
Abstract
Objective
To evaluate the effect of virtual reality on pain and anxiety during sedation-free colonoscopy in adults aged 18–70 years.
Methods
In this randomized controlled trial, patients were assigned to either a virtual reality group or a control group. The primary outcomes were pain, measured using the visual analog scale, and anxiety, assessed using the self-rating anxiety scale. Secondary outcomes included vital signs, procedural success and duration, patient satisfaction, virtual reality acceptability, and willingness to undergo future colonoscopies.
Results
Compared with the control group, the virtual reality group showed significantly lower pain, anxiety, heart rate, and blood pressure during the procedure (all p < 0.05). No significant differences were observed in respiratory rate, cecal intubation time, or total procedure duration (p > 0.05). Insertion success rates were identical. Importantly, a higher proportion of virtual reality participants expressed willingness to undergo future colonoscopies (p < 0.05), a patient-centered outcome relevant to screening adherence.
Conclusion
Virtual reality effectively reduces pain and anxiety during colonoscopy without compromising procedural outcomes. The inclusion of both subjective and physiological measures strengthens the evidence supporting the effects of virtual reality.
Trial registration: This randomized controlled trial was retrospectively registered in the Chinese Clinical Trial Registry (ChiCTR; registration number ChiCTR2400079076).
Introduction
Colorectal cancer (CRC) is among the leading causes of cancer-related morbidity and mortality worldwide. Early detection through systematic screening can substantially reduce disease incidence and improve survival outcomes. 1 Colonoscopy, which allows both visualization and removal of precancerous lesions, remains the reference standard for CRC prevention. 2 However, screening uptake in China is suboptimal. A nationwide cross-sectional survey conducted between 2012 and 2015 among 182,927 high-risk individuals revealed that only 25,593 completed the recommended colonoscopy, resulting in an overall participation rate of 14.0%. 3
Procedural pain refers to a sensory and emotional response triggered by actual or anticipated tissue injury. 4 Consequently, invasive medical procedures such as lumbar puncture, tracheal intubation, and surgery commonly evoke varying degrees of pain. Colonoscopy is often perceived as an invasive, painful, and uncomfortable procedure. Several factors contribute to this discomfort, such as looping of the colonoscope, sustained gas insufflation, pressure applied during scope advancement, the patient’s individual pain threshold, and the need for external abdominal compression. 5
In addition to physical discomfort, colonoscopy frequently induces emotional distress, manifested as anxiety, fear, or embarrassment. Anxiety can be defined as a state of heightened apprehension regarding potential negative outcomes. 6 During colonoscopy, such anxiety may result from prolonged immobility, awkward body positioning, exposure-related embarrassment, anticipation of diagnostic results, and fear of procedural pain. 7
Both pain and anxiety can compromise cooperation between patients and endoscopists, leading to longer examination times and procedural difficulties. Furthermore, negative experiences related to pain and anxiety often discourage patients from returning for future screenings.8,9 These psychological and physical barriers are major contributors to the low participation rates in CRC screening. Consequently, interventions that alleviate such factors—such as virtual reality (VR)—have the potential to improve the overall patient experience, fostering a more positive perception of the procedure and promoting higher rates of adherence to future screenings. Because reluctance to undergo repeat screening is primarily driven by discomfort and emotional distress, effectively managing these factors is essential for improving patient tolerance and compliance.
The conventional approach to reducing pain and anxiety during colonoscopy involves analgesia and sedation. Recently, there has been growing interest in nonpharmacologic strategies aimed at improving patient experience. These include auditory stimulation techniques, such as binaural beats, as well as music therapy and visual distraction methods.10–12
VR creates immersive, multi-sensory environments that engage patient’s attention and can redirect it away from procedural discomfort. 13 This distraction not only alleviates immediate pain and anxiety but also helps reshape the patient’s overall perception of the procedure, potentially increasing adherence to future screenings. By improving the immediate colonoscopy experience, VR may foster a sense of control and comfort, reduce fear of subsequent procedures, and encourage repeat screenings. Prior research has demonstrated the efficacy of VR across various clinical contexts. Czech et al. 14 reported that VR distraction effectively mitigated needle-related pain in pediatric patients. Luo et al. 15 found that the additional use of VR significantly reduced pain intensity in burn patients undergoing physical therapy. Chirico et al. 16 showed that VR decreased anxiety and improved mood in breast cancer patients receiving chemotherapy. Turoń-Skrzypińska et al. 17 conducted a study among 85 patients undergoing chronic hemodialysis and suggested that VR can reduce the occurrence of anxiety and depressive symptoms in this patient group.
As this trial represents an initial exploratory evaluation of VR during colonoscopy, enrollment was restricted to adults aged 18–70 years to ensure feasibility and safety. VR requires wearing a head-mounted display and maintaining engagement with immersive visual content, which may be more challenging for individuals aged over 70 years and could lead to intolerance, such as dizziness or difficulty communicating discomfort. This age restriction reflects a practical consideration for this early-stage investigation and defines the population to which the present findings are most applicable while acknowledging that future studies specifically designed for older adults are warranted.
Given the encouraging results of VR in other medical procedures, we hypothesized that this technology could also enhance patient comfort during colonoscopy. Accordingly, the present study aimed to assess the effect of VR on patients’ pain and anxiety during unsedated colonoscopy. In addition, we hypothesized that by improving the procedural experience through reduction of pain and anxiety, VR could enhance patients’ willingness to undergo repeat colonoscopy and, consequently, participation in CRC screening.
