
Abstract
Objective
To evaluate the effectiveness of telerehabilitation on pain intensity and functional outcomes in patients with nonoperatively managed tendinopathy compared with home exercise or in-person physical therapy.
Methods
A systematic search of major databases was conducted to identify randomized controlled trials comparing telerehabilitation with home exercise or in-person physical therapy. The primary outcomes were pain intensity and functional recovery. Methodological quality was assessed using the Physiotherapy Evidence Database scale and the Cochrane Risk of Bias tool, whereas the certainty of evidence was evaluated using the Grading of Recommendations Assessment, Development, and Evaluation framework. This review was prospectively registered with International Prospective Register for Systematic Reviews (Registration Number: CRD420251207558).
Results
A total of 10 studies comprising 412 participants were included. Compared with home exercise, telerehabilitation demonstrated a potential advantage in reducing pain (standardized mean difference = 0.99, p < 0.001) and improving functional outcomes (standardized mean difference = 0.52, p < 0.001). Conversely, compared with in-person physical therapy, telerehabilitation showed no statistically significant difference in either pain reduction (standardized mean difference = −0.34, p = 0.49) or functional improvement (standardized mean difference = 0.04, p = 0.76). Sensitivity analyses using the leave-one-out method identified specific outliers contributing to heterogeneity, and the pooled estimates shifted appreciably, indicating limited robustness. The overall certainty of evidence was rated as low to very low because of risk of bias and imprecision.
Conclusions
Telerehabilitation shows potential benefit for patients with tendinopathy, providing clinical outcomes that may be superior to home exercise and comparable to conventional in-person therapy. By facilitating consistent progressive loading through remote supervision, telerehabilitation may serve as a promising option for patients facing barriers to traditional care. However, confidence in these findings remains limited, and the results should be interpreted with caution because of the low certainty of evidence, high risk of bias across most studies, and limited robustness of the pooled estimates. These findings highlight the need for future high-quality, adequately powered trials.
Introduction
Tendinopathy is a prevalent musculoskeletal disorder encompassing a spectrum of overuse injuries affecting tendons such as the rotator cuff, Achilles, patellar, and lateral elbow extensors.1,2 Clinically, it manifests as activity-related pain, focal tenderness, and reduced functional capacity, often resulting in a substantial decline in exercise tolerance and quality of life. 3 The burden of tendinopathy is considerable, affecting a broad population ranging from athletes to the general working population and imposing substantial economic pressure on healthcare systems because of its chronic nature and the need for long-term management.4–6
Clinical guidelines, including those from major orthopedic societies, universally recommend conservative management as the first-line intervention.7,8 Effective nonoperative management encompasses multidimensional strategies such as patient education, activity modification, and the implementation of progressive loading exercises to stimulate tendon remodeling.9–11 However, the successful delivery of these interventions through traditional in-person physical therapy faces significant logistical barriers. Patients frequently encounter challenges such as geographical limitations, particularly in rural areas; scheduling conflicts; financial constraints; and unequal distribution of healthcare resources.12,13 Furthermore, although home exercise programs are a common alternative, they often lack the required supervision and feedback, leading to poor adherence and suboptimal implementation of loading protocols.14,15
In response to these challenges, telerehabilitation has emerged as a promising alternative to traditional in-person rehabilitation. Defined as the provision of rehabilitation services through telecommunication technologies, including synchronous video conferencing, mobile applications, and telephone support, telerehabilitation enables clinicians to bridge geographical barriers. 16 Importantly, this modality offers the distinct advantage of continuous remote supervision. Through approaches such as real-time correction of exercise techniques and app-based biofeedback, telerehabilitation enables patients to perform progressive loading exercises consistently and correctly without the burden of frequent clinic visits. 17
Although telerehabilitation has been extensively studied in the contexts of postoperative recovery 18 and osteoarthritis, 19 its specific efficacy in the nonoperative management of tendinopathy remains incompletely defined. Existing evidence is fragmented, with studies employing highly heterogeneous interventions ranging from simple telephone support to sophisticated digital therapeutics.20,21 Furthermore, it remains unclear whether telerehabilitation is merely superior to home exercise or whether it provides clinical outcomes comparable to those of conventional in-person physical therapy. The diversity in intervention modalities and anatomical sites in the current literature necessitates a unified analysis to better guide clinical practice.
