
Abstract
A 41-years-old woman presented with left-sided headache, diplopia, and ptosis of the left eyelid. Cerebral computed tomography angiography revealed a left persistent primitive trigeminal artery cavernous sinus fistula and a dissecting aneurysm in the V4 segment of the left vertebral artery. Digital subtraction angiography confirmed the diagnosis. The fistula was successfully occluded using dual-microcatheter coil embolization combined with Onyx-18 injection, assisted by balloon protection of the internal carotid artery. The vertebral artery dissecting aneurysm was managed conservatively by administering dual antiplatelet therapy (aspirin (100 mg/day) and clopidogrel (75 mg/day) for 3 months). Follow-up imaging at 11 months demonstrated complete resolution of the aneurysm.
Keywords
Introduction
Persistent primitive trigeminal artery (PPTA) is a rare congenital vascular anomaly, representing persistent embryonic anastomosis between the internal carotid and basilar arteries. Its incidence is reported to be 0.2%–0.6% in cerebral angiography series.1,2 Rupture of the PPTA may result in the formation of a carotid-cavernous fistula (CCF), an extremely rare clinical entity. We report a case of spontaneous CCF caused by PPTA rupture, coexisting with a vertebral artery dissecting aneurysm, successfully treated via endovascular embolization.
Case report
Clinical presentation
A patient in her early 40s was admitted to Longyan Second Hospital (Longyan, Fujian, China) in September 2024, presenting with a 2-weeks history of left temporal headache and tinnitus, followed by a 1-week history of diplopia and left eyelid ptosis (Figure 1). She had an 11-months history of hypertension (blood pressure: 156/79 mmHg) and was not taking any antihypertensive medication; she had no history of trauma or family history of stroke. On examination, she demonstrated left ptosis, conjunctival chemosis, and impaired adduction of the left eye. A left retroauricular bruit synchronous with the pulse was auscultated. No motor or sensory deficits were observed.
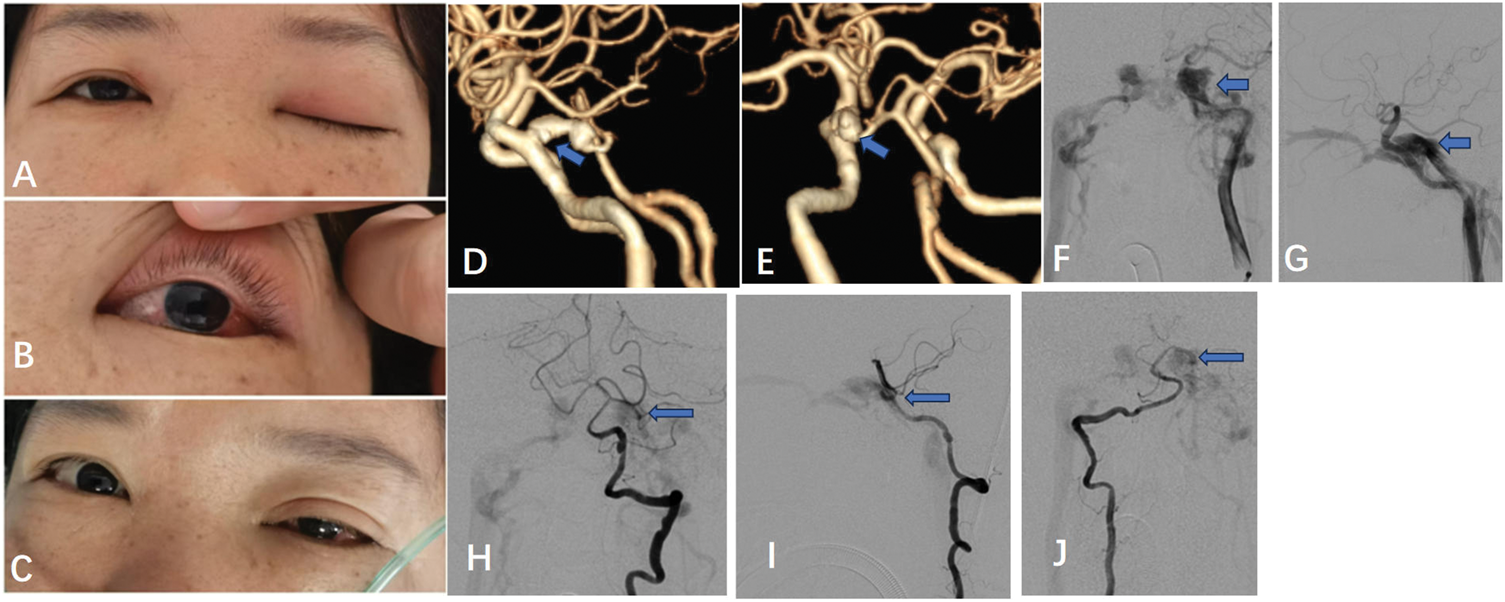
(a and b) Preoperative symptoms: left-sided ptosis and conjunctival edema. (c) Ocular findings show symptom improvement at 1 day postoperatively. (d and e) CTA shows PPTA trunk (arrow) originating from the C4 segment of the left internal carotid artery and terminating in the anterior inferior cerebellar artery (AICA). (f and g) Cerebral angiography suggests cavernous sinus fistula (arrow). (h, I, j) The PPTA trunk branch from the basilar artery (arrow). CTA: computed tomography angiography; PPTA: persistent primitive trigeminal artery.
Imaging findings
Cerebral computed tomography angiography (CTA) revealed a PPTA with a fistulous communication into the cavernous sinus. A dissecting aneurysm was also identified in the V4 segment of the left vertebral artery. Digital subtraction angiography (DSA) confirmed a CCF fed by both internal carotid and basilar arteries. The fistulous shunt was localized to the mid-portion of the PPTA, measuring approximately 2.5 mm in diameter. This defect established a direct high-flow communication between the PPTA lumen and cavernous sinus, resulting in immediate opacification of the superior ophthalmic vein and petrosal sinuses.
