
Abstract
Objective
To investigate the mediating role of serum lipids in the association between dietary fiber intake and gallstones prevalence.
Methods
This study analyzed the data from 4896 adults participating in the National Health and Nutrition Examination Survey conducted between 2017–March 2020 and August 2021–August 2023. Logistic regression models and subgroup analyses were conducted to assess the correlation between dietary fiber intake and gallstone prevalence. Additionally, smooth curve fitting based on the generalized additive model was applied to elucidate nonlinear relationships. The mediating effects of lipid-related indicators, including low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, total cholesterol, non-high-density lipoprotein cholesterol, residual cholesterol, and atherogenic index of plasma were also evaluated.
Results
High-density lipoprotein cholesterol and atherogenic index of plasma significantly mediated the association between dietary fiber intake and gallstone prevalence, with mediation proportions of 5.06% and 4.26%, respectively (all p < 0.05). Conversely, the mediating effects of other lipid parameters (non-high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, total cholesterol, triglycerides, and residual cholesterol) were not statistically significant.
Conclusion
There exists a complex relationship between dietary fiber intake, serum lipid levels, and gallstone formation, with serum lipids potentially serving as mediators. Future research should explore this mechanism in greater depth to offer new insights for the prevention and treatment of gallstones.
Keywords
Introduction
Gallstones, a common biliary tract disease, affect approximately 20% of adults globally 1 and represent the most common digestive system disorder necessitating hospitalization in Western countries. 2 Their occurrence is closely linked to various factors. In recent years, with advancements in nutritional and medical research, the relationship between dietary fiber intake and gallstones formation has received increasing attention. Concurrently, dyslipidemia, a significant risk factor for cardiovascular diseases, has also been implicated in the development of gallstones. 3 Therefore, investigating the mediating role of serum lipids in the relationship between dietary fiber intake and gallstones is crucial. This investigation can enhance our understanding of gallstones pathogenesis and help develop effective prevention strategies. Dietary fiber, an indispensable and vital component of the human diet, confers multiple health benefits. It comprises non-starch polysaccharides indigestible by human gastrointestinal enzymes, along with structurally similar lignin. Found mainly in plant cell walls, dietary fiber does not provide energy but plays a crucial role in maintaining good health by increasing fecal bulk, promoting weight loss, lowering blood pressure, reducing postprandial blood glucose and insulin responses, decreasing total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C) levels, exerting prebiotic effects, and potentially preventing cancer. 4 Notably, dietary fiber intake exhibits a significant inverse association with type 2 diabetes, cardiovascular diseases, hyperuricemia, inflammatory bowel disease, and various malignancies, including ovarian, colon, bladder, and premenopausal breast cancers.5–9 Furthermore, clinical studies have indicated that dietary fiber supplementation effectively prevents gallstones formation in obese patients undergoing diet-induced weight loss. 10
Lipid metabolism disorders, particularly low levels of high-density lipoprotein cholesterol (HDL-C), constitute significant risk factors for gallstones formation. 11 Although both dietary fiber intake and dyslipidemia are established risk factors for gallstones, the specific pathways underlying their interaction remain incompletely characterized. Serum lipid levels may act as key mediating factors between dietary fiber intake and gallstones pathogenesis. This study aimed to investigate the mediating role of serum levels in the association between dietary fiber intake and gallstones. The findings of this research will not only advance our understanding of gallstones pathogenesis but also provide a robust scientific foundation for developing evidence-based prevention strategies. Furthermore, they have significant implications in the promotion of healthy dietary patterns and reduction in the risk of both gallstones and cardiovascular diseases.
Materials and methods
Study population
The data source was the National Health and Nutrition Examination Survey (NHANES) administered by the National Center for Health Statistics (NCHS). The NHANES is a nationwide survey designed to comprehensively collect data through laboratory tests, physical examinations, and interviews from the US population in order to monitor the health and nutritional status of adults and children in the US. All relevant data can be downloaded from the official NHANES website (http://www.cdc.gov/nchs/nhanes.htm). The NHANES protocol was approved by the Ethics Review Board of the Centers for Disease Control and Prevention and NCHS, ensuring that all participants had signed written informed consent forms. This study was conducted in accordance with the Declaration of Helsinki (1975 version, revised in 2024).
This cross-sectional study initially involved 27,493 individuals; among these, 22,597 were excluded owing to the following reasons: (a) missing demographic information (n = 13,196); (b) missing data on presence of gallstones (n = 9); and (c) incomplete covariate data (n = 9392). In total, 4896 participants (2325 men and 2571 female) were ultimately included. The screening process is illustrated in Figure 1.

Flowchart of participant selection.
Diagnosis of gallstones
The gallstones statistics were derived using the multiple-choice questionnaire, which asked, “Has a doctor or other healthcare professional ever told you that you have gallstones?” to determine the presence of gallstones. 12
Dietary fiber intake
Dietary fiber intake data were collected through 24-h dietary recall interviews. The first recall was administered by trained interviewers at mobile examination centers, whereas the second was conducted via telephone interviews 3–10 days later. To ensure the validity of study findings, maintain an adequate sample size, and mitigate potential discrepancies arising from the use of two distinct survey methodologies, only data from the first recall were utilized for analytical purposes.
Covariates
We assessed multicollinearity among covariates using the variance inflation factor (VIF). All variables had a VIF <5, indicating no substantial multicollinearity. Thus, we concluded that the covariates were independent, and the regression estimates were stable (Figure 2).
