
Abstract
This narrative review examined how artificial intelligence is increasingly being applied in anesthesiology to support clinical decision-making across the perioperative period. It outlines current applications of artificial intelligence in preoperative risk assessment, intraoperative monitoring and automation, and postoperative complication prediction. We also examined the underlying artificial intelligence architectures that form the technical foundations of these tools, including machine learning, deep learning, and natural language processing. We propose that in the future, rather than narrow task-specific tools, artificial intelligence in anesthesiology should involve the development and clinical translation of large, generalizable foundation models capable of integrating multimodal perioperative data. In addition, developments in multimodal data integration, closed-loop control systems, and interpretable modeling may further refine these approaches. Further progress in artificial intelligence–driven anesthesiology may require multidisciplinary collaboration, prospective clinical validation, and careful integration into perioperative workflows to ensure safe and clinically meaningful adoption.
Keywords
Introduction
The perioperative period represents a highly dynamic and complex phase of medical care, requiring precise coordination of preoperative assessment, intraoperative management, and postoperative recovery (Figure 1).1,2 As surgical populations become increasingly heterogeneous and comorbid, anesthesiologists face escalating demands for individualized care, timely decision-making, and enhanced patient safety.3,4 Traditional clinical workflows, although effective, are limited by human cognitive capacity, inter-provider variability, and delays in data interpretation. 5

Applications of AI across the perioperative continuum. This flowchart presents key areas where AI technologies are transforming perioperative anesthetic care, from preoperative risk assessment and planning, through intraoperative monitoring and automation, to postoperative complication prediction and recovery optimization. AI techniques such as ML, deep learning, and NLP support data-driven decision-making at each stage, thereby improving patient safety, operational efficiency, and the personalization of care throughout the surgical pathway. AI: artificial intelligence; ML: machine learning; NLP: natural language processing.
In recent years, artificial intelligence (AI) has emerged as a transformative force across various domains of healthcare, 6 exhibiting the potential to optimize clinical decisions, 7 streamline workflows, 8 and improve outcomes. 9 AI encompasses a broad spectrum of computational techniques, including machine learning (ML), 10 deep learning (DL), 11 natural language processing (NLP), 12 and reinforcement learning, 13 all of which enable machines to learn from data and assist or even automate complex tasks. 14 In anesthesiology, AI is progressively being integrated into perioperative care, ranging from predictive analytics in the preoperative setting to automated drug delivery and real-time monitoring during surgery and early complication detection postoperatively. 15
Despite its growing presence, the clinical application of AI in anesthesia is in its early stages, with several barriers to widespread adoption, including data heterogeneity, model generalizability, regulatory constraints, and ethical concerns.15,16 However, with increasing access to high-resolution perioperative data, advancements in computational power, and the rise of interpretable AI models, the field is poised for significant evolution.
17
This review aimed to achieve the following objectives: (a) summarize current AI applications across the perioperative continuum; (b) critically analyze challenges and limitations; and (c) propose future directions with a focus on foundation models. A recent comprehensive review by Dost et al. addressed AI applications in anesthesiology using a structured thematic approach.
18
The present review differs from and extends their work in several ways:
It places greater emphasis on the emerging paradigm of foundation models and multimodal data integration as a future trajectory. It provides a more detailed discussion of AI applications in postoperative pain management and resource allocation. It systematically analyzes implementation barriers, ethical challenges, and regulatory gaps from a clinical perspective.
Thus, although overlapping in scope, this review offers a distinct analytical lens and forward-looking framework.
Methodology
This narrative review was guided by the Scale for the Assessment of Narrative Review Articles (SANRA). 19 We conducted a structured literature search of PubMed and Scopus to identify studies on the application of AI in anesthesia and perioperative care. The search strategy included the keywords, “artificial intelligence,” “machine learning,” “deep learning,” “anesthesia,” “perioperative,” “prediction,” and “monitoring,” and was limited to English-language publications up to July 2025. The full search strategy is presented in Supplementary Appendix 1.
Inclusion and exclusion criteria. Peer-reviewed original research, review articles, and conference abstracts published in English directly addressing AI applications in anesthesia or perioperative care were included. Animal studies, preclinical research, editorials, letters, non-English publications, and studies without a clearly described AI methodology were excluded.
Screening process. Two authors independently screened titles and abstracts, followed by full-text review. Disagreements were resolved through discussion or consultation with a third author.