Treatment
Pre-procedural assessment confirmed that sacrificing the PPTA would not compromise posterior circulation perfusion due to the adequate caliber of the proximal basilar artery. Endovascular coil embolization was planned. Two Echelon-10 microcatheters (ev3, USA) were navigated into the fistula through the left internal carotid artery (ICA) (Figure 2). The cavernous sinus was packed with coils (Target 9 mm × 30 cm; Stryker, USA), and the PPTA remnant was occluded with additional coils (Target 3 mm × 8 cm and 3 mm × 6 cm; Stryker, USA). Intraoperative angiography revealed persistent fistulous shunting after coil embolization, prompting the decision to occlude the PPTA. A HyperGlide balloon (4 mm × 20 mm; ev3, USA) was inflated in the ICA to prevent reflux. Onyx-18 (ev3, USA) (0.3 mL) was injected via the second microcatheter to complete the embolization. Post-procedural angiography confirmed complete occlusion of the fistula with preserved flow of the carotid and basilar arteries. The vertebral artery dissecting aneurysm was managed medically with dual antiplatelet therapy (aspirin (100 mg/day) and clopidogrel (75 mg/day) for 3 months).

(a) Two microcatheters were navigated into the fistula (within the PPTA trunk). (b) Three coils were deployed; however, the fistula tract persisted. (c) The HyperGlide balloon was inflated. (d, e, f) Onyx was injected until a portion of it entered the PPTA trunk branch arising from the basilar artery. (f and g) Post-treatment left internal carotid angiogram. (h) Basilar artery after the treatment. (i and j) Follow-up imaging at 3 and 11 months shows complete resolution of the vertebral artery dissection (white arrow). Blue arrows: Left AICA (d, e, h); PPTA trunk (f, g). AICA: anterior inferior cerebellar artery; PPTA: persistent primitive trigeminal artery.
Follow-up
The patient recovered well postoperatively. Conjunctival edema was resolved, and she was able to open her eyes the following day. At 3 months, no recurrence of the fistula was observed. Follow-up imaging at 11 months demonstrated complete resolution of the vertebral artery dissection. Functional assessments performed at both 3-months and 11-months follow-ups showed consistent favorable outcomes (mRS score: 0 and Mini-Mental State Examination (MMSE) score: 30), indicating excellent functional recovery and preserved neurocognitive function despite PPTA sacrifice.
Discussion
Spontaneous CCF caused by PPTA rupture is exceedingly rare. Only 14 such cases have been reported in PubMed between 1983 and 2024,3–6 with a strong female predominance (12/14). The exact mechanism of rupture remains unclear; however, hypotheses include aneurysmal rupture or congenital vascular wall weakness. 4
The treatment goal for PPTA-related CCF is to occlude the fistula while preserving cerebral perfusion. In this case, angiographic evaluation confirmed a Saltzman type II PPTA, characterized by termination in the anterior inferior cerebellar artery (AICA) with posterior circulation maintained via the vertebrobasilar system and posterior communicating arteries. This anatomy permits safe sacrifice of the PPTA, unlike Type I variants where the PPTA serves as the exclusive supply source for the distal basilar artery. Endovascular options include detachable balloon or coil embolization as well as combined coil and Onyx embolization.7–9 Given the confirmed Saltzman type II anatomy, the fact that the large fistulous shunt effectively excluded the PPTA from posterior circulation supply, and the considerable size of the fistula which rendered selective preservation of the PPTA trunk technically demanding, we carefully weighed the negligible risk of posterior circulation ischemia against the certainty of fistula closure. Onyx-18 was selected for its ability to achieve precise penetration of the fistula niche; however, we acknowledge the inherent risk involved in distal migration. To mitigate this, a “coil-first” strategy was employed to reduce flow velocity, complemented by balloon protection to prevent Onyx reflux into the ICA. A transvenous approach was also considered feasible but was designated as a secondary option due to the risk of Onyx reflux into the ICA.
To the best of our knowledge, this represents the first reported case of PPTA-related CCF coexisting with a vertebral artery dissecting aneurysm. At the 11-months follow-up, the vertebral artery lesion achieved complete resolution, a finding consistent with the well-documented natural history of spontaneous remodeling in asymptomatic dissecting aneurysms. Although the patient’s hypertension history may have contributed to generalized vascular wall fragility—a risk factor for both vascular dissection and aneurysm formation—and underlying connective tissue abnormalities could have theoretically increased susceptibility to both conditions, no direct causal relationship between the two lesions can be established based on the available data. The favorable treatment response suggests that the dissection was stable and capable of spontaneous healing after PPTA embolization.
Conclusion
Endovascular treatment using dual-microcatheter coil embolization combined with Onyx-18 injection assisted by balloon is effective for PPTA cavernous sinus fistula. Conservative antiplatelet therapy may suffice for selected cases of vertebral artery dissection.
Footnotes
Acknowledgments
We would like to thank the patient for their cooperation during the study.
Author contributions
Cheng-Cai Wen and Rui-Shu Jiang designed the work. Shi-Jie Wen collected and analyzed the data. Cheng-Cai Wen drafted the work and substantively revised it. All authors have read and approved the final manuscript.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Declaration of conflicting interests
The authors have no conflicts of interest to disclose.
Ethics statement
The patient provided informed consent for undergoing treatment and for the publication of this case report. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki (1975, as revised in 2024) and was approved for publication by the institutional review board. We have deidentified all patient details, and the reporting of this study conforms to the Case Report (CARE) guidelines. 10
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.