
Abstract
Spinal intradural hemorrhage/hematoma is an uncommon but clinically significant complication of lumbar puncture. We report a previously healthy man in his mid-30s who developed severe low-back pain with bilateral radiculopathy and dysesthesia later the same day followi lumbar puncture performed for headache and fever. He represented 5 days later; coagulation test results were normal. Contrast-enhanced lumbar magnetic resonance imaging demonstrated a ventral mass-like intrathecal lesion extending from L4 to S1 with minimal enhancement, compatible with an early subacute intradural hematoma. He improved with conservative management and close observation without neurologic deficits. To contextualize this case, we performed a targeted PubMed/MEDLINE search through November 2025 and a narrative review of postlumbar puncture spinal intradural hemorrhage/hematoma reports published over the past 10 years. Thirty publications describing 37 patients with spinal intradural hemorrhage/hematoma were identified: symptom onset occurred within 24 h in 54.0% and beyond 48 h in 13.5%; thoracic/thoracolumbar involvement slightly exceeded lumbar/lumbosacral involvement (54.1% vs. 45.9%); and the subarachnoid (45.9%) and subdural (37.8%) compartments predominated. Spinal intradural hemorrhage/hematoma may occur despite normal coagulation findings and can mimic an intradural mass on early magnetic resonance imaging; prompt spinal magnetic resonance imaging and early specialist input are warranted when severe or progressive postlumbar puncture symptoms develop.
Keywords
Introduction
Lumbar puncture (LP) is a widely used diagnostic and therapeutic procedure in neurologic practice. Although generally safe, LP has rarely been associated with serious complications, including spinal intradural hemorrhage/hematoma (SIDH). Earlier literature studies1–3 have emphasized associations with coagulopathy, anticoagulant exposure, or thrombocytopenia; however, accumulating reports4–6 suggest that procedural factors and mechanical trauma may also precipitate SIDH in patients with apparently normal coagulation profiles.
The pathophysiology of iatrogenic SIDH is likely multifactorial, involving vascular injury and cerebrospinal fluid (CSF) dynamics. A “suction effect” related to CSF leakage has been proposed as a mechanism that may facilitate blood entry into the subdural compartment and potentially contribute to hematoma expansion. Despite these mechanistic hypotheses, the optimal initial management—particularly the selection and timing of surgical decompression vs. conservative treatment—remains uncertain, especially in patients without recognized hemostatic risk factors.
Brown et al. 7 reported in a pooled review that pre-existing bleeding diathesis was associated with worse outcomes, whereas the type of intervention was not clearly associated with prognosis in their dataset. More recent case reports, 8 including those from the modern magnetic resonance imaging (MRI) era, suggest that selected haemostatically normal patients may recover well with close observation, thereby challenging the assumption that all symptomatic cases require immediate operative intervention.
Although SIDH after LP is not exceptionally rare within the case report literature, it remains under-recognized in routine practice and is frequently discussed in a fragmented manner. Moreover, clinical decision-making has evolved over the past decade with changes in patient profiles, wider use of contemporary antithrombotic agents, and increasingly early access to MRI. However, a focused update synthesizing the contemporary case-based literature on post-LP SIDH is lacking. Therefore, we present a representative case of post-LP SIDH in a young, previously healthy man who improved with conservative management and provide an updated narrative review of reports published during the last 10 years, aiming to highlight current patterns of presentation, imaging pitfalls, and practical considerations for timely diagnosis and management.