Assessment of relevance and methodological quality. Studies were considered relevant if their primary focus was the application of AI for preoperative risk assessment, intraoperative monitoring/automation, or postoperative outcome prediction. With respect to methodological quality, priority was given to studies with external validation, large sample sizes, multicenter design, or prospective methodology. No formal scoring tool was used, consistent with the narrative review design. After duplicate removal, 1124 articles were retrieved. Title and abstract screening yielded 312 articles for full-text review. Following full-text assessment based on the above criteria, 100 studies were finally included. The included studies were synthesized using a thematic approach structured around the perioperative continuum, including preoperative, intraoperative, and postoperative phases. This framework was predefined based on the clinical workflow of anesthesiology. Within each domain, key themes (risk prediction, monitoring, automation, and outcome assessment) were identified and iteratively refined during the review process to provide a structured and clinically relevant synthesis of the literature. A simplified study selection flow diagram is provided in Supplementary Figure 1.
The architecture of AI in medicine
In medicine, AI represents a multilayered framework that turns clinical data into practical information through systematic stages of data acquisition, preprocessing, model development, validation, and clinical integration.6,20 By leveraging ML, DL, and NLP, AI enables automated interpretation of physiological signals, electronic health records (EHRs), and narrative text.10,21 Representative AI techniques and their perioperative applications are summarized in Table 1. These algorithms are increasingly used in anesthesiology to predict perioperative risk, optimize intraoperative management, and enhance postoperative outcomes.23,30–34 The overall workflow and architectural framework of perioperative AI application, from data acquisition to clinical integration, are illustrated in Figure 2. Ensuring interpretability and clinician trust remains central to this process. Overall, this framework highlights that successful clinical translation of AI in anesthesiology depends not only on algorithmic performance but also on data quality, external validation, interpretability, and workflow integration. These interconnected components provide a conceptual structure for evaluating perioperative AI applications discussed in subsequent sections.
Comparison of AI methods and their applications in perioperative anesthesia.

ML: machine learning; MACCE: major adverse cardiac and cerebrovascular event; PONV: postoperative nausea and vomiting; AKI: acute kidney injury; Tx: transplantation; HPI: hypotension prediction index; POD: postoperative delirium; AUROC: area under the receiver operating characteristic curve; AUC: area under the curve; CI: confidence interval
Visual abstract: Schematic overview summarizing artificial intelligence (AI) applications across the perioperative continuum in anesthesiology. AI tools support preoperative risk stratification, intraoperative monitoring and automation, postoperative complication prediction, and institutional resource allocation.
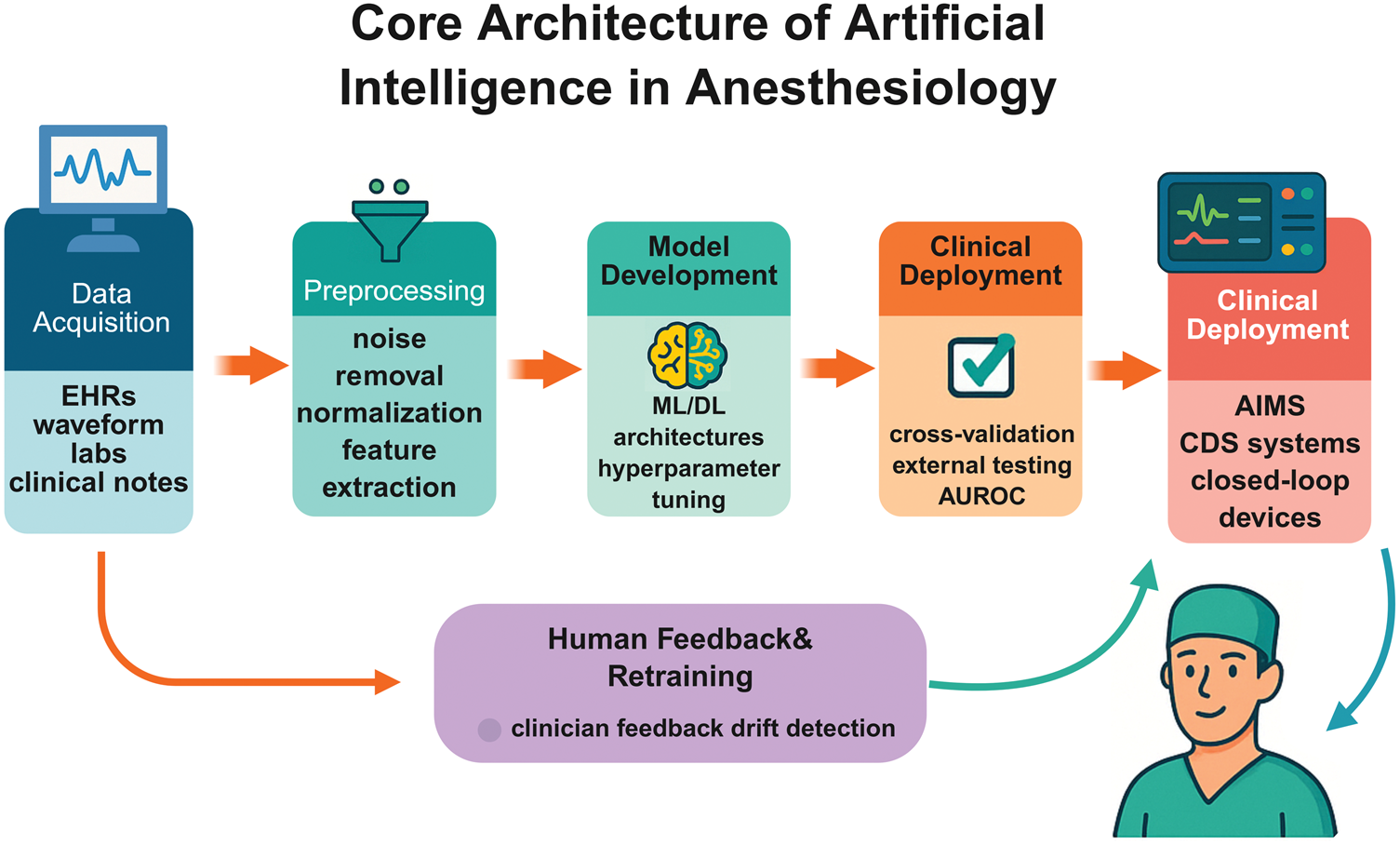