Consequently, a comprehensive systematic review and meta-analysis is warranted to synthesize the current evidence. The primary objective of this study was to evaluate the effectiveness of telerehabilitation on pain intensity and functional outcomes in patients with nonoperatively managed tendinopathy. Particularly, this review aimed to compare telerehabilitation with both conventional in-person physical therapy and home exercise programs. The findings of this analysis may provide valuable insights for clinical decision making and help determine whether digital care models may serve as a viable alternative for tendinopathy management.
Methods
Registration and literature search
We strictly adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement when conducting and reporting this study. 22 The study protocol was prospectively registered with the International Prospective Register for Systematic Reviews (PROSPERO; Registration Number: CRD420251207558). Two independent reviewers (LZ and ZB) conducted a systematic literature search across PubMed, Embase, Scopus, Web of Science, and the Cochrane Library databases from inception through 11 November 2025. In addition, we manually screened the reference lists of relevant reviews to identify additional studies; however, no eligible studies were identified. The search framework was based on two core concepts: (a) telerehabilitation terminology and (b) tendinopathy terminology. To ensure comprehensive retrieval, synonyms within each concept group were combined using the “OR” operator, whereas the two concept groups were linked using the “AND” operator. A complete description of the search strategy is provided in Appendix S1.
Eligibility criteria and study selection
The inclusion criteria were established according to the Participants, Interventions, Comparisons, Outcomes, and Study design (PICOS) framework:
Participants. Individuals aged ≥18 years who were diagnosed with any type of tendinopathy were included. Interventions. The intervention group received telerehabilitation interventions, including mobile applications, video conferencing, telephone support, and related modalities. Comparisons. The control group received either conventional in-person rehabilitation or home-based exercise protocols. We retrieved specific details regarding these protocols from the descriptive data of the included studies. Outcomes. The primary outcomes were pain and functional outcomes. Study design. The included studies were parallel-group randomized controlled trials (RCTs).
We excluded studies that did not include a telerehabilitation component, failed to report quantitative data, or involved surgical procedures such as postsurgical rehabilitation. In addition, conference proceedings, editorials, letters, reviews, and manuscripts without accessible full text were excluded.
Two independent investigators (LZ and YG) conducted the literature screening process in strict accordance with the predefined eligibility criteria. All retrieved records were imported into EndNote X9 for citation management and removal of duplicates. Following deduplication, titles and abstracts were screened to identify potentially relevant studies, followed by a full-text review to determine final eligibility. Any disagreements during the screening process were resolved through discussion, and when consensus could not be reached, a third author (SF) was consulted to make the final decision.
Data extraction
Two reviewers (LZ and ZB) independently conducted data extraction. Any discrepancies were resolved through consultation with a third researcher (SF) to achieve consensus. Extracted data included study characteristics (lead author and year of publication), sample size, participant demographics (e.g. age, sex, and clinical population), intervention protocols (content and duration), and outcome measures.
Quality evaluation and bias risk assessment
Two independent reviewers (SN and YA) assessed the methodological quality and risk of bias of the included studies using the Cochrane Risk of Bias tool (RoB 2.0) and the Physiotherapy Evidence Database (PEDro) scale. Both instruments have established validity for the evaluation of scientific literature.23,24 Final ratings were determined through consensus between the primary reviewers, and any unresolved disagreements were adjudicated by a third senior reviewer (LZ).
Risk of bias in RCTs was assessed using the RoB 2.0 instrument. 25 This tool evaluates five specific domains: bias arising from the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Studies were classified as having a “low risk of bias” only when all five domains satisfied the low-risk criteria. Conversely, studies were categorized as having “some concerns” if concerns were identified in at least one domain, whereas a rating of “high risk of bias” was assigned when high risk was identified in any domain.
