
Abstract
Background
Postoperative bleeding in patients with intracranial aneurysms remains a serious complication associated with high mortality. The platelet-to-albumin ratio, reflecting thrombotic potential and endothelial health, has demonstrated prognostic value in various clinical settings. However, its association with postoperative bleeding following endovascular treatment of intracranial aneurysms has not yet been investigated.
Methods
This retrospective cohort study (January 2021 to January 2025) included 219 participants undergoing endovascular treatment. Multivariable logistic regression, smooth curve fitting, and piecewise linear regression were used to assess the association between the platelet-to-albumin ratio and bleeding risk, adjusting for potential confounders. Predictive performance was evaluated using receiver operating characteristic curves and decision curve analysis.
Results
Bleeding occurred in 58 participants (26.5%). A significant nonlinear inverse L-shaped relationship was observed between the platelet-to-albumin ratio and bleeding risk (nonlinearity p = 0.010), with an inflection point at the platelet-to-albumin ratio of 5.05. Below this threshold, a higher ratio was associated with reduced risk (odds ratio: 0.607, 95% confidence interval: 0.445–0.829, p = 0.0017); whereas above this value, the association was neutral. The incidence of bleeding decreased significantly across increasing platelet-to-albumin ratio quartiles (Q1: 45.5% vs. Q4: 14.3%, p < 0.001). Multivariable analysis confirmed platelet-to-albumin ratio as an independent predictor (continuous: odds ratio: 0.73, 95% confidence interval: 0.59–0.90, p = 0.004; Q4 vs. Q1: odds ratio: 0.05, 95% confidence interval: 0.01–0.21, p < 0.001). The platelet-to-albumin ratio demonstrated superior discriminative capacity (area under the curve, 0.670) compared with platelet count (area under the curve, 0.624) or albumin alone (area under the curve, 0.607). Decision curve analysis confirmed clinical application.
Conclusion
The platelet-to-albumin ratio independently predicts postoperative bleeding with a nonlinear relationship. It should be considered an adjunctive marker within a multimodal framework to help balance bleeding and ischemic risks.
Keywords
Introduction
Intracranial aneurysms (IAs) represent a critical cerebrovascular pathology with a global prevalence of approximately 3.2%–6.0%, posing a significant public health burden. These rates vary considerably across populations and regions because of genetic, environmental, and healthcare disparities. 1 These saccular or berry-type aneurysms collectively account for approximately 80% of nontraumatic subarachnoid hemorrhages (SAH), a condition associated with devastating outcomes, including a 35% mortality rate prior to hospital admission and severe neurological disability in 30% of survivors. 1 Endovascular therapy has emerged as the predominant treatment modality, largely replacing microsurgical clipping in many centers and accounting for >70% of contemporary aneurysm management. 2 Coil embolization and flow diversion are the widely used techniques; however, microsurgical clipping remains prevalent for ruptured anterior circulation aneurysms, particularly in resource-limited settings. 2 Despite significant advancements in endovascular techniques, postoperative bleeding remains a critical complication, with reported incidence rates of 5%–15% and associated mortality exceeding 30%. 3 This persistent challenge underscores the limitations of current technologies, which collectively contribute to difficulties in achieving durable occlusion and preventing thromboembolism. Intraoperative monitoring and postoperative anticoagulation management are pivotal for mitigating bleeding risks; therefore, multicenter studies are warranted to optimize this balance and refine evidence-based clinical protocols.
The current landscape of IA rupture prediction models predominantly relies on well-established imaging-derived anatomical and hemodynamic parameters, including aneurysm size, volume, aspect ratio, and oscillatory shear index, all of which demonstrate significant discriminatory power in distinguishing ruptured from unruptured lesions. 4 However, recent studies underscore the critical yet inadequately explored contribution of systemic inflammatory and nutritional biomarkers in improving risk stratification and complementing imaging-based assessments, particularly for small aneurysms that defy conventional size-based predictions, 5 thereby highlighting a significant gap in current predictive paradigms. For instance, specific serum inflammatory markers, including the systemic immune-inflammatory index (SII) and white blood cell-to-platelet ratio (WPR), have demonstrated efficacy as independent predictors of instability, validating their clinical relevance, particularly in small saccular IAs. Composite models integrating these markers have achieved an area under the curve (AUC) of 0.905 in predicting rupture or symptomatic progression, 5 significantly outperforming models based solely on morphology. These findings are consistent with the key pathophysiological understanding, wherein inflammation disrupts vascular homeostasis and exacerbates endothelial dysfunction and wall degradation via increased proteolytic activity and matrix metalloproteinase expression, processes central to formation, growth, and rupture of IAs. 6
The interplay between platelet count and albumin (ALB) concentration represents a critical pair of complementary biomarkers in cerebrovascular interventions, reflecting fundamental thrombotic potential and endothelial homeostasis, respectively. Platelet count, a well-established indicator of thrombotic risk, demonstrates an inverse L-shaped relationship with adverse clinical outcomes in patients with ischemic stroke and transient ischemic attack (TIA), wherein both thrombocytopenia (<150 × 109/L) and thrombocytosis (>450 × 109/L) are associated with increased risks of recurrent stroke, mortality, and poor functional outcomes. 6 This inverse L-shaped relationship represents the dual nature of platelets in both prothrombotic and inflammatory pathways: excessive activation promotes endothelial dysfunction and atherothrombosis, contributing to a prothrombotic state, whereas low counts often reflect increased consumption due to underlying vascular pathology. 6 In contrast, serum ALB, a key regulator of crucial endothelial integrity and systemic antioxidant capacity, is established as an independent predictor in cerebrovascular disease. Hypoalbuminemia (<35 g/L) is strongly associated with impaired collateral circulation, larger ischemic foci, and hemorrhagic transformation following revascularization. These effects are attributed to its critical role in maintaining blood–brain barrier (BBB) stability and mitigating oxidative stress through osmotic regulation and free radical scavenging.7,8 The platelet-to-albumin ratio (PAR), which integrates these parameters, has emerged as a novel composite inflammatory and nutritional prognostic index, serving as a surrogate indicator of overall vascular health. This ratio reflects an integrated assessment of inflammatory status, nutritional state, and coagulation function. PAR has shown robust independent predictive value for outcomes across diverse conditions (e.g. acute kidney injury, cardiovascular disease, malignancy, and infectious diseases), 9 demonstrating particularly strong predictive performance for sepsis and surgical site infections, 10 thereby validating its clinical utility.
Despite its established application in other clinical domains, PAR remains unexplored in the context of neuroendovascular procedures, particularly with respect to postoperative complications. Therefore, this study aimed to assess the predictive accuracy of PAR for postoperative bleeding following endovascular treatment of IAs using a retrospective cohort design, thereby providing clinicians with an economical and readily accessible tool for risk stratification.
