
Abstract
Objectives
Intracerebral hemorrhage is a cerebrovascular disease associated with high mortality and disability rates. Electrolyte disorders are common in intensive care unit patients; however, most current studies have focused on the association between a single electrolyte abnormality and intracerebral hemorrhage prognosis, lacking a comprehensive quantitative assessment of multiple electrolyte disturbances. This study aimed to explore the prognostic value of a multielectrolyte disturbance scoring system for adverse outcomes in intensive care unit patients with intracerebral hemorrhage.
Methods
This retrospective observational cohort study analyzed data from the Medical Information Mart for Intensive Care IV database. A scoring system covering six electrolytes was constructed, with scores assigned according to the abnormal range, number of concurrent abnormalities, and duration. Multivariate logistic and Cox regression analyses were used to evaluate the association between the score and 30-day severe disturbance of consciousness or in-hospital mortality. Subgroup analyses and restricted cubic spline analyses were further performed.
Results
Among 1540 patients, 321 (20.84%) developed 30-day severe disturbance of consciousness. The electrolyte disturbance score was significantly higher in patients with disturbance of consciousness than in those without disturbance of consciousness. Multivariate regression analysis (Model 3, adjusted for all covariates) showed that, compared with T1, both T2 and T3 were associated with an increased risk of 30-day severe disturbance of consciousness and in-hospital mortality. Subgroup analyses confirmed a stable association across most subgroups. Restricted cubic spline analysis revealed a nonlinear positive correlation between the score and both outcomes, with accelerated risk elevation when the score exceeded 2.
Conclusion
The constructed electrolyte disturbance scoring system is a reliable prognostic tool for predicting 30-day severe disturbance of consciousness and in-hospital mortality in intensive care unit patients with intracerebral hemorrhage. A score >2 was associated with a significantly accelerated risk of adverse outcomes, providing a practical threshold for clinical intervention and individualized management.
Keywords
Introduction
Intracerebral hemorrhage (ICH) is among the cerebrovascular diseases associated with the highest mortality and disability rates worldwide, and approximately 30%–50% of patients with ICH require transfer to the intensive care unit (ICU) for advanced life support. 1 Despite advances in diagnostic and therapeutic technologies in recent years, the 30-day in-hospital mortality rate among ICU patients with ICH remains as high as 30%–55%. 2 Among surviving patients, 80%–90% experience residual severe neurological deficits, including disturbance of consciousness, and most lose the ability to work and perform activities of daily living independently, thereby imposing a substantial burden on families and society. 3 Therefore, identifying the key risk factors affecting the prognosis of ICU patients with ICH is of great significance for optimizing clinical management and improving outcomes.
Electrolyte disorders are common complications in ICU patients, with an incidence rate of 40%–60%. These disorders mainly involve imbalances in ions such as sodium (Na+), potassium (K+), calcium (Ca2+), magnesium (Mg2+), chloride (Cl−), and phosphorus (P).4,5 As core regulators of cellular metabolism, neuroelectrophysiological activity, and vascular homeostasis, electrolyte disturbances may exacerbate brain injury through multiple mechanisms. Studies have shown that hyponatremia can induce cerebral edema and increase intracranial pressure; hyperkalemia may lead to arrhythmia and reduced cerebral perfusion; and calcium–magnesium imbalance may inhibit neurotransmitter release and aggravate disturbance of consciousness. 5 However, most current studies have focused on the association between a single electrolyte abnormality and ICH prognosis, lacking a comprehensive quantitative assessment of multiple electrolyte disturbances. In addition, ICU patients often have comorbid underlying diseases, such as diabetes mellitus and chronic kidney disease, which may exacerbate the interaction between electrolyte imbalance and brain injury. Nevertheless, existing studies have not systematically explored the prognostic value of multiple electrolyte disturbances in this population.
Based on the publicly available Medical Information Mart for Intensive Care IV (MIMIC-IV) database, this study constructed a scoring system covering six types of electrolyte disturbances and systematically analyzed its association with 30-day severe disturbance of consciousness and in-hospital mortality in ICU patients with ICH. Subgroup analyses were further conducted to explore differences in the associations between electrolyte disturbances and severe disturbance of consciousness as well as 30-day mortality across different subgroups. Meanwhile, restricted cubic spline (RCS) analysis was used to investigate the associations between the electrolyte disturbance score and mortality as well as disturbance of consciousness. This study aimed to provide evidence-based support for clinical prognostic assessment and intervention.
