
Abstract
Choroidal osteoma is a rare, benign ossifying tumor of the choroid. As the disease progresses, significant visual loss may occur. Approximately one-third of patients with choroidal osteoma develop a choroidal neovascular membrane. Choroidal neovascular membrane–associated exudation and photoreceptor disruption can lead to progressive visual decline. However, no established standard treatment exists, particularly for choroidal neovascular membrane secondary to choroidal osteoma. A healthy male in his 30s with known bilateral choroidal osteomas presented with metamorphopsia and decreased vision in his left eye. Intraretinal fluid and subretinal fluid were detected on optical coherence tomography, and an active choroidal neovascular membrane was identified on optical coherence tomography angiography. Despite monthly intravitreal anti–vascular endothelial growth factor injections of ranibizumab and aflibercept, both intraretinal fluid and subretinal fluid persisted. The treatment was therefore switched to intravitreal faricimab, resulting in complete resolution of intraretinal fluid and subretinal fluid. Furthermore, the treatment interval was successfully extended to 16 weeks without recurrence. This case suggests that faricimab may be a viable therapeutic option for choroidal osteoma secondary to choroidal neovascular membrane in selected patients. However, further studies are warranted to confirm its efficacy, durability, and safety.
Keywords
Background
Choroidal osteoma is a rare, benign ossifying tumor of the choroid that most commonly occurs in otherwise healthy young women and typically presents unilaterally. 1 Long-term visual preservation is challenging in affected patients owing to complications such as the development of a choroidal neovascular membrane (CNVM), reported in 47.7% of eyes in the series by Seong et al. 2 Reported treatments for CNVM secondary to choroidal osteoma include intravitreal anti–vascular endothelial growth factor (VEGF) therapy (commonly used as a first-line treatment), photodynamic therapy, and laser-based approaches, which may be used either alone or in combination depending on the lesion characteristics and activity.1,2
Faricimab is a dual inhibitor of VEGF-A and angiopoietin-2 (Ang-2). It was approved by the Food and Drug Administration in 2022 following investigation in the TENAYA and LUCERNE trials as a potential treatment for neovascular age-related macular degeneration (nAMD).3,4 These trials demonstrated that faricimab produced visual outcomes comparable with those of aflibercept and allowed for extended dosing intervals, thereby potentially reducing the treatment burden. 3
However, intravitreal faricimab has not been extensively evaluated as a treatment modality for CNVM secondary to choroidal osteoma. Herein, we present a case of CNVM secondary to choroidal osteoma that was successfully treated with intravitreal faricimab. Extension of the treatment interval to 16 weeks was achieved, with no CNVM reactivation over a period of 1 year.
Case report
A healthy male in his late 30s with known bilateral choroidal osteomas presented to a tertiary care hospital in Riyadh, Saudi Arabia, with complaints of decreased vision and metamorphopsia in his left eye, despite having received an intravitreal ranibizumab injection 1 month prior to presentation. The patient had previously received a loading course of intravitreal ranibizumab injections at another clinic and was subsequently maintained on monthly injections for 1 year. At presentation, his corrected Snellen visual acuity was 20/80 in the right eye and 20/60 in the left eye, with normal intraocular pressure in both eyes. Biomicroscopic examination of the anterior segment was within normal limits. Dilated fundus examination revealed bilateral juxtapapillary and macular choroidal osteomas (Figure 1(a) to (b)).