Although previous randomized controlled trials have suggested that VR can effectively alleviate pain and anxiety during colonoscopy and improve patient satisfaction, most were limited by small sample sizes or narrow inclusion criteria.18–20 Furthermore, little is known about whether VR can influence long-term screening behavior, such as adherence to repeat colonoscopy. Objective assessments of physiological correlates of anxiety—including heart rate, blood pressure, and respiratory rate—are also scarce. To address these gaps, we conducted a randomized controlled trial incorporating both subjective patient-reported outcomes and objective physiological indicators, enabling a more comprehensive evaluation of VR’s effects during sedation-free colonoscopy. Secondary analyses explored its potential impact on willingness to undergo repeat procedures.
Methods
Study design and population
This trial strictly adhered to the Consolidated Standards of Reporting Trials (CONSORT) recommendations. 21 The protocol was retrospectively registered in the Chinese Clinical Trial Registry (ChiCTR; registration number ChiCTR2400079076) on 26 September 2025. The complete study protocol and detailed trial information are publicly accessible at https://www.chictr.org.cn/showproj.html?proj=190776.
We conducted a single-center, randomized, parallel-group, superiority trial at the Endoscopy Center of the Affiliated Hospital of Hangzhou Normal University, China. The study was performed in full compliance with the ethical principles of the Declaration of Helsinki (as revised in 2024) and received approval from the Institutional Review Board of the Affiliated Hospital of Hangzhou Normal University, Hangzhou, China (Approval No. 2022(ES)-HS-109, Date: 28 June 2022). Patients and members of the public were not involved in the design, implementation, or reporting of this trial.
Sample size calculation
The sample size was calculated a priori using PASS 15.0 software. Estimates were based on pain scores reported by Karaveli et al., 19 in which the mean visual analog scale (VAS) pain scores were 2.76 ± 1.25 in the VR group and 3.76 ± 2.11 in the control group. A two-sided significance level (α) of 0.05 and a power (1–β) of 0.90 were assumed. The calculation indicated that 65 participants per group (130 in total) would be required. To account for potential dropouts, 200 patients were screened for enrollment.
Participants
From May 2023 to February 2024, 200 patients scheduled for colonoscopy who preferred sedation-free procedures were screened for eligibility. Patients who maintained this preference and were deemed suitable candidates by the attending endoscopist were invited to participate. Written informed consent was obtained from all participants prior to enrollment. The inclusion criteria were as follows: (a) adults aged 18–70 years and (b) American Society of Anesthesiologists physical status I or II. The exclusion criteria were as follows: (a) visual or hearing impairment; (b) mental disorders; (c) epilepsy; (d) brain damage; and (e) motion sickness. Participation was voluntary, and withdrawal at any time did not affect standard medical care. Of the 200 patients screened, 27 were excluded prior to randomization (24 due to age >70 years and 3 due to a history of motion sickness), resulting in the enrollment of 173 participants in the study.
Withdrawal criteria
Participants could be removed from the study if they met any of the following criteria: (a) withdrawal of consent; (b) the colonoscopy was cancelled; (c) serious adverse events occurred during the procedure, making continuation inappropriate; or (d) their clinical condition deteriorated. Participants retained the right to withdraw from the trial at any time. All withdrawals and the corresponding reasons were recorded by the investigators.
Randomization and allocation concealment
Eligible participants were randomly assigned in a 1:1 ratio to either the VR or control group (without VR) using a computer-generated randomization sequence. The randomization sequence was prepared by a physician who was not involved in participant recruitment or procedures. Group assignments were concealed in opaque envelopes, which were opened after enrollment to determine allocation. Due to the nature of the intervention, blinding of participants and endoscopists was not feasible. However, the data analyst remained blinded to group allocation.
Interventions
All participants received standard bowel preparation, and instructions for using the VR headset were provided approximately 20 min before their scheduled appointments. Colonoscopies were performed using an Olympus colonoscope (GIF-Q290, Olympus, Tokyo, Japan) by three expert endoscopists, each with experience of more than 20,000 procedures.
In the VR group, participants wore a PICO 4 all-in-one VR headset (Beijing Digibird Technology Co., Ltd., China; cost of approximately US$305). The device operated independently and displayed one of the three immersive nature videos (15–20 min each), featuring natural sceneries such as Mount Qomolangma, Hawaiian beaches, or the Amazon rainforest, accompanied by relaxing music (e.g. River Flows in You or Endless Horizon). Technical parameters of the VR system—including display resolution, frame rate, and field of view—were standardized across participants and are detailed in the Supplementary Appendix.
Before the procedure, nurses assisted in adjusting the headset for fit, brightness, and volume to ensure participant comfort and clear communication. The immersive audiovisual experience lasted from intubation to scope withdrawal.
Participants in the control group underwent colonoscopy without VR, following the same technical and nursing standards. No sedatives or analgesics were administered in either group. Both interventions were delivered as intended, and all participants completed the assigned procedures without major deviations from the study protocol.
Outcomes
The primary outcomes were pain and anxiety during sedation-free colonoscopy. Secondary outcomes included patient satisfaction, cecal intubation rate and time, willingness to undergo repeat colonoscopy, and acceptance of the VR headset. Objective physiological parameters—heart rate, blood pressure, and respiratory rate—were also recorded as correlates of procedural stress and anxiety.
Measurement instruments
Pain was assessed using a validated VAS. Anxiety was evaluated using the self-rating anxiety scale (SAS). Objective physiological parameters, including heart rate, blood pressure, and respiratory rate, were continuously monitored using an electrocardiography (ECG) monitor and automated cuff manometer. These parameters reflect autonomic responses to procedural pain and anxiety 22 and were recorded at baseline and during cecal intubation.