Methods
Study design and data source
This retrospective observational study used data obtained from the MIMIC-IV database. This database contains detailed clinical records of ICU patients treated at Beth Israel Deaconess Medical Center between 2008 and 2019 and is publicly accessible. After completion of the Collaborative Institutional Training Initiative program, one author (HW) obtained access to the MIMIC-IV database (Certification Number: 73468818). The study was conducted in accordance with the Declaration of Helsinki of 1975, as revised in 2024. Because all analyzed data were deidentified, the requirement for written informed consent was waived by the Institutional Review Board of Beth Israel Deaconess Medical Center (Boston, Massachusetts, USA). The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 6
Study participants
The inclusion criteria were as follows: (a) age ≥18 years; (b) clinical diagnosis of intracerebral hemorrhage; (c) first ICU admission (for patients with multiple admissions, only data from the first hospitalization were included); and (d) complete electrolyte test data to enable calculation of the electrolyte disturbance score.
The exclusion criteria were as follows: (a) age <18 years; (b) ICU length of stay <24 h, to exclude patients admitted for short-term observation; (c) missing electrolyte test data, including sodium, potassium, calcium, magnesium, chloride, and phosphorus; and (d) missing data for key covariates, such as vital signs and comorbid underlying diseases. The flowchart of the patient inclusion process is shown in Figure 1. We consecutively included all patients who met the pre-specified inclusion criteria from the MIMIC-IV database between 2008 and 2019, without selective or random sampling during the inclusion process.
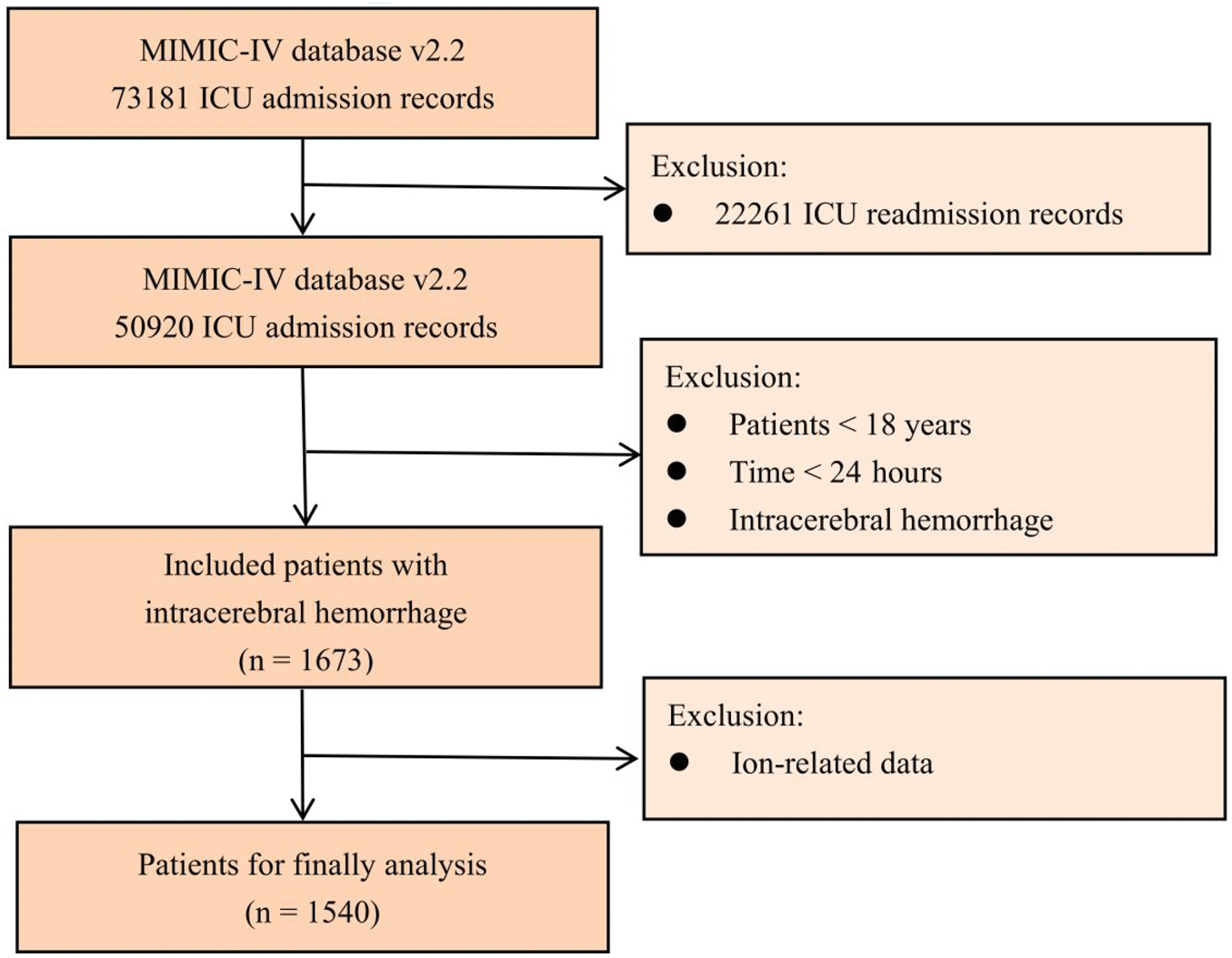
Flowchart of patient inclusion and exclusion from the MIMIC-IV database. Medical Information Mart for Intensive Care IV (MIMIC).