The methodological quality of the included studies was further evaluated using the 11-item PEDro scale. This checklist includes eight items related to internal validity and three related to statistical reporting (e.g. between-group comparisons and point estimates of variability). Because the first item, eligibility criteria, pertains to external validity, it is not included in the total score calculation. Consequently, total PEDro scores range from 0 to 10. Trials with scores ≥6 were considered high quality, whereas those with scores <6 were considered to have a greater risk of bias.26,27
Certainty of evidence
The certainty of evidence for each outcome was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework. 28 We systematically evaluated five primary domains: inconsistency, indirectness, risk of bias, publication bias, and imprecision. Based on this assessment, the quality of evidence was categorized into four levels: high, moderate, low, or very low. To summarize these findings, evidence profiles were generated using GRADE Profiler software (version 3.6, GRADEpro).
Statistical analysis
Statistical analyses were performed using Review Manager (RevMan) software (Cochrane Collaboration; Copenhagen, Denmark). Standardized mean differences (SMDs) were calculated for pain-related and functional outcomes by analyzing change scores, defined as the difference between postintervention and baseline means, along with their corresponding SDs across all study groups. Effect sizes were interpreted according to Cohen’s benchmarks, 29 in which an SMD of 0.20 indicates a small effect, 0.50 a moderate effect, and 0.80 a large effect. Heterogeneity among the included trials was evaluated using the I2 statistic. We classified heterogeneity levels as low (25%–50%), moderate (50%–75%), or high (75%–100%). 30 When significant heterogeneity was detected (I2 ≥ 50%), we applied a random-effects model. Conversely, when heterogeneity was low (I2 < 50%), a fixed-effects model was used under the assumption of a common effect size. To identify potential sources of heterogeneity, we conducted sensitivity analyses by sequentially excluding individual studies (leave-one-out method). Assessment of publication bias using funnel plots was not performed because each subgroup analysis included fewer than 10 studies, rendering the method underpowered to distinguish chance findings from true asymmetry.
Results
Study selection
We identified 3031 potential records through searches across databases. After removing 625 duplicates prior to screening, 2406 unique records remained. Subsequently title and abstracts were screened, and 2320 records were excluded, leaving 86 reports for full-text retrieval assessment. Of these, 54 reports could not be retrieved. The majority of unretrieved records comprised clinical trial registrations (e.g. ClinicalTrials.gov entries) and conference abstracts without full published results. We systematically attempted to contact corresponding authors via email to obtain unpublished data or full-text manuscripts; however, no responses or additional data were received. The remaining 32 reports underwent full-text eligibility assessment. Of these, 22 reports were excluded for the following reasons: inappropriate intervention (n = 8), inappropriate study design (n = 13), and non-study disease population (n = 1). Ultimately, 10 studies met all inclusion criteria and were included in the systematic review. The study selection process is illustrated in Figure 1.

Flowchart of the study selection process.
Study quality and risk of bias
As shown in Figure 2, risk of bias assessment across the 10 included studies was conducted using the five RoB 2.0 domains. Regarding the randomization process (D1), six studies were rated as low risk, whereas four studies were judged to have some concerns. For deviations from intended interventions (D2), three studies were rated as high risk and seven as low risk. Regarding outcome measurement (D4), five studies were considered high risk, primarily due to lack of blinding or reliance on subjective outcome assessment. For selection of the reported result (D5), six studies were rated as low risk. Overall, one study was rated as low risk, three as having some concerns, and six as high risk of bias.