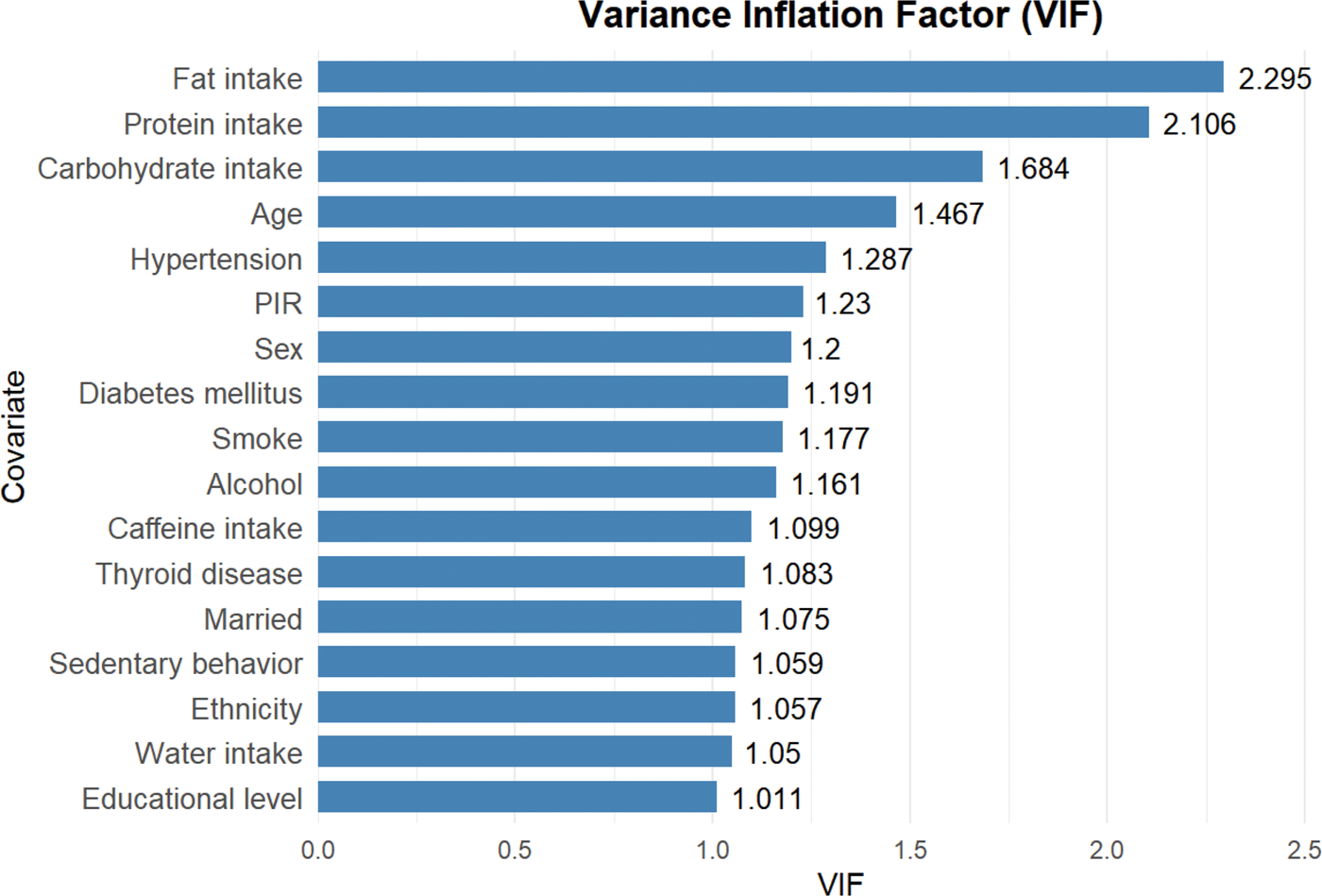
Multicollinearity analysis of the covariates in this study.
Sociodemographic characteristics included age, sex, race (Mexican American, non-Hispanic White, non-Hispanic Black, and Other races), marital status, educational level, and poverty-income ratio (PIR). Marital status was categorized as cohabiting (married/living with a partner) or living alone (widowed/divorced/separated/never married). The PIR was stratified into three tiers, including low income (PIR < 1.3), middle income (1.3 ≤ PIR< 3.5), and high income (PIR ≥ 3.5). Educational level was classified into three categories: (a) less than high school completion, below 9th grade, 9th to 11th grade, or 12th grade without diploma; (b) high school graduation, including high school diploma or General Educational Development (GED) or equivalent; and (c) post-secondary education, including some college or Associate of Arts (AA) degree and college graduation or above. Dietary data were collected via 24-h dietary recall interviews. For analytical purposes, we utilized data from the first survey, encompassing protein, carbohydrate, fat, dietary fiber, caffeine, and water intakes. Health-related variables comprised diabetes, hypertension, thyroid disease, sedentary behavior (minutes), smoking status, and alcohol consumption. Detailed measurement methods and data collection for each variable are available at www.cdc.gov/nchs/nhanes.
Statistical analyses
All statistical analyses were conducted using R (version 4.3.2, http://www.R-project.org) and EmpowerStats (version 4.2, http://www.empowerstats.com). Statistical significance was defined at a p-value <0.05. To ensure national representativeness, all analyses incorporated the complex sampling design of the NHANES, including stratification, clustering, and sampling weights. Continuous variables were summarized as weighted means ± standard errors, whereas categorical variables were presented as weighted proportions (numbers). Group comparisons for continuous variables were performed using Student’s t-tests, and chi-square tests were applied for categorical variables.
Weighted logistic regression analysis was performed to determine the odds ratios (ORs) and 95% confidence intervals (CIs) for the association between dietary fiber intake and gallstones. In this study, four logistic regression models were constructed with adjustment for different sets of confounding factors. Model 1 was an unadjusted crude model with no covariate included. Model 2 was adjusted for demographic characteristics, including age, sex, race/ethnicity, educational level, marital status, and PIR. Model 3 was further adjusted for dietary factors in addition to the covariates in Model 2, including intakes of protein, fat, caffeine, carbohydrates, and water. Model 4 was the fully adjusted model, which additionally controlled for health‑related variables, including diabetes, hypertension, thyroid disease, sedentary behavior, smoking status, and alcohol consumption. Dietary fiber intake was analyzed both as a continuous and categorical variable based on quartiles (Q1–Q4), and both forms were entered into the multivariable logistic regression models. GAM with smooth curve fitting were employed to characterize nonlinear associations between dietary fiber intake and gallstones risk. Subgroup analyses and interaction tests were used to identify potential differences among specific populations.