Data collection and variable definition
Based on the first electrolyte test results after ICU admission and dynamic monitoring data, six core electrolytes (Na+, K+, Ca2+, Mg2+, Cl−, and P) were included, and the scoring criteria were defined as follows:
A score of 1 was assigned when the level of a single electrolyte was outside the normal reference range. A score of 2 was assigned when the level of any electrolyte deviated by >20% from the upper or lower limit of the normal range. An additional 1 point was added when two or more electrolyte abnormalities were present simultaneously. An additional 1 point was added when the duration of electrolyte abnormalities exceeded 48 h.7–9
Total scores were categorized by tertiles as follows: T1 (low-score group, <1), T2 (medium-score group, 1–2), and T3 (high-score group, >2).
The following potential confounding factors were included: (a) Demographic indicators. Age, sex, body mass index (BMI), and ethnicity; (b) Vital signs. Oxygen saturation (SpO2), heart rate, admission Glasgow Coma Scale (GCS) score, Sequential Organ Failure Assessment (SOFA) score, and mechanical ventilation; (c) Laboratory indicators. Red blood cell count (RBC), white blood cell count (WBC), hemoglobin, platelet count (PLT), serum creatinine; (d) Medication use. Diuretics, aspirin, statins, beta-blockers, angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers (ACEI/ARB), insulin, and vasopressors; (e) Comorbid underlying conditions. Hypertension, diabetes mellitus, heart failure, and chronic kidney disease.
Outcome measures
The primary outcome was severe disturbance of consciousness occurring within 30 days, defined as a GCS score <8. The secondary outcome was 30-day in-hospital mortality, confirmed by hospital discharge records or death certificates.
Statistical analysis
Statistical analyses were performed using Statistical Package for Social Sciences (SPSS) version 26.0 and R version 4.3.0, with a two-tailed significance level (α) of 0.05.
For descriptive statistics, continuous variables were expressed as “mean ± SD (x ± s),” and categorical variables were presented as “count (percentage, %).”
For intergroup comparisons, independent-samples t-tests were used for normally distributed continuous variables, whereas the Mann–Whitney U test was used for non-normally distributed variables. Pearson’s chi-square test or Fisher’s exact test (when the expected frequency was <5) was used for categorical variables.
For correlation analysis, multivariate logistic regression analysis was used to explore the association between the electrolyte disturbance score and the risk of 30-day severe disturbance of consciousness. Multivariate logistic and Cox regression analyses were used to evaluate the association between the electrolyte disturbance score and the risk of 30-day in-hospital mortality. Three models were constructed for each regression analysis: (a) Model 1. Unadjusted model (univariate analysis); (b) Model 2. Adjusted for age, sex, and BMI; and (c) Model 3. Adjusted for age, sex, BMI, hypertension, diabetes mellitus, heart failure, chronic kidney disease, SpO2, heart rate, RBC, WBC, PLT, hemoglobin, serum creatinine, admission GCS score, SOFA score, mechanical ventilation, and medication use.
For subgroup analysis, stratified analyses were conducted according to age (≤65 years/>65 years), sex (male/female), BMI (≤30 kg/m2/>30 kg/m2), and comorbid underlying conditions (hypertension/no hypertension and diabetes mellitus/no diabetes mellitus, among others) to evaluate the stability of the association between the electrolyte disturbance score and outcome.
In addition, RCS analysis was performed to investigate the associations between the electrolyte disturbance score and mortality as well as disturbance of consciousness.
Results
Baseline characteristics of patients
Among the 1540 patients, 321 (20.84%) developed severe disturbance of consciousness within 30 days (disturbance of consciousness group), whereas 1219 (79.16%) maintained normal consciousness (normal group). Comparisons of baseline characteristics between the two groups are presented in Table 1. The total electrolyte disturbance score was significantly higher in the disturbance of consciousness group than in the normal group (2.14 ± 1.14 vs. 1.37 ± 1.02, p < 0.001). In addition, there were significant differences between the two groups in SpO2, RBC, WBC, hemoglobin, PLT, serum creatinine, admission GCS score, SOFA score, and mechanical ventilation as well as in the use of diuretics, aspirin, beta-blockers, ACEI/ARB, insulin, and vasopressors (p < 0.05). However, there were no significant differences found between the two groups in age, sex, BMI, or comorbid underlying conditions, including hypertension, diabetes mellitus, heart failure, and chronic kidney disease (p > 0.05).
Baseline characteristics of study population.

ACEI/ARB: angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers; BMI: body mass index; GCS: Glasgow Coma Scale; PLT: platelet count; RBC: red blood cell count; SOFA: Sequential Organ Failure Assessment; SpO2: oxygen saturation; WBC: white blood cell count.