Case report
A man in his mid-30s with no significant past medical history presented to the emergency department of this institution in April 2023 with a 1-month history of headache and 4 days of fever. Physical examination and initial imaging findings were unremarkable. LP was performed by the neurology service to evaluate for central nervous system infection. Opening pressure was 15 cm H2O, and the CSF appeared clear. CSF analysis showed: white blood cells <2/µL, red blood cells 100/µL, protein 42.9 mg/dL, glucose 80 mg/dL (serum glucose 108 mg/dL), and lactate 1.55 mmol/L. Although the presence of red blood cells suggested a minor traumatic tap, the findings were not suggestive of infection, and the patient was discharged. Later the same day, he developed lower back pain with bilateral leg-radiating pain and dysesthesia. Symptoms persisted without improvement. Five days after LP, he returned to the emergency department of this institution. Laboratory evaluation showed no elevation of inflammatory markers (white blood cell count, C-reactive protein, erythrocyte sedimentation rate). Coagulation parameters (platelet count, prothrombin time (PT), and activated partial thromboplastin time (aPTT)) were within normal limits. Contrast-enhanced lumbar MRI demonstrated a ventrally located, mass-like intrathecal lesion extending from L4 to S1. The lesion was hyperintense on T1-weighted imaging and hypointense on T2-weighted imaging, with minimal postcontrast enhancement (Figure 1). These features were most consistent with an early subacute spinal subdural hematoma. He was admitted to the Department of Neurosurgery for observation and treated conservatively, including symptomatic management. No neurologic deficits were observed, including no evidence of cauda equina syndrome or motor weakness. During hospitalization, he reported persistent headache, prompting brain MRI, which showed no intracranial hemorrhage or other acute pathology. Symptoms gradually improved with conservative treatment, including pregabalin 75 mg twice daily, and he was discharged in stable condition after 14 days. A follow-up lumbar MRI was not performed because the patient declined the scan. Although the patient expressed dissatisfaction regarding the postprocedural complications, the symptoms improved following conservative management. At the 1-month follow-up visit, the patient presented with complete resolution of neurological symptoms. Consequently, all pharmacological treatments were discontinued. The institutional review board of Chonnam National University Hospital, South Korea, approved this study (IRB No. CNUH-2023-398) and waived the requirement for informed consent because of the retrospective nature of the study and the use of anonymized data. All treatments were performed with the patient’s informed consent. Written informed consent for publication was waived because no identifiable patient information is presented. This case report was prepared in accordance with the CAse REport (CARE) guidelines.