Core architecture of AI in anesthesia. This diagram illustrates the core architecture of AI systems applied in anesthesiology. The workflow begins with multimodal data collection from patient monitoring systems, EHRs, and imaging. The data undergo preprocessing and feature engineering before entering various AI models, including ML, deep learning, and NLP. Model validation and performance evaluation ensure clinical reliability. The final outputs support real-time decision-making, risk prediction, and automated control during anesthesia care, forming a continuous feedback loop that enhances perioperative outcomes.
Data acquisition
Data acquisition is the foundational step for implementing AI in clinical practice. High-quality, time-resolved clinical data form the basis for AI application in anesthesiology. Data sources include structured fields (vital signs, labs), semi-structured records (electronic anesthesia charts), and unstructured data (clinical notes, waveforms, images). For example, Liu et al. have developed and prospectively validated a ML model named Personalized Operative Pain Score (POPS), which used preoperative EHR data of more than 230,000 adult surgical patients to predict maximum postoperative pain scores on the day of surgery and over the subsequent 4 days. The model demonstrated promising predictive performance and was reported to outperform clinician estimates across postoperative days in a prospective multicenter validation cohort. 35 Their study suggests that integrating rich, structured preoperative data supports personalized risk stratification. Such curated datasets that link demographics, laboratory values, and clinical history are essential for developing robust perioperative AI models. 35
Data preprocessing and feature engineering
Raw clinical data must be cleaned and transformed before modeling. Steps include outlier removal, imputation, normalization, and alignment of time-series signals. Feature engineering then extracts informative predictors from raw signals. For instance, advanced hypotension prediction algorithms compute multiple features from the arterial pressure waveform. 36 One such system (the Hypotension Prediction Index (HPI)) evaluates key waveform-derived features to anticipate mean arterial pressure drops. In validation studies, the HPI has demonstrated area under the receiver operating characteristic curves (AUROCs) of approximately 0.93, 0.90, and 0.88 for predicting hypotension 5, 10, and 15 min in advance, respectively. 36 Such physiological signal processing transforms complex biosignals into actionable information for AI-based interpretation.
Model development and training
Supervised learning models are then trained on historical perioperative data to map features to clinical outcomes. 37 Intraoperative vital-sign features and patient covariates serve as inputs, and outcomes such as hypotension or complications act as labels. For example, Michard et al. recently reviewed multiple AI tools developed for hemodynamic assessment in surgical and critically ill patients. These systems, including ML models trained on pulse oximetry waveforms, showed potential for continuous non-invasive blood pressure monitoring and hypotension prediction, although limitations such as calibration requirements and false-positive alerts remained. 38 More generally, large annotated datasets allow training of ensemble or DL models to recognize patterns of risk. Throughout development, best practices such as cross-validation, regularization, and hyperparameter tuning are applied to improve generalizability. These steps help ensure that the model learns robust perioperative patterns (rather than noise) and avoids overfitting.