Association between the electrolyte disorder score and 30-day severe disturbance of consciousness or in-hospital mortality
Multivariate regression analyses showed that an increase in the electrolyte disturbance score was significantly associated with both the risk of 30-day severe disturbance of consciousness and the risk of 30-day in-hospital mortality. For the risk of 30-day severe disturbance of consciousness, a higher score was significantly associated with an increased risk regardless of whether covariates were adjusted for (Figure 2(a)). In Model 3 (adjusted for all covariates), compared with the T1 group, patients in the T2 group had a 56% higher risk (odds ratio (OR) = 1.56), whereas patients in the T3 group had a 105% higher risk (OR = 2.05); both differences were statistically significant (p < 0.001). Meanwhile, the electrolyte disturbance score was significantly positively associated with the risk of 30-day in-hospital mortality, and this association remained stable after covariate adjustment (Figure 2(b)). In Model 3, compared with the T1 group, patients in the T2 group (hazard ratio (HR) = 1.91; OR = 2.17) and T3 group (HR = 1.76; OR = 2.08) both had an increased risk, and these differences were also statistically significant (p < 0.001). Multivariate logistic regression and Cox regression analyses yielded consistent and stable effect estimates for the association between the electrolyte disturbance score and the risk of 30-day in-hospital mortality. These findings indicate that a higher degree of electrolyte disturbance is associated with a greater risk of severe disturbance of consciousness and 30-day mortality, and that this association remains statistically significant after adjustment for multiple covariates.
