
Abstract
Objective
To evaluate whether flexible family visitation reduces postoperative delirium in older patients admitted to an orthopedic intensive care unit and to explore whether its effects vary by surgical type.
Methods
This single-center, parallel-group randomized controlled trial enrolled patients aged ≥60 years who were admitted to the orthopedic intensive care unit within 24 h following orthopedic surgery. Participants were randomized to daytime flexible family visitation or routine restricted visitation. Delirium during intensive care unit stay was assessed daily using the Confusion Assessment Method for the Intensive Care Unit and the Intensive Care Delirium Screening Checklist. Secondary outcomes included sedative use, hospital-acquired infection, length of stay, and hospitalization costs.
Results
Among 405 participants, flexible visitation reduced delirium incidence (29.5% vs 44.4%, P = 0.002) and sedative use (32.0% vs 44.9%, P = 0.008). Patients undergoing cervical spine surgery showed the greatest benefit (36.5% vs 57.6%, P = 0.026). Flexible visitation did not increase hospital-acquired infections (3.5% vs 3.9%, P = 0.916) or length of stay (median, 16 days in both groups, P = 0.367) but lowered total hospitalization costs (P < 0.001). Flexible visitation may improve outcomes and reduce costs in high-risk orthopedic intensive care unit patients.
Conclusions
Flexible family visitation was associated with lower delirium burden, reduced sedative exposure, and lower hospitalization costs in older orthopedic intensive care unit patients, without increasing infection or prolonging hospitalization. The benefit appeared most pronounced after cervical spine surgery.
Keywords
Introduction
Postoperative delirium (POD) is a common acute cognitive disorder, particularly prevalent among older critically ill patients. It is characterized by fluctuations in consciousness, inattention, and cognitive decline, often accompanied by symptoms such as anxiety and hallucinations. POD significantly impairs short-term recovery and is associated with long-term cognitive deterioration, functional loss, and increased mortality rates.1,2 Older patients, owing to their baseline cognitive decline, increased comorbidities, and the stress of surgical trauma, are considered to be at high-risk for developing POD. 3 The incidence of POD in these patients can exceed 30%, with intensive care unit (ICU) patients, particularly those undergoing orthopedic surgery or admitted because of severe illness, showing an even higher incidence rate, reaching ≥40%. 4 The mechanisms through which different types of orthopedic surgeries contribute to POD may vary. For example, older patients undergoing spinal surgeries often experience prolonged bed rest, the use of immobilizing devices, and anxiety regarding potential neurological impairments, all of which may increase their anxiety and psychological burden and thereby raise the risk of developing delirium. 5 In contrast, hip surgery patients are generally older and more frail, and the occurrence of POD is influenced by a combination of physiological and psychological factors, such as advanced age, cognitive impairment, and surgical trauma. 6 Although both groups are considered high-risk for delirium, their recovery needs and postsurgical response mechanisms differ. Therefore, individualized interventions, particularly for delirium prevention and management, should be thoroughly addressed in future studies involving patients undergoing these distinct types of surgeries.
Family visitation, a non-pharmacological intervention, has been increasingly recognized for its positive effects on improving patients’ psychological well-being, reducing anxiety, and promoting recovery.7–9 Traditional ICU visitation policies are often strict, limiting the duration and frequency of family visits primarily for infection control and ICU environment management. However, studies have demonstrated that these restrictive policies may exacerbate patients’ feelings of loneliness and elevate their anxiety levels, which, in turn, can contribute to an increased incidence of POD. 10 In contrast, flexible visitation policies, which allow family members to stay at the bedside for longer periods, provide patients with more emotional support. 11 Studies have shown that flexible visitation policies can effectively improve patients’ emotional states, reduce the incidence of delirium, and are associated with lower rates of delirium and sedative use in various ICU settings.12,13
The primary aim of this study was to investigate the effect of flexible visitation on the prevention of POD in older orthopedic ICU patients and to examine its heterogeneous effects across different types of orthopedic surgeries. We focused on assessing the incidence of delirium in patients undergoing spinal and hip surgeries under a flexible visitation policy, further exploring whether this strategy can reduce patient anxiety and sedative use, thereby decreasing the incidence of delirium. Through this study, we aimed to provide new evidence for developing more personalized visitation policies and alleviating the burden of POD, particularly for older orthopedic patients.
Methods
Study design and setting
This study was a single-center, parallel-group, randomized controlled trial conducted in the orthopedic ICU of Beijing Jishuitan Hospital Guizhou Hospital. The trial protocol was approved by the institutional ethics committee of Guizhou Hospital of Beijing Jishuitan Hospital (21 July 2023, Approval Number: KY20230721-16) and was registered with the Chinese Clinical Trial Registry (ChiCTR2600117290). The study was conducted in accordance with the 1975 Declaration of Helsinki, as revised in 2024. Eligible patients were screened within 24 h after ICU admission following orthopedic surgery. Written informed consent was obtained from all participants or their legal representatives before enrollment. This study report complies with the Consolidated Standards of Reporting Trials (CONSORT) statement, and no patients or members of the public were directly involved in the design, conduct, or reporting of this study. 14
Participants
Patients were eligible for inclusion if they met all of the following criteria: (a) age ≥60 years; (b) admission to the orthopedic ICU within 24 h following orthopedic surgery; (c) no evidence of delirium both before surgery and at ICU admission, as indicated by negative Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) assessments at both time points; (d) preserved ability to communicate sufficiently for delirium assessment at ICU admission; (e) an expected ICU stay of at least 24 h; and (f) availability of at least one fixed family member or primary caregiver willing to participate in bedside visitation according to the study protocol. To improve the transparency of the eligibility assessment, communication ability at ICU admission was operationally defined as the patient being awake enough to cooperate with bedside questioning and complete delirium screening by the study nurses. Patients with negative preoperative and ICU admission CAM-ICU results were considered eligible with respect to baseline delirium status.