Model validation and testing
Rigorous validation is essential to ensure model reliability across settings. After initial training, models must be tested on external datasets (different hospitals or patient populations) to confirm generalizability. Performance metrics such as AUROC, sensitivity, specificity, and calibration are evaluated. For instance, Sillesen et al. have developed an NLP model to detect postoperative complications from narrative clinical text. They validated it on data from 18 Danish hospitals (17,486 surgical cases) and found high receiver operating characteristic (ROC) area under the curves (AUCs) (∼0.99) for detecting infections and sepsis. 39 This multicenter analysis suggests that the NLP model maintained performance across institutions and data sources. In general, such studies indicate that perioperative AI models may retain acceptable performance when applied to new hospitals or patient populations. 39
Deployment and clinical integration
Deployment involves embedding AI tools into clinical information systems such as anesthesia information management systems (AIMSs), patient monitors, and real-time decision-support platforms, requiring low latency, interpretability, and reliable model calibration across different patient populations. In addition to these technical requirements, appropriate model calibration and external validation are essential to ensure consistent performance across diverse clinical settings. For example, Rinehart et al. tested a closed-loop vasopressor controller that automatically titrates norepinephrine to keep systolic blood pressure at a target value. In 12 high-risk surgeries, this system infused norepinephrine ∼95% of the time and kept blood pressure within 10% of the target value in 92% of the cases, with hypotension occurring only 1.8% of the time. 40 These results suggest improved intraoperative hemodynamic stability within the study cohort. In practice, such AI modules must also address interoperability with monitors and infusion pumps and meet regulatory requirements. Ultimately, successful deployment is likely to depends on seamless incorporation into the anesthesiologist’s workflow (with clear alerts and controls) and on demonstration of real clinical benefit as above.
AI in preoperative management: precision risk assessment and planning
The preoperative phase plays a vital role in identifying individual risks, optimizing comorbidities, and formulating personalized perioperative care plans. Conventional risk assessment tools such as the American Society of Anesthesiologists Physical Status Classification, Revised Cardiac Risk Index, and Charlson Comorbidity Index provide broad estimations but often lack the precision needed for patient-specific prediction. 41 AI offers a new possibility for integrating heterogeneous clinical data to generate real-time, individualized risk assessments and decision support. 6
Predictive analytics for risk stratification
AI models have shown considerable promise in predicting postoperative complications and perioperative adverse events using preoperative variables for risk stratification. These include postoperative complications such as acute kidney injury (AKI), 42 pneumonia, 43 and delirium, 44 as well as cardiovascular events such as myocardial infarction and intraoperative hypotension.45,46 For example, Yuan et al. have shown that several ML algorithms (random forest, gradient boosting, and support vector machine) achieve AUCs up to 0.983 for 30-day postoperative mortality after major abdominal surgery. 47 These models can incorporate complex structured data (demographics, lab values, vitals) and even imaging or genomic inputs to capture nonlinear risk interactions. In practical examples, Bishara et al. applied XGBoost and neural networks to predict postoperative delirium, achieving an AUC of ≈0.85 (versus ≈0.76 for logistic regression). 27 Likewise, Kiyatkin et al. developed a random forest “RESPIRE” model for postoperative respiratory failure that achieved an AUROC of 0.93, significantly outperforming conventional risk scores (≈0.82). 48 These ML-based tools have consistently outperformed traditional scoring systems by modeling complex interactions among multiple risk factors.
Enhancing preoperative evaluation
AI is streamlining preoperative workflows by automating information capture and patient interaction. NLP can extract pertinent clinical details from free-text EHRs. In one study, Suh et al. applied an NLP engine to pre-anesthesia clinic notes and found that it agreed with anesthesiologist-documented conditions 81.2% of the time, while identifying 16.6% additional relevant conditions that clinicians had missed. 33 Conversational AI (chatbot) systems are also being explored for history-taking. For instance, Lin et al. have reported that perioperative chatbots are generally well received by patients (pooled satisfaction proportion: 73% (95% confidence interval 62%–85%)) and appear to improve knowledge acquisition during the preoperative period. 49 Although this suggests acceptable patient acceptance, comparative benchmarks for satisfaction against traditional preoperative education are limited, and the clinical significance of this finding warrants further prospective evaluation. Integrative decision-support dashboards are also emerging; these platforms combine laboratory values, imaging data, and surgical history to create real-time displays to help anesthesiologists identify high-risk patients and plan tailored interventions. Together, these innovations reduce manual documentation and support a more standardized, efficient approach to preoperative assessment.
