
Abstract
Objective
Cytomegalovirus reactivation is a clinically significant complication after allogeneic hematopoietic stem cell transplantation. Valganciclovir is commonly used for cytomegalovirus prophylaxis; however, the optimal dosing strategy remains unclear. This study compared the efficacy and safety of ultra-low-dose valganciclovir (450 mg every other day) and low-dose valganciclovir (450 mg daily) in preventing cytomegalovirus reactivation after allogeneic hematopoietic stem cell transplantation.
Methods
We retrospectively reviewed adult patients who underwent allogeneic hematopoietic stem cell transplantation from January 2020 to December 2023. Individuals receiving low-dose (n = 31) or ultra-low-dose (n = 35) valganciclovir as cytomegalovirus prophylaxis were included. Cytomegalovirus DNAemia was evaluated within the first 14 weeks and then at 14–28 weeks after transplantation. Cytomegalovirus disease, acute graft-versus-host disease, survival outcomes, and hematologic toxicities were also assessed.
Results
The prevalence of early cytomegalovirus reactivation was 13.8% in the low-dose group and 20.0% in the ultra-low-dose group (p = 0.301). Late reactivation rates were similarly low in the low-dose and ultra-low-dose groups (3.6% vs. 6.2%, p = 1.000). Hematologic adverse events were comparable; however, treatment discontinuation due to cytopenia was significantly more common with low-dose therapy (48.4% vs. 17.1%, p = 0.007). Overall survival (80.6% vs. 75.8%, p = 0.839) and acute graft-versus-host disease (29.1% vs. 45.7%, p = 0.381) rates did not exhibit statistically significant differences between the two groups.
Conclusions
Ultra-low-dose valganciclovir demonstrated better tolerability but may provide less protection against cytomegalovirus reactivation.
Introduction
Allogeneic hematopoietic stem cell transplantation (HSCT) (allo-HSCT) plays a critical role in the treatment of hematologic disorders. Cytomegalovirus (CMV) infection is a critical complication of allo-HSCT that leads to substantial morbidity and mortality. 1 Previous reviews have reported an incidence of 30%–70% for CMV reactivation after allo-HSCT. 2 CMV infection has exerted a particularly significant impact in Taiwan, with the CMV seroprevalence consistently exceeding 90% over the past 40 years.3,4 Moreover, CMV reactivation is a common complication of allo-HSCT in Taiwan. 5 CMV disease can affect multiple organs, including the lungs, liver, gastrointestinal tract, eyes, and central nervous system, posing a persistent threat to post-transplant outcomes. Currently, gastrointestinal disease is the most common manifestation of CMV infection.1,6
Both prophylactic and preventive treatments were administered to manage CMV reactivation after allo-HSCT. However, according to previous systematic reviews, prophylaxis is the preferred approach.7,8 Preventing CMV reactivation in high-risk patients is critical for post-transplant care. High-risk groups include CMV-seropositive recipients; those receiving HLA-mismatched donor grafts; and patients treated with in vivo T-cell medicines, such as antithymoglobulin and alemtuzumab, or post-transplant cyclophosphamide. 9
Letermovir is an antiviral agent with a unique mechanism of action that targets the CMV DNA terminase complex by binding to its components, including UL51, UL56, or both. It has been shown to significantly reduce the incidence of clinically significant CMV infections following allo-HSCT and improve mortality. 10 Therefore, letermovir is considered a first-in-class drug by the US Food and Drug Administration. 11 However, letermovir poses a significant financial burden compared with traditional antiviral agents used in a preventive therapy-only strategy, which limits its accessibility in resource-constrained regions. 12 Moreover, letermovir does not prevent herpes simplex or herpes zoster virus infections in post-transplant patients.
Before letermovir became the standard for CMV prophylaxis in allo-HSCT recipients, other antiviral medications were administered. Randomized studies have demonstrated that ganciclovir, high-dose acyclovir, and valacyclovir are effective in reducing the risk of CMV infection following HSCT.13–15 Valganciclovir, an oral prodrug of ganciclovir, provides significant advantages in managing CMV infections in HSCT recipients, with approximately 60% oral bioavailability and a safety profile comparable to that of ganciclovir. 16 Its oral administration, well-established efficacy, and safety make it the preferred choice for outpatient preventive CMV treatment in HSCT settings. 17
Prophylactic valganciclovir has also been shown to be effective in preventing CMV infections in various transplantation settings. Although standard dosing (450 mg twice daily) significantly reduces CMV infection rates, its use is often limited by leukopenia, leading to treatment discontinuation in >50% of cases. 18 Low-dose valganciclovir (450 mg/day) has been explored in allo-HSCT to mitigate bone marrow suppression, with only 15% of patients developing CMV DNAemia by week 14. However, 20% of patients on low-dose valganciclovir discontinued treatment prematurely due to adverse effects compared with only 10.2% of patients on letermovir, indicating that, although effective, low-dose valganciclovir remains less tolerable than letermovir in allo-HSCT patients.10,19 The efficacy and safety of ultra-low-dose valganciclovir in preventing CMV reactivation after allo-HSCT remain uncertain and warrant further investigation. Therefore, we conducted a retrospective study to address this research question.
In this retrospective study, we evaluated allo-HSCT recipients to compare the effectiveness of ultra-low-dose valganciclovir (450 mg every other day) and low-dose valganciclovir (450 mg daily) in preventing CMV reactivation and infection. We also examined differences in CMV infection rates, hematologic adverse effects, and incidence of graft-versus-host disease (GVHD) between the two dosing regimens.