Exclusion criteria were as follows: (a) documented moderate-to-severe dementia, severe cognitive impairment, or severe psychiatric disorders requiring long-term psychotropic treatment; (b) severe hearing or visual impairment, aphasia, or other communication barriers that precluded reliable delirium assessment; (c) acute central nervous system disorders, such as traumatic brain injury, acute stroke, or status epilepticus, that could interfere with delirium evaluation; (d) anticipated continuous deep sedation or neuromuscular blockade for ≥24 h after surgery or delirium already present at ICU admission; (e) mandatory isolation due to highly transmissible infection or multidrug-resistant organisms that precluded family visitation; (f) expected survival of <24 h or a treatment plan focused on comfort care; and (g) any other condition considered by the investigators to make study participation inappropriate.
For pre-specified subgroup analyses, surgical procedures were classified into three categories: cervical spine surgery, hip fracture surgery, and other orthopedic procedures. The category of other orthopedic procedures included pelvic fracture fixation, internal fixation for femoral shaft or tibial plateau fractures, primary or revision shoulder or knee arthroplasty, and upper-extremity fracture surgery.
Randomization and allocation concealment
Patients were randomized within 24 h of ICU admission after confirmation of eligibility and acquisition of written informed consent. Participants were assigned to either the flexible visitation group or the restricted visitation group in a 1:1 ratio. The random allocation sequence was generated using Research Randomizer and implemented through sequentially numbered, opaque, sealed envelopes. The envelopes were prepared and kept by an investigator who was not involved in patient recruitment, clinical management, or outcome assessment. Allocation was disclosed only after enrollment had been completed.
Visitation protocol and peri-ICU management
Before initiation of the study, the routine ICU visitation policy was one visit per day from 16:00 to 17:00, with no visits allowed at other times and no overnight bedside stay permitted. The restricted visitation group followed the same routine ICU visitation policy. After randomization, patients were managed in two physically separated ICU areas, one for flexible visitation and one for restricted visitation, with the areas separated by screens and located approximately 5 m apart. Patients who were not enrolled in the trial were admitted to single rooms outside the study areas. Apart from the visitation policy, all participants received the same standard postoperative ICU care according to institutional protocols. Analgesia was guided by the visual analog scale (VAS), and analgesics were titrated to maintain a pain score <4 in both groups. Monitoring, respiratory support, hemodynamic management, and routine non-pharmacological delirium prevention measures were otherwise identical between groups.
In the flexible visitation group, up to two family members were allowed to visit each day without a predefined limit on the total duration of visitation, and family members could alternate during the day. Visits could be initiated at the patient’s request or on the recommendation of the clinical staff. For patients who required invasive mechanical ventilation, bedside visitation was permitted after extubation in accordance with local infection control policy. In the restricted visitation group, family members were allowed to visit only once daily from 16:00 to 17:00, and visits at other times or overnight bedside presence were not permitted.
Outcome assessment
The primary outcome was the occurrence of delirium during the ICU stay. Delirium was assessed once daily using both the CAM-ICU and the Intensive Care Delirium Screening Checklist (ICDSC). Delirium was defined as at least one positive CAM-ICU assessment and/or an ICDSC score ≥4 during ICU admission. Assessments continued until ICU discharge, transfer out of the ICU, or in-hospital death.
Secondary outcomes included hospital-acquired infection, ICU length of stay, total hospital length of stay, total hospitalization cost, ICU-related cost, and sedative use during periods without invasive mechanical ventilation. Sedatives of interest included dexmedetomidine, estazolam, amobarbital, and midazolam. Hospital-acquired infections were defined as new infections occurring 48 h or more following admission and diagnosed according to institutional criteria. Safety evaluation in this study focused primarily on hospital-acquired infections because of their potential relevance to the visitation policy. No separate structured surveillance system or dedicated assessment scale was used to actively capture all intervention-related adverse events. Therefore, beyond the pre-specified infection outcome, the study did not include a systematic evaluation of other potential adverse events related to the visitation strategy, and any such events would only have been identifiable if documented during routine clinical care. Clinical and resource-use data were collected prospectively from bedside records and the electronic medical record until hospital discharge or death.
Statistical analysis
Sample size estimation was performed a priori using Power Analysis and Sample Size (PASS) software. The required sample size was calculated based on the expected difference in POD incidence between the two groups. Assuming incidences of 45% in the restricted visitation group and 30% in the flexible visitation group, with a two-sided α of 0.05 and 80% power, at least 170 patients were required in each group. To account for an anticipated dropout rate of 15%, the planned total sample size was increased to 400 patients.
Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) version 25.0 (IBM Corp.; Armonk, NY, USA). Continuous variables were first evaluated for normality. Normally distributed variables were presented as mean ± SD and compared using the independent-samples t test. Non-normally distributed variables were summarized as median and interquartile range (IQR) and compared using the Mann–Whitney U test. Categorical variables were presented as counts and percentages and compared using the Pearson chi-squared test or Fisher’s exact test, as appropriate. All tests were two-sided, and a P-value <0.05 was considered statistically significant. Pre-specified subgroup analyses were conducted according to surgical category, including cervical spine surgery, hip fracture surgery, and other orthopedic procedures; these analyses were considered exploratory.