Personalized anesthetic planning
AI-driven decision support enables more individualized anesthesia management by integrating patient-specific physiology, pharmacogenomics, and clinical factors. Algorithms can recommend the optimal anesthesia modality and dosing strategy for each patient. As noted by Naaz et al., the integration of genomics with AI allows the creation of customized anesthetic protocols, simplifying dosing decisions and reducing perioperative risk. 50 In practice, DL has been used for intraoperative drug delivery and monitoring. For example, Park et al. have developed a deep neural network to analyze real-time electroencephalography (EEG) signals for anesthesia depth monitoring, achieving more accurate predictions than conventional bispectral index (BIS) monitors. 51 In high-risk cases, AI-generated risk profiles might trigger preoperative optimizations (e.g. anemia correction, 52 glycemic control, 53 and beta-blocker initiation) or suggest adjustments such as enhanced monitoring (intensive care unit (ICU) admission) or enrollment in Enhanced Recovery After Surgery (ERAS) protocols. 54 These personalized recommendations can improve perioperative safety and optimize patient outcomes. 55
Limitations and considerations
Despite its potential, AI in preoperative care faces significant challenges. A key issue is the “black box” nature of many ML models; lack of explainability can undermine clinician trust. As Müller-Stich et al. emphasize, transparency and interpretability are essential for effective integration of AI into clinical practice. 56 Furthermore, most existing models are trained on retrospective, single-center datasets, which raises concerns about generalizability and biases. For instance, Arina et al. have reported that 75% of perioperative ML tools are developed using single-center data, and only 13% included external (multicenter) validation. 41 Lee et al. reported an internal AUROC of 0.868 using their gradient boosting model for postoperative AKI prediction, which decreased to 0.757 after external validation. This performance decline suggests reduced model generalizability across different patient populations and clinical settings. Although the original study did not report a formal statistical comparison, such reductions are commonly observed in externally validated AI models and underscore the importance of multicenter validation and cautious clinical implementation. These findings further highlight the need for prospective multicenter validation and careful clinical implementation to ensure reliable and equitable deployment of AI tools.
AI in intraoperative care: monitoring, decision support, and automation
The intraoperative period involves rapid physiological fluctuations that require precise and timely interventions in a data-intensive environment. Anesthesiologists must continuously interpret complex physiological signals to maintain hemodynamic stability and ensure surgical safety. AI has emerged as a promising concept that may support intraoperative management by improving the precision, consistency, and responsiveness of clinical decision-making. Through continuous integration and analysis of multimodal biosignals, AI systems have the potential to assist real-time decision-making and adaptive control, as illustrated in Figure 3.

AI–augmented intraoperative monitoring and decision support. This diagram illustrates how AI enhances intraoperative care by integrating continuous physiological data using predictive analytics and decision-support systems. AI algorithms enable real-time assessment of sedation depth, nociception, and hemodynamic trends, supporting automated drug delivery, early complication detection, and optimized anesthetic management. Human-in-the-loop models ensure clinician oversight and intervention when necessary, fostering safety and precision during surgery. AI: artificial intelligence.
Intelligent physiological monitoring
Conventional intraoperative monitoring primarily relies on clinicians to interpret multiparametric data streams such as electrocardiography (ECG), arterial blood pressure, pulse oximetry, and capnography, using threshold-based alarms to detect abnormalities. 57 However, these alarms often lack specificity and can contribute to alert fatigue, thereby reducing their clinical usefulness. In contrast, AI-based systems integrate complex, continuous biological signals to identify early warning patterns that may not be apparent to human observers. Recent studies have applied DL to multimodal waveforms, including EEG, blood pressure, photoplethysmography (PPG), and ECG, to characterize a patient’s nociceptive or anesthetic state in real time.58–60 In a recent prospective study, spectral analysis of intraoperative frontal EEG during anesthesia induction identified specific neurophysiological markers such as reduced alpha and beta band power and lower aperiodic offset, which predicted vulnerability to postoperative delirium in older patients, achieving an AUC of 0.73 for the logistic regression model. 61 AI analysis of EEG has also been shown to enhance depth-of-anesthesia monitoring as AI-driven EEG indices can quantify cortical sedation with finer temporal resolution than conventional BIS metrics. 62 These multimodal AI-derived indices may provide greater sensitivity and stability than single-signal alarms, enabling more reliable intraoperative assessment and maintaining awareness of both nociceptive and sedative states. Nevertheless, heterogeneity in monitoring platforms and lack of standardized thresholds currently limit cross-institutional generalizability.
Predictive decision-support systems
Intraoperative AI applications are increasingly incorporating predictive analytics to support anticipatory clinical decision-making. 63 For instance, the HPI, a ML model based on arterial waveform analysis, has demonstrated predictive accuracy comparable with that of traditional mean arterial pressure thresholds for forecasting intraoperative hypotension up to 15 min in advance, with both methods achieving AUROC values of approximately 0.89. 64 Additionally, AI–enhanced decision-support tools contribute to goal-directed therapy by informing fluid responsiveness, guiding vasopressor titration, and optimizing transfusion strategies.65,66 These systems offer valuable assistance to anesthesiologists, particularly during complex surgeries where rapid decision-making is essential. 67
Automation and closed-loop anesthesia systems
AI has also paved the way for automation in anesthetic delivery through closed-loop systems that dynamically adjust drug administration based on continuous physiological feedback. The classic example is closed-loop propofol infusion guided by EEG–derived BIS; trials and meta-analyses have shown that BIS–controlled closed-loop systems significantly reduce propofol consumption and reduce blood pressure fluctuations compared with manual dosing. 68 In practice, closed-loop anesthesia systems have been studied for hypnotics, opioids, and neuromuscular blockers. For instance, an automated norepinephrine infusion controller (vasopressor pump) was tested in intermediate-to-high-risk surgery and maintained systolic arterial pressure within 10% of the target value for >90% of case time. 40 Overall, these AI-guided closed-loop systems may reduce human variability and cognitive load and can improve hemodynamic and anesthetic controls in selected settings. However, most studies remain limited to controlled settings, and broader clinical adoption will require prospective validation and integration with existing anesthetic workflows.