Materials and methods
Patient population
The reporting of this study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational research. 20 Briefly, we retrospectively reviewed the medical records of adult patients (aged ≥18 years) who underwent allo-HSCT with peripheral blood stem cells at our institution between January 2020 and December 2023. Patients were consecutively included according to predefined inclusion and exclusion criteria, and a total of 99 patients were initially screened. All patients had preserved renal and liver functions prior to allo-HSCT. Patients were excluded for the following reasons: (a) absence of antithyroglobulin (ATG) in the GVHD prophylaxis regimen (n = 1); (b) no CMV prophylaxis or development of CMV DNAemia or CMV disease prior to initiation of prophylaxis (n = 15); and (c) receipt of valganciclovir at dosing frequencies other than 450 mg/day or 450 mg every other day (n = 14). For patients who underwent multiple transplantations (n = 3), only data from the first transplantation were included. After applying these criteria, a total of 66 patients were included in the final analysis.
Participant details were deidentified, and the study was conducted according to the current version of the Declaration of Helsinki. The Institutional Review Board of Taichung Veterans General Hospital approved this study (Approval Number: CE24388B). The Institutional Review Board of Taichung Veterans General Hospital agreed to waive the requirement of written informed consent from the participants owing to the retrospective nature of the study.
GVHD prophylaxis
The GVHD prophylaxis regimen consisted of cyclosporine (target trough level 150–250 ng/mL), mycophenolic acid (720 mg twice daily starting on day −2 and typically continued until approximately day 60), and short-course methotrexate (15 mg/m2 on day 1 and 10 mg/m2 on days 3, 6, and 11), except in patients undergoing haploidentical transplantation. For patients who underwent haploidentical transplantation, post-transplant cyclophosphamide (50 mg/kg) was administered. In addition, ATG was routinely administered at 2 mg/kg/day from day −4 to −2, with a consistent dosing schedule across donor types, including matched sibling, matched unrelated, and haploidentical donors. Granulocyte colony-stimulating factor was administered per a standardized institutional protocol to promote neutrophil recovery following transplantation.
CMV prophylaxis and monitoring
In terms of CMV prophylaxis, patients were categorized into two groups, the low-dose valganciclovir group (n = 31) and ultra-low-dose valganciclovir group (n = 35), based on the valganciclovir prophylactic regimen. In the low-dose group, patients received oral valganciclovir at a dose of 450 mg daily, whereas in the ultra-low-dose group, they received valganciclovir at a dosage of 450 mg every other day. In both groups, valganciclovir prophylaxis was initiated at the time of absolute neutrophil engraftment and was typically discontinued approximately 14 weeks after transplantation (day 100).
CMV monitoring was performed using quantitative polymerase chain reaction. Plasma CMV viral load was measured using a real-time polymerase chain reaction assay (COBAS AmpliPrep/COBAS TaqMan CMV system; Roche Molecular Systems, Inc.; Branchburg, NJ, USA). A viral load <1000 copies/mL was considered negative. Preventive antiviral therapy, with or without CMV-specific immunoglobulin, was initiated at ≥1000 copies/mL. Repeat testing and clinical judgment were applied to confirm persistent CMV DNAemia and avoid misinterpretation of transient low-level “blips.” 21
Screening for CMV DNAemia was conducted prior to allo-HSCT and weekly for the first 14 weeks after transplantation. Surveillance was performed approximately every 2 weeks from weeks 14 to 48. CMV disease was defined as the presence of clinical manifestations consistent with CMV infection, as documented in medical records, with histopathological or virological confirmation through immunohistochemical staining or DNA hybridization.
Outcome measurements
Data on baseline demographic and clinical characteristics, including age, sex, donor type (matched sibling donor, matched unrelated donor, or haploidentical donor), CMV serostatus of donors and recipients, and conditioning regimen type, were collected from medical records. Hematologic recovery was assessed by the median time to absolute neutrophil and platelet engraftment, defined according to the European Society for Blood and Marrow Transplantation criteria. Neutrophil engraftment was defined as the first of 3 consecutive days with an absolute neutrophil count ≥500/mm³ after post-transplant nadir. Platelet engraftment was defined as a platelet count ≥20,000/mm³ without transfusion dependency in the preceding 7 days. 22
The primary outcomes included the incidence of CMV DNAemia within the first 14 weeks and at 14–28 weeks after transplantation. Secondary outcomes included the incidence of CMV disease during both time intervals, acute GVHD occurrence, and overall survival. We also evaluated grade ≥3 hematologic adverse events, as defined by the Common Terminology Criteria for Adverse Events, version 5.0, associated with valganciclovir prophylaxis, including leukopenia, neutropenia, anemia, thrombocytopenia, and neutropenic fever. Additionally, the proportion of patients who discontinued valganciclovir prophylaxis prematurely and the reasons for discontinuation were documented.
Statistical analyses
Categorical variables were compared using the chi-square or Fisher’s exact test, as appropriate. Continuous variables were analyzed using the Mann–Whitney U test. Overall survival was estimated using the Kaplan–Meier method, and differences between groups were assessed using the stratified log-rank test. We also estimated the cumulative incidence of CMV reactivation, defined as DNAemia levels exceeding 1000 copies/mL, using competing risk analysis. Cox proportional hazards regression was performed to identify prognostic factors associated with CMV reactivation, with hazard ratios (HRs) and corresponding 95% confidence intervals (CIs) reported. All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) software for Windows, with the statistical significance set at a two-sided p-value <0.05.