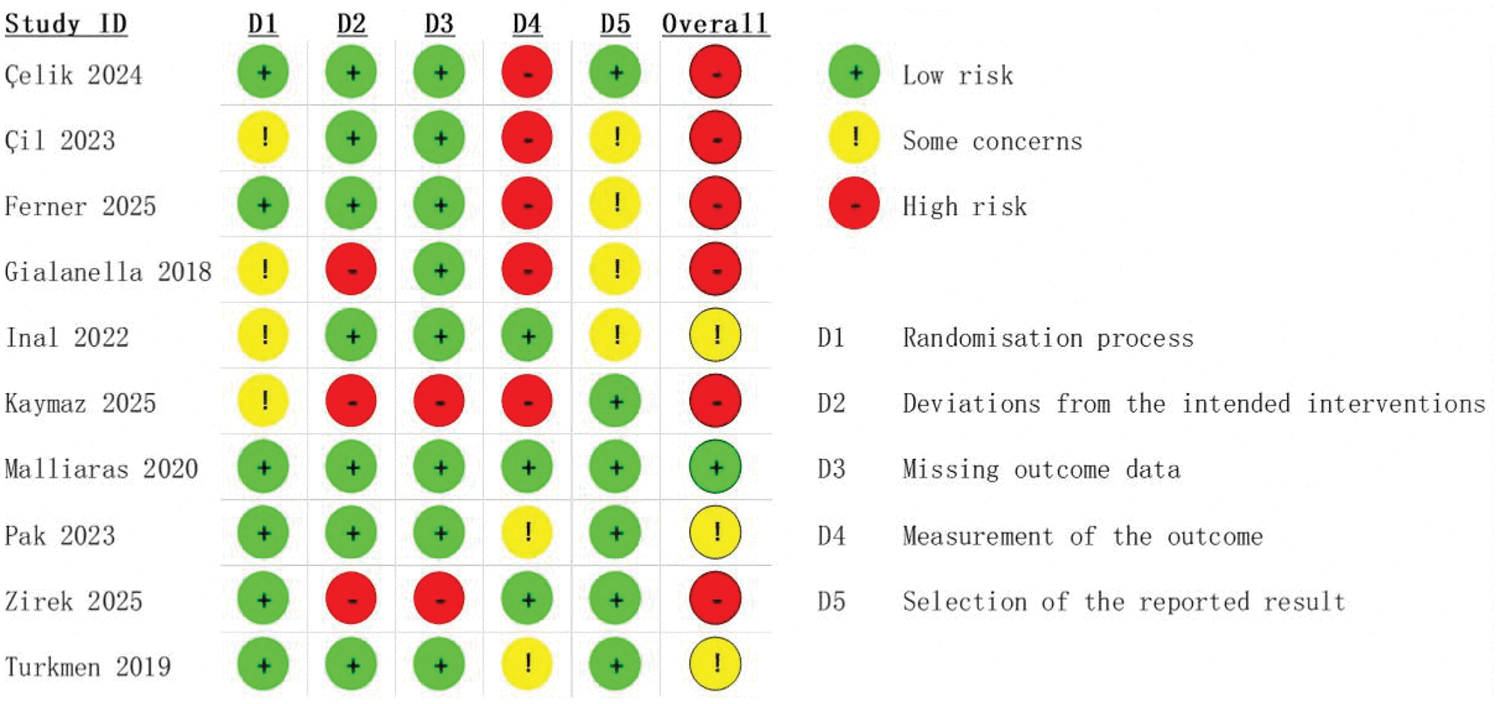
Risk of bias assessment of the included studies.
Table S1 presents the methodological quality assessment of the included studies using the PEDro scale. Total scores ranged from 3 to 8. As most studies scored ≥6, the overall methodological quality was considered moderate to high.
Study characteristics
The 10 included studies comprised a total of 412 participants, with sample sizes ranging from 24 to 82. The studies were conducted in Turkey (n = 6), Italy (n = 1), Australia (n = 1), the USA (n = 1), and Germany (n = 1). The experimental group received telerehabilitation, primarily including video conferencing, telephone support, mobile applications, and related modalities. In contrast, the control group received either home exercise programs or in-person physical therapy. All included RCTs were published in English. Table 1 presents detailed characteristics of the included studies.20,21,31–38
Characteristics of the included studies.

In the study by Pak et al. (2023), one participant in the intervention group did not disclose their sex; hence, actual total of Male + Female = 40 instead of 41.
AT: Achilles tendinopathy; C: control; DASH: disabilities of the arm, shoulder, and hand; I: intervention; LET: lateral epicondyle tendinopathy; M/F: male/female; NPRS: numerical pain rating scale; NR: not reported; PRTEE-T: Turkish version of the patient-rated tennis elbow evaluation; PT: patellar tendinopathy; Quick DASH: quick disabilities of the arm, shoulder, and hand; RC: rotator cuff; rCMS: revised constant total score; SPADI: shoulder pain and disability index; VAS: visual analog scale; VISA-A: Victorian Institute of Sport Assessment–Achilles; VNS: visual numeric scale; WORC: Western Ontario Rotator Cuff Index.