Herein, the ‘mediation’ package in R (version 4.3.2) was used to evaluate the mediating roles of lipid profile indicators (LDL-C, HDL-C, triglycerides (TGs), TC, non-high-density lipoprotein cholesterol (non-HDL-C), residual cholesterol (RC), and atherogenic index of plasma (AIP)) in the pathway linking dietary fiber intake to gallstones formation, with adjustments made for covariates; CIs for the indirect effects were estimated using the Bootstrap method with 1000 resamples, and the proportions of the mediation effects for each lipid parameter were calculated accordingly. 13
Results
Baseline characteristics of the study population
This study included a total of 4896 participants; among these, 536 had gallstones. Table 1 presents the baseline demographic characteristics of the cohort, categorized by gallstones status. The mean participant age was 48.65 years; the cohort comprised 49.23% male and 50.77% female. Compared with participants without gallstones, those with gallstones were older (p < 0.0001). Furthermore, the cohort with gallstones had a higher proportion of women (p < 0.0001) and individuals aged ≥60 years (p < 0.0001). The non-Hispanic White ethnicity was overrepresented, whereas non-Hispanic Black ethnicity was underrepresented (p = 0.04). With respect to socioeconomic characteristics, the gallstones group had a greater proportion of individuals with low income and a lower proportion with high income (p = 0.01). In terms of health variables, diabetes, hypertension, and thyroid disease were more prevalent (p < 0.0001) in the gallstones group. With respect to lifestyle, past alcohol consumption was more common, whereas heavy drinking was less common (p < 0.0001) in the gallstones group. Dietary intake data revealed that the intakes of protein, carbohydrates, fat, and dietary fiber were significantly lower (p < 0.0001) and the levels of the lipid markers, TG and AIP, were significantly higher (p = 0.02) in the gallstones group. No significant differences were observed in the marital status; educational level; smoking status; caffeine intake; sedentary behavior; and TC, LDL-C, or HDL-C levels between the two groups (all p > 0.05).
Basic characteristics of study participants.

PIR: poverty-income ratio; IFG: impaired fasting glucose; TG: triglycerides; TC: total cholesterol; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; AIP: atherogenic index of plasma.
Association of dietary fiber intake with gallstone disease prevalence
Further multivariable logistic regression analyses were performed with sequential adjustment for confounding factors (Table 2). When dietary fiber intake was modeled as a continuous variable, it exhibited a protective association against gallstone disease across all models. Dietary fiber intake was categorized into quartiles (Q1 as the lowest and Q4 as the highest quartile), with Q1 used as the reference. For Q2 (9.2–14.2 g/day), the ORs across the four models ranged from 0.86 to 0.97, with all p-values >0.05, indicating no statistically significant association. For Q3 (14.2–21.1 g/day), significant associations were observed in Models 1–3 (OR: 0.59–0.67); however, this association lost statistical significance in Model 4 (OR = 0.73, p = 0.73). For Q4 (21.1–117.3 g/day), significant associations were also observed in Models 1–3 (OR: 0.44–0.60); however, the association became nonsignificant in Model 4 (OR = 0.64, p = 0.64). Trend tests were significant across all models (p for trend <0.05), suggesting a linear trend between dietary fiber intake and risk of gallstones. Based on these results, we characterized the nonlinear relationship between dietary fiber intake and gallstones using GAM with smooth curve fitting. As dietary fiber intake increased, gallstones prevalence progressively declined, demonstrating an inverse association (Figure 3).
Logistic regression analysis of the association between dietary fiber intake and gallstones.
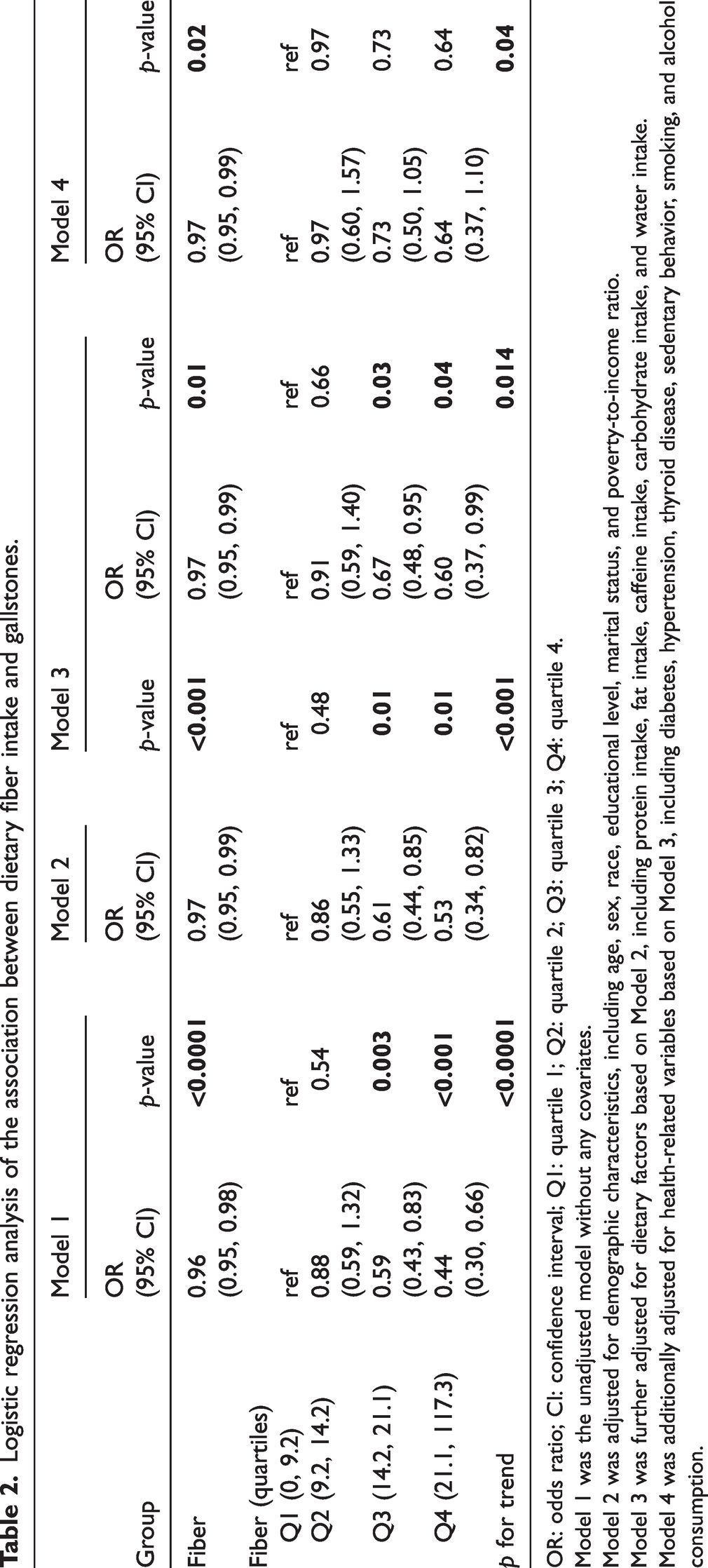
OR: odds ratio; CI: confidence interval; Q1: quartile 1; Q2: quartile 2; Q3: quartile 3; Q4: quartile 4.