Results
Clinical characteristics of the study participants
Table 1 presents the baseline characteristics of the study population. The median age was 48 and 50 years in the low-dose and ultra-low-dose valganciclovir groups, respectively (p = 0.589). Sex distribution was also comparable between the groups, with males comprising 51.6% of the low-dose group and 45.7% of the ultra-low-dose group (p = 0.632). Acute myeloid leukemia was the most prevalent underlying diagnosis in both cohorts, accounting for 71.0% and 54.3% of the patients in the low-dose and ultra-low-dose groups, respectively (p = 0.337). Haploidentical donor transplantations were performed in 41.9% and 51.4% of the patients in the low-dose and ultra-low-dose groups, respectively (p = 0.317). CMV immunoglobulin G (IgG) seropositivity was high in both groups, occurring in 71.0% of the low-dose group and 68.6% of the ultra-low-dose group (p = 0.921). The median time to absolute neutrophil engraftment was 15 days in both groups (p = 0.326). Similarly, the median time to platelet engraftment was 15 and 16 days in the low-dose and ultra-low-dose groups, respectively (p = 0.339). The median follow-up duration was lengthier in the low-dose group than in the ultra-low-dose group, likely reflecting differences in cohort enrollment timing (22.8 vs. 15.0 months); however, this difference was not statistically significant. Overall, the baseline characteristics were well-balanced between the two treatment groups.
Comparison of the clinical characteristics between patients administered low-dose valganciclovir and ultra-low-dose valganciclovir prophylaxis.
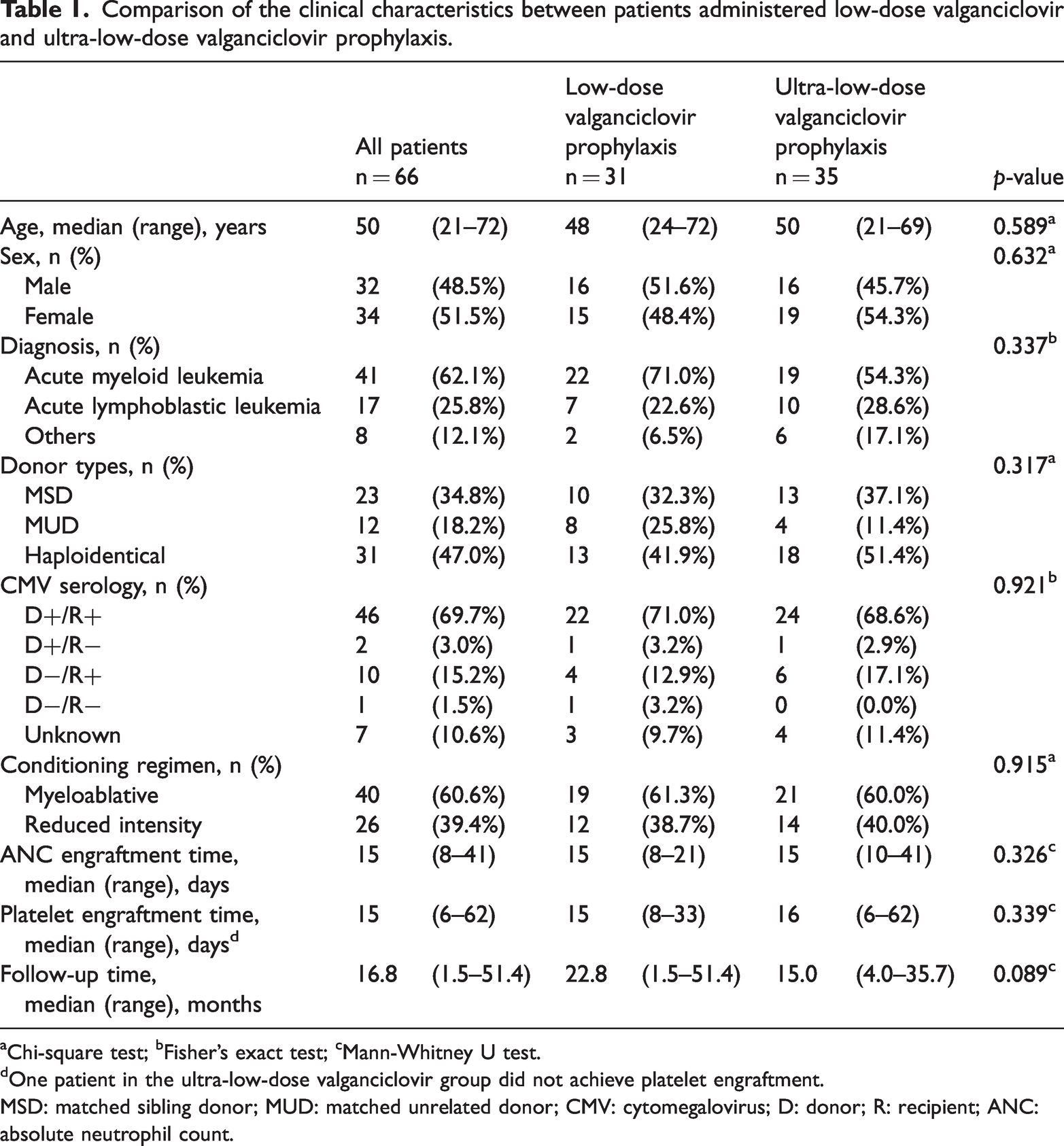
Chi-square test; bFisher’s exact test; cMann-Whitney U test.