Patient satisfaction and willingness to undergo future colonoscopy were measured using 11-point Likert scales (0–10). Acceptance of the VR headset was recorded using a four-point scale: “very good,” “good,” “fair,” or “poor.”
Data collection and outcome assessment
On the day of their colonoscopy appointment, all patients received an introduction to the purpose and procedure of the study. Baseline data, including demographics such as name, age, and sex as well as colonoscopy indications, history of previous abdominal surgeries, and number of prior colonoscopies, were collected using a standardized form and are presented in Table 1.
Baseline characteristics.
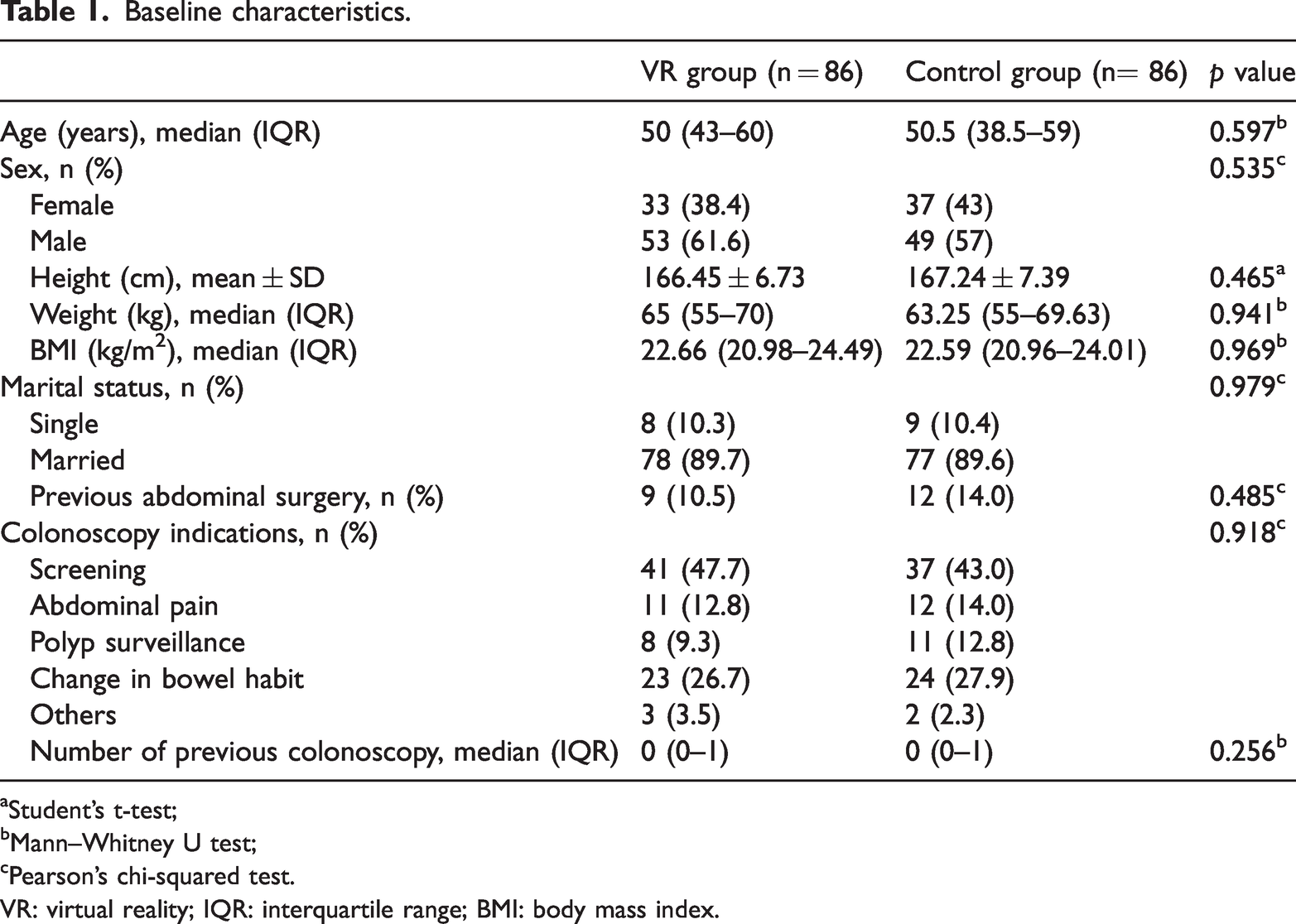
Student’s t-test;
Mann–Whitney U test;
Pearson’s chi-squared test.VR: virtual reality; IQR: interquartile range; BMI: body mass index.
During the preprocedural waiting period, patients rested quietly for at least 5 min before their respiratory rate, heart rate, and blood pressure (systolic and diastolic) were measured by trained nurses.
Each participant completed two validated questionnaires: the 10-cm VAS 23 for pain and SAS 24 for anxiety assessment. The SAS consists of 20 self-report items scored on a 4-point Likert scale (1 = rarely to 4 = most always). Standardized scores were derived by multiplying raw scores by 1.25 and interpreted as follows: <50, no anxiety; 50–59, minimal-to-mild anxiety;60–69, moderate-to-marked anxiety; >70, severe anxiety.24,25 The SAS was administered before the procedure to assess baseline anxiety over the preceding week. During the colonoscopy, respiratory rate, heart rate, and blood pressure were monitored continuously using an ECG monitor and cuff manometer. A trained nurse recorded the physiological parameters used for analysis at the time of cecal intubation, when the endoscopist successfully reached the cecum. Successful cecal intubation was confirmed by visualization of the appendiceal orifice and ileocecal valve. 26 The procedure was considered successful when the cecum was reached and adequate visualization of the cecal lumen was achieved. Cecal intubation time, total procedure duration, and success of cecal intubation were documented.