Methods
Study population
This retrospective cohort analysis was conducted at Guangyuan Central Hospital from January 2021 to January 2025. Consecutive patients who underwent endovascular embolization for IAs during this period were enrolled. The primary outcome measure was hemorrhagic complications occurring during 7 days of the procedure, confirmed either radiologically or clinically. Access-site hematomas and systemic hemorrhagic episodes unrelated to the primary procedure were excluded from this endpoint. This definition aligns with current multicenter studies and national registry standards, which typically identify intracranial hemorrhage related to neuroendovascular procedures via imaging confirmation or clinically meaningful neurological deterioration. Exclusion criteria were as follows: (a) missing or inadequate laboratory data or outcome records; (b) diagnosis of hereditary or acquired coagulation disorders; (c) chronic anticoagulant use beyond perioperative prophylaxis requirements; (d) concurrent major surgical procedures during the index hospitalization; (e) mortality within 24 h of surgery; and (f) age <18 years. 11 (Figure 1).
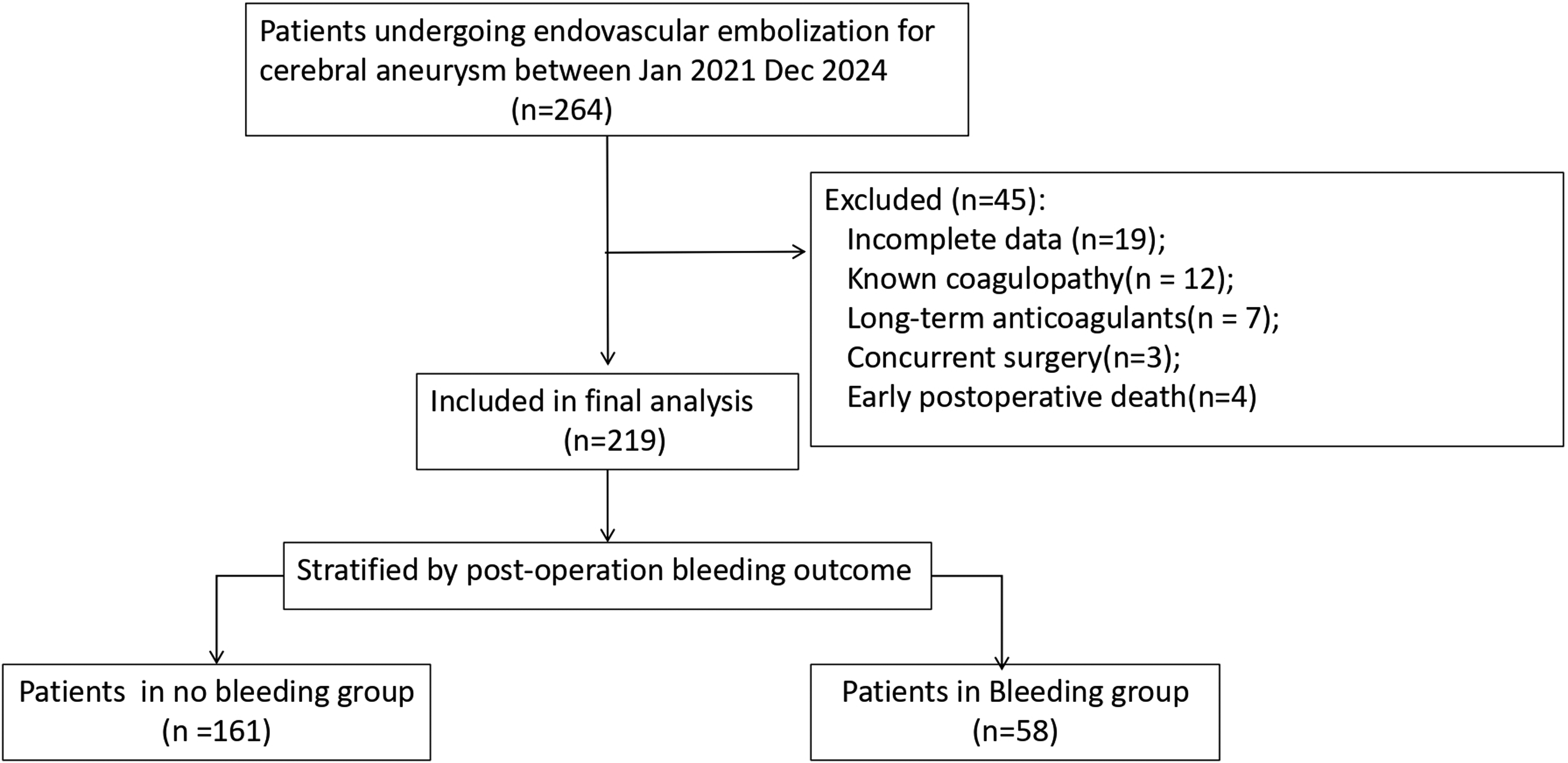
Flow chart illustrating the patient enrollment process, numbers excluded per exclusion criterion, and final selection of the study population.
Definition of postoperative bleeding. The primary outcome of this study was postoperative bleeding, defined as any intracranial hemorrhage confirmed by imaging (CT or MRI) within the first 7 days following surgery. This included any of the following criteria: (a) new intracranial hemorrhage identified on postoperative imaging; (b) intracranial hemorrhage confirmed by reoperation or interventional procedure; or (c) newly developed neurological deficits attributed to hemorrhage and confirmed by imaging. To comprehensively evaluate the risk of postoperative bleeding, a broad definition was adopted that included all imaging-detectable hemorrhagic events regardless of clinical symptomatology. Access-site hematomas and systemic hemorrhagic events unrelated to the primary procedure were excluded from the outcome.
Data collection
Demographic characteristics, comorbid conditions, aneurysm features (including location, dimensions, and rupture status), and perioperative metrics were prospectively collected from hospital databases. Laboratory parameters measured within the 24-h period before the procedure were obtained in accordance with the standardized collection protocols.
Covariate selection
Prior to constructing the multivariable logistic regression model, multicollinearity was assessed among continuous variables that were statistically significant in univariate analysis. As all variables deviated from a normal distribution (Shapiro–Wilk test, p < 0.05), Spearman's rank correlation coefficient was used to evaluate correlations between variables. According to empirical criteria, a correlation coefficient of |rs| ≥ 0.7 was considered indicative of significant multicollinearity, warranting variable selection or combination. For covariate selection in the multivariable logistic regression analysis, a forward stepwise selection method was applied, with a significance level of p <0.05 for inclusion of primary covariates.