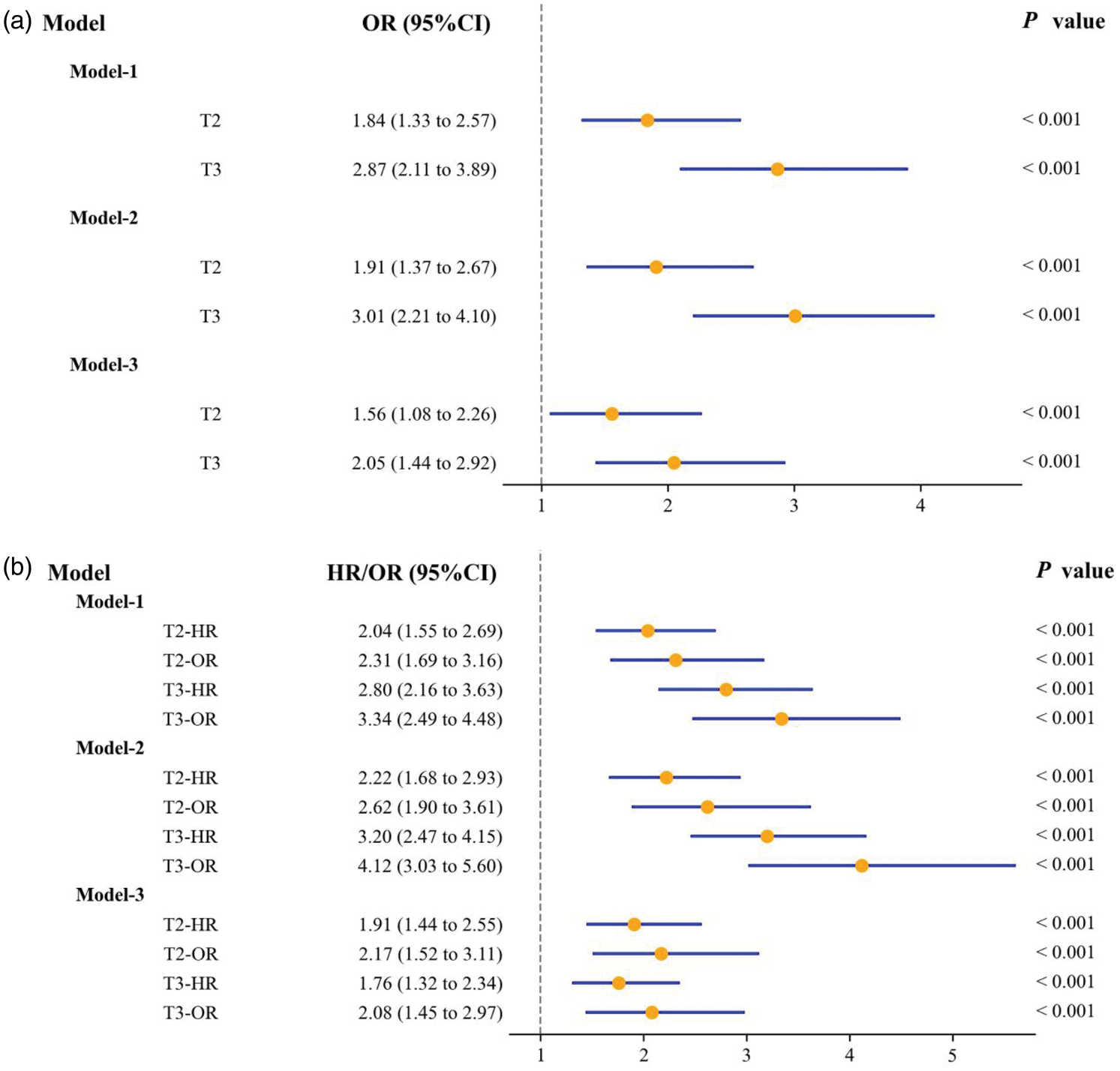
Forest plot of the association between electrolyte imbalance score and 30-day severe consciousness disorder (a) and in-hospital mortality (b). Model 1. No covariates adjusted (univariate analysis); Model 2. Adjusted for age, sex, and BMI; Model 3. Adjusted for age, sex, BMI, hypertension, diabetes mellitus, heart failure, chronic kidney disease, SpO2, heart rate, RBC, WBC, PLT, hemoglobin, serum creatinine, admission GCS, SOFA, mechanical ventilation, and medication use. OR: odds ratio; HR: hazard ratio; CI: confidence interval; BMI: body mass index; SpO2: Oxygen saturation; RBC: red blood cell; WBC: white blood cell; PLT: platelet count; GCS: Glasgow Coma Scale; SOFA: Sequential Organ Failure Assessment.
Subgroup analyses of the association between the electrolyte disturbance score and 30-day severe disturbance of consciousness or in-hospital mortality
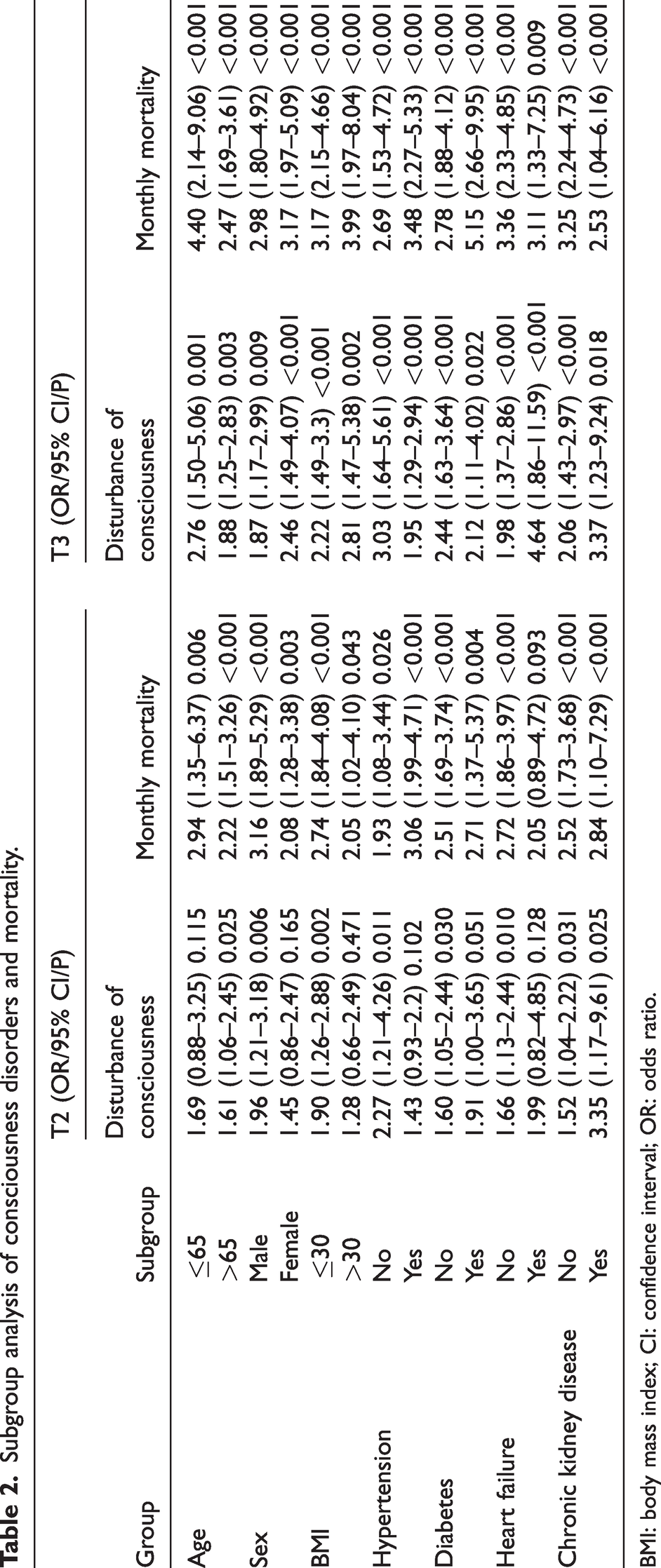
Subgroup analyses for severe disturbance of consciousness and 30-day in-hospital mortality were conducted to explore whether the associations between the electrolyte disturbance score (T2 and T3 tertiles) and these outcomes differed across subgroups. The subgroups were stratified according to age, sex, BMI, and the presence or absence of hypertension, diabetes mellitus, heart failure, and chronic kidney disease (Table 2).