After completing the colonoscopy, patients immediately rated their pain and anxiety experienced during the procedure using VAS and SAS within 10 min before leaving the examination room. The SAS was re-administered in an adapted format to capture participants’ subjective anxiety related to the procedure, recognizing that it is not specifically designed to assess immediate state anxiety and was therefore used in an exploratory manner. In addition, two 11-point Likert scales were used to assess satisfaction with the procedure and willingness to undergo future colonoscopy (0 = not at all satisfied/willing; 10 = extremely satisfied/willing).
All data were recorded on paper forms, either completed directly by patients or documented by nurses. Reasons for withdrawal were systematically recorded.
Statistical analysis
All data were analyzed using Statistical Package for Social Sciences (SPSS), version 27.0 (IBM, Armonk, NY, USA). The Shapiro–Wilk test was applied to assess the normality of data distribution. Continuous variables were presented as mean ± SD or median (interquartile range (IQR)), as appropriate, and categorical variables were presented as frequency (percentage). Inter-group comparisons of normally distributed data were performed using the unpaired Student’s t-test, while the Mann–Whitney U test was used for non-normally distributed data. Pearson’s chi-squared test was applied to assess differences in categorical variables. Two-sided p values <0.05 were considered statistically significant. In addition to hypothesis testing, effect sizes were calculated to quantify the magnitude of between-group differences. For normally distributed continuous variables, Cohen’s d with 95% confidence intervals (CI) was reported. For non-normally distributed continuous variables analyzed using the Mann-Whitney U test, effect sizes were expressed as the rank biserial correlation coefficient (r). Effect sizes are reported alongside p-values in Tables 2 to 4.
Comparison of pain and anxiety scores according to groups.
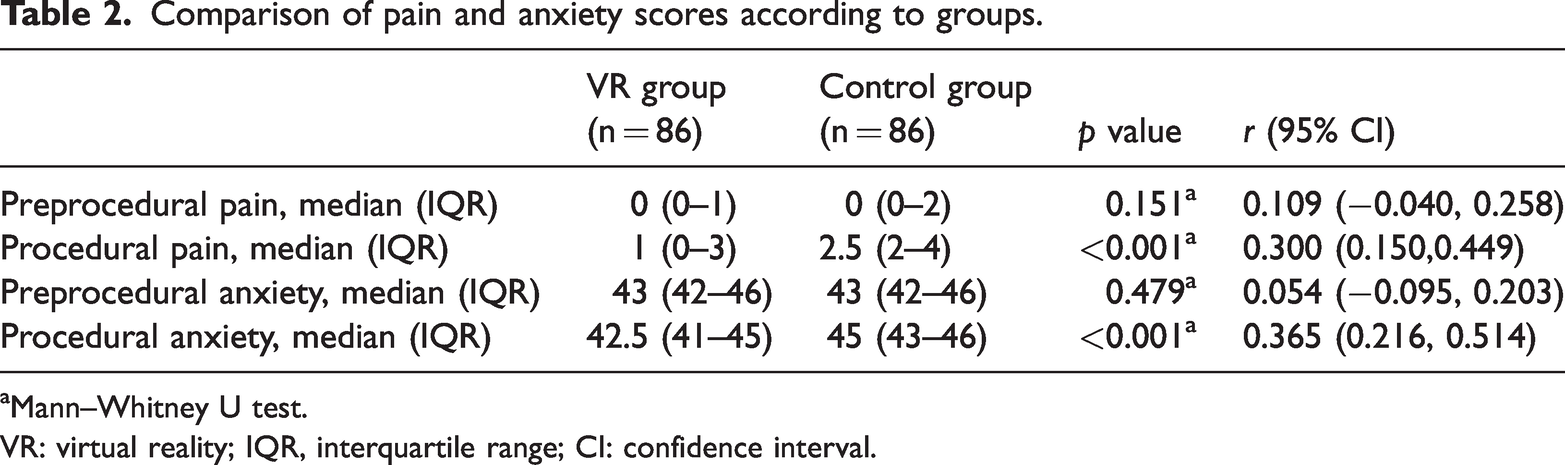
Mann–Whitney U test.
VR: virtual reality; IQR, interquartile range; CI: confidence interval.
Outcomes of colonoscopy procedure.

Mann–Whitney U test.
VR: virtual reality; IQR: interquartile range; r: rank biserial correlation coefficient; CI: confidence interval.
Only one participant withdrew after randomization due to height-related discomfort triggered by the VR scene. Because this missing observation was unrelated to pain, anxiety, or physiological outcomes and represented a negligible proportion of the data (<1%), no imputation was performed. A qualitative sensitivity assessment was planned to evaluate any potential impact.
Pain and anxiety were defined a priori as the trial’s primary outcomes. Secondary exploratory outcomes included physiological parameters (heart rate, systolic and diastolic blood pressure, and respiratory rate), procedural indicators, and satisfaction-related measures. As these endpoints were exploratory in nature, no formal adjustment for multiple comparisons (e.g. Bonferroni correction) was applied; consequently, results from secondary analyses should be interpreted as hypothesis-generating.