Model 1 was the unadjusted model without any covariates.
Model 2 was adjusted for demographic characteristics, including age, sex, race, educational level, marital status, and poverty-to-income ratio.
Model 3 was further adjusted for dietary factors based on Model 2, including protein intake, fat intake, caffeine intake, carbohydrate intake, and water intake.
Model 4 was additionally adjusted for health-related variables based on Model 3, including diabetes, hypertension, thyroid disease, sedentary behavior, smoking, and alcohol consumption.
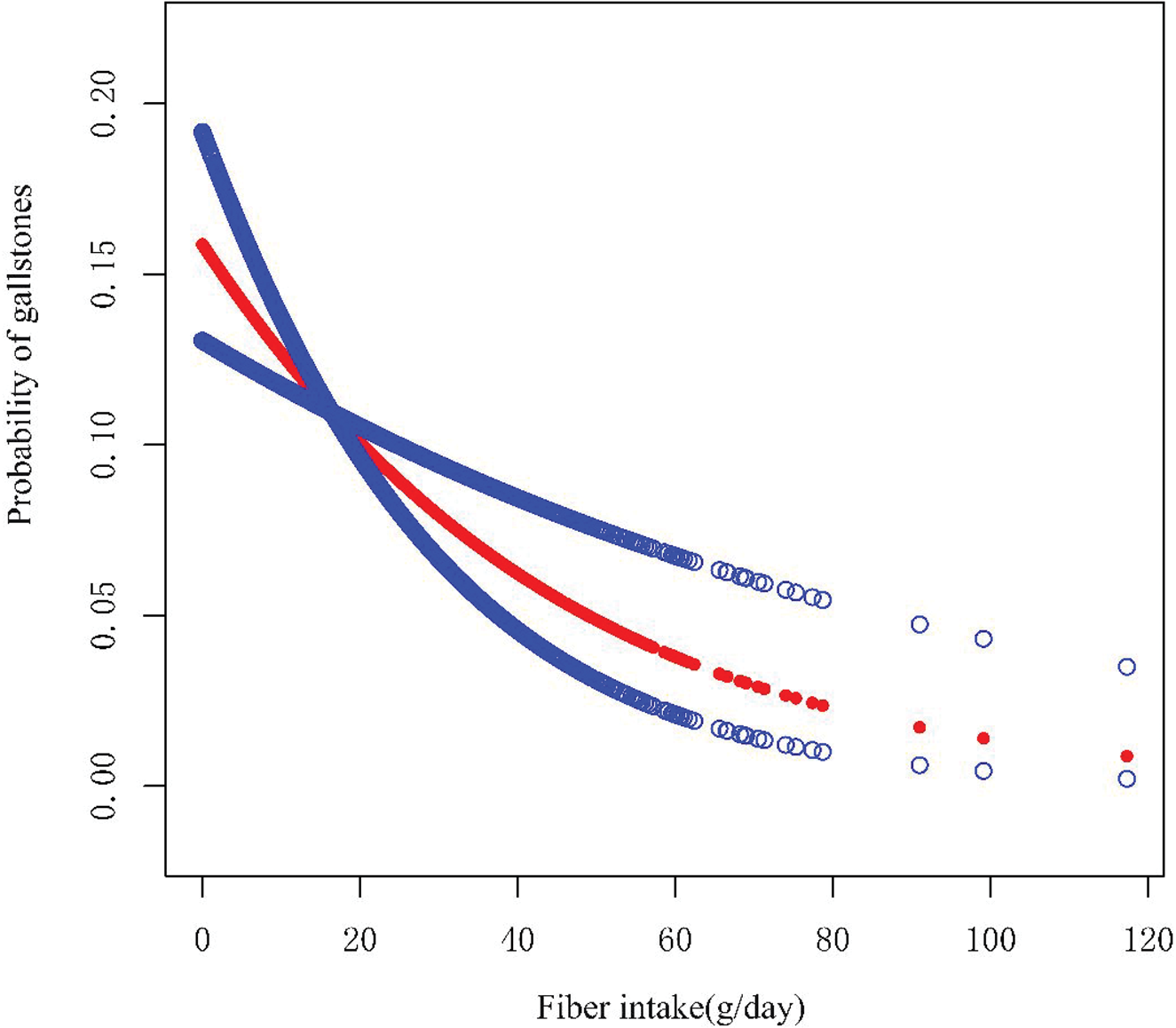
Nonlinear relationship between dietary fiber intake and gallstones. The smooth curve fitting plot was generated using generalized additive models in EmpowerStats (version 4.2). No nonlinear association was observed between dietary fiber intake (g/day) and occurrence of gallstones (p for nonlinearity >0.05). In the figure, the solid curve represents the smooth fit between the two variables, whereas the blue band denotes the 95% confidence interval of the fitted values. The model was adjusted for the following confounding factors: age, sex, race, educational level, marital status, poverty-to-income ratio, protein intake, fat intake, caffeine intake, carbohydrate intake, water intake, as well as the presence of diabetes, hypertension, thyroid disease, sedentary behavior, smoking, and alcohol consumption.