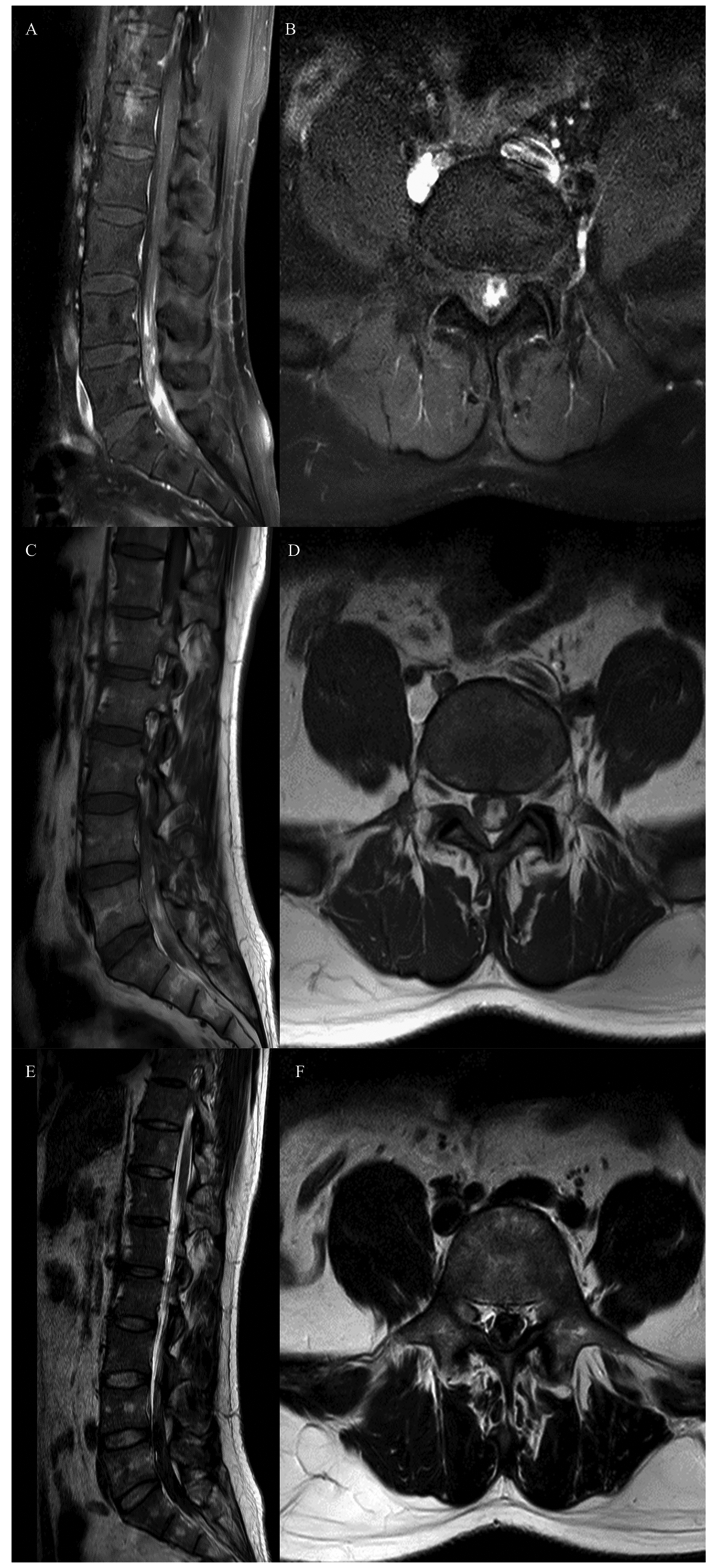
Lumbar spine magnetic resonance imaging obtained 6 days after lumbar puncture. (a, b) T1-weighted images. Sagittal images showed a mixed hyperintense intradural lesion extending from L4 to S1. The axial image at the L5–S1 level demonstrated a predominantly hyperintense lesion, consistent with a combined subacute subdural and subarachnoid hematoma causing severe compromise of the central canal. (c, d) T2-weighted images. Sagittal images showed a hypointense intradural lesion extending from L4 to S1. The axial image at the L5–S1 level demonstrated a predominantly hypointense lesion, consistent with a combined Continued.subacute subdural and subarachnoid hematoma causing severe compromise of the central canal. (e, f) Contrast-enhanced T1-weighted images. A hyperintense lesion was observed at the L4–S1 levels, similar to the noncontrast images; however, no contrast enhancement was identified.
Literature review
To contextualize this case, we performed a targeted literature search and narrative review of published reports describing SIDH after LP. PubMed/MEDLINE was searched through November 2025 using combinations of terms related to LP and spinal intradural bleeding. We included case reports and case series in which an intradural spinal hematoma (subdural, subarachnoid, or mixed) occurred temporally after LP and extracted available data on demographics, anticoagulation/coagulopathy, puncture technique (when reported), symptom onset, imaging characteristics, management, and clinical outcome. Findings are summarized descriptively; given the nature of the case-based literature, no formal meta-analysis or comparative inference was undertaken.
A total of 37 cases of spinal intradural hematoma following LP were identified and included (Tables 1 and 2)1–5,7–31. The cohort included 22 males (59.5%) and 15 females (40.5%), with a mean age of 46.6 ± 22.3 years (range: 5 months to 84 years). The interval from LP to symptom onset varied. Most patients (54.0%, n = 20) developed symptoms within 24 h; 32.4% (n = 12) presented within 12 h. Delayed presentations beyond 48 h occurred in 13.5% (n = 5), with the longest reported latency of 1 week.
Comprehensive review of reported cases of postlumbar puncture spinal intradural hematoma (1974–2025).