After randomization, 10 patients in the flexible visitation group did not complete follow-up because of unplanned discharge or transfer (n = 6) or marked clinical deterioration (n = 4). In the restricted visitation group, five patients were excluded from the final analysis because of incomplete data. Overall, 15 of 420 randomized patients (3.6%) were not included in the final analysis. Missing outcome data were not imputed. Because the missingness was assumed to be completely at random, the primary analysis was conducted using a complete-case approach.
Results
Baseline characteristics of the older orthopedic ICU cohort
A total of 420 patients were randomized, of whom 405 with available outcome data were included in the final analysis, including 200 in the flexible visitation group and 205 in the restricted visitation group. Overall, 15 randomized patients (3.6%) were not included in the final analysis. In the flexible visitation group, 10 of 210 patients (4.8%) did not complete follow-up because of unplanned discharge or transfer (n = 6) or significant clinical deterioration (n = 4). In the restricted visitation group, 5 of 210 patients (2.4%) were excluded from the final analysis because of incomplete data (Figure 1).
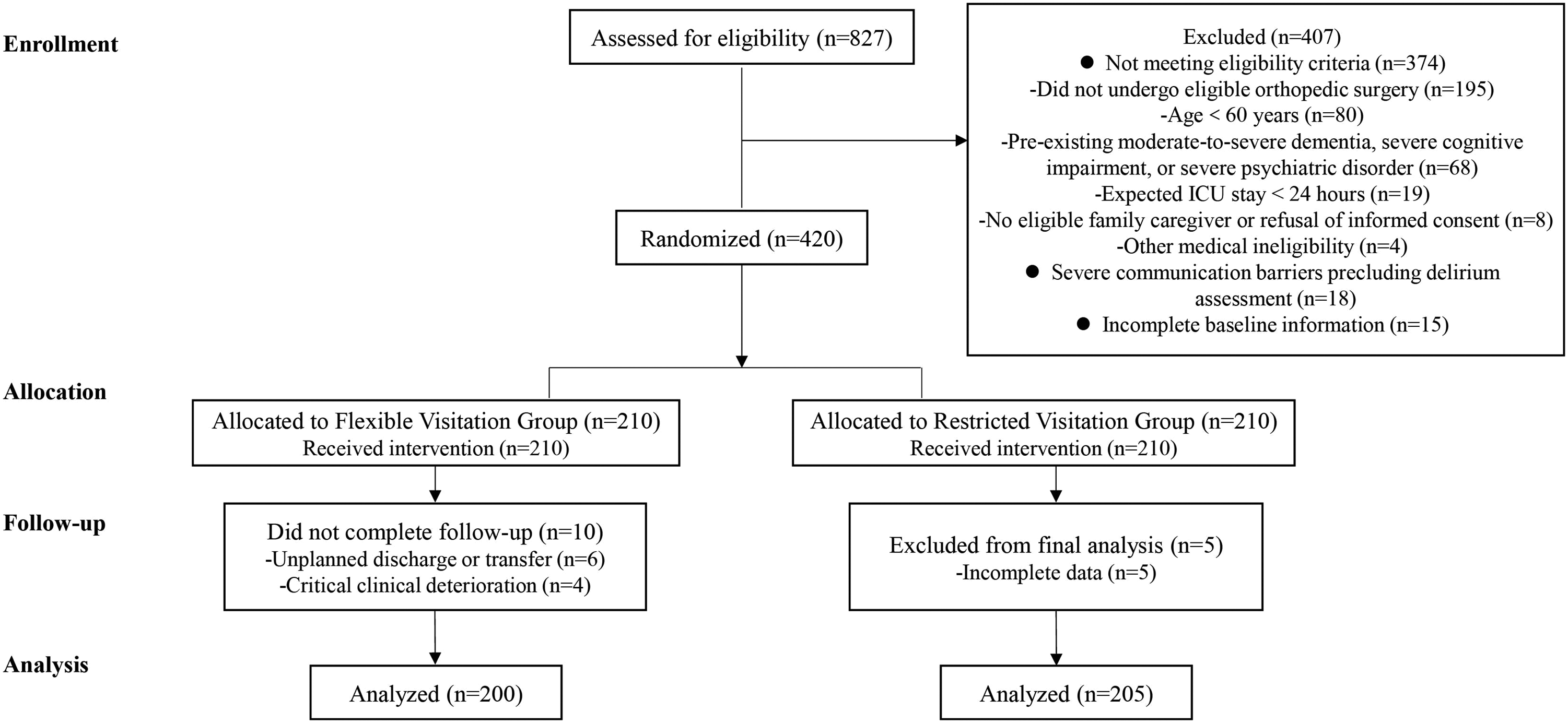
Flow diagram of participant screening, randomization, follow-up, and final complete-case analysis in the trial comparing flexible versus restricted family visitation in the orthopedic ICU. ICU: intensive care unit.