According to the subgroup analysis (Table 3), the inverse association between dietary fiber intake and gallstones risk remained consistent across most subgroups. However, a significant interaction was detected for diabetes status (p for interaction = 0.01). The protective effect of dietary fiber was more pronounced in the nondiabetic subgroup, whereas this association was attenuated and became nonsignificant among individuals with diabetes.
Results of subgroup and interaction analyses.
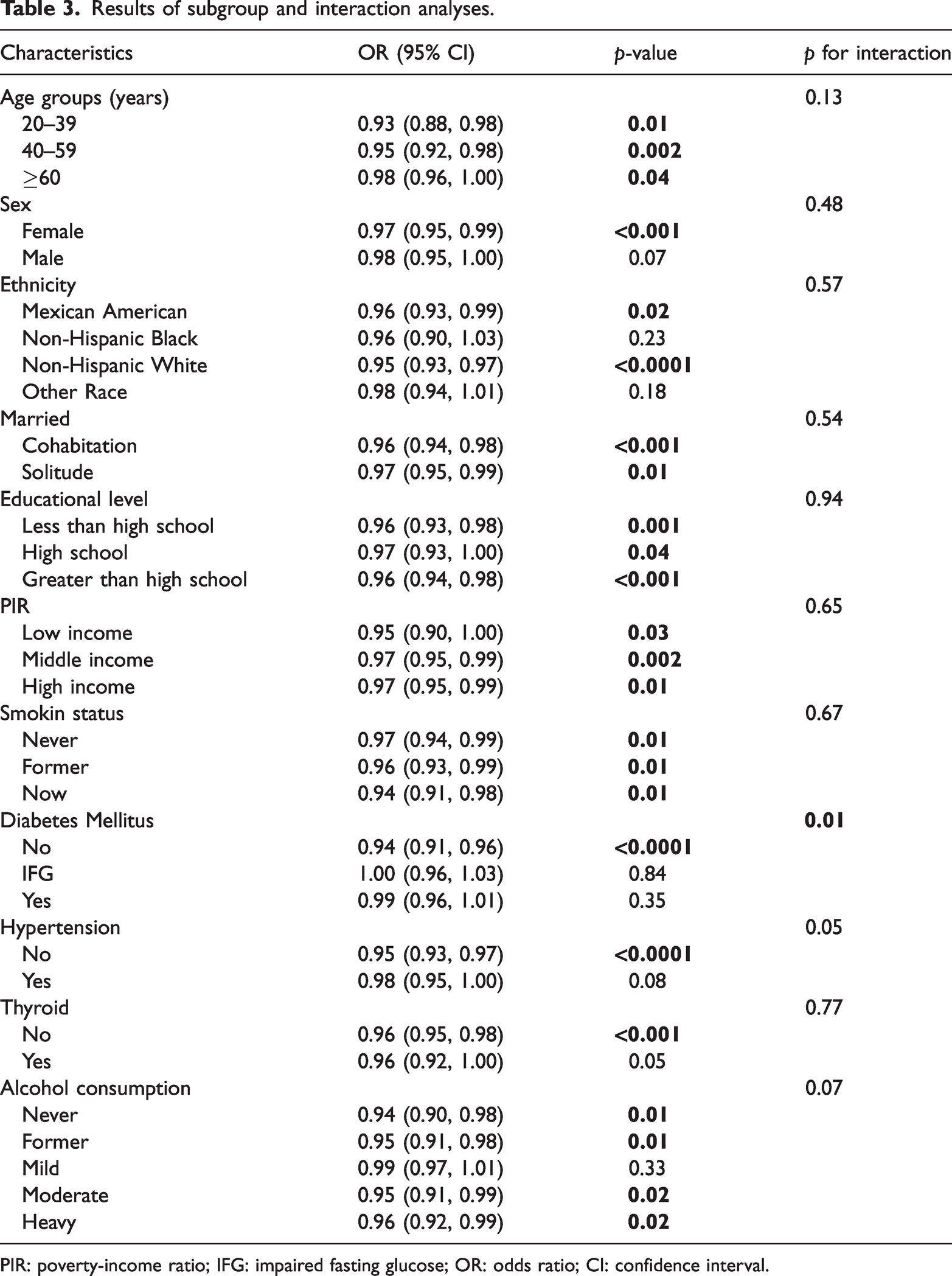
PIR: poverty-income ratio; IFG: impaired fasting glucose; OR: odds ratio; CI: confidence interval.
Mediator analysis of serum lipid
We conducted mediation analysis to evaluate the potential role of lipid-related indicators in the association between dietary fiber intake and gallstones. Significant mediating effects of HDL-C and AIP were observed in the dietary fiber–gallstones association, explaining 5.06% and 4.26% of the mediation, respectively (both p < 0.05, Figure 4). In addition, we evaluated the mediating effects of other lipid-related indicators, including non-HDL-C, LDL-C, TC, TG, and RC; none of these mediating effects reached statistical significance. Further mediation analyses performed in subgroup populations demonstrated that the significant mediating roles of HDL-C and AIP in the association between dietary fiber intake and gallstones risk were only present in the following subgroups: (a) females; (b) non-Hispanic White individuals; (c) those aged 20–39 years; (d) cohabiting participants; (e) individuals with educational level above high school; (f) alcohol consumers; (g) never smokers; (h) and participants with no history of diabetes, hypertension, or thyroid disease (see Supplementary Figures S1–S10).