No harms were assessed, as the VR intervention was noninvasive and not expected to cause adverse effects.
Results
A total of 200 patients were enrolled in the study (Figure 1). Of these, 24 patients aged over 70 years and 3 patients with a history of motion sickness were excluded before randomization. After allocation, one patient in the VR group withdrew due to fear of heights triggered by a VR scene depicting a cliff; this participant’s data were excluded from the final analysis. Consequently, 172 participants (86 per group) were included in the analysis. No imputation for missing data was performed, as the withdrawal was unrelated to the intervention’s safety or efficacy, and no side effects were observed. Baseline characteristics are presented in Table 1. Among the 172 patients (mean age: 48.85 years, range: 20–70), no significant differences were observed between groups in demographic or clinical characteristics, including age, sex, height, weight, body mass index (BMI), marital status, history of abdominal surgery, colonoscopy indications, or prior colonoscopy frequency (all p > 0.05). Indications were comparable between groups (p = 0.918), with screening being the most common in both VR (47.7%, 41/86) and control groups (43.0%, 37/86). Changes in bowel habits represented the largest diagnostic subgroup (VR: 26.7%, 23/86; control: 27.9%, 24/86), followed by abdominal pain (12.8% vs. 14.0%), polyp surveillance (9.3% vs. 12.8%), and other indications (3.5% vs. 2.3%). A sensitivity assessment was conducted to evaluate the potential impact of the early withdrawal. As the participant withdrew immediately after allocation and provided no outcome data, formal inclusion in statistical analyses was not possible. The withdrawal was therefore assessed qualitatively and determined not to materially affect the direction or conclusions of the primary and secondary outcomes.
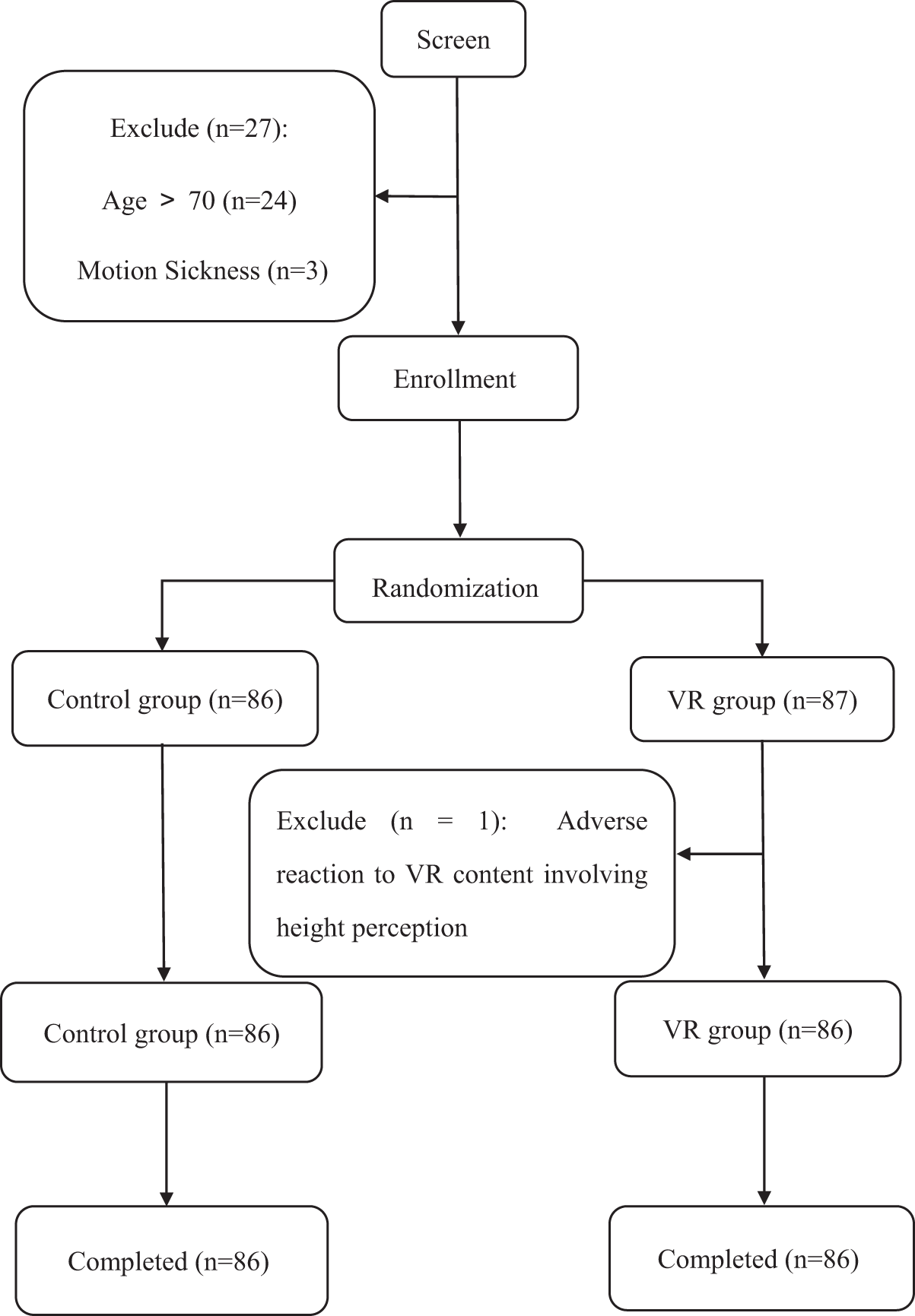
Study flowchart.