Robotics and AI–enhanced devices
The integration of AI with surgical robotics is rapidly expanding the capabilities of intraoperative support technologies. For instance, AI-assisted ultrasound guidance has been applied to regional anesthesia; convolutional neural networks can detect nerves and vessels in real time, highlighting the correct target anatomy for needle placement. In one study, AI software accurately identified the target nerve in 93.5% of the cases and reduced block failure rates. 69 Furthermore, smart infusion pumps and intelligent ventilators are increasingly incorporating AI algorithms to personalize fluid delivery and ventilatory support based on continuous patient feedback.70,71 When coupled with real-time analytics, these technologies contribute to the development of semi-autonomous systems capable of supporting critical intraoperative functions with enhanced precision.
AI in postoperative recovery: complication prediction and enhanced outcomes
The postoperative period is critical for early recognition of complications, effective symptom management, and initiation of rehabilitation strategies. Despite advances in surgical and anesthetic techniques, a significant proportion of patients experience adverse postoperative events, including delirium, infection, respiratory compromise, pain, and prolonged hospitalization.72,73 AI offers a promising approach to improving postoperative outcomes through early detection, continuous risk monitoring, and personalized recovery planning.
Predictive models for postoperative complications
ML algorithms are increasingly utilized to anticipate a range of postoperative complications. These include conditions such as postoperative delirium, AKI, 74 respiratory depression, 75 sepsis, 76 surgical site infections, and the likelihood of 30-day readmission or mortality. 77 Such models analyze a diverse set of perioperative parameters, encompassing intraoperative hemodynamic data, anesthetic exposure profiles, medication usage, laboratory trends, and patient comorbidities. 78 Notably, ensemble learning techniques have demonstrated high accuracy in forecasting ICU admissions and as early indicators of clinical deterioration, thereby enabling timely clinical responses.79,80 As these models are updated with real-world clinical data, they may support dynamic and adaptive risk assessment rather than relying solely on static prediction frameworks.
AI for postoperative pain and symptom management
AI is also being applied to anticipate and tailor postoperative analgesia. Recent studies have shown that ML-based tools can identify patients likely to experience severe pain and thus guide pain management strategies. In one multicenter study, a neural-network–based score, “POPS,” was developed using preoperative EHR data and prospectively validated: it outperformed anesthesiologists’ predictions of patients’ maximum pain scores on each of the first 4 postoperative days. 35 Thus, the model achieved significantly better discrimination than clinicians on most postoperative days in forecasting pain intensity (on a scale of 0–10). 35 Narrative reviews reinforce this potential; current ML models “demonstrate satisfactory performance to predict pain outcomes and their prognostic trajectories,” identifying risk factors and patient subgroups that might benefit from intensified pain control. 81 These findings suggest that AI helps personalize analgesic plans (for example, identifying patients who might need higher opioid doses or regional blocks) by anticipating postoperative pain levels preoperatively. In the future, such tools may support anesthesiologists in optimizing opioid dosing or non-opioid adjuncts on a per-patient basis, improving recovery and reducing complications associated with over- or under-treatment.
AI in postoperative monitoring and follow-up
Postoperative neurological monitoring may further be supported by AI through the interpretation of intraoperative EEG biomarkers. In a prospective study, Pollak et al. analyzed frontal EEG during propofol-induced loss of consciousness and identified spectral features, including decreased alpha and beta power as well as reduced aperiodic offset, which were associated with an increased risk of postoperative delirium in older patients, with an AUC of 0.73 for the predictive model. 82 Similarly, early warning systems using AI on physiologic data (e.g. vital-sign trends) have been proposed to identify deterioration sooner in the post-anesthesia care unit (PACU) or ward, enabling proactive care.83,84
Resource allocation
AI may contribute to perioperative efficiency by optimizing workflows and resource allocation. In a recent study, ML models were developed to predict PACU discharge readiness using perioperative clinical and Aldrete score data and demonstrated good performance (AUC = 0.85 and accuracy = 0.86), and outperforming the standard Aldrete checklist. 85 This application illustrates the potential of AI to support more objective and data-driven assessment of discharge readiness and perioperative efficiency. Similarly, ML-based scheduling systems have been reported to reduce PACU wait times, improve operating room throughput, and enable more accurate estimation of case durations and recovery needs. 86 By supporting real-time staffing and bed management, AI-driven decision support may help streamline perioperative operations and optimize human and facility resources without compromising patient safety. 86
Limitations, ethical considerations, and challenges associated with AI use in anesthesia
Although AI demonstrates considerable potential to revolutionize perioperative anesthesia care, its clinical implementation remains associated with notable challenges. Issues related to technical robustness, ethical integrity, data privacy, and clinical usability should be addressed to facilitate responsible and equitable integration. 87 A nuanced understanding of these barriers is crucial for guiding future development and regulatory frameworks.