Subgroup analysis of consciousness disorders and mortality.
BMI: body mass index; CI: confidence interval; OR: odds ratio.
Association with severe disturbance of consciousness: Except in the subgroups of patients aged ≤65 years, female patients, patients with BMI >30 kg/m2, patients with hypertension, patients with diabetes mellitus, and patients with heart failure, in which the association between the T2 tertile and severe disturbance of consciousness was not statistically significant (p > 0.05), higher electrolyte disturbance scores were significantly associated with an increased risk of 30-day severe disturbance of consciousness across all other subgroups (p < 0.05). The strongest association was observed in patients with heart failure in the T3 tertile (OR = 4.64, 95% confidence interval (CI): 1.86–11.59, p < 0.001).
Association with in-hospital mortality: Except for the T2 tertile in patients with heart failure (OR = 2.05, 95% CI: 0.89–4.72, p = 0.093), the T2 and T3 tertiles of the electrolyte disturbance score were significantly positively associated with an increased risk of in-hospital mortality across all other subgroups (p < 0.05). The strongest association was observed in patients with diabetes mellitus in the T3 tertile (OR = 5.15, 95% CI: 2.66–9.95, p < 0.001).
RCS analysis of the association between electrolyte disturbance score and 30-day severe disturbance of consciousness or in-hospital mortality
RCS analysis showed that the electrolyte disturbance score had a significant nonlinear positive association with both the risk of 30-day severe disturbance of consciousness and the risk of 30-day in-hospital mortality. Both the overall and nonlinear tests for these associations were statistically significant (p < 0.001).
Association with 30-day severe disturbance of consciousness
When the electrolyte disturbance score was <1, the OR was <1. When the score reached ≥1, the OR began to increase rapidly. When the score exceeded 2, the OR continued to rise, suggesting that the risk of severe disturbance of consciousness increased nonlinearly with worsening electrolyte disturbances (Figure 3(a)).
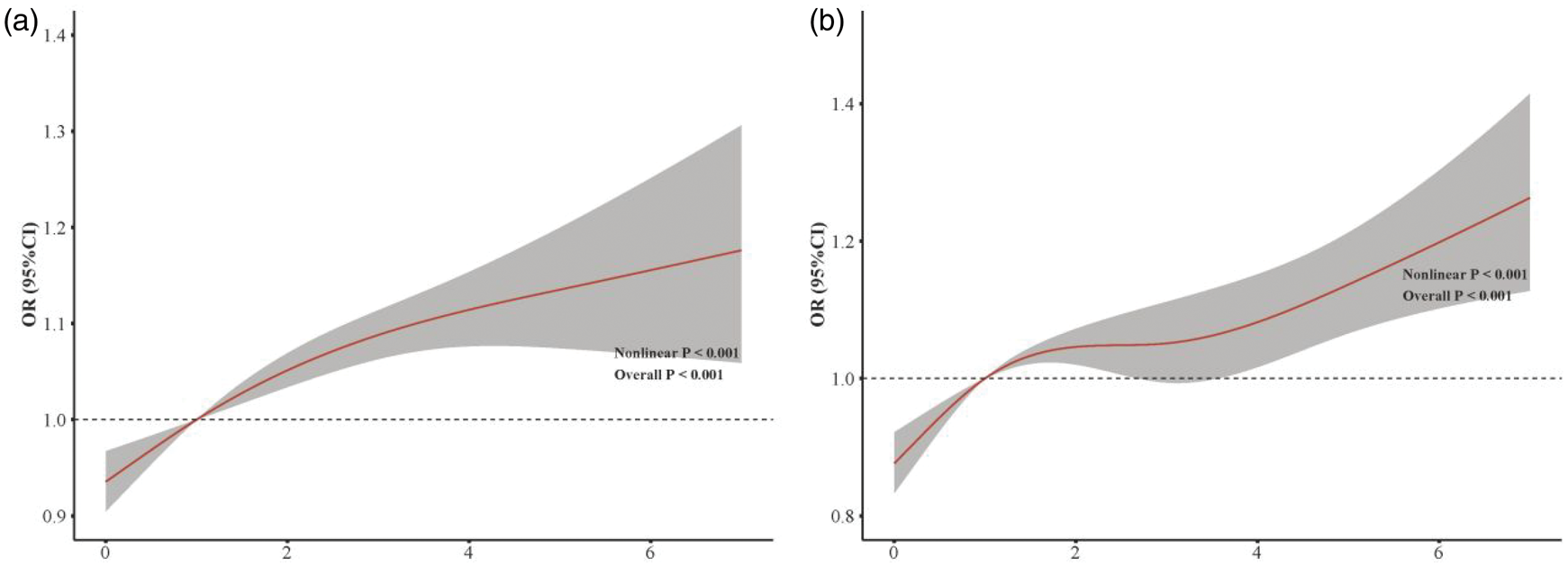
The electrolyte imbalance score and the restricted cubic spline curves for the 30-day risk of severe consciousness disorder (a) and in-hospital mortality (b). CI: confidence interval; OR: odds ratio.
