, as revised in 2024). To ensure patient confidentiality, all patient health data were anonymized prior to analysis. The Institutional Review Board (IRB) of Chi Mei Medical Center reviewed and approved the study protocol (IRB No. 11204-007) and granted an exemption from the requirement for informed consent due to the retrospective chart-review design.
Data collection and definitions
Data were meticulously extracted by HWH and WJAL using a standardized abstraction form. Collected variables included demographic data (age and sex) and clinical information, including the duration of visual complaints. Initial ocular complaints were broadly defined to include primary visual disturbances (e.g. blurred vision, decreased visual acuity, diplopia, photopsia, and metamorphopsia) and associated complaints (e.g. periorbital or ocular pain). All patients underwent comprehensive ophthalmologic and neuro-ophthalmologic examinations. These examinations included measurement of best-corrected visual acuity (BCVA), which was subsequently converted to the logarithm of the minimum angle of resolution (LogMAR) for analysis; intraocular pressure (IOP) assessed using Goldmann applanation tonometry; and visual field (VF) testing performed using standard automated perimetry (Humphrey Field Analyzer, Carl Zeiss Meditec, Dublin, CA).
Diagnostic confirmation and outcomes
Neuroimaging, predominantly magnetic resonance imaging (MRI), was used to confirm the diagnosis, determine tumor location, and assess tumor size and characteristics. To ensure diagnostic accuracy, MRI findings were cross-referenced and reviewed by both a neuroradiologist and a neurosurgeon. For patients who underwent surgical intervention, histopathologic reports were obtained to classify the tumor type according to the latest World Health Organization grading system and to confirm the diagnosis. Treatment approaches (e.g. surgery and radiotherapy) and the final visual outcomes, recorded at the most recent follow-up visit, were documented as primary outcome measures. Each patient’s complete medical record was reviewed from the time of initial presentation through the most recent hospital visit across all clinical departments within the institution to ensure comprehensive outcome ascertainment.
Statistical analysis and reporting standards
Descriptive statistics were utilized to summarize cohort characteristics. Continuous variables were reported as mean ± SD or median with interquartile range, as appropriate. Categorical variables were presented as frequencies and percentages. Given the small sample size (n = 13), analyses were strictly descriptive, and no inferential statistical testing was performed. The reporting of this case series follows the recommendations of the Case Report (CARE) guidelines, 5 which emphasize completeness and transparency in the reporting of patient-level data essential for small case series.
Results
Patient demographics and tumor characteristics
A total of 13 patients (N = 13) with primary intracranial mass lesions who presented with neuro-ophthalmic manifestations were included in this retrospective study. The cohort demonstrated a nearly balanced sex distribution, comprising seven females and six males. The mean age at diagnosis was 45.15 ± 13.10 years, with an age range of 18–68 years (Table 1). The most common underlying pathology was pituitary adenoma (five cases, 38.5%). Notably, three of these pituitary adenomas were classified as macroadenomas, indicating a higher likelihood of compressive effects. The remaining cases represented a diverse spectrum of tumor types, including meningiomas (atypical, n = 2; microcystic, n = 1), craniopharyngiomas (n = 2), and single cases of vestibular schwannoma (acoustic neuroma), Schwannoma, and cavernous malformation (Figure S1).
Basic information of each patient.