Statistical analysis
Variable distribution characteristics were determined through histogram evaluation. Continuous variables conforming to a Gaussian distribution were summarized as mean ± SD, whereas those exhibiting skewness were reported as median with interquartile range (IQR). Categorical data were expressed as frequency counts and percentages (%). Chi-square or Fisher's exact test was applied to analyze intergroup differences for categorical variables, one-way analysis of variance (ANOVA) for normally distributed continuous measures across multiple groups, and the Kruskal–Wallis H test for non-normally distributed parameters. Post hoc comparisons employed Bonferroni adjustment or the least significant difference (LSD) method, as appropriate. The relationship between PAR and postoperative hemorrhage was investigated via logistic regression. Confounder selection was based on established clinical relevance and univariate screening significance. Three hierarchical models were constructed: Model 1 incorporated primary adjustments for age, sex, and body mass index (BMI); Model 2 was additionally adjusted for intraoperative blood loss; and Model 3 was further adjusted for coagulation profiles, including prothrombin time (PT), activated partial thromboplastin time (APTT), fibrinogen, D-dimer, fibrinogen degradation products (FDP), and hepatic enzymes (alanine aminotransferase (ALT) and aspartate aminotransferase (AST)). Model 4 was adjusted for intraoperation blood loss, ALT, and urea nitrogen. Multivariable logistic regression with smooth curve fitting was used to characterize the independent PAR–bleeding association. Threshold effect analysis was performed using a segmented linear regression model with smoothing splines, with nonlinearity assessed via a likelihood ratio test comparing one-segment versus segmented models. Predictive performance was quantified by receiver operating characteristic (ROC) curve AUC and decision curve analysis (DCA). 12 All computations were executed in R version 3.32 (R Foundation for Statistical Computing; Vienna, Austria).
Ethics statement
This investigation adhered to the principles outlined in the Declaration of Helsinki (1975, as amended in 2024). The Institutional Review Board of Guangyuan Central Hospital granted exemption from ethical approval and waived the requirement of written informed consent for this retrospective analysis of deidentified clinical records. All personally identifiable information was removed before data processing, safeguarding participant privacy throughout the study. 13
Results
Baseline characteristics
Table 1 presents the baseline characteristics of the 219 enrolled participants, who were categorized into postoperative bleeding (n = 58) and nonbleeding (n = 161) groups. Among the 58 patients who experienced bleeding, 34 (58.6%) had asymptomatic imaging findings (e.g. minor subarachnoid hemorrhage, small hematoma, or contrast extravasation), whereas 24 (41.4%) were symptomatic. Most demographic variables (sex, age, and BMI), lifestyle factors (smoking and alcohol consumption), comorbidities (hypertension, coronary artery disease, and liver disease), and aneurysm features (size, location, Fisher grade, multiplicity, rupture status, and coiling technique) showed comparable distributions between groups (all p > 0.05). Significant intergroup differences were observed in laboratory parameters: the bleeding cohort exhibited lower platelet counts (174.5 ± 93.2 vs. 204.2 ± 79.1 × 109/L, p = 0.022), reduced ALB levels (35.4 vs. 37.0 g/L, p = 0.016), and lower PAR (3.8 vs. 5.3, p < 0.001). Altered coagulation profiles were observed in the bleeding group, including elevated PT, international normalized ratio (INR), and APTT as well as increased fibrinogen and FDP levels. Intraoperative blood loss volume was significantly lower in the bleeding cohort (101.2 ± 21.6 mL vs. 129.6 ± 20.2 mL, p < 0.001).
Baseline characteristics of patients.
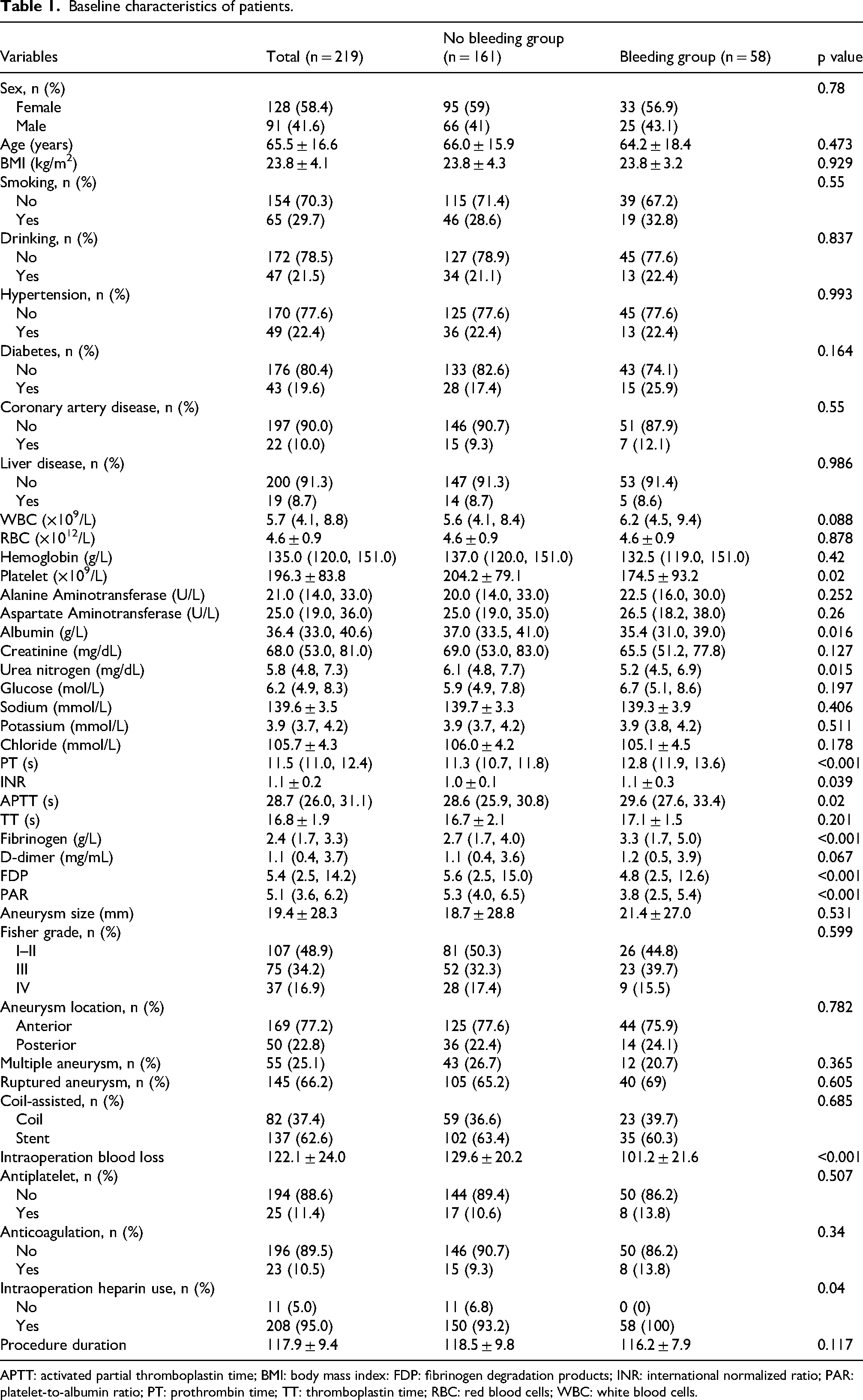
APTT: activated partial thromboplastin time; BMI: body mass index: FDP: fibrinogen degradation products; INR: international normalized ratio; PAR: platelet-to-albumin ratio; PT: prothrombin time; TT: thromboplastin time; RBC: red blood cells; WBC: white blood cells.