Association with 30-day in-hospital mortality
When the electrolyte disturbance score was <1, the OR was <1 (reference value = 1), suggesting that mild electrolyte disturbances might have a weak protective effect. As the score increased to 1–2, the OR rapidly increased above 1. When the score exceeded 2, the OR continued to increase at an accelerated rate, and the increase in risk became more pronounced, particularly when the score was ≥4. These findings indicate that greater severity of electrolyte disturbances was associated with a nonlinear accelerated increase in mortality risk (Figure 3(b)).
Discussion
Based on the MIMIC-IV database, this study constructed a scoring system covering six types of electrolyte disturbances and systematically explored its association with 30-day severe disturbance of consciousness and in-hospital mortality in ICU patients with ICH. The results demonstrated the following: 1. An increase in the electrolyte disturbance score was significantly associated with a higher risk of both adverse outcomes, and this association remained stable after adjustment for multiple factors. 2. Subgroup analyses further confirmed its predictive value in high-risk populations, including older patients, male patients, and patients with diabetes mellitus. 3. RCS analysis further revealed a nonlinear acceleration in risk, with mortality risk increasing markedly when the score exceeded 2 points. This electrolyte disturbance scoring system may serve as a simple and practical indicator for prognostic assessment in patients with ICH, thereby facilitating the development of individualized monitoring and correction strategies.
Electrolyte disturbances may affect the prognosis of ICU patients with ICH primarily through disruption of neuroelectrophysiological function and the intracranial environment. Na+ and K+ ions are essential for maintaining the membrane potential of nerve cells. Hyponatremia can cause osmotic imbalance in nerve cells and cerebral edema, increase intracranial pressure, compress brain tissue, and directly induce disturbance of consciousness.10,11 Hyperkalemia, in contrast, may inhibit myocardial contractility, trigger arrhythmia, reduce cerebral perfusion pressure, and exacerbate cerebral ischemia and hypoxia.12,13 In addition, calcium ions are involved in the regulation of neurotransmitter release, such as glutamate. Hypocalcemia may lead to abnormal neuronal excitability, increase the risk of epileptic seizures, and further aggravate brain injury.14,15 Electrolyte disturbances are also often accompanied by metabolic imbalance. Previous studies have shown that hypomagnesemia can inhibit ATPase activity, resulting in disorders of cellular energy metabolism.16,17 Hyperphosphatemia has been associated with vascular calcification and endothelial dysfunction, thereby aggravating cerebral microcirculatory disturbances. 18 In the present study, the WBC count was significantly elevated in the patients with disturbance of consciousness group (p < 0.001), suggesting that electrolyte disturbances may activate inflammatory pathways (e.g. NF-κB) to promote the release of pro-inflammatory factors, exacerbate blood–brain barrier disruption and neuroinflammation, and form a vicious cycle of “electrolyte imbalance–inflammatory response–brain injury.”19–21
In addition, interactions may exist between underlying diseases and treatment strategies. Subgroup analysis showed that, in patients with diabetes mellitus, the OR for mortality risk in the T3 group reached 5.15 (p < 0.001), whereas in patients with chronic kidney disease, the OR for disturbance of consciousness in the T3 group was 3.37 (p = 0.018). This may be attributed to the fact that patients with diabetes mellitus are often affected by insulin resistance, and insulin use (utilization rate of 85.05% in the patients with disturbance of consciousness group; p < 0.001) can promote intracellular K+ influx, thereby exacerbating hypokalemia.22–24 Patients with chronic kidney disease have impaired renal excretory function, making them more susceptible to hyperkalemia and hyperphosphatemia. Hyperphosphatemia, in turn, may lead to vascular calcification and microcirculatory disturbances, further reducing cerebral blood supply.25,26 Additionally, in patients with heart failure, the OR for disturbance of consciousness in the T3 group reached 4.64 (p < 0.001), which may be related to the high utilization rate of diuretics in patients with heart failure (71.53% in the normal group). Diuretics can promote the loss of Na+, K+, and Mg2+, thereby aggravating electrolyte disturbances. 27
Compared with single electrolyte abnormalities, the synergistic effects of multiple electrolyte disturbances may be more severe. Most previous studies have focused on single electrolyte abnormalities, whereas the scoring system developed in this study incorporated six types of ions and accounted for both the number and duration of abnormalities. It was found that multiple ion abnormalities (with an additional 1 point) were significantly associated with an increased risk of adverse outcomes. This may be because multiple electrolyte disturbances can exert synergistic effects. Previous studies have shown that when hyponatremia is combined with hypomagnesemia, the combined effects of neuronal edema and impaired energy metabolism result in substantially greater damage to brain function than either disorder alone.28,29 Furthermore, prolonged duration of abnormalities (>48 h, with an additional 1 point) may extend the exposure time to brain injury, leading to irreversible neurological damage and further increasing the risk of adverse outcomes.