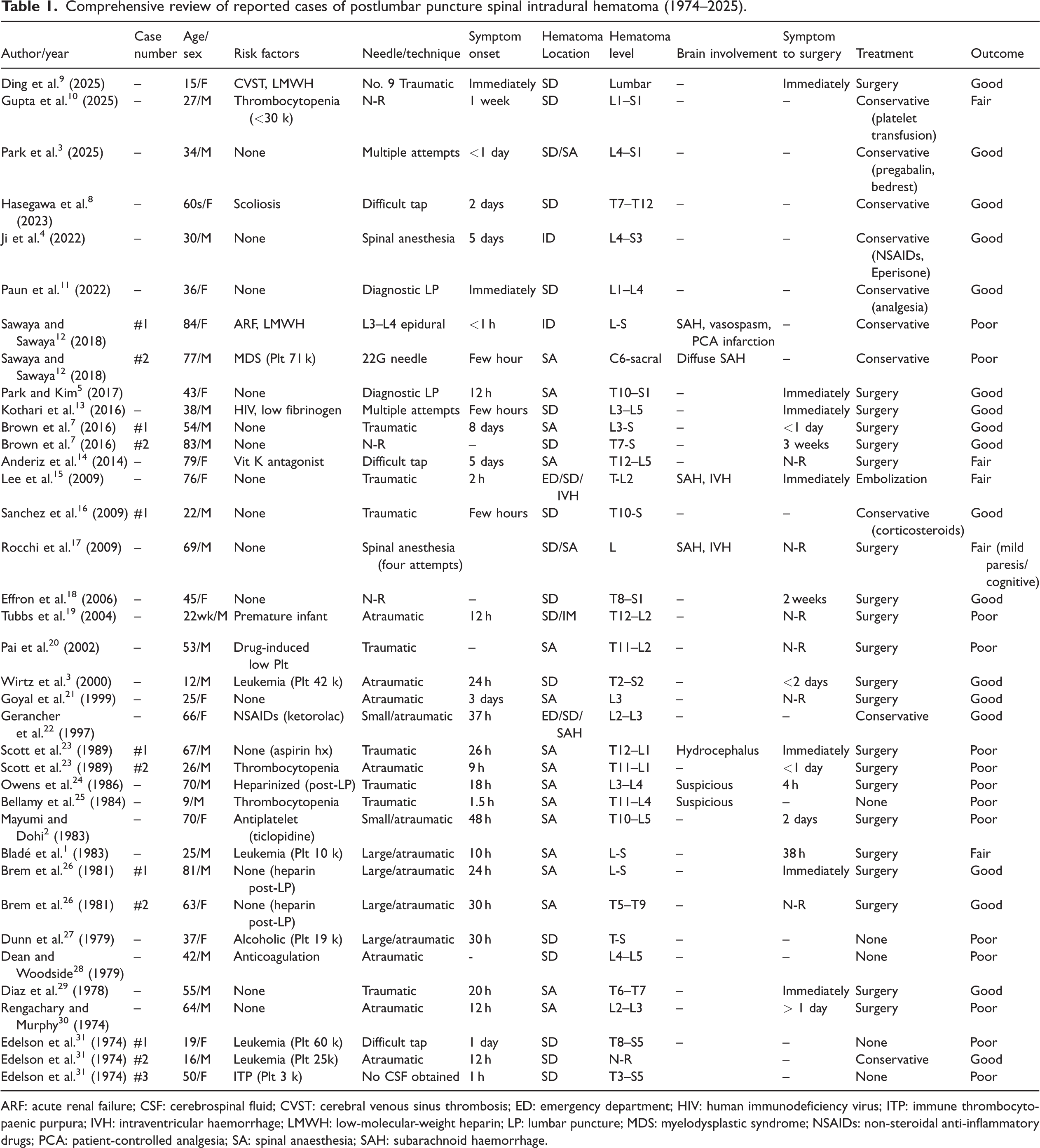
ARF: acute renal failure; CSF: cerebrospinal fluid; CVST: cerebral venous sinus thrombosis; ED: emergency department; HIV: human immunodeficiency virus; ITP: immune thrombocytopaenic purpura; IVH: intraventricular haemorrhage; LMWH: low-molecular-weight heparin; LP: lumbar puncture; MDS: myelodysplastic syndrome; NSAIDs: non-steroidal anti-inflammatory drugs; PCA: patient-controlled analgesia; SA: spinal anaesthesia; SAH: subarachnoid haemorrhage.