Nonlinearity relationship between PAR and postoperative bleeding
Multivariable logistic regression with smooth curve fitting demonstrated a nonlinear association between PAR and postoperative bleeding (Figure 2). Application of piecewise regression modeling revealed two distinct linear segments with an identified inflection point at PAR of 5.050. The significant nonlinearity (p = 0.010, Table 2) validated the segmented model approach. Below this threshold, each unit increase in PAR corresponded to decreased bleeding risk (odds ratio (OR): 0.607, 95% confidence interval (CI): 0.445–0.829, p = 0.0017). Above 5.050, no significant association was observed (OR: 1.093, 95% CI: 0.842–1.421, p = 0.0503).

Relationship between PAR and postoperative bleeding. The relationship between postoperative bleeding risk and PAR was assessed using a smooth curve with 95% bootstrap confidence bands. The dashed vertical line indicates the reference point (5.0504), and the dashed horizontal line marks an OR of 1.0. The blue histogram shows the distribution of the PAR in the study sample. The red solid line represents the estimated OR as a function of PAR, with the pink shading indicating the 95% confidence band.
Nonlinear relationship between PAR and postoperative bleeding.

CI: confidence interval; OR: odds ratio; PAR: platelet-to-albumin ratio.
Stratification by PAR quartiles revealed significant heterogeneity in baseline characteristics (Table 3). The incidence of bleeding incidence demonstrated a significant inverse gradient across quartiles (p < 0.001), decreasing from 45.5% in Group 1 to 14.3% in Group 4. Significant variations were observed in diabetes prevalence (p = 0.002), Fisher aneurysm grade (p < 0.001), and location distribution (p = 0.014) as well as across multiple laboratory parameters, including hematological indices (white blood cells (WBCs), hemoglobin, and platelets), metabolic markers (creatinine, urea, and glucose), electrolytes (potassium and chloride), and coagulation profiles (PT, fibrinogen, D-dimer, and FDP) (all p < 0.05). In contrast, age, BMI, smoking status, aneurysm size, rupture status, and most procedural factors demonstrated comparable distributions across quartiles.
Baseline characteristics of patients classified by PAR.
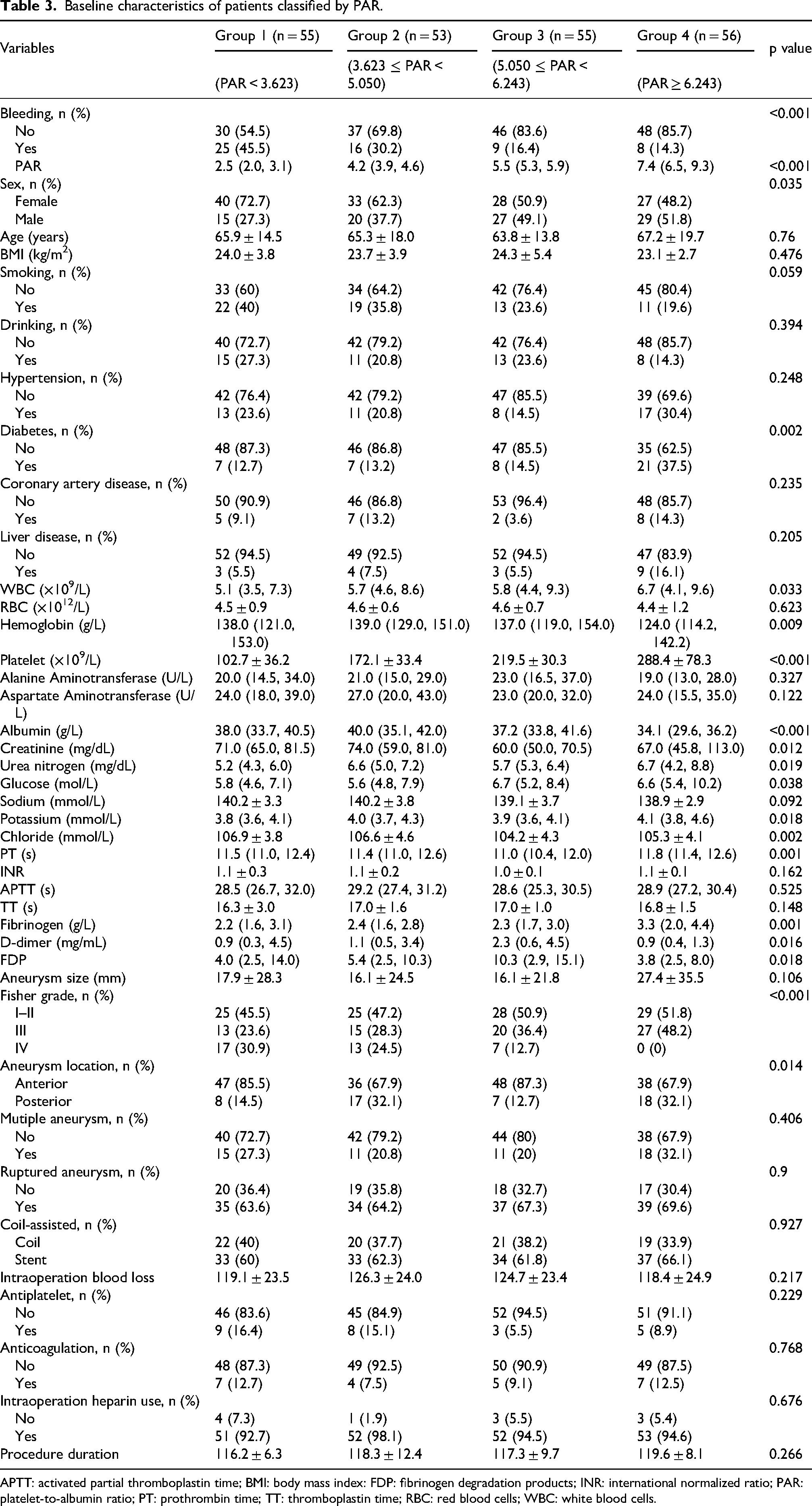
APTT: activated partial thromboplastin time; BMI: body mass index: FDP: fibrinogen degradation products; INR: international normalized ratio; PAR: platelet-to-albumin ratio; PT: prothrombin time; TT: thromboplastin time; RBC: red blood cells; WBC: white blood cells.