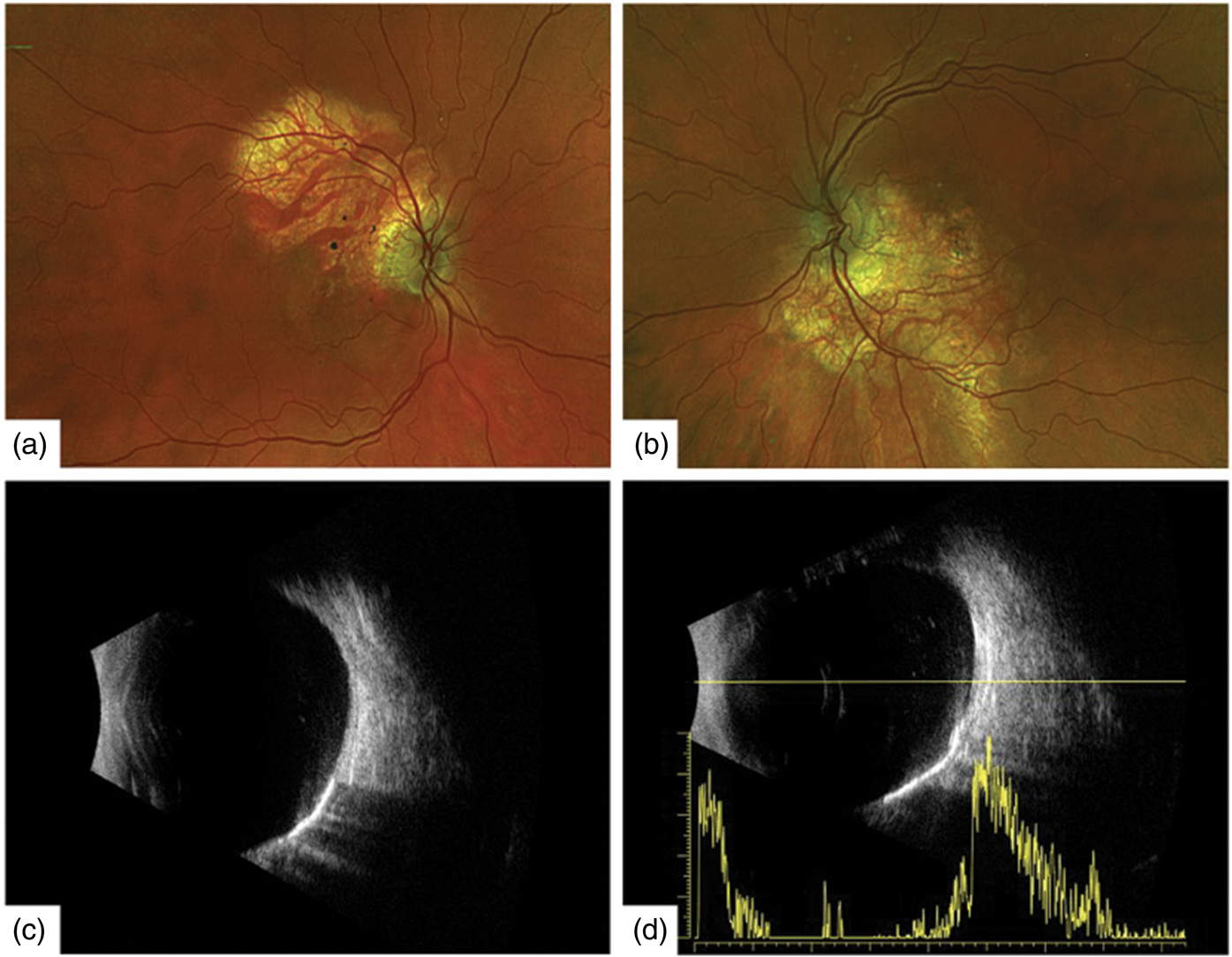
Multimodal imaging findings. (a and b) Color fundus photographs of both eyes showing juxtapapillary and macular choroidal osteomas; (c) longitudinal B-scan ultrasonography of the right eye showing juxtapapillary and macular plaque-like choroidal lesions with acoustic shadowing; (d) longitudinal B-scan ultrasonography of the left eye showing similar plaque-like choroidal lesions with acoustic shadowing; the overlaid A-scan demonstrates high-intensity echo spikes consistent with choroidal osteoma.
B-scan ultrasonography of both eyes revealed juxtapapillary and macular plaque-like lesions at the level of the choroid with acoustic shadowing (Figure 1(c) to (d)). A-scan ultrasonography revealed high-intensity echo spikes, consistent with choroidal osteoma (Figure 1(d)). Optical coherence tomography (OCT) of the right eye showed a choroidal osteoma with loss of the outer retinal layers (Figure 2(a)). OCT of the left eye demonstrated a choroidal osteoma with intraretinal fluid (IRF), subretinal fluid (SRF), and associated choroidal excavation (Figure 2(b)). Optical coherence tomographic angiography (OCT-A) was performed, which revealed a large CNVM in the left eye (Figure 3). Fluorescein angiography and indocyanine green angiography were not performed, as the results of structural OCT and OCT-A were sufficient for the diagnosis and monitoring of CNVM activity as well as for guiding management.