The Mann–Whitney U test was used to compare median pain and anxiety scores between the VR and control groups (Table 2). No significant differences were observed in either pain or anxiety scores between the two groups prior to the procedure (all p > 0.05), indicating comparable baseline levels. During the procedure, however, significant differences emerged. The VR group reported a significantly lower median pain score (1 (IQR, 0–3)) compared to the control group (2.5 (IQR, 2–4)) (p < 0.05). Similarly, procedural anxiety scores were significantly lower in the VR group (42.5 (IQR, 41–45)) than in the control group (45 (IQR, 43–46)) (p < 0.05). These findings indicate that the VR intervention was effective in reducing both perceived pain and anxiety during colonoscopy.
The results for vital signs are summarized in Table 3. Prior to the procedure, there were no significant differences between the VR and control groups in terms of respiratory rate, heart rate, or diastolic and systolic blood pressure (all p > 0.05), confirming comparable baseline physiological status. During cecal intubation, the VR group exhibited significantly lower systolic blood pressure (median: 119.5 vs. 132.5 mmHg, p = 0.004), diastolic blood pressure (median: 79 vs. 83 mmHg, p = 0.009), and heart rate (median: 78 vs. 82.5 bpm, p = 0.005) compared with the control group. These results suggest that VR may help attenuate the physiological stress responses commonly associated with colonoscopy.
Comparison of vital signs according to groups.
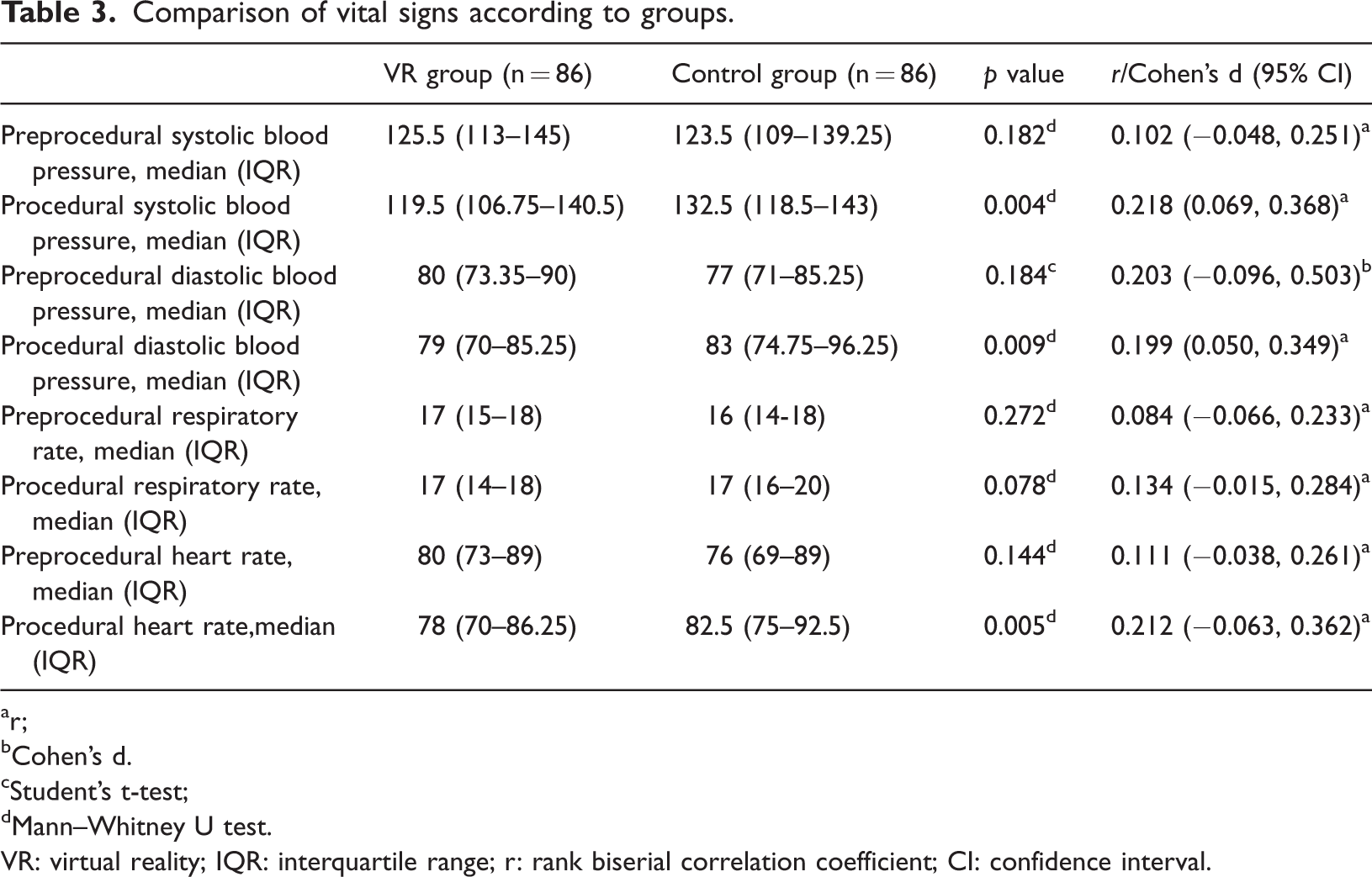
r;
Cohen's d.
Student’s t-test;
Mann–Whitney U test.