Logistic regression analysis
Univariate analysis identified significant predictors of postoperative hemorrhage (Table 4). Reduced PAR demonstrated protective effects against bleeding (OR: 0.84, 95% CI: 0.72–0.97, p = 0.15). Similarly, lower ALB concentrations, urea nitrogen levels, and intraoperative blood loss volume were associated with reduced bleeding risk. Conversely, elevated ALT, AST, APTT, fibrinogen, and FDP levels were associated with increased hemorrhagic risk. No significant associations were observed for most demographic factors, comorbidities, additional laboratory parameters, aneurysm characteristics, or procedural details. To assess multicollinearity, Spearman correlation analysis was performed (S Figure 1). Strong positive correlations were observed between PAR and platelet count (rs = 0.89) and between AST and ALT (rs = 0.73); a strong negative correlation was found between PAR and ALB (rs = −0.82). Correlations among other variables were weak, suggesting relative independence. In multivariable logistic regression analysis adjusted for ALT, urea, APTT, fibrinogen, FDP, and intraoperative blood loss, PAR remained an independent protective factor against postoperative bleeding (OR: 0.72, 95% CI: 0.61–0.87, p < 0.001). ALT was identified as an independent risk factor (OR: 1.04, 95% CI: 1.02–1.06, p < 0.001), whereas urea exhibited a protective effect (OR: 0.79, 95% CI: 0.66–0.96, p = 0.016). Intraoperative blood loss was inversely associated with postoperative bleeding (OR: 0.90, 95% CI: 0.87–0.93, p < 0.001). APTT, fibrinogen, and FDP were associated with bleeding in univariate analysis but lost significance in the multivariable model, suggesting that their effects may be explained by PAR, intraoperative blood loss, or other covariates. Based on these findings, ALT, urea, and intraoperative blood loss were selected as the primary covariates(S Table 1).
Logistic regression analysis.
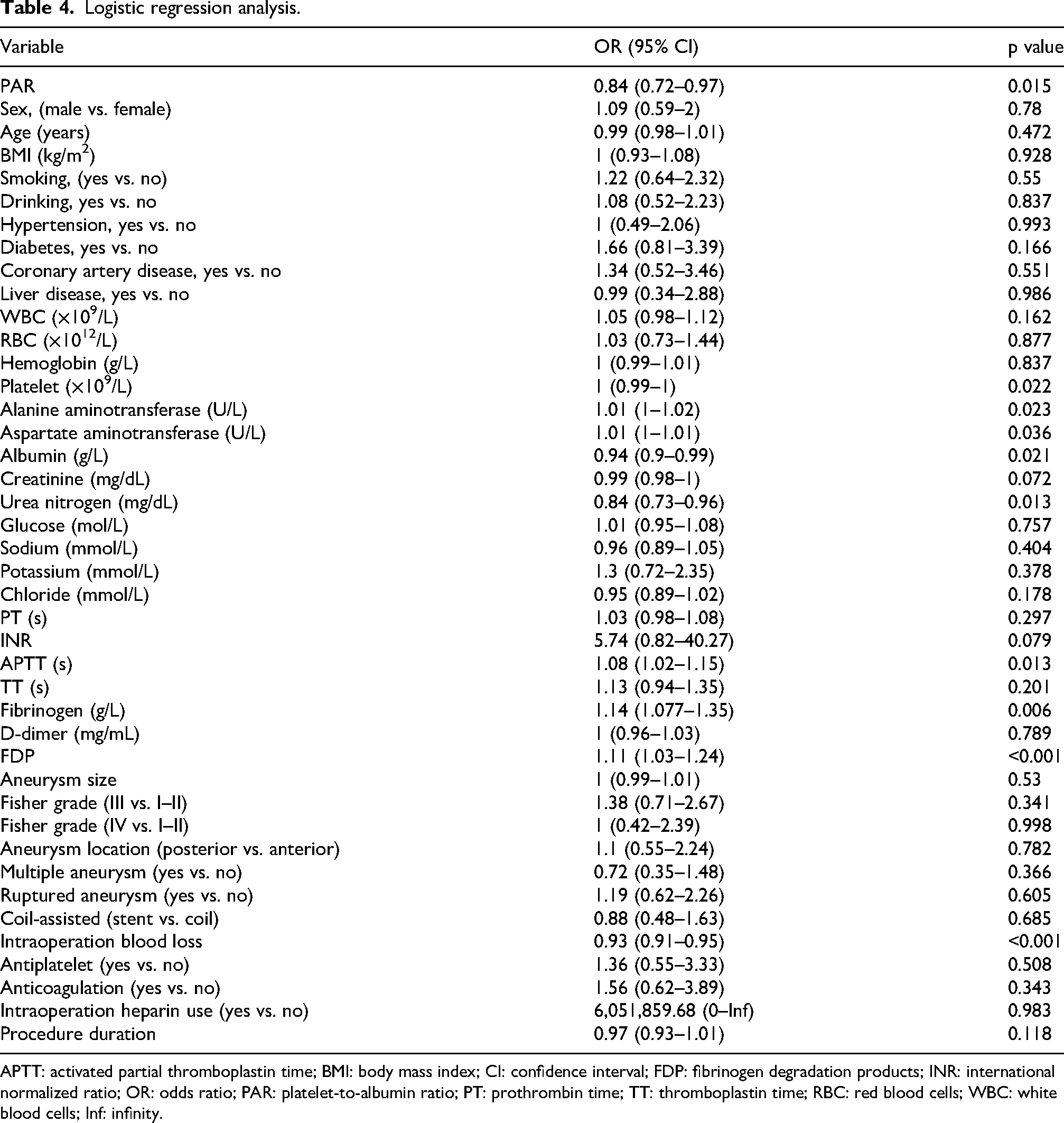
APTT: activated partial thromboplastin time; BMI: body mass index; CI: confidence interval; FDP: fibrinogen degradation products; INR: international normalized ratio; OR: odds ratio; PAR: platelet-to-albumin ratio; PT: prothrombin time; TT: thromboplastin time; RBC: red blood cells; WBC: white blood cells; Inf: infinity.
Multivariable regression confirmed PAR as an independent predictor of reduced bleeding risk (Table 5). As a continuous variable, higher PAR values maintained significant inverse associations with bleeding risk across all adjustment tiers (fully adjusted Model 3: OR: 0.73, 95% CI: 0.59–0.90, p = 0.004). When analyzed by quartiles, the highest PAR quartile (Group 4) showed substantially lower risk than the lowest quartile (Group 1), particularly in Model 3 (OR: 0.07, 95% CI: 0.01–0.37, p = 0.002) and Model 4 (OR: 0.05, 95% CI: 0.01–0.21, p < 0.001). A significant dose-dependent inverse relationship was evident across ascending PAR quartiles in Models 2–4 (pfor trend < 0.001).
Multivariable logistic regression analyses of the association of PAR with postoperative bleeding.