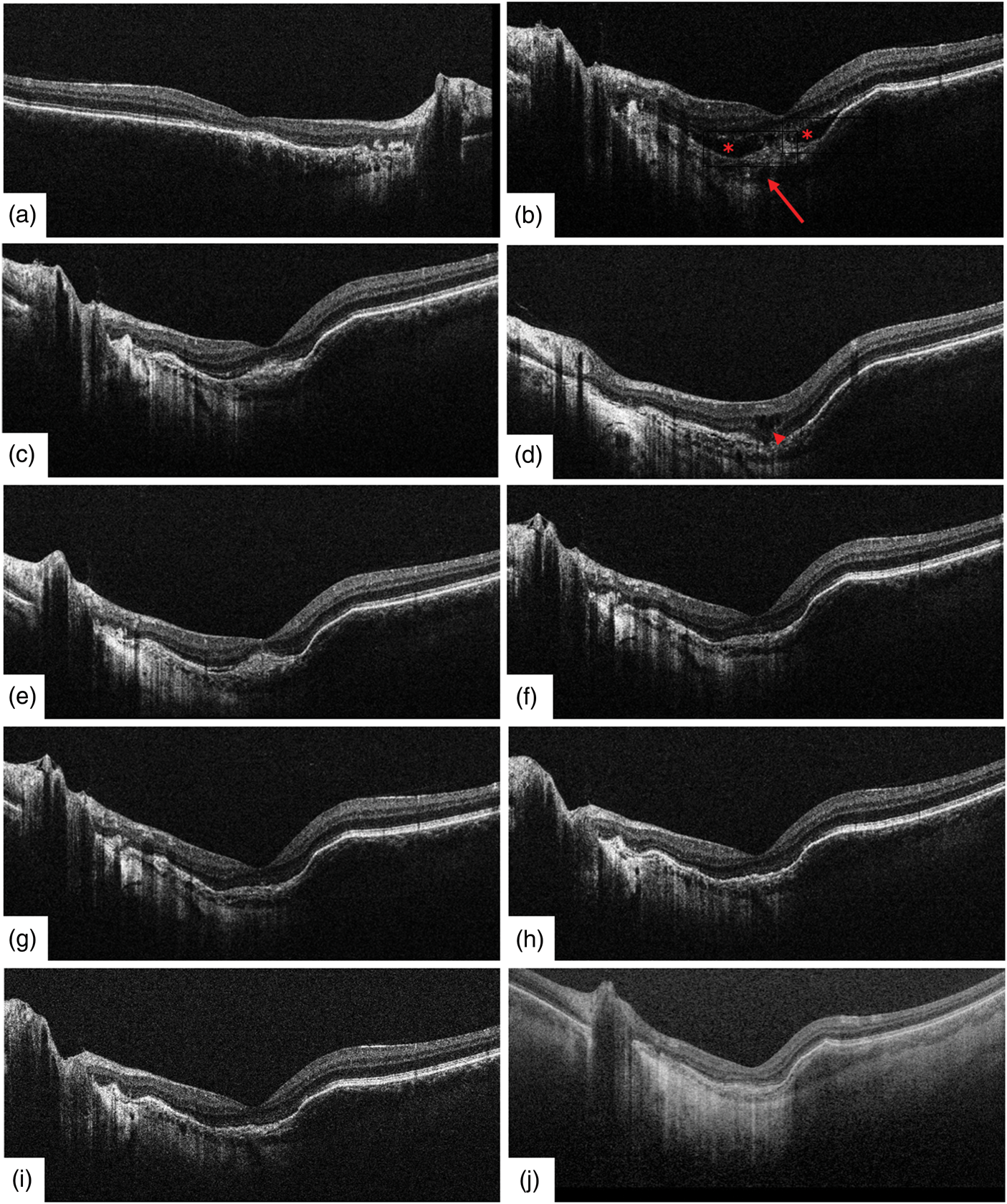
Spectral-domain optical coherence tomography (SD-OCT) findings. (a) Right macula showing choroidal osteoma with loss of the outer retinal layers; (b) left macula showing choroidal osteoma with intraretinal fluid (IRF) and subretinal fluid (SRF) (asterisk) due to choroidal neovascularization, with associated focal choroidal excavation (arrow), at baseline (1 month after ranibizumab); (c) persistent SRF 1 month after the first aflibercept injection; (d) persistent IRF (arrowhead) 1 month after the second aflibercept injection; (e) persistent SRF 1 month after the third aflibercept injection; (f to h) resolution of SRF 1 month after the first, second, and third monthly faricimab injections, respectively; (i and j) sustained resolution of IRF and SRF at 16 weeks after the third faricimab injection and at 1-year follow-up from the initiation of faricimab therapy (16-week interval), respectively.