Effects of telerehabilitation on pain
As shown in Figure 3, the intervention effect of telerehabilitation on pain intensity was reported in 9 studies, comprising 188 participants in the experimental group and 190 participants in the control group. Based on the type of comparator, a subgroup analysis classified these nine studies into two groups: those comparing telerehabilitation with home exercise (five studies) and those comparing telerehabilitation with in-person physical therapy (four studies). Using a random-effects model (I2 = 88%, p < 0.001) for pooled analysis, results showed that compared with home exercise, telerehabilitation demonstrated a significant improvement with a large effect size in reducing pain (SMD = 0.99, 95% confidence interval (CI): 0.50–1.47; I2 = 56%, p < 0.001). However, compared with in-person physical therapy (SMD = −0.34, 95% CI: −1.31 to 0.63; I2 = 90%, p = 0.49), no statistically significant difference was observed between groups.
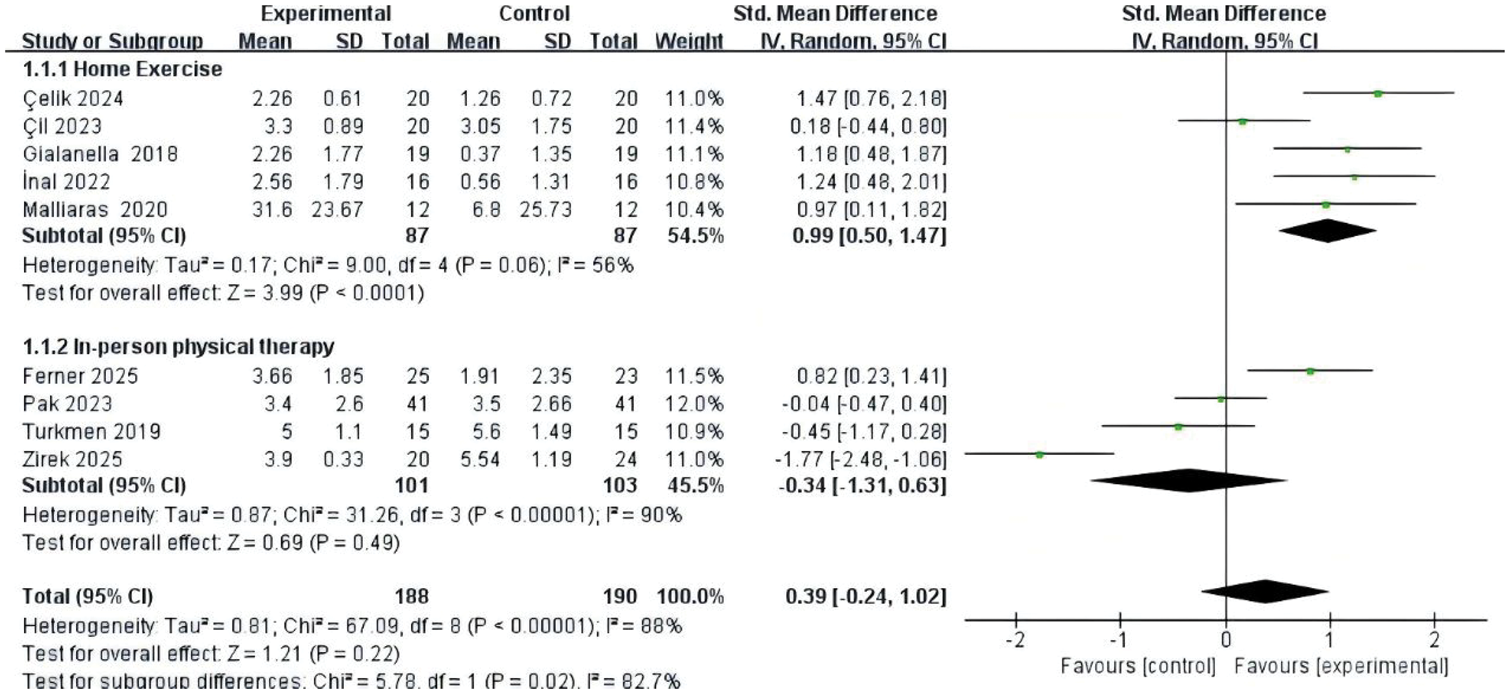
Forest plot for pain outcomes.