Demographics and clinical characteristics of 37 patients with postlumbar puncture spinal hematoma.
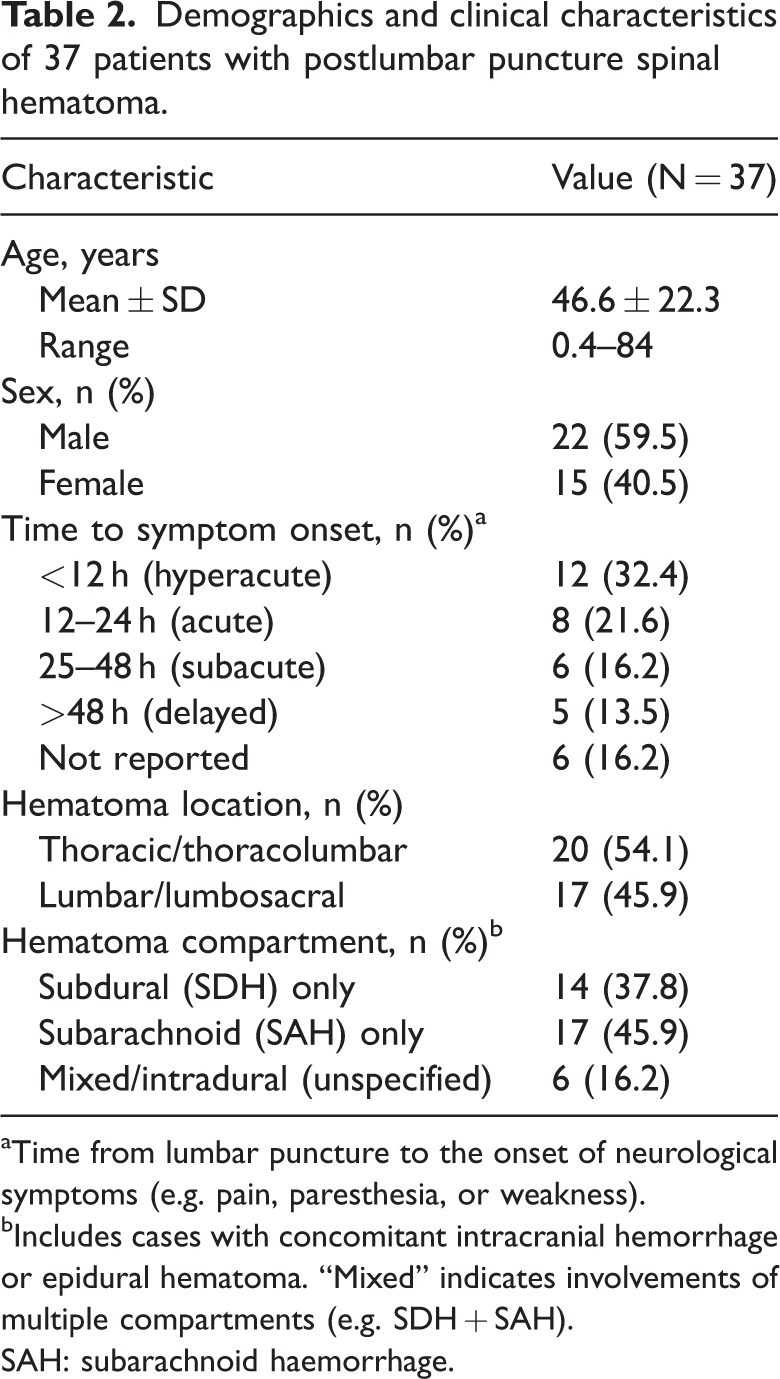
Time from lumbar puncture to the onset of neurological symptoms (e.g. pain, paresthesia, or weakness).
Includes cases with concomitant intracranial hemorrhage or epidural hematoma. “Mixed” indicates involvements of multiple compartments (e.g. SDH + SAH).
SAH: subarachnoid haemorrhage.