As shown in Table 1, the two groups were broadly comparable at baseline. The median age was 76.5 years (69–84) in the flexible visitation group and 77.0 years (70–84) in the restricted visitation group, and the proportions of male patients were 37.0% and 43.9%, respectively (P > 0.05). Disease severity and pain at ICU admission were similar between groups, with comparable acute physiology and chronic health evaluation (APACHE) II scores and VAS pain scores. The burden of comorbidities reflected a high-risk population but did not differ significantly between groups. The rates of diabetes (17.5% vs 15.1%), pneumonia (37.5% vs 35.1%), and coronary heart disease (23.5% vs 20.0%) were similar, and approximately one-quarter of patients in each group were receiving mechanical ventilation at ICU admission (24.5% vs 20.5%). There was a borderline higher prevalence of hypertension in the flexible visitation group (55.8% vs 40.0%, P = 0.054). With respect to surgical type, hip fracture surgery was the most common procedure, particularly in the restricted visitation group (48.0% vs 58.5%), whereas cervical spine surgery accounted for roughly one-quarter of cases in both groups (26.0% vs 28.8%). Other orthopedic procedures were more frequent in the flexible visitation group (26.0% vs 12.7%). Overall, these findings indicate that the randomized groups were generally well balanced in terms of key demographic and clinical characteristics, providing an appropriate basis for evaluating the effects of flexible visitation on delirium and healthcare costs in this older orthopedic ICU population.
Baseline characteristics of older patients undergoing orthopedic surgery admitted to the ICU.
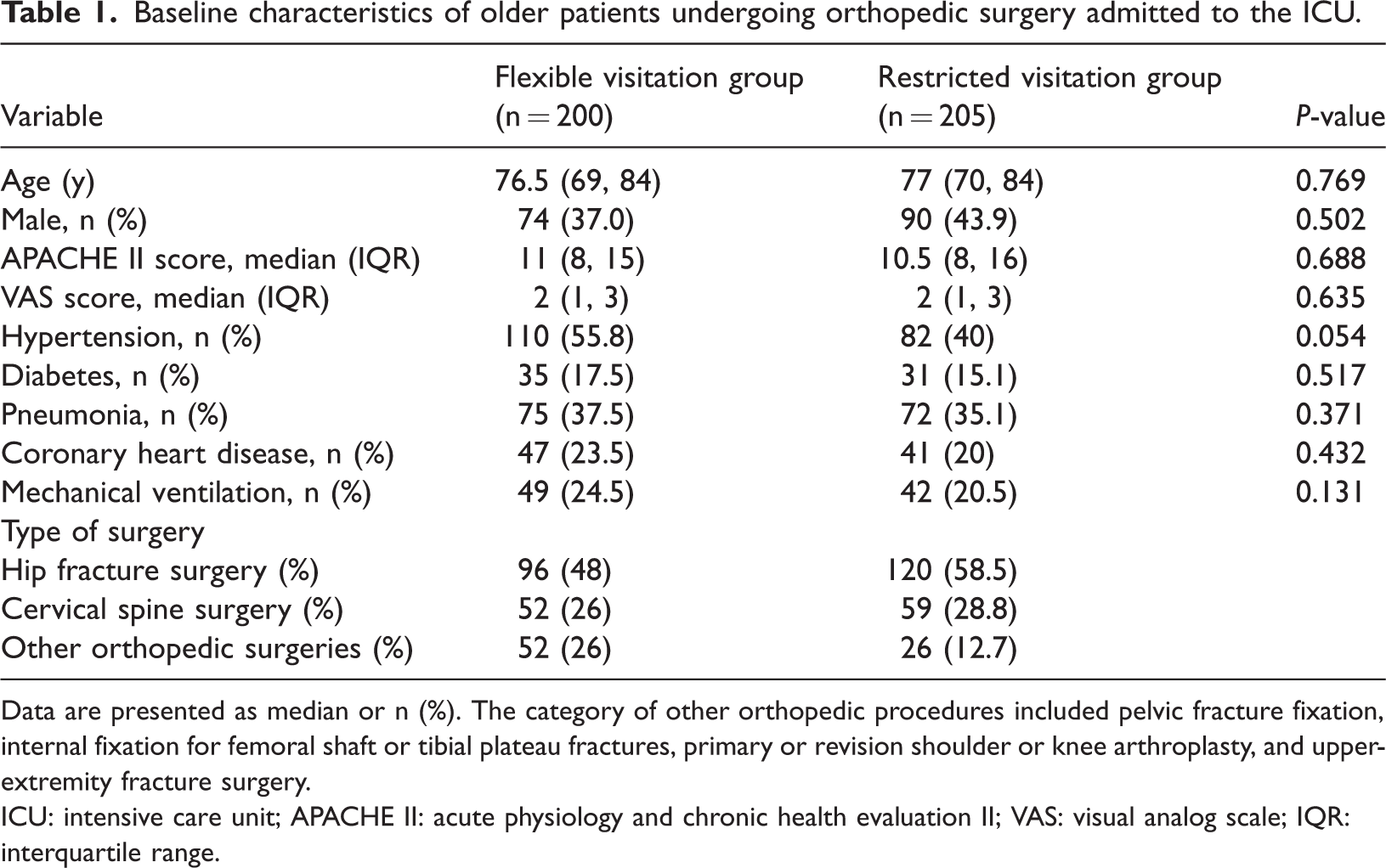
Data are presented as median or n (%). The category of other orthopedic procedures included pelvic fracture fixation, internal fixation for femoral shaft or tibial plateau fractures, primary or revision shoulder or knee arthroplasty, and upper-extremity fracture surgery.
ICU: intensive care unit; APACHE II: acute physiology and chronic health evaluation II; VAS: visual analog scale; IQR: interquartile range.
Effect of flexible visitation on delirium and sedative use by surgical type
Implementation of the visitation policy resulted in a clear difference in family presence at the bedside (Table 2). Median daily visiting time was 5.0 h in the flexible visitation group compared with 0.9 h in the restricted group (P < 0.001), confirming good separation of the two strategies. In the overall cohort, flexible visitation was associated with a lower delirium burden. Delirium occurred in 59 of 200 patients (29.5%) in the flexible visitation group and in 91 of 205 patients (44.4%) in the restricted group (P = 0.002). Consistently, the median ICDSC score was lower in the flexible group than in the restricted group (P = 0.011). The proportion of patients with at least one positive CAM-ICU assessment was numerically lower with flexible visitation (32.0% vs 36.1%), although this difference did not reach statistical significance (P = 0.081).