Effects of telerehabilitation on functional outcomes
As shown in Figure 4, the intervention effect of telerehabilitation on functional outcomes was reported in 10 studies, comprising 203 participants in the experimental group and 209 participants in the control group. Based on the comparator type, these 10 studies were divided into two subgroups: those comparing telerehabilitation with home exercise (six studies) and those comparing telerehabilitation with in-person physical therapy (four studies). Using a fixed-effects model (I2 = 47%, p = 0.05) for pooled analysis, results indicated that compared with home exercise, telerehabilitation demonstrated a significant improvement with a moderate effect size in functional outcomes (SMD = 0.52, 95% CI: 0.24 to 0.80; I2 = 0%, p < 0.001). However, compared with in-person physical therapy (SMD = 0.04, 95% CI: −0.23 to 0.32; I2 = 60%, p = 0.76), no statistically significant difference was observed between groups.
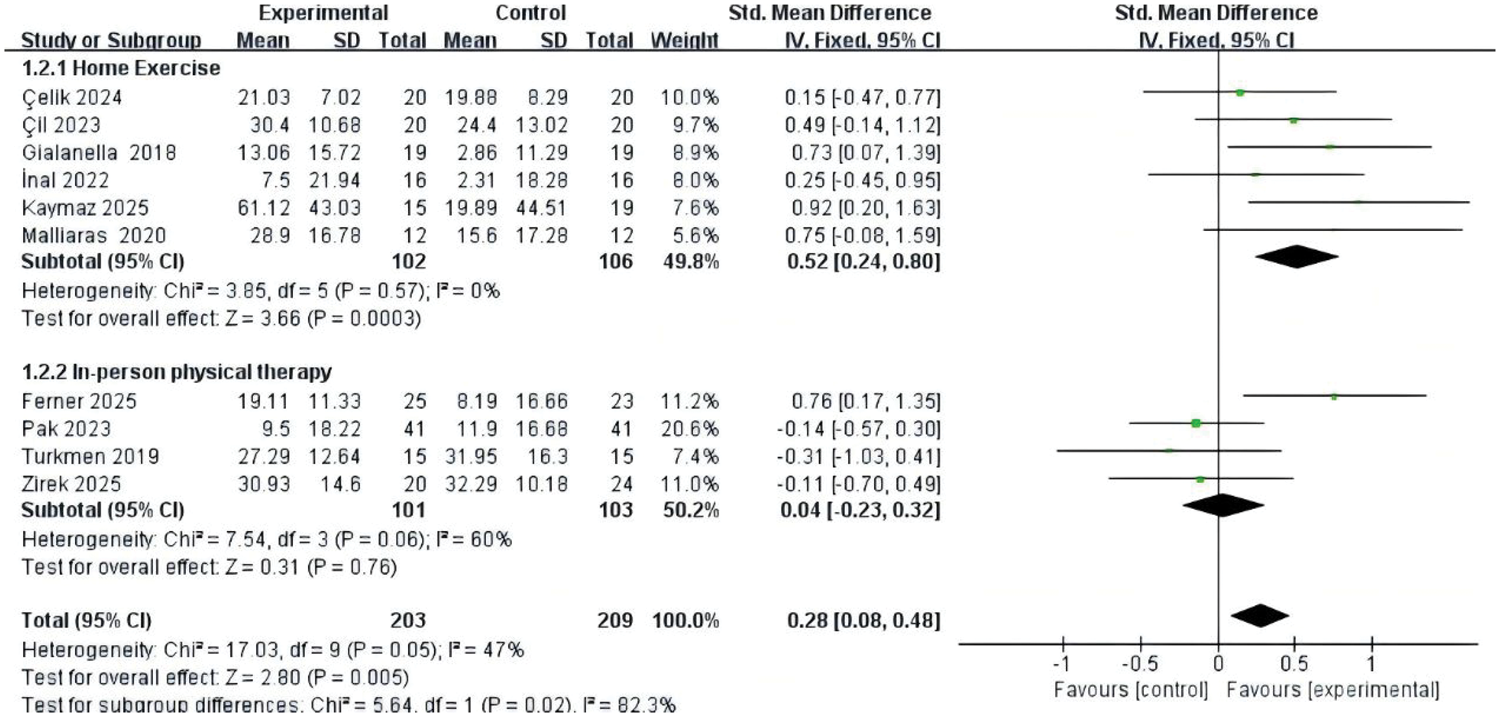
Forest plot for functional outcomes.