One patient in the ultra-low-dose valganciclovir group did not achieve platelet engraftment.
MSD: matched sibling donor; MUD: matched unrelated donor; CMV: cytomegalovirus; D: donor; R: recipient; ANC: absolute neutrophil count.
CMV reactivation and disease
Before week 14, CMV DNAemia occurred in four (13.8%) and seven (20.0%) patients in the low-dose and ultra-low-dose groups, respectively (p = 0.301). The cumulative incidences of CMV reactivation by competing risk were 12.8% and 19.8% in the low- and ultra-low-dose groups, respectively (p = 0.440) (Figure 1(a)). Late reactivation, defined as CMV DNAemia between weeks 14 and 28, was found in one (3.6%) and two patients (6.2%) in the low-dose and ultra-low-dose groups, respectively (p = 1.000). Notably, no cases of CMV disease were observed in either group during follow-up. The incidence of acute GVHD, relapse, and survival were not significantly different between the two groups (Table 2, Figure 1(b)).
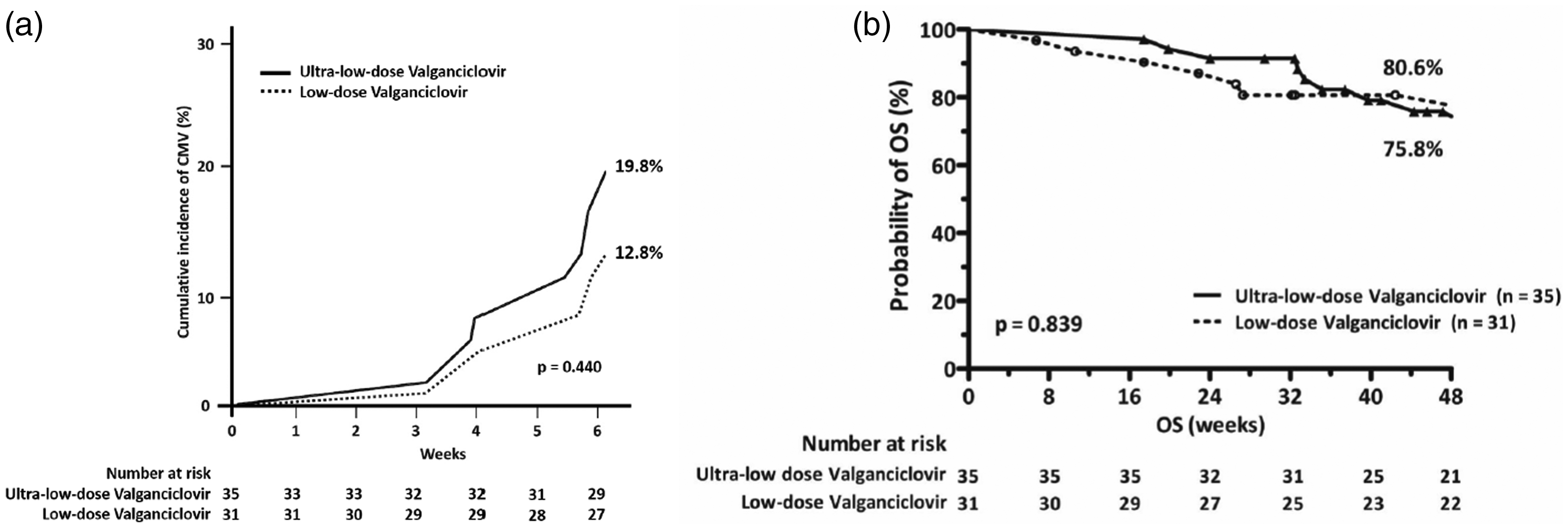
(a) The cumulative incidences of cytomegalovirus (CMV) reactivation by competing risk were 12.8% and 19.8% in the low- and ultra-low-dose groups, respectively (p = 0.440). (b) The overall survival (OS) rates in in the low- and ultra-low-dose groups were 80.6% and 75.8%, respectively (p = 0.839).
Comparison of outcomes between patients administered low-dose valganciclovir and ultra-low-dose valganciclovir prophylaxis.