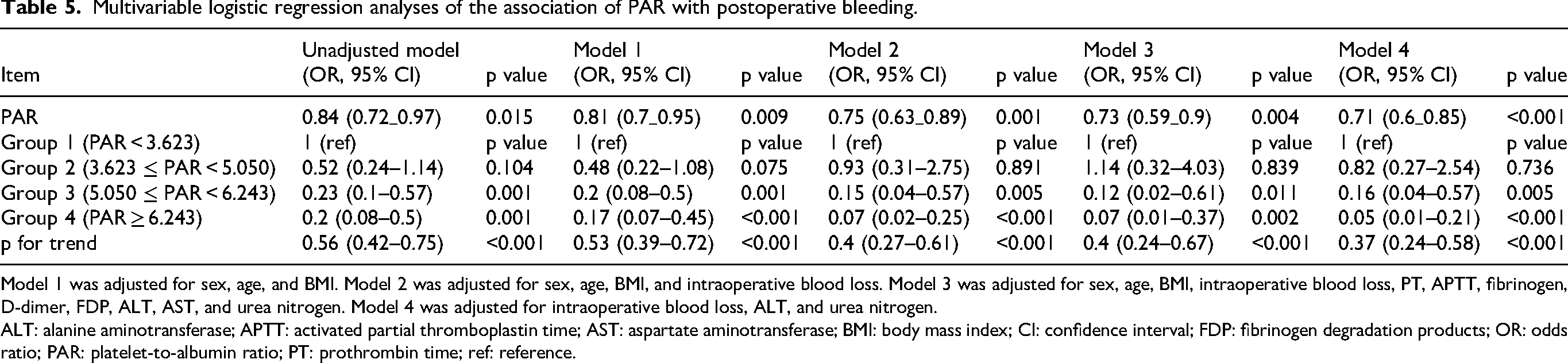
Model 1 was adjusted for sex, age, and BMI. Model 2 was adjusted for sex, age, BMI, and intraoperative blood loss. Model 3 was adjusted for sex, age, BMI, intraoperative blood loss, PT, APTT, fibrinogen, D-dimer, FDP, ALT, AST, and urea nitrogen. Model 4 was adjusted for intraoperative blood loss, ALT, and urea nitrogen.
ALT: alanine aminotransferase; APTT: activated partial thromboplastin time; AST: aspartate aminotransferase; BMI: body mass index; CI: confidence interval; FDP: fibrinogen degradation products; OR: odds ratio; PAR: platelet-to-albumin ratio; PT: prothrombin time; ref: reference.
Predictive performance and risk stratification
ROC curve analysis demonstrated that PAR exhibited superior discriminative ability for predicting bleeding compared with platelet count or ALB alone. The AUC for PAR was 0.670 (95% CI: 0.589–0.750), significantly higher than platelet count (AUC = 0.624, 95% CI: 0.540–0.707; p = 0.032) and ALB (AUC = 0.607, 95% CI: 0.522–0.692; p = 0.007) (Figure 3). DCA further validated the clinical utility of PAR across a relevant threshold probability range (20%–60%). Within this interval, PAR provided greater net benefit than either isolated biomarker and outperformed the “treating all” and “treating none” strategies, indicating its potential as a clinically useful predictive tool (Figure 4).

ROC curve of the logistic regression model. ROC curves comparing three biomarker panels for classification are shown. The dashed diagonal line represents a random classifier. The area under the curve (AUC) values are as follows: PAR, 0.6695; platelet count, 0.6238; and albumin, 0.6069.
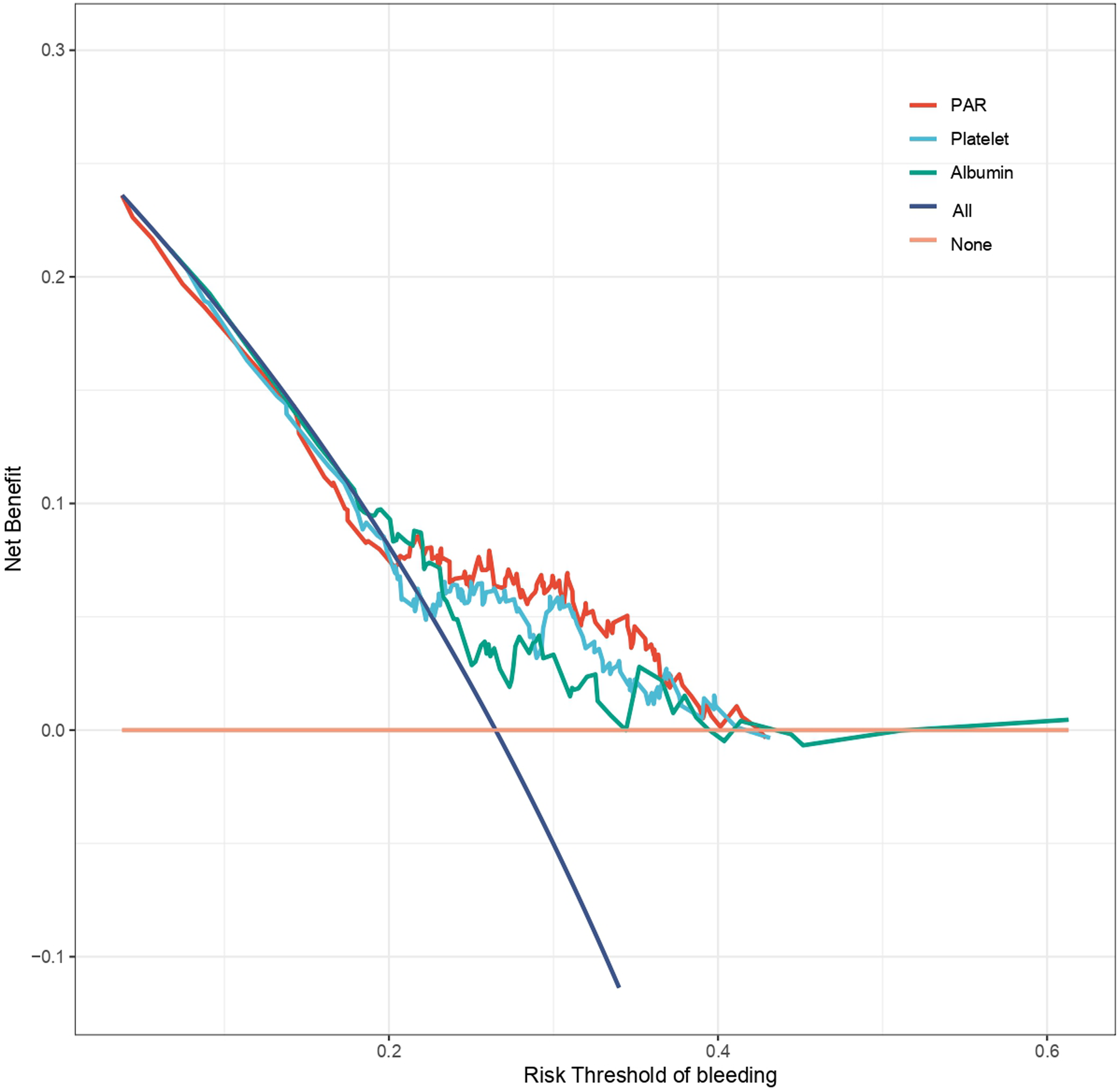
Decision curve analysis. Net benefit curves from decision-analytic threshold analysis for different biomarker panels are shown. The red, cyan, green, and navy lines represent PAR, platelet count, and albumin, respectively, with an additional none option shown in peach. The x-axis shows the risk threshold of bleeding, and the y-axis shows the net benefit. The figure compares the clinical value of using each biomarker panel to guide decisions across a range of threshold probabilities.