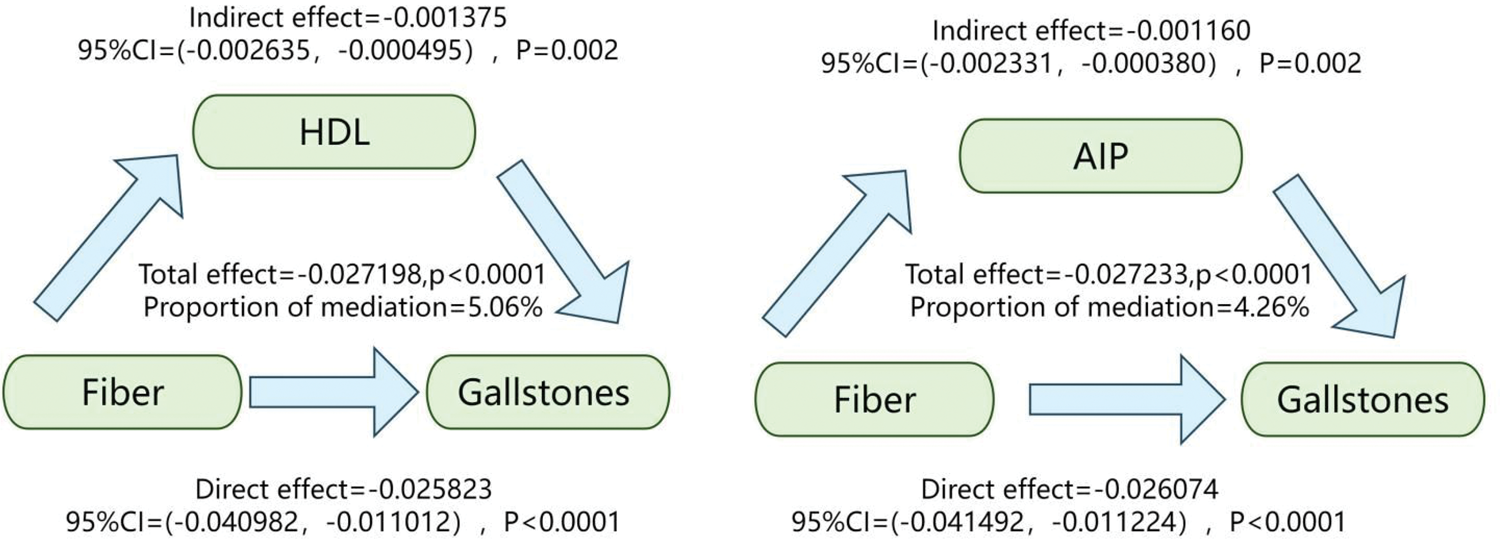
Mediating role of HDL-C (left) and AIP (right). HDL-C: high-density lipoprotein cholesterol; AIP: atherogenic index of plasma.
Discussion
The present results align with those of multiple cohort studies that have also demonstrated the protective effect of dietary fiber against gallstones.10,14 Crucially, our analysis uncovered the mediating role of serum lipid levels (particularly HDL-C and AIP) in the association between dietary fiber and gallstones. Increased dietary fiber intake partially reduces gallstones risk by ameliorating lipid metabolism.
The observed inverse correlation between dietary fiber intake and gallstones risk in this study may involve mechanisms beyond those explained by the involvement of serum lipids. Approximately 95% of bile acids undergo reabsorption in the ileum. These reabsorbed bile acids return to the liver via enterohepatic circulation. Dietary fiber can bind to primary bile acids (particularly cholic acid) forming nonabsorbable complexes. These complexes inhibit the enterohepatic reabsorption of primary bile acids and enhance their fecal excretion. 15 This process reduces bile acid concentration in the bile, thereby preventing the supersaturation and crystallization of cholesterol, 16 which ultimately suppresses cholesterol stone formation. Furthermore, low fiber intake is linked to impaired gallbladder motility, allowing adequate time for cholesterol nucleation and gallstones growth. 17 Reduced fiber consumption may also weaken colonic motility, prolonging intestinal bile acid retention, consequently heightening the risk of gallstones formation. 14
Herein, participants in the gallstones group differed significantly from those in the no gallstones group in terms of demographic characteristics, dietary intake, socioeconomic status, and comorbidity profiles. Specifically, individuals with gallstones were older, predominantly female, and had lower income levels; they also exhibited generally reduced dietary intake, including lower intake of protein, carbohydrates, fat, dietary fiber, and water, alongside a higher prevalence of comorbidities such as diabetes, hypertension, thyroid disease, and hypertriglyceridemia. Interaction analysis revealed a significant interaction effect of diabetes history on gallstones risk (p for interaction = 0.01), with the protective effect of dietary fiber intake only observed among participants without a history of diabetes. The risk factors for gallstones are primarily classified as unmodifiable and modifiable. 17 The observed unmodifiable factors—such as aging and female sex—align with established findings, thereby validating this study’s design. Female predisposition to gallstones likely stemmed from estrogen-driven mechanisms such as enhanced hepatic cholesterol production/secretion that promotes stone formation and reduced bile salt synthesis mediated by estrogen receptor 1 and G protein-coupled receptor 30 (GPR30) upregulation.18,19 Furthermore, pregnancy and oral contraceptive use constitute additional risk factors, primarily owing to their association with gallbladder motility impairment. Modifiable risk factors include diabetes, metabolic syndrome, sedentary behavior, obesity, and imbalanced nutritional patterns—specifically excessive calorie, carbohydrate, and fat intake coupled with inadequate dietary fiber intake, among others. 20 Unexpectedly, compared with those without gallstones, patients with gallstones had markedly lower consumption of protein, carbohydrates, and fat, which may reflect adaptive dietary modifications following diagnosis. This study reinforces the established association between gallstones and multiple metabolic/chronic comorbidities. Specifically, the elevated gallstones risk in diabetic populations is well-documented, with diabetic patients exhibiting a 1.75-fold higher risk than nondiabetic individuals, 21 likely due to impaired gallbladder emptying and reduced bile salt secretion. 22 The hypertension–gallstones association may stem from leptin elevation induced by hypertension. This process triggers gallbladder wall inflammation and impairs contractile function, causing bile stasis. Concurrently, it induces hyperinsulinemia that produces cholesterol-supersaturated bile and directly alters biliary composition, synergistically promoting gallstones formation. 23 We found a highly significant association between thyroid disorders and gallstones (p < 0.0001), underscoring the critical role of thyroid function in bile metabolism. Specifically, thyroid hormone levels directly regulate cholesterol crystallization risk and gallstones formation. Studies have demonstrated that hyperthyroidism promotes cholesterol gallstones formation through the upregulation of hepatic nuclear receptors, liver X receptor alpha (LXRα) and retinoid X receptor, which are core regulators of cholesterol metabolism. However, hypothyroidism contributes to cholesterol gallstones formation by increasing cholesterol biosynthesis. 24 One of the most notable findings of this study was the significant interaction effect of diabetes history on gallstones risk (p for interaction = 0.01), with the protective effect of dietary fiber exclusively detected in participants without a history of diabetes. Metabolic disturbances in diabetic patients are often accompanied with insulin resistance, which may disrupt the metabolic protective pathways mediated by dietary fiber, thereby diminishing its protective effects against gallstones formation. For hypertension (p for interaction = 0.05), the observed pattern was consistent with that of diabetes; a significant protective effect of dietary fiber intake was only found in nonhypertensive individuals. This phenomenon may be linked to the elevated leptin levels discussed previously; thus, dietary fiber intervention alone may exert limited protective effect against gallstones formation in hypertensive individuals. Furthermore, the pattern and magnitude of the effects linked to certain traditional gallstones risk factors may be modified within these specific subgroups. For individuals in these subgroups, simply increasing dietary fiber intake may not be adequate to counteract their underlying pathophysiological abnormalities. Given the potential implications for the development of precision nutrition and precision medicine strategies targeting gallstones prevention, further large-scale and in-depth mechanistic studies are strongly warranted.