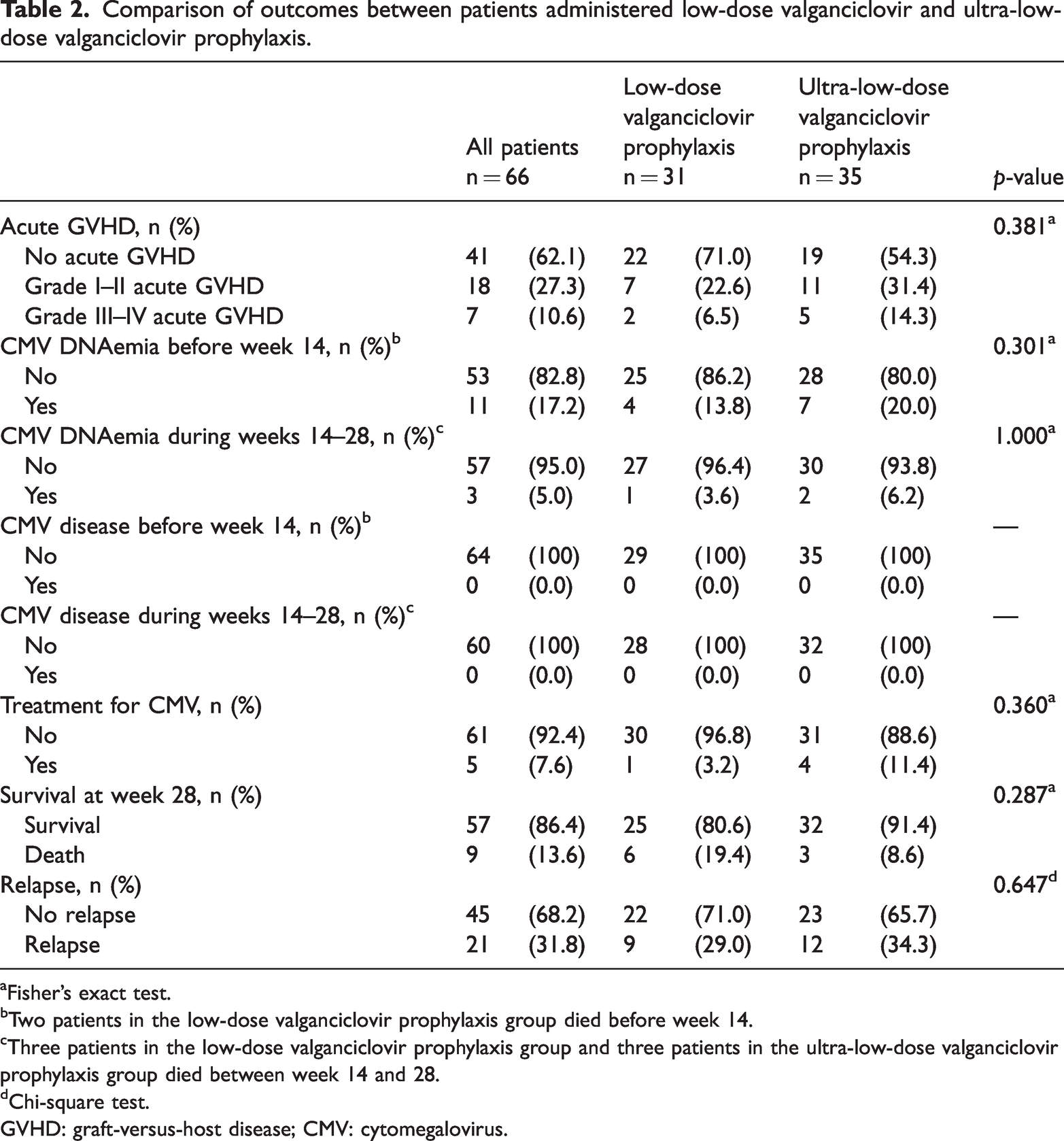
Fisher’s exact test.
Two patients in the low-dose valganciclovir prophylaxis group died before week 14.
Three patients in the low-dose valganciclovir prophylaxis group and three patients in the ultra-low-dose valganciclovir prophylaxis group died between week 14 and 28.
Chi-square test.
GVHD: graft-versus-host disease; CMV: cytomegalovirus.
Hematologic adverse events
Table 3 summarizes hematologic adverse events associated with valganciclovir prophylaxis. The incidence of grade ≥3 leukopenia, neutropenia, anemia, and neutropenic fever was comparable between the low-dose and ultra-low-dose groups (35.5% vs. 45.7%, p = 0.458; 38.7% vs. 40.0%, p = 0.915; 19.4% vs. 22.9%, p = 0.728; and 6.5% vs. 2.9%, p = 0.597, respectively). In contrast, grade ≥3 thrombocytopenia was more frequent in the ultra-low-dose group than in the low-dose group (31.4% vs. 6.5%, p = 0.011).
Grade ≥3 hematological adverse effect of low-dose valganciclovir and ultra-low-dose valganciclovir prophylaxis.