Optical coherence tomography angiography (OCT-A) findings. Choroidal neovascularization slab image of the left macula obtained by optical coherence tomography angiography (Canon OCT-A1, version 4.6.0) showing an active choroidal neovascular membrane with abnormal flow (arrow).
The patient had not received any intravitreal injections in the right eye; however, he had been receiving monthly intravitreal anti-VEGF injections of ranibizumab (0.05 mL of a 10 mg/mL solution) in the left eye for the treatment of an active CNVM. Despite 1 year of monthly ranibizumab therapy, IRF and SRF persisted at presentation (Figure 2(b)). Subsequently, intravitreal therapy was switched to aflibercept (2 mg in 0.05 mL of a 40 mg/mL solution), and 3 monthly doses were administered. However, the response remained suboptimal, with persistent SRF (Figure 2(c) to (e)). The treatment was subsequently switched to intravitreal faricimab (6 mg in 0.05 mL of a 120 mg/mL solution). At the 4-week follow-up following the first faricimab injection, the patient reported resolution of metamorphopsia and a marked improvement in the left eye visual acuity to 20/25, which had not been achieved with prior anti-VEGF therapies. OCT demonstrated a complete resolution of IRF and SRF (Figure 2(f)). The patient subsequently received 3 monthly loading doses of intravitreal faricimab, with no recurrence of IRF or SRF (Figure 2(g) to (h)). The treatment interval was subsequently successfully extended to 16 weeks, with a continued absence of IRF or SRF (Figure 2(i)). Best-corrected visual acuity remained stable at 20/25. No ocular adverse events were reported (e.g. traumatic cataract, elevated intraocular pressure, intraocular inflammation, endophthalmitis, rhegmatogenous retinal detachment, retinal tear, retinal pigment epithelial tear, retinal vasculitis, or retinal occlusive events), and no systemic adverse events (e.g. stroke or myocardial infarction) occurred. The patient was maintained on a 16-week faricimab injection interval for 1 year, with no recurrence of IRF, SRF, or intraretinal or subretinal hemorrhage (Table 1). This case report adhered to the principles of the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of Princess Nourah Bint Abdulrahman University (IRB Approval Number: 24-0907; Approval Date: 1 December 2024). Written informed consent was obtained from the patient for both treatment and publication, and all patient data were fully deidentified to ensure anonymity. The reporting of this study conforms to the Case Report (CARE) guidelines. 5
Timeline of clinical visits and treatments administered, with visual acuity and optical coherence tomography (OCT) findings.

Discussion
Secondary CNVM is the most common complication in patients with choroidal osteoma and represents the primary cause of vision loss in this population. 1 In the present case, switching to intravitreal faricimab resulted in the complete resolution of exudation and enabled extension of the treatment interval to 16 weeks, with no recurrence over a 1-year follow-up period.
Choroidal osteoma typically presents as a slightly elevated, yellowish-orange lesion with well-defined margins in the juxtapapillary or peripapillary region, which may extend to the macula. 1 B-scan and A-scan ultrasonography, along with OCT, can assist in the diagnosis of choroidal osteoma. In this patient, B-scan imaging demonstrated elevated reflective choroidal lesions with acoustic shadowing, whereas A-scan showed high-intensity echo spikes, both of which are characteristic features of choroidal osteoma.
Choroidal osteoma is characterized by the replacement of the normal choroid with mature cancellous or lamellar bone located between a disrupted choriocapillaris and the outer choroidal layers, typically accompanied by thinning and atrophy of the overlying retinal pigment epithelium (RPE). Progressive RPE dysfunction and atrophy, particularly in areas of tumor remodeling such as regions of decalcification, can compromise the integrity of the RPE–Bruch’s membrane complex. This structural disruption creates a permissive environment for the development and extension of choroidal neovascularization through defects in this barrier.6,7
Visual prognosis in choroidal osteoma is influenced by several factors, including RPE atrophy, tumor location, decalcification, persistence of SRF, presence of subretinal hemorrhage, and development of CNVM. Tumors with overlying hemorrhage and irregular surfaces are associated with a higher risk of CNVM. The reported probability of severe vision loss within 10 years due to CNVM development is 56%–58%. 6 In the present case, as described in the literature, decreased vision was attributed to the presence of an active CNVM.