More importantly, our mediation analysis demonstrated that serum lipid parameters—specifically HDL-C and the AIP—serve as significant mediating pathways through which dietary fiber intake affects gallstones risk. In further subgroup mediation analyses, the significant mediating effects of HDL-C and AIP on the association between dietary fiber intake and gallstones risk were identified only in the following subgroups: non-Hispanic White individuals, those aged 20–39 years, cohabiting participants, individuals with educational level above high school, alcohol consumers, never smokers, and participants without diabetes, hypertension, or thyroid disease. The aforementioned populations are predominantly classified as having low metabolic risk, with no systemic metabolic disturbances induced by chronic diseases (including chronic inflammation, oxidative stress, and insulin resistance). Accordingly, the “dietary fiber–serum lipids–gallstones” pathway is more readily and reliably detected in these cohorts. The prevalence of cholesterol gallstones is significantly higher among non-Hispanic White individuals than in other ethnic groups, and the mediating effect of serum lipids is correspondingly more prominent. In contrast, the smaller sample sizes among other ethnic groups resulted in insufficient statistical power, meaning that even a genuine but weak mediating effect could not be identified at a statistically significant level. Middle-aged and older individuals have a longer duration of exposure to risk factors, and the longer-term, cumulative effects of multiple conditions, including obesity, metabolic syndrome, previous pregnancy, and impaired gallbladder emptying, weaken the relative contribution of the lipid pathway to the overall pathogenic effect. In contrast, younger individuals tend to have relatively fewer pathogenic risk factors, making the role of this pathway more distinct and observable. Cohabiting individuals generally follow a regular family dietary pattern, which ensures more stable dietary fiber intake. Furthermore, cohabitation provides substantial social support and emotional comfort, effectively alleviating adverse psychological states such as depression and anxiety, and thus indirectly modulating systemic lipid metabolism. Individuals with higher educational level generally have stronger health awareness and more adequate time and resources to maintain a balanced, healthy diet. Moderate alcohol consumption is closely associated with elevated HDL-C levels, likely through inhibition of cholesteryl ester transfer protein (CETP)-mediated conversion of HDL-C to LDL-C, which reduced biliary cholesterol saturation. Meanwhile, modest alcohol intake enhances gallbladder contractility, exerting a synergistic protective effect in combination with dietary fiber intake. 14 However, strict caution is required regarding the severe health risks linked to excessive alcohol consumption, including fatty liver disease, alcoholic cirrhosis, and pancreatitis.
Dietary fiber, especially soluble dietary fiber, has been proven to more effectively reduce serum TC and LDL-C levels in both adults and children. 25 Evidence from clinical trials performed on Asian populations suggests that dietary fiber intake exerts beneficial effects on HDL-C metabolism. 26 Specifically, in a prospective interventional study involving 14 overweight or obese women with hypertension, daily supplementation of mixed dietary fiber (12 g for 8 weeks) significantly increased HDL-C levels and reduced blood pressure. 27 Notably, a study by Zhang et al. 28 involving Chinese adults with mild-to-moderate hypercholesterolemia provided further supportive evidence. During the 6-week trial, compared with the control group that consumed wheat flour noodles (100 g/day), the intervention group receiving instant oat cereal (100 g/day) demonstrated significantly higher dietary fiber intake. More critically, the control group demonstrated a significant reduction in HDL-C levels compared with the oats group by the end of the intervention period. Furthermore, a Chinese trial involving 1034 rural-to-urban migrant workers investigated the association between daily dietary fiber intake and serum lipid profiles. The results suggest that daily fiber intake >30 g may significantly improve plasma HDL-C levels in men. 29 The core lipid-lowering mechanism of dietary fiber initiates with microbial fermentation in the colon, which produces short-chain fatty acids (SCFAs)—primarily butyrate, acetate, and propionate. These metabolites regulate lipid metabolism through the activation of G protein-coupled receptor 41 (GPR41), G protein-coupled receptor (GPR43), and peroxisome proliferator-activated receptor γ (PPAR-γ). 30 Simultaneously, acetate and propionate may suppress endogenous lipolysis, whereas propionate specifically upregulates lipoprotein lipase expression to accelerate extracellular lipoprotein hydrolysis. Both mechanisms collectively reduce circulating plasma lipid levels and decrease body weight. 31 Moreover, butyrate improves lipid metabolism through a dual mechanism; it activates uncoupling proteins (UCPs) to stimulate mitochondrial thermogenesis, thereby increasing energy expenditure and lipid oxidation. Concurrently, butyrate upregulates adiponectin secretion, which enhances insulin sensitivity and promotes fatty acid metabolism. These synergistic actions collectively reduce serum lipid levels. 32 More importantly, butyrate can regulate the secretion of apolipoprotein A-IV (apoA-IV), thereby modulating reverse cholesterol transport, which may increase HDL-C levels, 33 potentially explaining how dietary fiber intake influenced the gallstones risk through HDL-C in this study. When dietary fiber intake is insufficient, the gut microbiota shifts toward proteolytic and lipolytic metabolisms, leading to the accumulation of harmful metabolites such as lipopolysaccharides (LPS).34–36 This induces dysbiosis-associated metabolic endotoxemia, triggering chronic low-grade inflammation and oxidative stress, which ultimately contribute to hyperlipidemia, insulin resistance, β-cell dysfunction, hyperglycemia, and obesity. 37 Moreover, soluble and viscous fibers reduce lipid absorption by delaying gastric emptying, enhancing bile acid excretion, modulating the gut microbiome, and ameliorating insulin resistance—which is associated with elevated cholesterol synthesis. 38 Simultaneously, they reduce serum lipids by lowering the total energy intake owing to their low caloric density, slower digestion rate, and higher satiety. 25 The lipid-lowering physiological effects of dietary fiber are modulated by its water solubility, water holding capacity, viscosity, particle size, fermentability, colonic pH alterations, cation exchange capacity, and organic acid absorption. 25