Outcomes and subgroup analysis by surgery type.
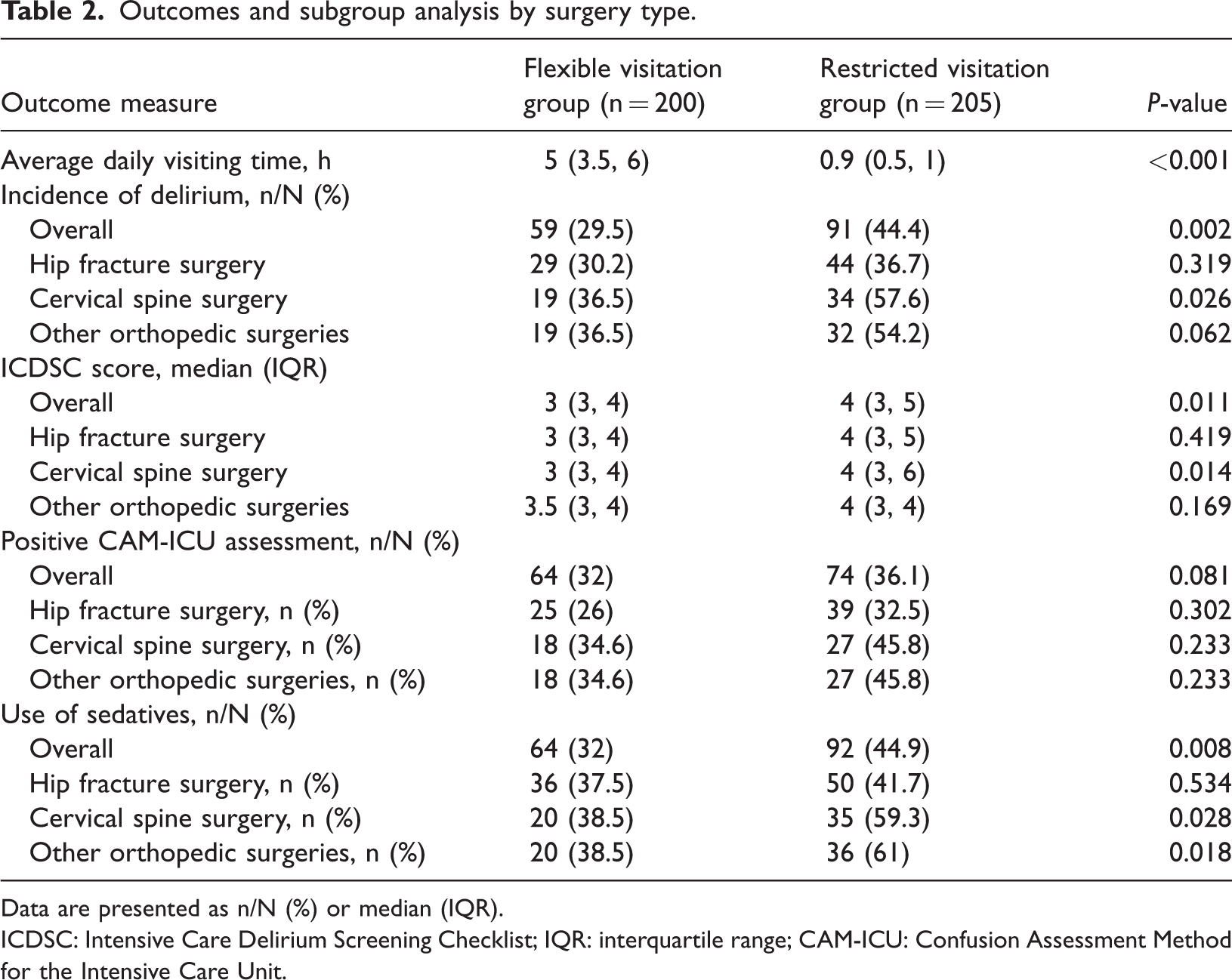
Data are presented as n/N (%) or median (IQR).
ICDSC: Intensive Care Delirium Screening Checklist; IQR: interquartile range; CAM-ICU: Confusion Assessment Method for the Intensive Care Unit.
Subgroup analyses by surgical type suggested heterogeneous treatment effects. Among patients undergoing cervical spine surgery, flexible visitation significantly reduced delirium incidence (36.5% vs 57.6%, P = 0.026) and ICDSC scores (P = 0.014), and fewer patients had a positive CAM-ICU assessment (34.6% vs 54.2%, P = 0.023). In contrast, among patients with hip fracture, delirium incidence (30.2% vs 36.7%, P = 0.319), ICDSC scores (P = 0.419), and CAM-ICU positivity (26.0% vs 32.5%, P = 0.282) did not differ significantly between visitation strategies. For other orthopedic procedures, delirium incidence (36.5% vs 54.2%, P = 0.062) and delirium scores showed a favorable but non-significant trend with flexible visitation.