By anatomical region, hematomas were reported slightly more often in the thoracic or thoracolumbar spine (54.1%) than in the lumbar or lumbosacral spine (45.9%). Regarding the intradural compartment, pure subarachnoid hematomas were most frequently described (45.9%), followed by subdural hematomas (37.8%); mixed or unspecified intradural hematomas accounted for the remainder.
Outcomes were assessed according to reported coagulation status and management approach. Among patients with coagulopathy and/or anticoagulant exposure (n = 22), poor outcomes were reported in 54.5% (12/22). Within this subgroup, outcomes were numerically more favorable among surgically managed patients (good/fair in 58.3%, 7/12) than among conservatively managed patients (good/fair in 30.0%, 3/10), although these findings should be interpreted cautiously given the small numbers and the likelihood of selection bias. In the conservatively managed coagulopathy/anticoagulation subgroup, poor outcomes (permanent neurological deficits or death) were reported in 70.0% (7/10).
In contrast, patients with normal coagulation profiles (n = 15) showed overall more favorable outcomes, with 86.7% (13/15) achieving good/fair recovery. In this subgroup, favorable outcomes were reported after surgery in 80.0% (8/10). All conservatively managed patients with normal coagulation profiles (n = 5) achieved good outcomes (100%), which may reflect selection bias whereby patients with less severe initial deficits and/or smaller hematomas were preferentially managed without surgery.
Discussion
The principal value of this report lies less in the rarity of post-LP SIDH than in the need for a contemporary, practice-facing synthesis. During the last decade, the clinical context of LP has evolved: patient profiles and antithrombotic exposure have diversified, and early MRI has become more readily available. Yet the evidence remains dispersed across case-based publications, and clinicians are often left without a concise update on present-day patterns of presentation, common diagnostic pitfalls on modern imaging, and practical considerations for timely triage. Against this background, our case provides a representative example of SIDH occurring despite normal routine coagulation parameters, with a favorable course under carefully monitored conservative management.
Mechanistically, iatrogenic SIDH is multifactorial, involving direct vascular injury in conjunction with CSF hydrodynamics. Contemporary reports 9 have described operative findings compatible with a through-and-through puncture mechanism that can injure ventral intrathecal structures, as well as serial imaging findings consistent with dynamic extravasation and rapid morphological change early in the course—features that reinforce the concept that “early MRI is not necessarily static.” The ventral predominance and lumbosacral extent in our patient are compatible with these proposed mechanisms, although causality cannot be established in a conservatively managed case.
Across the collected reports, the latency from puncture to symptoms was variable: although many patients developed symptoms within the first 24 h, delayed presentations beyond 48 h were also described. This variability is clinically important because it creates an “expected discomfort” window in which evolving SIDH may be misattributed to routine postprocedural pain. In our patient, symptoms began on the day of puncture with severe back pain and bilateral radicular symptoms, but he represented 5 days later—illustrating how symptom persistence, rather than immediate severity alone, should lower the threshold for spinal imaging after LP.
Although early recognition and intervention are paramount determinants of prognosis, the radiological presentation of SIDH often mimics spinal neoplasms, abscesses, or arachnoiditis, leading to dangerous diagnostic delays. Recently, Gupta et al. 10 reported a case in which iatrogenic SIDH was misdiagnosed as an intradural extramedullary neoplasm because of MRI findings showing clumping of the cauda equina nerve roots. This misinterpretation led to a 1-week delay in definitive diagnosis, resulting in persistent neurogenic bladder dysfunction. To avoid such diagnostic pitfalls, meticulous analysis of contrast-enhancement patterns is essential. Although hematomas typically do not exhibit enhancement—unlike neoplasms—exceptions exist during the hyperacute phase of ongoing hemorrhage. Kothari et al. 13 documented a case in which initial postcontrast MRI revealed a thin curvilinear focus of enhancement; however, subsequent imaging obtained 7 min later demonstrated a change in morphology and size. They correctly identified this finding not as the static enhancement of a tumor but as active vascular extravasation of a contrast agent. In our case, the diagnosis was supported by characteristic T1 hyperintensity and the lack of contrast enhancement. Clinicians must maintain a high index of suspicion for SIDH in patients with a recent history of LP who present with a spinal mass lesion.