The electrolyte disturbance score constructed in this study is both comprehensive and practical. It covers the six most common types of electrolyte abnormalities in ICU patients, with scoring criteria based on routine laboratory indicators. No complex calculations are required, allowing rapid bedside assessment. In addition, the early warning threshold is clearly defined. RCS analysis showed that the risk of adverse outcomes increased markedly when the score exceeded 2 points, suggesting that a score of 2 may serve as an intervention threshold in clinical practice. For patients with a score ≥2, enhanced electrolyte monitoring (e.g. every 12 h) should be implemented, and electrolyte disturbances should be corrected promptly through fluid replacement and ion supplementation. Furthermore, the score allows accurate identification of high-risk subgroups. Subgroup analyses indicated that patients aged >65 years, patients with diabetes mellitus, and patients with chronic kidney disease are key populations requiring intervention. These patients should undergo electrolyte disturbance scoring upon admission, and individualized monitoring and correction strategies should be developed. For example, patients with diabetes mellitus require careful balancing of insulin use and potassium supplementation, whereas patients with chronic kidney disease should avoid medications associated with high potassium levels.
Limitations
This study explored the association between the electrolyte disturbance score and 30-day severe disturbance of consciousness as well as in-hospital mortality in ICU patients with ICH. Although the constructed electrolyte disturbance score is comprehensive and simple and may serve as a potential indicator for clinical prognostic evaluation, several limitations should be acknowledged. (1) This study adopted a retrospective design, which cannot completely exclude the influence of residual confounding factors (e.g. ICH volume and surgical methods that were not included as covariates), potentially affecting the accuracy of the results. (2) The score was developed and validated using data from a single database (internal validation only). Because the data were derived from a single database and were not tested in an independent external cohort, the generalizability and predictive performance of the score in other populations remain uncertain. (3) The score in this study was calculated based on the first electrolyte test obtained after admission. Dynamic changes in the score during ICU hospitalization were not evaluated, and it remains unclear whether the risk decreases after correction of electrolyte disturbances. Prospective studies are needed to further verify the interventional value of the score. (4) The data were derived from a single medical center in the United States, which limits the geographic and demographic representativeness of the study population. Differences in ethnicity and treatment protocols, including the types and dosages of diuretics, may exist across regions; therefore, caution is warranted when generalizing these findings to other population.
Conclusion
This study constructed a comprehensive electrolyte disturbance scoring system (incorporating six core electrolytes and three key abnormality parameters: range, quantity, and duration) and systematically verified its prognostic value for 30-day severe disturbance of consciousness and in-hospital mortality in 1540 ICU patients with ICH. The results demonstrated that the electrolyte disturbance score may serve as an independent risk factor for both adverse outcomes, with stable associations observed across most subgroups after adjustment for multiple confounding factors. Importantly, RCS analysis revealed a nonlinear accelerated risk pattern. When the score exceeded 2, the risks of severe disturbance of consciousness and mortality increased markedly, providing a clear and clinically actionable threshold for intervention. Compared with previous studies focusing on single electrolyte abnormalities, this scoring system captures the synergistic effects of multiple electrolyte disturbances, is easy to calculate using routine laboratory data, and supports rapid bedside assessment. Therefore, it may serve as a practical tool for prognostic evaluation and individualized management in ICU patients with ICH. Future prospective multicenter studies are needed to further validate the predictive performance of this scoring system and optimize intervention strategies for patients with scores ≥2, ultimately improving the prognosis of this high-risk population.
Footnotes
Acknowledgments
Not applicable.
Author contributions
Conceptualization: HW; Data curation: HZ; Formal analysis: PZ, HW, and MC; Investigation: PZ and JT; Methodology: HW; Project administration: ZC; Resources: CH; Software: HW, PZ, and MC; Supervision: ZC; Validation: JM; Visualization: HW and YL; Writing–original draft: HW; Writing–review & editing: ZC. All authors provided critical review of the manuscript and approved the final version for submission.
Data availability statement
The data used in this study were obtained from the publicly accessible Medical Information Mart for Intensive Care IV (MIMIC-IV) database. Further inquiries may be directed to the corresponding author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.