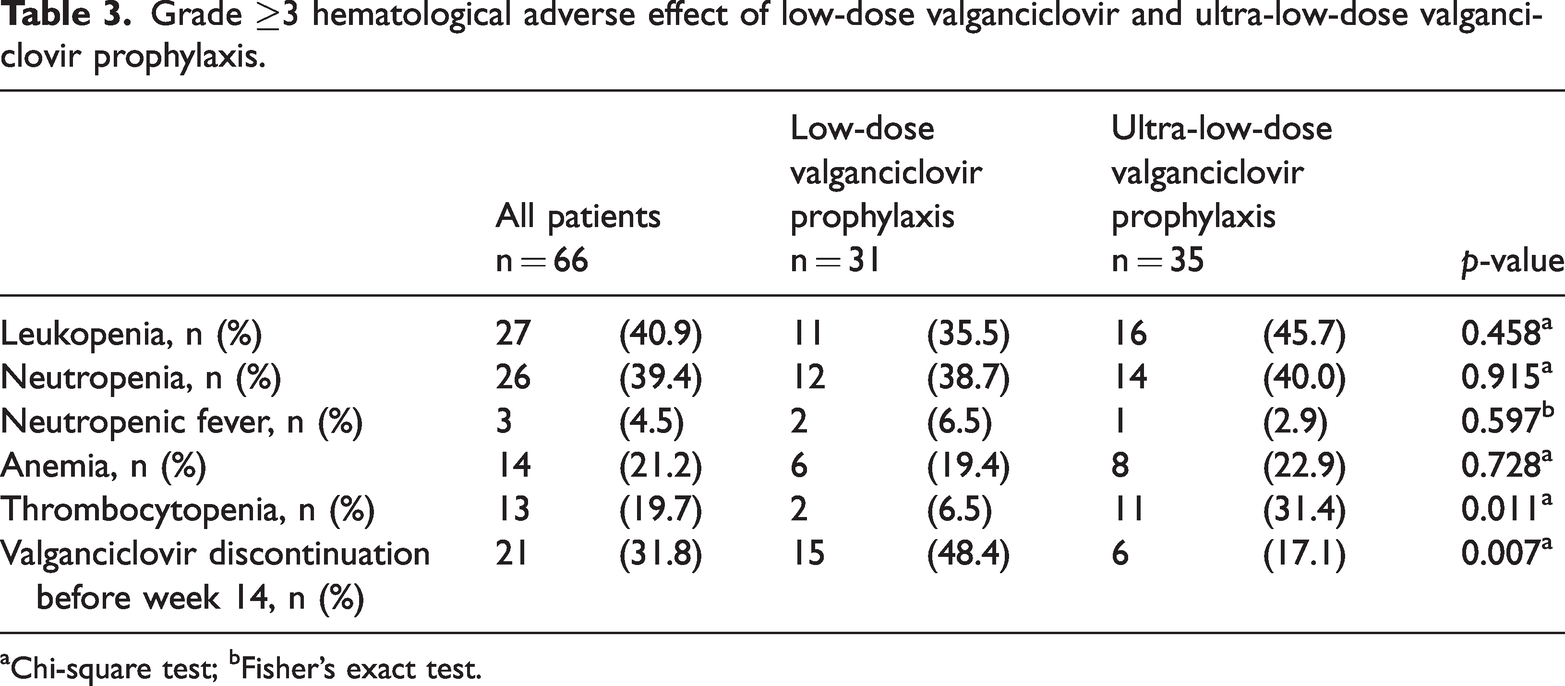
Chi-square test; bFisher’s exact test.
Valganciclovir discontinuation occurred more frequently in the low-dose group than in the ultra-low-dose group (48.4% vs. 17.1%; p = 0.007). In the low-dose group, cytopenia was the most common reason for treatment discontinuation, whereas in the ultra-low-dose group, discontinuation was more often driven by CMV reactivation requiring therapeutic intervention (Supplementary Table 1). Discontinuation decisions were based on overall clinical judgment rather than laboratory parameters alone.
Cox regression analysis revealed no significant associations between CMV reactivation and donor type, age, sex, or conditioning regimen. Furthermore, CMV serology did not appear to affect reactivation, potentially owing to the small sample size. The risk of CMV reactivation was comparable between the low-dose and ultra-low-dose valganciclovir groups (p = 0.517) (Table 4).
Risk factors of CMV DNAemia at week 14.
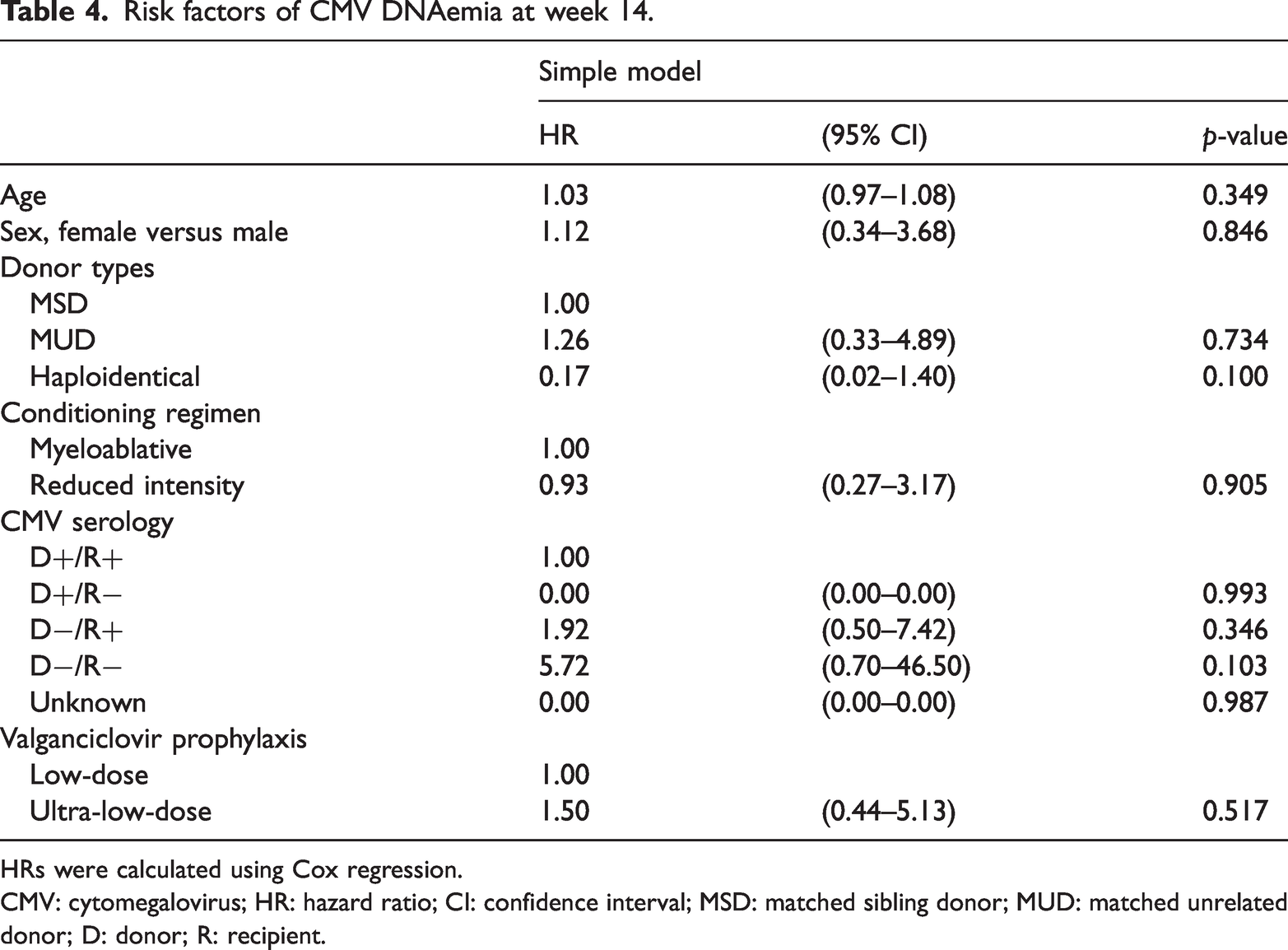
HRs were calculated using Cox regression.