Discussion
Our cohort analysis identified PAR as an independent predictor of postoperative bleeding following endovascular aneurysm intervention. A significant nonlinear association was identified, with an inflection point at PAR value of 5.05 (p for nonlinearity = 0.01). Multivariable piecewise regression confirmed this inverse L-shaped relationship (nonlinearity p = 0.010), revealing that PAR ≥ 5.05 maintained a null association with bleeding risk. Consistent with this pattern, bleeding incidence decreased progressively across increasing PAR quartiles (p < 0.01). Compared with the reference quartile, patients in the third and fourth quartiles demonstrated 88% and 93% lower bleeding risk, respectively, accompanied by a significant dose–response trend (p < 0.001). Furthermore, PAR showed superior discriminative capacity (AUC 0.670) compared with isolated platelet count (AUC 0.624, p = 0.032) or ALB (AUC 0.607, p = 0.007), with clinical utility validated by DCA demonstrating greater net benefit across 20%–60% threshold probabilities.
The postoperative bleeding rate in this study was 26.5% (58/219), exceeding the 5%–15% range commonly reported in the literature. 3 This discrepancy is primarily attributable to the broad definition of bleeding adopted in the present study. Reported bleeding rates vary substantially depending on the definition used. Baldvinsdóttir et al., 3 in a Swedish nationwide prospective study, reported an adverse event rate of 5%–15% among patients with ruptured aneurysms after endovascular treatment, which primarily reflects symptomatic bleeding requiring clinical intervention. The ARETA study, 14 a prospective multicenter cohort involving 1140 patients, used a strict definition limited to clinically significant rebleeding and reported a 1-year rebleeding rate of 1.0% (95% CI: 0.3%–1.7%) for patients with ruptured aneurysms. In contrast, when the definition expanded to include asymptomatic imaging findings, the incidence increases substantially. Pressman et al. 15 reported a 27% incidence of “nuisance bleeding” (defined as easy bruising, bleeding from small cuts, petechiae, and ecchymosis) in patients treated with the pipeline embolization device, consistent with our findings. Therefore, the bleeding rate observed in our study reflects the true incidence under a broader definition rather than an abnormally elevated clinical risk.
The sample size in this study was limited by the number of cases available from a single-center over a defined period. A total of 219 participants were enrolled, with a postoperative bleeding rate of 26.5% (58/219). Based on sample size estimation using PASS software, 16 with an observed effect size (OR: 0.73), outcome event rate (26.5%), and four core covariates (PAR, ALT, urea, and intraoperative blood loss) in the multivariable model, a sample size of approximately 170–190 participants would be required to achieve 80% statistical power at a significance level of 0.05. Therefore, the final sample size of 219 participants met this requirement, yielding an events-per-variable (EPV) ratio of 14.5 (58 events/4 covariates), which exceeds the conventionally recommended threshold of 10. These findings indicate that the primary analyses are adequately powered and that the core conclusions are robust.
PAR has demonstrated utility as a biomarker for disease risk stratification across clinical contexts. 17 In patients with pediatric ulcerative colitis (n = 35), it demonstrated superior prognostic utility for surgical site infections compared with conventional markers (ALB, platelet count, and C-reactive protein (CRP)), achieving a sensitivity of 75.0% and specificity of 77.8% as the sole independent predictor. This supports its role in preoperative risk assessment to guide targeted prophylaxis. 10 In the present study, PAR exhibited a protective effect below 5.05, whereas above this threshold, this effect plateaued, neither further reducing nor increasing the risk. This finding suggests that a PAR value of 5.05 may serve as a potential clinical threshold for risk stratification. Patients with PAR below this threshold may benefit from more intensive perioperative management, whereas those with PAR above this value have a relatively stable risk profile. The AUC of PAR for predicting postoperative bleeding in this study was 0.670. Although significantly higher than that of platelet count (0.624) or ALB alone (0.607), it remains below the 0.80 threshold generally considered acceptable for a standalone clinical prediction tool. This finding suggests that PAR alone is insufficient to serve as an independent decision-making criterion for postoperative bleeding risk stratification. Instead, PAR should be considered an adjunctive marker within a multimodal risk assessment framework. Future studies should explore combining PAR with imaging parameters (e.g. aneurysm morphology, location, and size), clinical grading scales (e.g. Fisher grade and Hunt–Hess grade), and other biomarkers (e.g. inflammatory cytokines and coagulation parameters) to develop comprehensive prediction models that may improve the accuracy and clinical utility of risk stratification. It is important to emphasize that PAR should be positioned as a risk stratification tool rather than a standalone guide for anticoagulation adjustment. Perioperative management following endovascular treatment of IAs requires a careful balance between bleeding and ischemic risks. Although reducing anticoagulation intensity may lower bleeding events, it may increase the risk of thromboembolic complications, including in-stent thrombosis, ischemic stroke, and incomplete aneurysm occlusion. Therefore, until validated by prospective studies, PAR should be integrated into a comprehensive risk assessment framework that incorporates blood pressure control, optimization of intraoperative techniques, and individualized antithrombotic strategies. It should not be used as the sole basis for anticoagulation adjustment.
PAR serves as a prognostic indicator in acute hematogenous osteomyelitis (AHO). In a cohort of 101 patients with AHO, elevated levels of PAR independently predicted complicated clinical courses, including sepsis or metastatic infections. 18 Mechanistically, PAR integrates two cardinal pathological processes: inflammation-driven platelet elevation and ALB suppression secondary to inflammation or malnutrition. This dual-parameter approach provides a more nuanced risk assessment than isolated biomarkers. Elevated PAR is associated with sepsis severity, multiorgan dysfunction, and mortality, reflecting amplified inflammatory cascades. 17 When combined with complementary nutritional or inflammatory biomarkers, the prognostic assessment ratio significantly enhances predictive accuracy for severe infections, achieving superior discriminative performance, as evidenced by an AUC >0.85 in validation cohorts. This dual-parameter strategy leverages synergistic interactions between inflammatory and nutritional pathways, proving particularly valuable in resource-limited settings where advanced diagnostics are unavailable. Concurrently, diabetes exacerbates burn wound healing through multifactorial pathophysiology. Chronic inflammation, oxidative stress, compromised angiogenesis, and dysregulated cellular signaling collectively impair tissue regeneration. 19 The threshold effect observed between PAR and postoperative bleeding may reflect a pre-existing fragile vascular environment. We proposed that low PAR results from either thrombocytopenia and/or hypoalbuminemia. Reduced platelet count reflects impaired endothelial repair capacity. Emerging evidence suggests that platelets play a pivotal role in maintaining endothelial integrity by releasing growth factors such as vascular endothelial growth factor (VEGF) and transforming growth factor-β1 (TGF-β1), which are critical for endothelial cell proliferation and angiogenesis. 20 Meanwhile, low ALB indicates diminished antioxidant defense and compromised BBB integrity. The association between hypoalbuminemia and BBB integrity has become a key area of research in intracerebral hemorrhage and secondary brain injury. This may involve the ability of ALB to scavenge free radicals, regulate inflammatory cytokines, and stabilize endothelial cell junctions, all of which are crucial for maintaining BBB homeostasis. 21 This pre-existing “fragile vascular milieu” places patients at higher baseline risk of bleeding even before endovascular manipulation. Therefore, preoperative PAR, as an integrated indicator, effectively reflects the inherent fragility of the vascular wall and provides important predictive information for postoperative bleeding risk. However, optimal PAR thresholds may vary across populations and contexts, underscoring the need for validation in larger, multicenter cohorts. Despite these constraints, accumulating evidence supports PAR as a cost-effective indicator for infection risk stratification and severity assessment.