Technical limitations and generalizability
AI systems for anesthesia management often require large, high-quality datasets and rigorous validation for reliable performance across settings. Many models are developed using single-center data and can be subject to overfitting; they may not be applicable in new patient populations or different hospitals. For example, Lee et al. developed a ML model to predict AKI after noncardiac surgery using intraoperative data. They reported excellent performance on the original (internal) dataset (AUROC ≈ 0.868); however, there was a substantial decline in performance when an external open dataset was used (AUROC ≈ 0.757). 88 This gap illustrates how models tuned to one institution’s data may falter elsewhere. Other reviews similarly highlight that insufficient and non-representative training data, complex model architectures, and variability in monitoring equipment or clinical protocols can limit an AI system’s generalizability. 87 Overcoming such technical limits will require multicenter data sharing, robust external validation, and design of adaptable algorithms that can be customized to local environments.
Ethical concerns and bias
Use of AI tools and methods in anesthesia management raises critical ethical issues around fairness, transparency, and accountability. Algorithms may reflect the data they are trained on; therefore, biased or unbalanced datasets can produce unequal performance across patient groups. A recent study examining AI-generated images of anesthesiologists has reported that models predominantly depicted anesthesiologists as individuals of White ethnicity (64%–83% representation) and exhibited sex and age biases, suggesting limited alignment with the actual diversity in the clinical workforce. 89 Such findings underscore the risk that AI tools could underperform or mislead when treating underrepresented populations. Clinicians are also concerned about accountability for AI errors. In a survey of anesthesiologists, although most respondents reported that they believed AI would reduce complications, several of them expressed concerns about “who will be held accountable for inaccuracies” in AI recommendations. 90 These ethical and bias issues, ranging from the potential amplification of healthcare disparities to the lack of transparency in “black box” decision-making, highlight the importance of algorithm auditing, development of representative datasets, and establishment of clear frameworks for clinical accountability.
Data privacy and security
AI implementation in anesthesia management necessitates access to vast amounts of sensitive health data, which raises significant concerns about data privacy and cybersecurity. Even de-identified datasets carry the potential for re-identification, thereby threatening patient confidentiality. For instance, advances in AI have made it easier to re-identify individuals from datasets once thought anonymized; one analysis has noted that de-identification can be “nullified in light of new algorithms,” increasing risk to patient data. 91 In anesthesia management, intraoperative monitors and electronic anesthesia records could be included in such datasets; therefore, stringent safeguards are needed. Experts have emphasized that regulatory frameworks must enforce patient consent and data control and encourage sophisticated data protection methods. 92 Secure data handling (encryption and access controls) and regulatory oversight (such as independent audits or ethics boards) are therefore crucial to prevent the unauthorized use of perioperative data.
Clinical integration and human factors
The successful adoption of AI in anesthesia management depends not only on algorithmic accuracy but also on its ability to integrate seamlessly into clinical workflows without disrupting established practices. Even a well-performing AI tool will only improve care if it fits smoothly into clinical practice. Integration challenges include gaining clinician trust, fitting into workflow, and ensuring interpretability. Studies show that trust in the AI system is a key factor influencing adoption. 93 Anesthesiologists must understand how an AI tool reaches its conclusions and be able to override it if needed. In addition, appropriate calibration of alert thresholds and clear presentation of risk predictions are important to prevent unnecessary alarms and support clinical decision-making. Human factors such as alert fatigue or over-reliance on automation are concerns; one commentary has noted the need for “appropriate level of trust” and safeguards against practitioner de-skilling in automated systems. 94 For example, closed-loop anesthesia delivery systems automate drug infusion but require anesthesiologists to monitor and intervene if conditions change. Effective implementation also requires user-friendly interfaces, training, ongoing performance monitoring to ensure patient safety in real-world settings, and continued involvement of clinicians in decision-making.93,94 However, variability in institutional workflows and clinician acceptance may limit generalizability, underscoring the importance of context-specific implementation strategies.