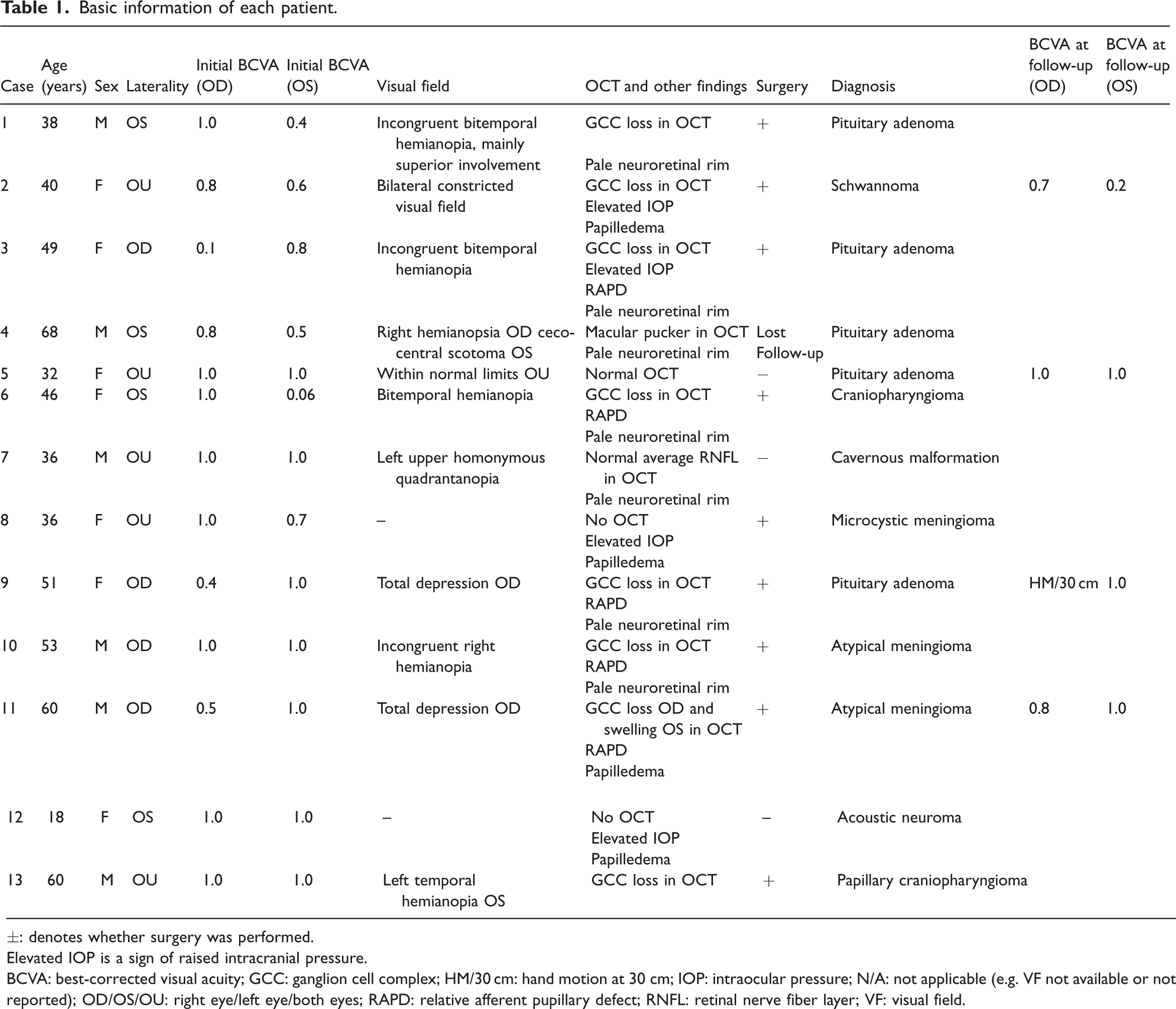
±: denotes whether surgery was performed.
Elevated IOP is a sign of raised intracranial pressure.
BCVA: best-corrected visual acuity; GCC: ganglion cell complex; HM/30 cm: hand motion at 30 cm; IOP: intraocular pressure; N/A: not applicable (e.g. VF not available or not reported); OD/OS/OU: right eye/left eye/both eyes; RAPD: relative afferent pupillary defect; RNFL: retinal nerve fiber layer; VF: visual field.
Presenting symptoms and visual acuity
At the initial visit, visual disturbances constituted the predominant subjective complaints (Figure 1). Five patients reported bilateral symptoms at presentation. Blurred vision was the most frequently reported complaint, affecting eight patients (61.5%). Other reported symptoms included pain (n = 3, consisting of ocular and periorbital types), floaters (n = 2), and isolated reports of metamorphopsia, convergence difficulty, and photopsia.