Dyslipidemia is closely linked to gallstones formation; the relationship between serum TC, LDL-C, and HDL-C levels and cholesterol gallstones development is multifactorial and complex. 39 Serum TC levels are closely associated with gallstones risk. In a meta-analysis integrating multicenter cross-sectional data, elevated serum TC levels significantly increased the risk of gallstones. 40 Elevated serum TC levels contribute to gallstones pathogenesis through two key mechanisms. First, they increase the cholesterol saturation index (CSI), causing biliary cholesterol concentration to exceed the micellar solubility limits; second, they accelerate cholesterol crystal nucleation by promoting precipitation from supersaturated bile. Both processes constitute critical precursors for gallstones formation. 40 Moreover, elevated TC levels may impair cholecystokinin (CCK) sensitivity and exacerbate gallstones risk by increasing bile cholesterol saturation and viscosity through mucin hypersecretion. 41 In addition to TC, lipid parameters—notably HDL-C—substantially contribute to gallstones pathogenesis. Andreotti et al. have demonstrated that HDL-C, a critical cholesterol transporter, significantly reduces gallstones incidence. Conversely, reduced HDL-C levels increase the gallstones formation risk by 4.2-fold. 42 Studies have demonstrated that elevated serum HDL-C levels enhance hepatic bile acid synthesis, reduce the CSI, and thereby improve cholesterol solubility in bile—effectively preventing gallstones formation. 40 Current research focuses on the association between LDL-C level and cholelithiasis risk. Genetic evidence has demonstrated that distinct LDL-C-lowering pathways exert divergent effects on gallstones pathogenesis. Statins may reduce the risk, whereas proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors and apolipoprotein B (apoB)-targeted therapies increase susceptibility; modulation through glycosphingolipid biosynthesis pathways decreases the risk, whereas interventions involving plasma lipoprotein assembly/remodeling/clearance or adenosine triphosphate (ATP)–binding cassette (ABC) transporters elevate the risk. 43
Despite the valuable findings of this study, certain limitations should be noted. First, the cross-sectional design precludes the establishment of causal relationships between dietary fiber intake, serum lipid levels, and gallstones formation. Future prospective cohort studies or randomized controlled trials are therefore needed to validate these associations and elucidate the underlying mechanisms. Second, although multivariable adjustment was performed to account for known confounders (e.g. age, sex, and protein intake), residual confounding due to unmeasured factors cannot be ruled out. Third, the mediation analysis revealed only partial mediating effects, suggesting the involvement of other potential pathways. For instance, inflammation is a well-recognized risk factor for gallstones, and further investigation is thus warranted to explore the role of inflammatory biomarkers in the relationship between dietary fiber intake and gallstones. Fourth, only a single 24-h dietary recall was performed to measure dietary fiber intake in this study. Although this approach helps minimize within-person day-to-day variability, a single recall may not accurately capture habitual dietary fiber intake. Dietary intake is subject to periodic fluctuations (e.g. between weekdays and weekends as well as seasonal variations), which cannot be accounted for by a single measurement. Moreover, such a measurement error may introduce regression dilution bias, potentially attenuating the true association between dietary fiber intake and health outcomes toward the null.
Conclusions
An intricate interplay exists between dietary fiber intake, serum lipid levels, and gallstones formation, wherein serum lipids may act as mediators. Future research should attempt to elucidate the underlying mechanisms to inform novel preventive and therapeutic strategies for gallstones management.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605261451085 - Supplemental material for Dietary fiber intake and gallstones: The mediating role of serum lipids
Supplemental material, sj-pdf-1-imr-10.1177_03000605261451085 for Dietary fiber intake and gallstones: The mediating role of serum lipids by Wenli Jiang, Furui Wang, Yuyu Lin, Xiu Luo, Ya Zheng, Jun Yan, Wei Yang and Zenan Hu in Journal of International Medical Research
Footnotes
Acknowledgments
The authors would like to acknowledge the use of the National Health and Nutrition Examination Survey (NHANES) database. During the preparation of this manuscript, the authors used artificial intelligence tools to improve the language and readability.
Authors’ contributions
WJ designed the study, performed statistical analysis, and drafted the initial manuscript. FW, YL, and XL performed data cleaning. YZ and JY checked the content for errors. WY and ZH reviewed and revised the manuscript and were accountable for the final product. Consent from all authors was obtained prior to submission.
Data availability statement
Declaration of conflicting interests
The authors declare no competing interests.
Funding
This research was funded by the Regional Science Fund Project of the National Natural Science Foundation of China (No. 32460305).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.