Regulatory and legal challenges
Regulatory and liability issues are among the biggest hurdles for clinical AI in anesthesia. Currently, only a few AI/ML-based medical devices (mostly in imaging and monitoring) have Food and Drug Administration (FDA) approval, and devices specific to anesthesia are scarce. 95 In other words, anesthesiologists using an FDA-cleared AI tool would still bear malpractice liability for adverse outcomes. These uncertainties create hesitation. Experts call for clear regulations on adaptive AI algorithms (for example, FDA’s planned “Software as a Medical Device Action Plan”) and legal standards that define responsibility between developers and providers. In parallel, medical societies and hospitals will need to develop policies (e.g. guidelines on AI oversight or informed consent) to ensure accountability and safe deployment of AI in anesthetic care. 94
Future directions and innovations in AI-driven anesthesia
AI continues to evolve, its applications in anesthesiology are poised to expand beyond current capabilities. The integration of advanced computational techniques with real-time perioperative data will facilitate a transition from reactive care to proactive, personalized, and autonomous anesthetic management. Several key innovations are expected to define the future of AI in anesthesia. 96 These future directions emphasize not only technological advances but also practical pathways for integrating AI into routine perioperative decision-making.
Real-time multimodal integration and personalized anesthesia
Future AI systems in anesthesiology are increasingly integrating multimodal data, including continuous vital signs, EHRs, imaging, and even genomic information, to tailor anesthesia to each patient. By synthesizing these diverse inputs, AI can perform real-time risk assessment, anticipate complications, and adjust drug dosing according to individual physiology. 96 For example, an EEG-guided propofol infusion protocol was shown to be safe and maintained stable hemodynamics in older cardiac surgery patients. 97 Similarly, a future AI system for predicting postoperative AKI could combine preoperative risk scores with intraoperative real-time data, including hourly urine output, blood pressure variability, and newly available laboratory results, to dynamically update risk estimates and suggest preventive strategies such as fluid adjustment or avoidance of nephrotoxic agents. 74 Such systems may be implemented initially through prospective validation in high-risk surgical populations before broader clinical deployment. 74 Such approaches exemplify the shift toward precision, proactive anesthesia guided by data-driven intelligence.
Autonomous systems and human-in-the-loop collaboration
Next-generation closed-loop anesthesia platforms are exploring semi-autonomous control using reinforcement learning and adaptive algorithms to maintain target blood pressure and sedation levels. These systems act as “intelligent co-pilots,” taking over routine tasks (e.g. infusion adjustments) while allowing the anesthesiologist to override if needed. In controlled trials, automated propofol delivery has matched manual control of target sedation (BIS) while greatly reducing clinician intervention.98,99 For example, a closed-loop propofol total intravenous anesthesia (TIVA) system maintained time-in-target BIS equivalent to manual infusion and required essentially no manual dose adjustments. 98 This model of human-in-the-loop AI ensures safety, enhances performance, and is particularly beneficial in high-complexity surgical settings.
Explainability, ethical design, and collaborative learning
As AI use expands, there is growing emphasis on transparency, ethics, and generalizability. Explainable AI (XAI) tools, such as SHapley Additive exPlanations (SHAP) values and saliency maps, help clarify model predictions. SHAP quantifies the contribution of individual features to model predictions, thereby enhancing transparency and interpretability in AI-driven decision-making. For instance, an interpretable ML model using SHAP has identified key predictors of inadequate postoperative analgesia, 100 illustrating how XAI can support individualized pain management. Meanwhile, federated learning frameworks are emerging to train models across institutions without sharing raw patient data.101,102 By enabling decentralized model training, federated learning preserves privacy while yielding larger, more robust AI models.
Conclusion
AI is beginning to reshape certain aspects of anesthetic care by enhancing decision-making across the perioperative process. ML and DL models show promise for risk prediction, individualized planning, monitoring, and automated drug delivery. However, widespread clinical adoption requires rigorous prospective validation, improved generalizability, and careful attention to ethical and implementation challenges. Rather than replacing clinicians, AI is likely to act as a real-time assistant to improve precision and safety. Future advances will depend on the successful integration of foundation models and multimodal perioperative data, alongside sustained clinician engagement.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605261454051 - Supplemental material for Transforming perioperative care: The current landscape and future trajectory of artificial intelligence in anesthesia–A narrative review
Supplemental material, sj-pdf-1-imr-10.1177_03000605261454051 for Transforming perioperative care: The current landscape and future trajectory of artificial intelligence in anesthesia–A narrative review by Pan Zhang, Ling Wu, Yunxi Liao and Hong Li in Journal of International Medical Research
Footnotes
Acknowledgements
The authors acknowledge the use of ChatGPT (OpenAI) solely for language polishing and grammar checking. All scientific content, analysis, and conclusions remain the sole intellectual responsibility of the authors.
Author contributions
H.L. conceived and designed this study; P.Z. wrote the manuscript. P.Z., Y.L., and L.W collected and screened the literature; and L.W. revised the manuscript. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Data availability statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Declaration of conflicting interests
The authors declare no competing interests.
Funding
No funding was received for this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.