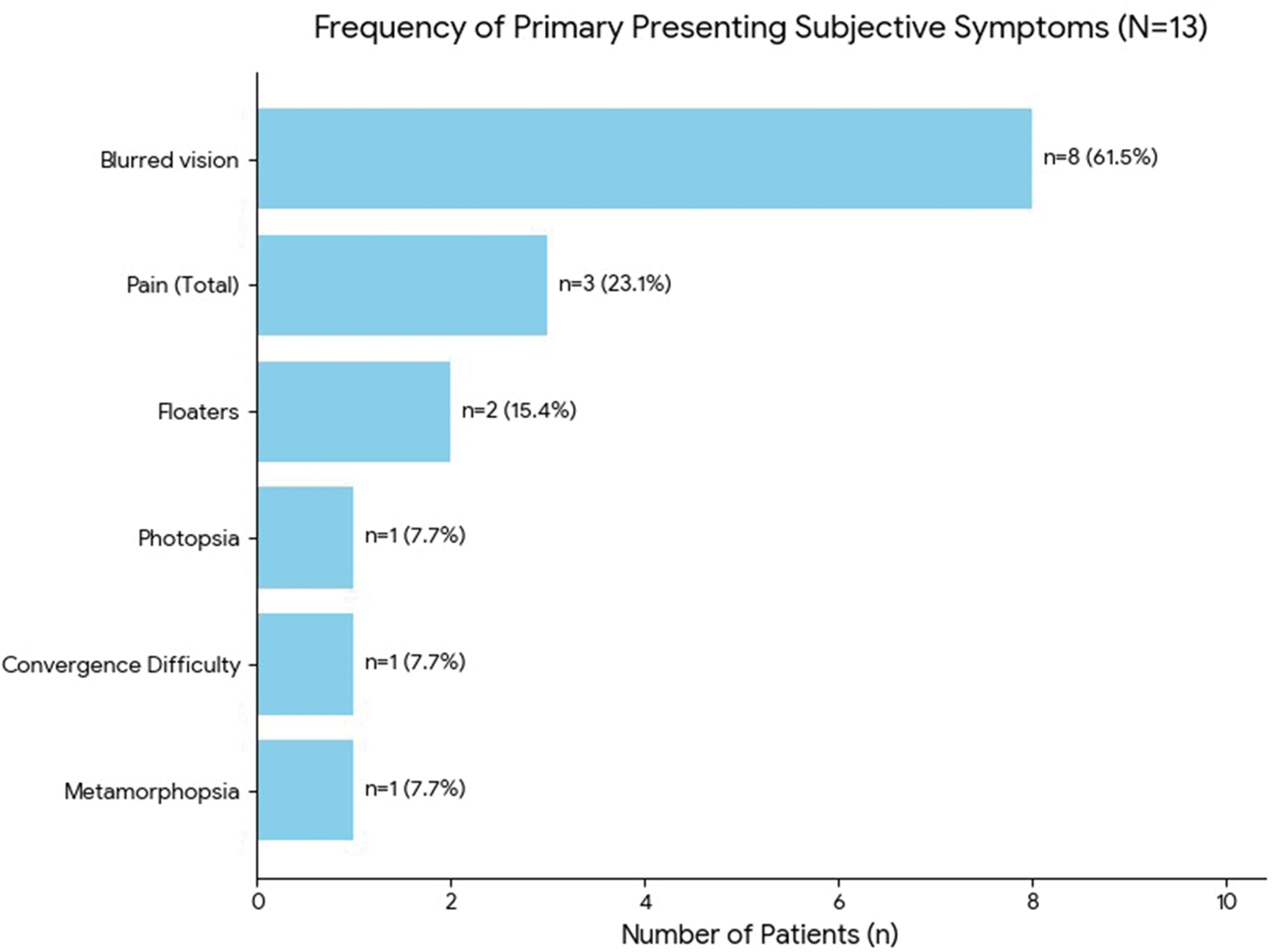
Presenting signs and symptoms for each patient. The chart uses the highest-level categories. The “Pain (Total)” category combines “Periorbital” and “Ocular” pain (1 + 2 = 3 patients). Each bar is labeled with both the absolute number of patients (n) and the corresponding percentage, clarifying the magnitude of each complaint. Blurred vision accounted for 61.5% of initial complaints.