Studies have shown that anti-VEGF agents used for CNVM secondary to choroidal osteoma are associated with anatomical improvement as well as stabilization or improvement in visual acuity in small case series and retrospective cohorts. Ranibizumab and bevacizumab are commonly used anti-VEGF agents for this indication. However, the treatment burden may be considerable, and some cases demonstrate persistent or recurrent exudation despite frequent dosing.8,9
Alternative approaches such as laser photocoagulation and photodynamic therapy have been used for CNVM in choroidal osteoma; however, these strategies have notable limitations. Laser photocoagulation may be less effective in the absence of sufficient pigment and in the presence of RPE atrophy over the tumor. Moreover, it is associated with a risk of permanent scotoma in subfoveal or juxtafoveal lesions. Photodynamic therapy has been reported in selected cases; however, treatment responses may be variable and recurrence is common, often necessitating additional treatments or adjunctive anti-VEGF therapy.10,11
Evidence supporting switching between anti-VEGF agents in refractory osteoma-associated CNVM remains limited, although it has been reported in the literature. Saitta et al. 10 described successful anatomical and functional improvement with intravitreal aflibercept as a rescue therapy for CNVM secondary to choroidal osteoma that was refractory to both bevacizumab and ranibizumab. This supports the concept that switching agents may be beneficial in selected cases with persistent exudation despite frequent treatment.
Faricimab is the first bispecific immunoglobulin G monoclonal antibody approved for intraocular use, selectively targeting both VEGF-A and Ang-2 pathways. This dual inhibition promotes vascular stabilization and reduces leakage and inflammation.3,12 The favorable anatomical and functional response observed after switching to faricimab in the present case is consistent with phase 3 data demonstrating durable disease control with extended dosing intervals in other retinal conditions. In nAMD, the TENAYA and LUCERNE trials demonstrated that faricimab was noninferior to aflibercept in terms of visual outcomes and enabled dosing intervals of up to 16 weeks in several patients, supporting meaningful treatment extension without compromising efficacy. 3
Similarly, in diabetic macular edema (YOSEMITE and RHINE), faricimab achieved significant visual gains with improved anatomical outcomes using individualized regimens, with treatment intervals extended up to 16 weeks. 13 Although these disease entities differ from osteoma-associated CNVM, these large trials reinforce the concept that dual VEGF-A and Ang-2 inhibition enhances vascular stability and reduces exudation, which may be relevant in refractory CNVM.
Through dual-pathway inhibition, faricimab may provide more effective and durable control of IRF and SRF compared with agents targeting VEGF-A alone, as suggested by reduced exudation and extended dosing intervals observed in large clinical trials. The favorable response to faricimab in the present case is notable compared with prior reports using ranibizumab or aflibercept, highlighting its potential role in refractory CNVM. In the present case, faricimab achieved complete resolution of IRF and SRF after an inadequate response to ranibizumab and aflibercept, with sustained anatomical stability on an extended 16-week dosing interval. In nAMD, 3 months of faricimab treatment has been associated with improvements in visual acuity and retinal morphology, along with reductions in subfoveal choroidal thickness and resolution of IRF and SRF. 14
This report is limited by its single-patient design, which precludes conclusions regarding comparative efficacy or safety. The observed improvement may reflect individual lesion characteristics and cannot be generalized. Nonetheless, this case contributes clinical evidence suggesting that faricimab may be considered as an alternative option when osteoma-associated CNVM remains active despite frequent anti-VEGF therapy. It also underscores the need for further reports and larger studies with standardized outcome measures and longer follow-up.
Conclusion
This case report provides hypothesis-generating evidence that intravitreal faricimab may be a feasible treatment option for CNVM secondary to choroidal osteoma and may be associated with improved control of exudation and extended dosing intervals in selected patients. Given the single-case design and absence of a comparator, comparative effectiveness cannot be determined. Larger studies with standardized imaging outcomes and longer follow-up are needed to confirm efficacy and safety.
Footnotes
Acknowledgments
Not applicable.
Authors’ contributions
All authors (FA, AAA, JSA, and WNA) contributed to the development of this manuscript. FA examined the patient, obtained patient consent and related images, and revised the manuscript. AAA, JSA, and WNA contributed to the writing and editing of the manuscript. All authors reviewed and approved the final version of the manuscript.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Data availability
All relevant data are included within the manuscript.
Declaration of conflicting interest
The authors declare no conflicts of interest.
Ethical considerations
This case report adhered to the principles of the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of Princess Nourah Bint Abdulrahman University (IRB approval number 24-0907, 1 December 2024).
Funding
This research project was funded by the Deanship of Scientific Research and Libraries at Princess Nourah Bint Abdulrahman University, through Research Funding Program grant no. (FRP-2025-9). The sponsor played no role in the writing of the report or in the decision to submit the article for publication.