CMV: cytomegalovirus; HR: hazard ratio; CI: confidence interval; MSD: matched sibling donor; MUD: matched unrelated donor; D: donor; R: recipient.
Discussion
In the current study, CMV DNAemia before week 14 occurred in 13.8% and 20.0% of patients in the low-dose and ultra-low-dose groups, respectively (p = 0.301). Late CMV reactivation (weeks 14–28) was observed in 3.6% and 6.2% of the patients in the respective groups (p = 1.000). The incidence of hematologic adverse effects was comparable between the groups. Valganciclovir discontinuation due to adverse events, primarily due to cytopenia, was more common in the low-dose group than in the ultra-low-dose group (48.4% vs. 17.1%; p = 0.007). The overall survival (80.6% vs. 75.8%; p = 0.839) and acute GVHD (29.1 vs 45.7%, p = 0.381) rates were similar between the low- and ultra-low-dose groups.
Valganciclovir plays a role in the prophylaxis and preventive treatment of CMV infections after HSCT. Boeckh et al. 23 have demonstrated that the administration of valganciclovir (900 mg daily for 6 months) does not significantly reduce the rates of mortality, CMV disease, or other invasive infections 270 days after transplantation. However, the study reported a substantial reduction in CMV DNAemia (≥1000 copies/mL) from 36% in the control group to 11% in the valganciclovir group. A previous analysis conducted at our institution further supports the efficacy of valganciclovir in preventing CMV reactivation after HSCT, even at a lower daily dose of 450 mg. In that retrospective study, patients receiving valganciclovir (450 mg daily) exhibited significantly lower CMV reactivation rates than those receiving placebo. 19 The cumulative incidence of CMV viremia reactivation prior to week 14 was 15.0% in the 450-mg/day group, which is consistent with the results of the present study (13.8%). These data suggest that valganciclovir prophylaxis effectively reduces the recurrence of CMV viremia in this high-risk population.
Hematologic toxicity associated with valganciclovir prophylaxis, including leukopenia, neutropenia, anemia, and neutropenic fever, was comparable between the low-dose and ultra-low-dose groups in our study. A meta-analysis by Kalil et al. 24 has demonstrated that reduced or alternate-day valganciclovir dosing is associated with a lower incidence of leukopenia and maintains comparable efficacy in CMV prevention. Notably, grade ≥3 thrombocytopenia was significantly more frequent in the ultra-low-dose group than in the low-dose group (31.4% vs. 6.5%, p = 0.011). This finding is unlikely to be solely attributable to valganciclovir exposure, as post-transplant cytopenia is multifactorial. 25 Similar platelet engraftment times suggest that this difference is not related to delayed hematopoietic recovery. The higher rate of CMV reactivation in the ultra-low-dose group might have contributed to this observation, consistent with prior studies demonstrating an association between CMV reactivation and thrombocytopenia. 26 These findings suggest that reducing valganciclovir exposure will not necessarily translate into lower hematologic toxicity in the allo-HSCT setting and could be associated with unintended clinical consequences.
Despite this, although fewer patients in the ultra-low-dose group discontinued valganciclovir due to cytopenia, the overall incidence of hematologic toxicity was similar between the two groups. This apparent discrepancy could reflect differences in clinical decision making rather than true differences in toxicity. In contrast to findings in solid organ transplantation, this pattern might also be influenced by the increased bone marrow vulnerability in the allo-HSCT setting.
From an efficacy perspective, although the discontinuation rate of valganciclovir was lower in the ultra-low-dose group (17.1% vs. 48.4%, p = 0.007), concerns remain regarding its efficacy for CMV prophylaxis. The CMV reactivation rate was higher in the ultra-low-dose group (20.0% vs. 13.8%, p = 0.301); however, this difference was not statistically significant. Given the relatively short half-life of valganciclovir, alternate-day dosing could result in reduced antiviral exposure, suggesting a trade-off between improved tolerability and antiviral efficacy.