Initial BCVA across all affected eyes demonstrated a wide range (Snellen: 0.06 to 1.0). Although most patients maintained relatively good visual acuity, two patients exhibited profound impairment, with BCVA less than 0.1 (LogMAR 1.0) in the affected eye, indicating a wide spectrum of visual impairment severity at presentation.
Objective ophthalmic findings
Comprehensive ophthalmological examinations revealed a high prevalence of objective visual pathway involvement (Figure 2, Table 1).
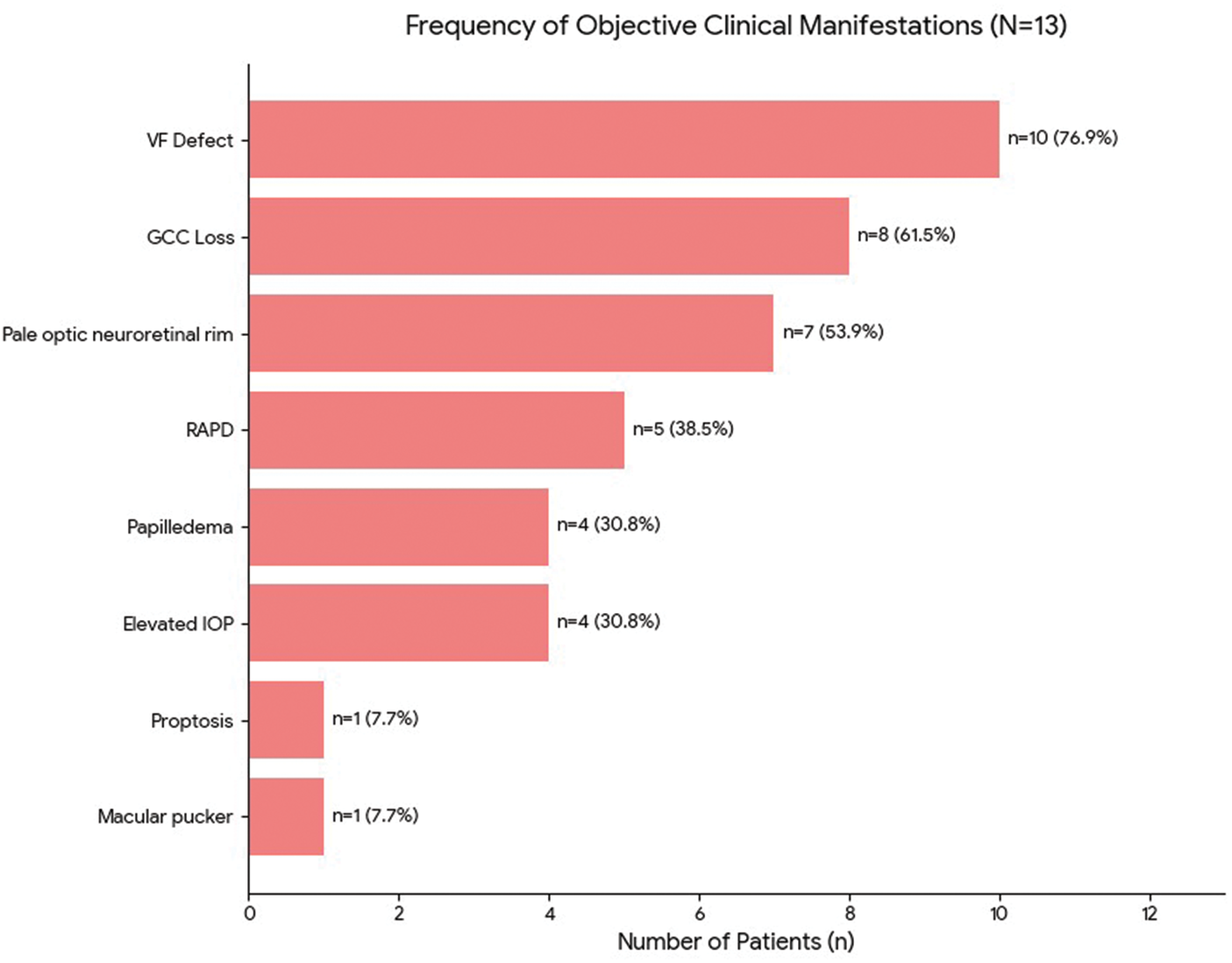
Clinical manifestations of each patient. Visual field (VF) defect was the most common objective sign, found in 10 of the 13 patients (76.9%). Ganglion cell complex (GCC) loss was the second most frequent finding, observed in eight patients (61.5%), indicating structural damage to the retina’s inner layers. Pale optic neuroretinal rim was noted in seven patients (53.8%). GCC: ganglion cell complex; IOP: intraocular pressure; RAPD: relative afferent pupillary defect; VF: visual field.