VR: virtual reality; IQR: interquartile range; r: rank biserial correlation coefficient; CI: confidence interval.
In contrast, no statistically significant difference was observed in respiratory rate during the procedure between the two groups (median (IQR), 17 (14–18) breaths/min in the VR group vs. 17 (16–20) breaths/min in the control group; p = 0.078). The identical median values and substantial overlap in distributions indicate that no clear between-group difference in respiratory rate was detectable under the current study conditions.
The success rate of colonoscope insertion was 100% in both groups (Table 4). Cecal intubation and total procedure times did not differ significantly (all p > 0.05), suggesting that VR did not affect procedural efficiency. However, the VR group reported significantly higher satisfaction with the procedure compared with the control group, with a median satisfaction score of 9 (IQR, 7–10) versus 7 (IQR, 6–9) (p < 0.001). Willingness to undergo future colonoscopy was also greater in the VR group (9 (IQR, 8–10) vs. 8 (IQR, 7–9); p = 0.009).
Acceptability of the VR experience was high. Among participants in the VR group, 44.2% rated the experience as “very good,” 48.8% as “good,” and 7.0% as “fair”; no participants rated the experience as “poor.” No adverse events or unintended effects related to the intervention were observed in either group.
Discussion
Our study evaluated the effects of VR on pain and anxiety in patients undergoing colonoscopy. We found that VR significantly reduced both pain and anxiety during the procedure, improved patient satisfaction and willingness to undergo future colonoscopies, and favorably influenced certain vital signs. Importantly, VR use was associated with comparable procedural efficiency and did not interfere with communication between endoscopists and patients. In our trial, the VR group reported a median pain score of 1 compared with 2.5 in the control group. In the context of unsedated colonoscopy, a 1.5-point reduction on the VAS may represent a clinically meaningful improvement in patient-reported pain, particularly given the low median pain scores observed. Such reductions may have important implications for patient cooperation and acceptance of the procedure.
The autonomic nervous system, comprising the sympathetic nervous system (SNS) and parasympathetic nervous system (PNS), regulates involuntary functions such as heart rate and respiration. Anxiety typically activates the SNS and suppresses the PNS, leading to physiological changes such as increased heart rate, respiratory rate, and blood pressure. 27
Our results showed that compared with the control group, patients in the VR group exhibited smaller increases in blood pressure and heart rate during colonoscopy. Acute pain and anxiety activate the SNS, leading to elevated heart rate and blood pressure, as demonstrated in previous physiological and clinical studies.28–30 Research on heart rate variability further indicates that painful stimuli alter autonomic balance, reinforcing cardiovascular parameters as objective physiological markers of pain. 30 The attenuated blood pressure and heart rate responses observed in the VR group are consistent with the reductions in subjective pain and anxiety, suggesting that VR may alleviate discomfort and stress by diverting attention and providing immersive engagement.18,31 Similar findings from other clinical trials have reported smaller procedure-related increases in cardiovascular parameters among patients receiving VR interventions, supporting its physiological calming effect during endoscopic procedures. 18 These autonomic patterns provide a physiological context for understanding the clinical implications of VR use.
Our findings are consistent with those of a randomized controlled trial by Liu et al. 20 and align with previous research exploring VR as an adjunct during colonoscopy. Vesiman et al. 32 conducted a pilot-controlled study and demonstrated that VR distraction could substitute for sedation, yielding comparable patient satisfaction, similar procedural outcomes, and faster post-procedure recovery of daily activities compared with standard sedated colonoscopy. Although their work primarily addressed the feasibility of unsedated colonoscopy using VR, our randomized controlled trial extends these observations by focusing on patient-centered outcomes, including pain, anxiety, and physiological responses. Specifically, we found that VR significantly reduced pain and anxiety scores, attenuated increases in blood pressure and heart rate, and improved patients’ willingness to undergo future colonoscopies without compromising procedure completion or duration.
In addition to the study by Vesiman et al., other studies have investigated VR in the endoscopy setting with similar conclusions. Veldhuijzen et al. 33 reported that VR distraction was well tolerated and acceptable to patients undergoing colonoscopy, without compromising procedural success. More recently, Shamali et al. 34 conducted a hybrid effectiveness–implementation trial, confirming the practicality of incorporating VR into routine endoscopy practice and emphasizing both its clinical benefits and real-world feasibility. Consistent with these reports, our trial demonstrated that VR is safe, acceptable, and effective in significantly reducing intraprocedural pain and anxiety while attenuating adverse changes in vital signs. By using pre-specified, nature-themed VR videos with relaxing music delivered uniformly to all participants, our study ensured high intervention fidelity and reproducibility, contrasting favorably with previous studies that relied on heterogeneous distraction methods. By including both subjective patient-reported outcomes and objective physiological parameters, our findings add to the growing body of evidence supporting VR as a promising nonpharmacologic adjunct to enhance patient comfort and satisfaction during colonoscopy.
Previous studies have shown that pain and anxiety are negatively correlated with patient satisfaction. Daifllah et al. 35 reported that post-treatment pain was associated with lower therapy satisfaction in patients with breast cancer. Ghobadi et al. 36 demonstrated that anxiety played a dominant role in satisfaction levels among dental implant patients, and Bello et al. 37 reported a similar relationship between perioperative anxiety and reduced satisfaction with anesthesia. In our study, VR reduced both pain and anxiety during colonoscopy, thereby improving overall patient experience. These findings are consistent with those of Veldhuijzen et al., who also demonstrated that VR increased patient satisfaction by alleviating procedural pain and anxiety. 33 Enhanced patient satisfaction with colonoscopy may encourage greater participation in future screening. Given that CRC is highly preventable and colonoscopy remains a critical tool for reducing its incidence and mortality, strategies that improve patient acceptance have significant public health implications. Notably, our study showed that VR significantly increased patients’ willingness to undergo future colonoscopies, suggesting the potential to improve CRC screening uptake.