Historically, this complication has been framed predominantly through the lens of bleeding diathesis. In the assembled cases, many reports1–3 involved coagulopathy and/or anticoagulant exposure, yet a meaningful subset occurred in patients with normal coagulation profiles. For contemporary triage, the most defensible take-home message is not comparative prognostication but diagnostic posture: clinicians should not exclude SIDH on the basis of normal PT/aPTT and platelet count when the clinical picture is concerning after LP.
Given the exclusively case-based nature of the evidence, management should be framed as structured clinical reasoning rather than as a prescriptive algorithm. The key determinants are neurological trajectory and compressive physiology: progressive deficit, objective cauda equina features, or substantial radiological compression should prompt urgent neurosurgical evaluation and consideration of decompression; conversely, conservative management may be reasonable in carefully selected patients who are neurologically intact or improving, provided that monitoring is active and escalation thresholds are explicit. In our patient, the absence of motor weakness or cauda equina syndrome, coupled with symptomatic improvement during observation, supported a conservative strategy with close follow-up. From a practical standpoint, the “red flags” that should prompt urgent MRI after LP include severe or escalating back pain out of proportion to expected postprocedural discomfort, new radiculopathy with sensory change, objective weakness, saddle anesthesia, or sphincter disturbance—irrespective of baseline hemostatic status.
Limitations
This work has the intrinsic limitations of a case report coupled with a narrative synthesis. Case-based literature is prone to publication bias, heterogeneous reporting of neurological severity and follow-up, and confounding by indication in management selection, which precludes robust comparative inference. Accordingly, the purpose of the present synthesis is to consolidate contemporary clinical signals—presentation timing, imaging pitfalls, and triage considerations—rather than to assert treatment superiority or definitive prognostic stratification. In summary, our report reframes post-LP SIDH as a condition that is not merely rare but clinically important because it is under-recognized, variably timed, and capable of masquerading as intradural mass pathology on early MRI. Our case, showing a ventral L4–S1 mass-like intrathecal hematoma with minimal enhancement and favorable evolution under observation, illustrates a modern diagnostic and management scenario that clinicians are likely to encounter and may miss without a deliberate, updated index of suspicion.
Conclusion
Post-LP SIDH is not merely a complication in patients receiving anticoagulation; it can occur even when routine coagulation parameters are normal and may present with delayed or evolving symptoms. Our case, demonstrating a ventral intrathecal hematoma spanning L4–S1 with minimal enhancement and favorable evolution under close observation, highlights the importance of avoiding diagnostic anchoring to expected post-LP discomfort. Clinicians should maintain a low threshold for urgent spinal MRI and early specialist consultation when severe or progressive back pain, new radiculopathy, objective neurological deficit, or sphincter disturbance develops after LP, irrespective of hemostatic status. Given the exclusively case-based nature of the available evidence, management should be individualized according to neurologic trajectory and compressive physiology, with active monitoring for selected stable patients and timely decompression considered for patients with progressive deficits or substantial radiological compression.
Footnotes
Acknowledgments
This work was supported by the Gwangju AI Healthcare Ecosystem Establishment Project funded by the Ministry of Science and ICT (MSIT, Korea) Balanced National Development Account (Project Name: Gwangju AI Healthcare Ecosystem Establishment Project/Project Number: H0401-26-1001). The authors used AI tools only to improve the English language and readability of the manuscript. No AI tools were used for study design, data analysis, interpretation, or generation of scientific content.
Author contributions
Wan Park drafted the manuscript. Ji-Ho Jung performed the data analysis. Moon-Soo Han collected the data. Jung-Kil Lee reviewed and critically revised the manuscript. Jong-Hwan Hong supervised the study and served as the corresponding author.
Data availability statement
Data sharing is not applicable to this article because no datasets were generated or analyzed for this case report.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support.