VF defects were the most common objective finding, identified in 10 patients (76.9%). These defects were diverse, including bitemporal hemianopia, homonymous hemianopia, quadrantanopia, and total depression, underscoring the varied locations of compression along the visual pathway.
Evidence of structural optic nerve damage was prevalent. Ganglion cell complex (GCC) loss on optical coherence tomography (OCT) was detected in eight patients (61.5%). This structural loss was frequently corroborated by fundoscopy, which revealed the presence of a pale optic neuroretinal rim in seven patients (53.8%), suggesting chronic involvement anterior to the lateral geniculate body. Furthermore, signs of elevated intracranial or intraorbital pressure were noted, with papilledema and elevated IOP each identified in four patients (30.8%).
Treatment and visual outcomes
Overall, 10 of the 13 patients (76.9%) underwent surgical intervention. Three patients were managed with regular checkups due to relatively favorable initial BCVA—two were diagnosed with pituitary microadenoma (a subtype of pituitary adenoma), and one with cavernous malformation. Unfortunately, six patients were lost to follow-up immediately after their initial diagnosis.
Follow-up BCVA data were available for five patients (Cases 2, 5, 9, 11, and one additional patient from the cohort based on the previous data, although only three cases were detailed in the prognosis section provided). Outcomes were variable: Case 11 exhibited a positive visual outcome, with the BCVA improving from 0.5 (LogMAR 0.3) to 0.8 (LogMAR 0.1) in the affected eye postoperatively, supporting the potential benefit of surgical decompression. Conversely, Case 5 demonstrated a stable, optimal BCVA of 1.0 in both eyes throughout the follow-up period under observation, confirming the efficacy of nonsurgical management for specific low-risk lesions. Less favorable outcomes were noted in Case 2, which reported mixed results with a decline in BCVA in the left eye following surgery, complicated by temporary facial palsy, and in Case 9, which suffered a severe loss of vision in the affected eye (OD: 0.4 to HM/30 cm) despite intervention. These cases underscore the complexity and potential risks associated with managing these lesions.
Presenting cases
Case 1. The patient initially presented with progressive blurred vision in the left eye over a 6-month duration. Despite a noncontributory initial ocular examination, subsequent VF testing revealed incongruent bitemporal hemianopia with predominant superior involvement (Figure S2(A)). This specific VF defect suggested compression of the optic chiasm from an inferior aspect, most commonly caused by a macroadenoma. This clinical suspicion was confirmed by MRI, which identified a pituitary macroadenoma measuring approximately 2.0 × 2.5 × 2.5 cm (Figure S2(B) and (C)). Integration of the imaging and visual findings yielded a clear etiological diagnosis consistent with the patient’s clinical presentation.
Case 2. The patient, a 40-year-old woman, presented with a history of otological symptoms—sudden hearing loss and tinnitus—that began 4 years ago and were attributed to a vestibular schwannoma originating from the cerebellopontine angle. Her recent visit was prompted by new-onset photopsia, blurred vision, and an unexplained reduction in color contrast sensitivity. Clinical examination immediately suggested optic pathway involvement, as she exhibited bilateral elevated intraocular pressure, sluggish pupillary light reflexes, and significant disc edema (Figure S3(A)). The severity of these findings was confirmed by a VF examination, which demonstrated bilaterally constricted VFs attributed primarily to papilledema (Figure S3(B)). Further investigation with MRI revealed the extent of the underlying cause, identifying a massive tumor measuring 5.2 × 3.8 × 4.6 cm. This mass caused obstructive hydrocephalus, as evidenced by dilation of the bilateral lateral ventricles and surrounding transependymal edema, resulting from compression of the brainstem and left middle cerebellar peduncle (Figure S4).