The inverse L-shaped association between PAR and bleeding risk reflects bidirectional pathophysiological mechanisms operating at distinct thresholds. When PAR is <5.05, synergistic interactions between platelets and ALB confer protective effects. Platelet levels ≥150 × 109/L facilitate primary hemostasis through the glycoprotein Ib/IX/V complex (GPIbα, GPIbβ, GPIX, and GPV), which mediates von Willebrand factor–dependent platelet adhesion at sites of vascular injury under high-shear stress. 22 Additionally, serum ALB levels ≥37 g/L preserve BBB integrity by stabilizing tight junction proteins (claudin-5 and occludin), inhibiting MMP-9 activity, and mitigating oxidative stress through intrinsic antioxidant properties. 23 The anti-inflammatory capacity of ALB further suppresses neuronal apoptosis following BBB compromise. 24 Conversely, when PAR >5.05, it may indicate pathological states characterized by inflammation-driven thrombocytopathy and relative hypoalbuminemia. Reduced availability of ALB impairs glutathione synthesis, thereby compromising endogenous antioxidant defenses. 25 Notably, ALB exerts regulatory influence over MMP-9, a zinc-dependent protease that degrades extracellular matrix components and tight junction proteins. This occurs through dual mechanisms, including zinc chelation and transcriptional downregulation, thereby helping prevent BBB disruption during ischemic events.26,27 This mechanistic interplay collectively underpins the inverse L-shaped association of PAR with hemorrhagic outcomes in ischemic stroke.
The clinical relevance of these findings is supported by extensive evidence linking hypoalbuminemia to increased morbidity and mortality in patients with stroke. Reduced ALB levels (<3.5 g/dL) are associated with heightened risks of cardiovascular complications, prolonged hospitalization, and delayed recovery, likely due to compromised BBB integrity and unmitigated neuroinflammation.28,29 Concurrently, MMP-9 serves as a crucial mediator of BBB disruption and hemorrhagic transformation in ischemic stroke, with dysregulated activity resulting in cerebrovascular damage through extracellular matrix degradation and tight junction proteolysis. 30 Elevated MMP-9 levels in plasma and cerebrospinal fluid are strongly associated with stroke severity, BBB permeability, and adverse clinical outcomes, as evidenced by increased serum protein extravasation, neutrophil infiltration, and edema formation in both experimental and clinical studies.30,31 Notably, the early post-ischemic surge of this protease destabilizes the neurovascular unit by degrading collagen IV, laminin, and zonula occludens-1 (ZO-1), thereby predisposing patients to vasogenic edema and secondary hemorrhage. 32 Albumin mitigates this pathological cascade by inhibiting MMP-9 activity.
Our study advances PAR research through three principal contributions: first, it provides preliminary validation within neuroendovascular contexts; second, it identifies a clinically actionable threshold (PAR = 5.05) through segmented regression; and third, it demonstrates superior net benefit compared with current practices via DCA. However, several limitations must be acknowledged. First, this single-center, retrospective study may introduce selection bias and unmeasured confounding. Moreover, the absence of external validation in an independent cohort suggests that the observed nonlinear relationship between PAR and postoperative bleeding, along with the identified inflection point (5.05), has not yet been confirmed in other populations. Second, as this was a retrospective study based on medical records, the absence of measurements of inflammatory cytokines (e.g. interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α)) and endothelial function markers (e.g. vascular cell adhesion molecule-1 (VCAM-1) and intercellular adhesion molecule-1 (ICAM-1)) limits mechanistic exploration of the relationship between PAR and vascular inflammation or endothelial injury. Furthermore, although liver disease history and hepatic enzyme indices did not significantly confound the independent predictive value of PAR in the present study, interpretation of PAR levels should still consider potential confounders, including, but not limited to, chronic liver disease, malignancy, and other conditions affecting platelet and ALB homeostasis. Further prospective, multicenter studies with larger sample sizes and external validation cohorts are warranted to establish the predictive value of PAR for postoperative bleeding following endovascular treatment of IAs, determine its optimal cutoff value and applicability across diverse populations, and provide a stronger evidence base for individualized risk stratification and perioperative management. In addition, the absence of measurements of inflammatory cytokines and endothelial function markers limits mechanistic exploration of the relationship between PAR and vascular inflammation or endothelial injury. Our subsequent research will focus on conducting multicenter, prospective cohort studies to validate and generalize these preliminary findings.
Conclusion
PAR is independently associated with postoperative bleeding following endovascular treatment of IAs, with a nonlinear relationship and an inflection point at 5.05. Patients with PAR below this threshold may require closer perioperative monitoring. However, the predictive performance of PAR did not meet the threshold for a standalone clinical tool, and the single-center retrospective design limits generalizability. Therefore, PAR should be considered an adjunctive marker within a multimodal risk assessment framework rather than a standalone decision-making criterion. In clinical practice, direct anticoagulation adjustment based solely on PAR is not recommended, as reducing anticoagulation intensity may increase thromboembolic risk, a more common complication after coiling. PAR is more effectively integrated with imaging, clinical scores, and other biomarkers to support individualized balancing of bleeding and ischemic risks.
Supplemental Material
sj-docx-1-imr-10.1177_03000605261448081 - Supplemental material for Platelet-to-albumin ratio and postoperative bleeding after endovascular treatment of intracranial aneurysms: A retrospective cohort study
Supplemental material, sj-docx-1-imr-10.1177_03000605261448081 for Platelet-to-albumin ratio and postoperative bleeding after endovascular treatment of intracranial aneurysms: A retrospective cohort study by Hong Liu and Zhengjun Wu in Journal of International Medical Research
Footnotes
Acknowledgments
The authors thank all the clinicians and staff at Guangyuan Central Hospital for their assistance in data collection.
Author contributions
Zhengjun Wu and Hong Liu conceived and designed the study. Hong Liu contributed to data collection and analysis. Zhengjun Wu drafted the manuscript. Hong Liu provided critical revisions and supervised the overall research process. All authors read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.