The study cohort comprised a high-risk population, with approximately 50% of patients undergoing haploidentical HSCT and all receiving anti-thymocyte globulin as part of GVHD prophylaxis, both known risk factors for CMV reactivation. 27 Furthermore, the reasons for valganciclovir discontinuation differed between the groups; in the low-dose group, cessation was primarily due to cytopenia, whereas in the ultra-low-dose group, CMV reactivation was the main reason. Given these findings, the clinical benefit of ultra-low-dose valganciclovir in the HSCT setting remains uncertain compared with that of the low-dose regimen. Further investigations are warranted to assess the efficacy of ultra-low-dose valganciclovir, particularly as an alternate-day dosing strategy, for CMV prophylaxis in this high-risk population.
In the pediatric setting, compared with ganciclovir, letermovir has demonstrated a more favorable efficacy and safety profile for CMV prophylaxis in adolescent patients undergoing HSCT. 28 In the adult setting, Limaye et al. 29 have conducted a randomized phase-3, non-inferiority trial comparing letermovir and valganciclovir for CMV prophylaxis in kidney transplant recipients. They have demonstrated that letermovir is not inferior to valganciclovir in preventing CMV disease over 52 weeks and is associated with a lower incidence of leukopenia and neutropenia, supporting its use in this population. In the context of allo-HSCT, valganciclovir is not considered a standard prophylactic agent for CMV disease according to the current US guidelines. 27 The 2017 European Conference on Infections in Leukemia guidelines provided a low level of evidence (C-II) for valganciclovir use in post-HSCT prophylaxis. 25 Furthermore, alternative anti-CMV agents have not demonstrated sufficient efficacy for preventing CMV disease in this setting. Although effective, foscarnet is limited by its nephrotoxicity and need to be administered intravenously. 30 Additionally, maribavir and brincidofovir have failed to significantly reduce CMV infection rates after allo-HSCT.31–33 Given these findings, letermovir remains the preferred agent for CMV prophylaxis in post-HSCT patients owing to its favorable safety and efficacy profile, as supported by most clinical guidelines. However, further studies comparing letermovir with valganciclovir and other antiviral agents are warranted.
This study has certain limitations. First, the retrospective design and small sample size represent significant limitations. Second, the absence of a standardized protocol for discontinuing prophylactic valganciclovir in response to leukopenia, anemia, or thrombocytopenia may account for the higher incidence of thrombocytopenia and lower valganciclovir discontinuation rate in the ultra-low-dose group. Despite these limitations, this study is the first to compare low-dose and ultra-low-dose valganciclovir administration for post-HSCT CMV prophylaxis, providing valuable preliminary data for future research.
Conclusion
Ultra-low-dose valganciclovir is associated with a lower discontinuation rate than low-dose valganciclovir in allo-HSCT; however, it may be associated with a higher rate of CMV reactivation. Its effectiveness in CMV prophylaxis therefore remains uncertain. The higher CMV reactivation rate in the ultra-low-dose group suggests that further dose reduction would reduce its antiviral efficacy in this high-risk population. In addition, unlike findings in solid organ transplantation, reduced dosing was not associated with a decrease in hematologic toxicity following allo-HSCT. These findings suggest that careful, individualized risk–benefit assessment is warranted when considering valganciclovir dose modification for CMV prophylaxis after allo-HSCT.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605261456028 - Supplemental material for Cytomegalovirus prophylaxis using low-dose and ultra-low-dose valganciclovir for patients who have undergone allogeneic hematopoietic stem cell transplantation: A retrospective study
Supplemental material, sj-pdf-1-imr-10.1177_03000605261456028 for Cytomegalovirus prophylaxis using low-dose and ultra-low-dose valganciclovir for patients who have undergone allogeneic hematopoietic stem cell transplantation: A retrospective study by Wei-Hsiang Tseng, Cheng-Hsien Lin, Yu-Chen Su, Ling-Chiao Teng and Chieh‐Lin Jerry Teng in Journal of International Medical Research
Footnotes
Author contributions
Wei-Hsiang Tseng: Conceptualization, Investigation, Formal analysis, and Writing–review & editing. Cheng-Hsien Lin: Conceptualization, Methodology, Investigation, and Writing–review & editing. Yu-Chen Su: Methodology, Investigation, and Writing–review & editing. Ling-Chiao Teng: Conceptualization, Supervision, and Writing–review & editing. Chieh‐Lin Jerry Teng: Conceptualization, Supervision, and Writing–review & editing. All authors gave final approval of the manuscript.
Consent for publication
All authors provided consent for publication.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
Chieh-Lin Jerry Teng received honorarium and consulting fees from Novartis, Roche, Pfizer, Takeda, Johnson and Johnson, Amgen, BMS Celgene, Kirin, and MSD. The other authors have no conflicts of interest.
Ethics approval and consent to participate
Participant details were deidentified, and the study was conducted according to the current version of the Declaration of Helsinki. The Institutional Review Board of Taichung Veterans General Hospital approved the study (CE24388B). The Institutional Review Board of Taichung Veterans General Hospital agreed to waive the requirement for obtaining informed consent from the participants owing to the retrospective nature of the study.
Funding
This study was partially supported by grants from Taichung Veterans General Hospital (TCVGH-1140701C, TCVGH-NHRI113003, and TCVGH-SCCS-SRD113005).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.