Discussion
Intracranial mass lesions often lead to progressive visual deficits that evolve over weeks or months, during which early signs and symptoms may be misinterpreted by both patients and clinicians, resulting in delays in diagnosis and treatment. 2 These lesions—which may arise in locations such as the optic nerve, pituitary gland, and cerebral cortex—can produce a wide range of visual symptoms, including blurred vision, VF defects, and elevated intraocular pressure, depending on the tumor size and location. In our study, the duration of visual symptoms before diagnosis varied widely, ranging from 1 day to 1 year. This variability highlights the challenges of early detection and emphasizes the critical need for timely diagnosis to preserve visual function. Because patients frequently present with isolated visual disturbances in the absence of overt systemic neurological symptoms, healthcare providers must maintain a high index of suspicion for intracranial mass lesions in individuals presenting with visual abnormalities.
The significance of early detection and specialized collaboration cannot be overstated. Timely diagnosis enables the prompt initiation of appropriate management, often requiring coordinated referral among neurosurgery, ophthalmology, and radiology specialties. 6 The diagnostic process relies critically on the integration of a thorough clinical evaluation, comprehensive ophthalmologic assessment, and advanced imaging, particularly MRI.
Contextualizing findings
Pituitary adenomas, which represented the most common etiology in our cohort (38.5%), frequently cause visual disturbances through compression of the optic nerve or chiasm. 7 Specific VF defect patterns, such as the classic bitemporal hemianopia resulting from compression of the crossing nasal fibers at the chiasm, are determined by the tumor’s precise location and size within the sellar region. Other VF defects, including superior quadrantanopia and monocular or homonymous defects, may also occur depending on the growth vector of the tumor.8–10 Prolonged compression may ultimately result in optic atrophy and permanent vision loss. Previous studies have emphasized the utility of GCC analysis using OCT, which can detect distinct patterns of loss (e.g. binasal, junctional, and homonymous) corresponding to VF changes, thus facilitating early detection and precise localization of compressive lesions within the anterior visual pathway.11,12
The case of vestibular schwannoma (acoustic neuroma) in our series illustrates a unique presentation. Although typically characterized by unilateral hearing loss and tinnitus,13–15 a mass effect from tumor growth can lead to visual disturbances by causing compression, resultant increased intracranial pressure, and subsequent papilledema. Our patient’s presentation with new-onset photopsia, blurred vision, papilledema, and bilateral left homonymous superior quadrantanopia was a direct consequence of the tumor size and mass effect, resulting in intracranial hypertension. 16 The 4-year interval between the patient’s initial hearing loss and the onset of visual symptom presentation highlights how prolonged these slow-growing tumors may remain undiagnosed before leading to life-threatening complications.
Study comparison and limitations
Our findings regarding patient demographics—including a comparable sex distribution (6:7) and a mean age of 45.15 years—and symptom profile align closely with reports from the international literature. For example, Masaya-Anon et al. 16 reported a similar mean patient age (43.5 years) and identified blurred vision as the most common presenting complaint (88.6% in their cohort), accompanied by a high prevalence of VF defects (80.5%) and abnormal optic disc findings (69.7%). These parallel findings reinforce the importance of comprehensive ophthalmological evaluation in patients presenting with visual disturbances. However, a key difference was observed in tumor etiology: pituitary adenoma was the most common diagnosis in our study (38.5%), whereas meningioma was the most prevalent (45%) in their cohort. 16 This discrepancy in tumor etiology may be attributed to two primary factors: first, nearly half of our cases were diagnosed solely based on neuroimaging findings rather than histopathological confirmation; and second, potential referral bias, as our study was conducted in an ophthalmology clinic, which is more likely to encounter patients with chiasmal compression (e.g. pituitary adenomas) presenting with primary visual loss complaints.