Sedative exposure during periods without invasive mechanical ventilation followed a similar pattern. Overall, 64 patients (32.0%) in the flexible visitation group and 92 patients (44.9%) in the restricted group received sedatives (P = 0.008). In the cervical spine surgery subgroup, sedative use was significantly lower with flexible visitation (38.5% vs 59.3%, P = 0.028), and in other orthopedic surgeries, it was also reduced (38.5% vs 61.0%, P = 0.018). No significant difference in sedative use was observed among patients with hip fracture (37.5% vs 41.7%, P = 0.534). These findings indicate that the flexible visitation strategy reduced delirium and sedative use overall, with the most pronounced benefit observed in older patients after cervical spine surgery.
Flexible visitation reduces healthcare costs without increasing infections or length of stay
As shown in Table 3, the flexible visitation strategy was not associated with an increased risk of hospital-acquired infection. Infection rates were low and comparable between the flexible and restricted visitation groups (3.5% vs 3.9%, P = 0.916), indicating that greater family presence at the bedside did not compromise patient safety. In contrast, flexible visitation was associated with substantially lower healthcare costs. Overall total hospitalization cost was reduced from 6.4 × 104 Chinese Yuan (CNY) (IQR, 4.9 × 104–8.1 × 104) in the restricted visitation group to 4.8 × 104 CNY (IQR, 3.8 × 104–6.6 × 104) in the flexible visitation group (P < 0.001). When stratified by surgical type, this cost advantage remained evident for both major target populations: hip fracture patients (4.5 × 104 vs 5.9 × 104 CNY, P < 0.001) and cervical spine surgery patients (4.5 × 104 vs 6.5 ×104 CNY, P < 0.001). Among patients undergoing other orthopedic procedures, total costs were numerically lower with flexible visitation; however, the difference was not statistically significant. ICU-specific costs showed a similar pattern: median ICU cost was 0.2 × 104 CNY in the flexible group versus 0.3 × 104 CNY in the restricted group (P = 0.022), driven mainly by a significant reduction among patients with hip fracture, whereas ICU costs did not differ significantly in the cervical spine or other orthopedic subgroups. Lengths of stay were comparable between the two visitation strategies. Median total hospital stay was 16 days in both groups (P = 0.367), and median ICU stay was 1 day in each group (P = 0.892), with no significant differences across any surgical subgroup. Therefore, in this older orthopedic ICU population, flexible visitation reduced both total and ICU-related costs without increasing hospital-acquired infections or prolonging ICU or hospital stay.
Healthcare resource utilization and hospital-acquired infections.
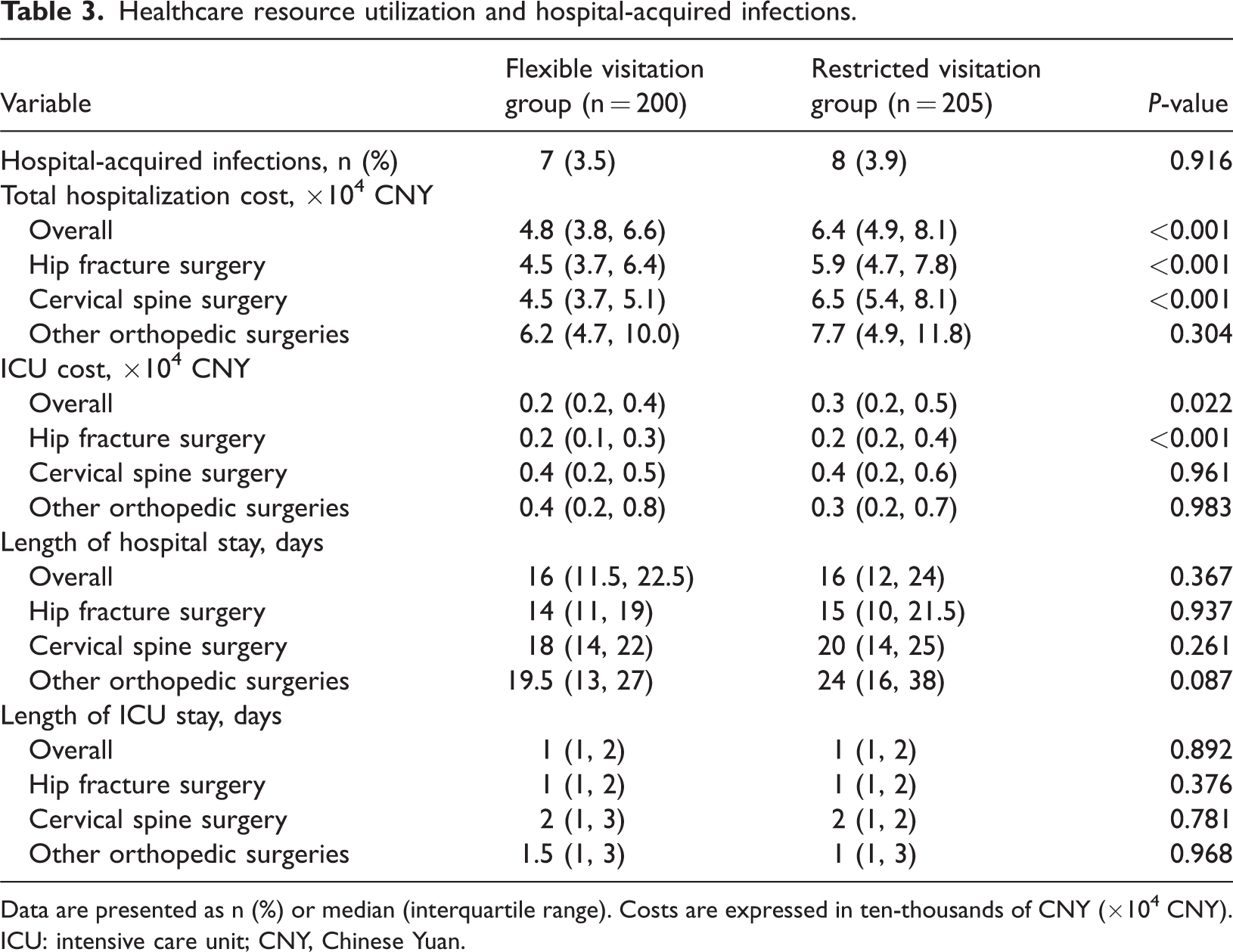
Data are presented as n (%) or median (interquartile range). Costs are expressed in ten-thousands of CNY (×104 CNY).