Importantly, VR use did not affect procedural efficiency. Cecal intubation and total procedure times were comparable between groups, indicating that VR can enhance patient experience without compromising procedural success. Moreover, VR use did not interfere with communication between endoscopists and patients, preserving the integrity of intraoperative interactions.
Several previous studies have explored visual and auditory distraction during colonoscopy. Zhang et al. 11 conducted a meta-analysis of five studies and found that visual distraction alone significantly reduced patient pain and tended to lower anxiety. In a randomized controlled study, Çelebi et al. 10 provided music therapy for 30 min during colonoscopy and observed significant reductions in both pain and anxiety. Similarly, Ko et al. 38 reported that listening to music reduced anxiety levels in unsedated colonoscopy. These studies collectively demonstrate that visual or auditory interventions alone can alleviate procedural discomfort. Unlike these approaches, VR integrates both visual and auditory stimuli to create an immersive experience that effectively diverts patients’ attention. During colonoscopy, patients in the VR group appeared to focus on the virtual natural scenery rather than procedural sensations, likely contributing to their lower pain and anxiety levels. Our findings support an attention-diversion mechanism, although direct measurement of attentional processes would further strengthen this interpretation.
As a nonpharmacological intervention, VR is noninvasive, broadly accessible, and cost-effective. However, several practical considerations remain. First, how can VR be made more accessible for older patients? Second, can VR provide meaningful benefits for patients with financial constraints? Third, what is the optimal approach to achieve effective immersion? To establish the role of VR in routine endoscopic practice, further high-quality, large-scale randomized controlled trials are warranted. Future studies should particularly focus on older populations, who may benefit substantially from nonpharmacologic interventions but face unique challenges related to device use, sensory impairments, and comorbidities. This study included multiple secondary comparisons without multiplicity correction. As these analyses were exploratory, their findings should be interpreted with caution, and confirmation in future trials is warranted.
Several limitations of this study should be acknowledged. First, endoscopists were not blinded to group allocation. Although they were unaware of the study hypotheses and comparative aims and followed routine procedural protocols, blinding was not feasible due to the visible nature of the VR intervention. This lack of blinding represents a theoretical risk of performance bias, as awareness of group assignment could potentially influence procedural behavior. Future studies could address this issue by using sham headsets to achieve blinding. Second, colonoscopies were performed by three senior endoscopists, with operator assignment following routine scheduling rather than stratified allocation. Although all operators had comparable experience, residual variability related to endoscopist identity cannot be fully excluded. Third, pain and anxiety could not be assessed in real time, and post-procedure recall may have introduced bias. Anxiety was measured using the SAS, which reflects anxiety symptoms over the preceding week. Its use in this procedural context therefore represents an adapted application and may not fully capture acute state anxiety. Accordingly, procedural SAS scores in this study should be interpreted as reflecting overall procedure-related subjective anxiety rather than immediate state anxiety. However, objective physiological parameters, including heart rate, blood pressure, and respiratory rate, were continuously monitored throughout the procedure, providing complementary evidence supporting the immediate effects of VR on stress and discomfort. Fourth, some participants reported dissatisfaction with the clarity or content of the VR video, highlighting the need for high-resolution and personalized content tailored to patient preferences. Other limitations include the exclusion of patients with sensory or neurological conditions, which may limit the generalizability of our findings, and the single-center, single-country design, which may restrict applicability to other healthcare systems, endoscopy practices, and patient populations. Finally, the trial was registered retrospectively, which could raise concerns regarding outcome selection bias. Although all primary and secondary outcomes were defined prior to data analysis and no post hoc changes were made, prospective registration would have further strengthened methodological transparency.
Conclusion
This randomized controlled trial demonstrates that VR is effective in alleviating pain and anxiety during colonoscopy. As a nonpharmacological intervention, VR provides a safe and feasible approach to enhance patient comfort without compromising procedural efficiency. Furthermore, by increasing patients’ willingness to undergo future colonoscopies, VR may contribute to improved adherence to CRC screening programs.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605261417213 - Supplemental material for Effect of virtual reality on pain and anxiety during colonoscopy: A randomized control trial
Supplemental material, sj-pdf-1-imr-10.1177_03000605261417213 for Effect of virtual reality on pain and anxiety during colonoscopy: A randomized control trial by Yijie Sun, Suhui Ying, Junjun Qin, Guodong Li and Xueqing Zhong in Journal of International Medical Research
Footnotes
Acknowledgments
The authors would like to thank the endoscopy staff for their valuable assistance.
Author contributions
All authors have read and approved the final manuscript.
Study design: Xueqing Zhong; Data collection: Yijie Sun, Suhui Ying, and Junjun Qin; Statistical analysis: Xueqing Zhong; Manuscript preparation: Yijie Sun, Xueqing Zhong, and Guodong Li
Availability of data and materials
The datasets used and analyzed during this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare that they have no conflicts of interest.
Funding
This work was supported by the Natural Science Foundation of Zhejiang Province (LQ19H030002) and by special projects of science and technology supported by the development of biomedical and health industries in Hangzhou (2022WJC020).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.