Furthermore, comparisons with studies of pediatric brain tumors reveal distinct patterns. 17 Children demonstrate a higher prevalence of extraocular movement (EOM) disorders (approximately 66%) and papilledema (44.1%–52.4%), findings that are often associated with the increased incidence of infratentorial tumors. In contrast to adults, only a small proportion of pediatric patients (8.6%) report blurred vision as the initial presenting symptom. These observations suggest that EOM disorders and VF abnormalities may represent more prominent primary manifestations in the pediatric population.
Several limitations should be considered when interpreting these findings. First, the small sample size (N = 13) inherently limits the statistical power and generalizability of the study findings. Second, the retrospective study design introduces potential risks of missing data, recall bias regarding symptom duration, and selection bias, as patients were recruited from a single ophthalmology clinic. This recruitment process likely skewed the cohort toward tumors that primarily manifest with visual symptoms, particularly chiasmal lesions. Third, the use of the Landolt C chart for visual acuity assessment—common in Taiwan—rather than the standardized Snellen chart introduces measurement variability and hinders direct comparability with studies using different standard charts. Finally, the considerable loss to follow up (six patients) and the absence of long-term visual acuity and VF data for many others—particularly those followed exclusively by neurosurgery—severely restrict our ability to comprehensively evaluate long-term treatment outcomes and progression of visual function. These limitations highlight the critical need for enhanced interdepartmental collaboration between neurosurgery and ophthalmology to ensure comprehensive patient monitoring.
In summary, our findings reinforce that visual symptoms represent critical and frequently early indicators of intracranial mass lesions. Although this retrospective observational study cannot infer causality, the results highlight vital clinical patterns that merit further investigation in larger, prospective cohorts.
Conclusion
Visual symptoms should be recognized as early indicators of intracranial mass lesions, necessitating thorough ophthalmologic and neuroimaging evaluations to preserve vision and optimize patient outcomes. Our study emphasizes the critical role of these assessments, particularly in patients for whom visual disturbances constitute the primary presenting complaint. The wide age range and near-equal sex distribution observed in our cohort highlight the need for diagnostic vigilance across diverse populations. Our findings demonstrate the critical importance of strengthening collaboration among ophthalmology, neurology, and neurosurgery to ensure comprehensive evaluation and management.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251410426 - Supplemental material for Seeing the unseen: A case series of intracranial mass lesions initially presenting with visual disturbances
Supplemental material, sj-pdf-1-imr-10.1177_03000605251410426 for Seeing the unseen: A case series of intracranial mass lesions initially presenting with visual disturbances by Huai-Wen Hsu, Tim Yi-Ting Chen, Shu-Chun Kuo and Wan-Ju Annabelle Lee in Journal of International Medical Research
Footnotes
Acknowledgments
The authors thank the research staff of the Chi Mei Medical Center for their assistance in data collection. Portions of this manuscript were edited for clarity and grammar using AI-assisted language tools (ChatGPT and OpenAI), with all interpretations and conclusions made solely by the authors.
Author contributions
H-S.H., W.-J. A. L., S.-C.K., and T. Y.-T. C. conceived and designed the experiments. H-S.H., S.-C.K., and W.-J. A. L. collected the case data. H-S.H., T. Y.-T. C., and W.-J. A. L. analyzed the data. H-S.H., W.-J. A. L., S.-C.K., and T. Y.-T. C. wrote the paper. All authors reviewed the manuscript. The authors read and approved the final manuscript.
Availability of data and materials
The presented data in this study are available from the corresponding authors upon reasonable request.
Declaration of conflicting interests
All authors declare no conflict of interest.
Ethics approval and informed consent
This study was approved by the Institutional Review Board at Chi Mei Medical Center (11204-007). The requirement for informed consent was waived due to the retrospective nature of the study. Signed consent may not be required for retrospective studies.
Funding
Part of the APC fee will be funded by Chi Mei Hospital Research Center if accepted (CMFHR114005). The funding source had no role in the design, analysis, interpretation, or reporting of results, or in the decision to submit the manuscript for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.