ICU: intensive care unit; CNY, Chinese Yuan.
Discussion
This randomized trial in an orthopedic ICU shows that a flexible family visitation strategy can meaningfully improve outcomes in older postoperative patients. Compared with a restricted 1-h daily visit, extending and liberalizing visiting time increased actual family presence at the bedside from a median of 0.9 to 5.0 h per day and was associated with a reduction in delirium incidence from 44.4% to 29.5%, lower ICDSC scores, and less exposure to sedative medications. At the same time, flexible visitation did not increase hospital-acquired infections or prolong ICU or hospital length of stay, and it significantly reduced both total hospitalization costs and ICU-related costs. These effects were not homogeneous across the population: patients undergoing cervical spine surgery derived the clearest benefit in terms of delirium prevention and sedation reduction, whereas patients with hip fracture did not show a statistically significant decrease in delirium despite substantial family presence. The clinical relevance of these findings is underscored by the established consequences of delirium in critically ill and surgical patients. Delirium has been associated with increased short-term mortality, longer ICU and hospital stays, higher healthcare costs, and long-term cognitive and functional impairment.1,15,16 In large cohorts of older adults undergoing major noncardiac surgery, postoperative delirium has been associated with markedly higher odds of death, major complications, and nonhome discharge. 17 Given these adverse sequelae, international guidelines and quality-improvement initiatives, including the ABCDEF “ICU Liberation” bundle—which stands for A: Assess, Prevent, and Manage Pain; B: Both Spontaneous Awakening Trials and Spontaneous Breathing Trials; C: Choice of Analgesia and Sedation; D: Delirium: Assess, Prevent, and Manage; E: Early Mobility and Exercise; F: Family Engagement and Empowerment—emphasize systematic delirium assessment and prevention, with family engagement as a core component.18,19 Our results support this paradigm by demonstrating that operationalizing the “F” element, family engagement, through a concrete flexible visitation policy can reduce delirium burden in a well-defined high-risk population.
Although family presence may reduce fear, loneliness, and disorientation, prolonged or poorly timed visits may also increase sensory load in vulnerable ICU patients. Environmental factors such as noise, light exposure, sleep fragmentation, and circadian disruption are biologically plausible contributors to ICU delirium.20,21 As this study emphasizes, the flexible visitation policy applies only to daytime visits and not to nighttime visits. This daytime-focused arrangement may have reduced the likelihood that family presence would interfere with nocturnal sleep opportunity or further disrupt the day–night rhythm and still allow patients to benefit from reorientation and emotional reassurance during waking hours. Such an approach is broadly consistent with ICU sleep-promotion principles, which emphasize minimizing nighttime interruptions and preserving a more physiologic sleep–wake pattern whenever possible.22,23
Evidence regarding ICU visiting policies and delirium has been mixed. The large multicenter ICU Visits trial found that a flexible 12-h visitation policy, combined with structured family education, did not significantly reduce delirium incidence compared with a more restrictive policy in a heterogeneous ICU population. 11 Conversely, a recent meta-analysis suggested that unrestricted visiting may lower delirium risk without increasing infections or mortality, although included studies were relatively small and heterogeneous. 24 More recent observational and quasi-experimental work, including a Chinese multicenter study, reported that flexible visitation could reduce delirium and improve aspects of nursing quality.8,12 Our trial helps reconcile these discrepancies by focusing on a particularly vulnerable subset, older orthopedic ICU patients, and by exploring treatment heterogeneity by surgical type. It is plausible that in unselected ICU cohorts with lower baseline delirium risk or very diverse pathologies, the effect of visiting policies is diluted, whereas in high-risk surgical populations environmental and psychosocial interventions may have greater leverage. Delirium in this study was assessed with two validated ICU-specific tools, the ICDSC and the CAM-ICU. The ICDSC is an 8-item checklist based on the Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria, scored from 0 to 8, with scores ≥4 indicating delirium and higher scores reflecting greater severity; it has demonstrated good validity and reliability in multiple ICU settings.10,25,26 The CAM-ICU is a widely used algorithmic tool that yields a binary diagnosis of delirium based on acute onset or fluctuation, inattention, altered consciousness, and disorganized thinking. 27 In our trial, ICDSC scores were significantly lower in the flexible visitation group, whereas the difference in CAM-ICU positivity showed only a non-significant trend. This pattern is consistent with prior work indicating that the ICDSC may be more sensitive to gradations in delirium burden over time, whereas CAM-ICU can be influenced by the timing of assessment and fluctuating symptoms.26,27 Using both tools strengthens the inference that the intervention reduced not only the probability but also the intensity of delirium.
The heterogeneity of treatment effect by surgical type is one of the most informative findings of this trial. Patients undergoing cervical spine surgery appeared to derive the greatest benefit, whereas no statistically significant reduction in delirium was observed among patients with hip fracture. This discrepancy is clinically plausible. Patients undergoing cervical spine surgery may be particularly vulnerable to anxiety, immobilization, communication frustration, and sensory deprivation related to collars, positioning, and concern about neurological status; these factors may be more directly amenable to reassurance, reorientation, and calming family interaction.4,28 By contrast, patients with hip fracture represent a major delirium-prone population in whom POD has been reported in approximately one-quarter to one-half of older cohorts. Their risk is often driven by advanced age, frailty, cognitive vulnerability, multimorbidity, anemia, delayed surgery, and other physiological stressors that may be less modifiable by visitation alone.5,6,29 Accordingly, the lack of a statistically significant reduction in delirium among patients with hip fracture in our study should not be interpreted as evidence that family involvement is unhelpful in this group; rather, it may indicate that visitation alone is insufficient and should be integrated with broader multicomponent prevention strategies. In addition, although baseline characteristics were broadly comparable at the overall cohort level, our study was not designed or powered to balance every surgery-specific factor across subgroups. Variables such as operation duration, anesthetic technique, transfusion exposure, and perioperative physiological instability were not analyzed in detail and may have influenced delirium risk differently across surgical categories. Prior literature suggests that some of these factors may be relevant in older patients undergoing hip fracture surgery.6,30–32 It is therefore possible that the absence of a significant delirium reduction in the hip fracture subgroup partly reflects a higher burden of unmeasured biological and perioperative risk that attenuated the apparent effect of visitation. Future studies should incorporate more granular intraoperative and perioperative variables to better distinguish true treatment heterogeneity from residual confounding.
An additional important finding is that flexible visitation was associated with significant reductions in total hospitalization and ICU costs, without prolonging ICU or hospital stay. Prior work has shown that delirium independently increases hospital costs and resource use in critically ill patients. 16 In our study, cost savings were most evident in hip fracture and cervical spine subgroups, even though only the latter showed a clear reduction in delirium. The mechanisms behind these economic benefits were not directly measured but may include lower sedative and diagnostic utilization, more efficient discharge planning driven by engaged families, and fewer complications related to uncontrolled agitation or restraints. These results align with the broader concept of the ABCDEF bundle as a high-value care framework that improves outcomes without increasing resource consumption.18,19 For hospital administrators facing rising volumes of older orthopedic patients, a low-cost organizational change such as flexible visitation may be an attractive adjunct to conventional medical and surgical optimization. Additionally, the safety profile observed in this trial is also reassuring. Hospital-acquired infection rates were low and virtually identical between groups, and neither ICU nor hospital length of stay differed significantly. Concerns that increased foot traffic could raise nosocomial infection risk or disrupt workflows have historically driven restrictive visiting policies; however, contemporary studies and meta-analyses, including our study, have generally not demonstrated higher infection rates under more liberal policies when standard infection control procedures are respected.33,34
This study has several strengths, including randomized allocation with concealed sequence, clear separation of visitation exposure, focus on a well-defined high-risk older orthopedic ICU population, use of two validated delirium screening tools, and inclusion of both clinical and economic endpoints. Nonetheless, several limitations should be acknowledged. First, the trial was conducted in a single specialized orthopedic ICU, which may limit the generalizability of the findings to other clinical settings and healthcare contexts. Second, although patients were individually randomized, intervention and control beds were located in physically separated areas, which may have introduced unmeasured environmental or team-level influences. Third, surgical type distribution differed somewhat between groups, and subgroup analyses were exploratory and not powered for definitive comparisons; therefore, the observed heterogeneity of treatment effects should be interpreted cautiously and requires confirmation in larger multicenter studies. Fourth, blinding of clinicians and family members to group allocation was not feasible, which may have introduced performance bias by influencing sedation practices, family behavior, or other aspects of care. In addition, although delirium assessments were performed using standardized instruments by trained nurses, detection bias cannot be completely excluded because outcome assessors may still have been aware of patients’ visitation status. Finally, delirium was assessed only once daily. Given the fluctuating nature of delirium, this assessment frequency may have missed transient episodes and led to underestimation of the true incidence.30,35 In addition, long-term cognitive outcomes were not collected, and thus the effects of flexible visitation on delirium duration, recovery trajectory, and post-ICU cognition remain uncertain.
Conclusion
This randomized trial demonstrated that flexible family visitation was associated with a lower delirium burden, reduced sedative exposure, and lower healthcare costs in older orthopedic ICU patients, without increasing hospital-acquired infections or prolonging hospitalization. The apparent benefit was most pronounced among patients undergoing cervical spine surgery, whereas the effect on delirium in patients with hip fracture was less evident. These findings support the incorporation of flexible, family-centered visitation into individualized delirium prevention strategies for selected high-risk postoperative patients and provide a rationale for future multicenter studies to refine patient selection and evaluate longer-term outcomes.
Footnotes
Acknowledgments
DeepSeek was used for partial language polishing during manuscript preparation; all authors reviewed and approved the final content.
Author contributions
Conceptualization and study design: Zhenyang Ke and Wanwei Jiang; data collection and curation: Tianhui He and Ping Luo; formal analysis and interpretation: Zhenyang Ke and Tianhui He; manuscript drafting: Zhenyang Ke and Ping Luo; critical revision of the manuscript: Zhenyang Ke and Wanwei Jiang; supervision and project administration: Wanwei Jiang. All authors read and approved the final manuscript.
Data availability
All data during the study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Funding
This work was supported by the Advantageous Discipline Construction Project of Guizhou Provincial Health Commission (2025), Wu Jieping Medical Foundation (320.6750.2024-05-8), and Beijing Jishuitan Hospital Guizhou Hospital Youth Innovation Fund (YQNCX (2023)18).