Sensitivity analysis
To assess the robustness of the findings and identify potential sources of heterogeneity, a sensitivity analysis was conducted using the leave-one-out method. For pain intensity, the comparison between telerehabilitation and home exercise initially showed moderate heterogeneity (I2 = 56%). This was effectively resolved (I2 = 0%, p = 0.84) after excluding the study by Çil et al. 38 Although statistical significance favoring telerehabilitation was maintained, the substantial change in the pooled effect size (from SMD = 0.99 to SMD = 1.23, 95% CI: 0.86 to 1.61; p < 0.001) indicates that the magnitude of effect is highly dependent on this individual study, suggesting limited robustness. In the comparison with in-person physical therapy, substantial heterogeneity (I2 = 90%) was primarily driven by the studies of Ferner et al. 20 and Zirek et al. 36 Excluding these two studies reduced heterogeneity to 0% (p = 0.34) without changing the nonsignificant between-group difference. However, the notable change in effect size (from SMD = −0.34 to −0.14, 95% CI: −0.52 to 0.23; p = 0.45) further indicates that the pooled estimates are highly sensitive to specific trials and lack stability (Figure S1).
For functional outcomes, the comparison between telerehabilitation and home exercise demonstrated high stability, with no initial heterogeneity observed (I2 = 0%). Leave-one-out analysis confirmed the consistency of these findings, maintaining a significant effect in favor of telerehabilitation. For the comparison with in-person therapy, the initial moderate heterogeneity (I2 = 60%) was eliminated (I2 = 0%) after excluding the study by Ferner et al. The re-calculated effect size remained statistically nonsignificant (SMD = −0.16, 95% CI: −0.48 to 0.15; p = 0.31). However, the change in effect size (from SMD = 0.04 to −0.16) indicates that the pooled estimate is sensitive to this individual trial, suggesting limited robustness in supporting comparable functional recovery (Figure S2).
GRADE certainty of evidence
GRADE evidence profiles for all outcomes are presented in Table S2. According to the GRADE assessment, the certainty of evidence for all outcomes was rated as low or very low. These ratings were primarily downgraded due to high risk of bias (particularly deviations from intended interventions and outcome measurement), inconsistency (with heterogeneity I2 reaching 90% in comparisons with in-person therapy), and imprecision due to small sample sizes. Although telerehabilitation demonstrated statistically significant improvements in pain and functional outcomes compared with home exercise, the certainty of this evidence was limited by methodological limitations. In contrast, comparisons with in-person physical therapy showed no significant differences for either outcome and were characterized by inconsistent effect estimates. Overall, these limitations indicate that the current evidence base is uncertain, highlighting the need for higher-quality, adequately powered trials to strengthen future conclusions.
Discussion
This meta-analysis suggests a potential benefit of telerehabilitation in the management of tendinopathy, indicating more favorable outcomes compared with home exercise programs in both pain relief and functional recovery, achieving results comparable to conventional in-person physical therapy. Particularly, our findings demonstrated that telerehabilitation yielded a large effect size in reducing pain intensity (SMD = 0.99; 95% CI: 0.50 to 1.47) and a moderate effect size in improving functional outcomes (SMD = 0.52; 95% CI: 0.24 to 0.80) compared with the home exercise control group. However, when compared with in-person physical therapy, telerehabilitation showed no statistically significant difference in either pain reduction (SMD = −0.34) or functional improvement (SMD = 0.04). According to the GRADE assessment, the certainty of evidence for these outcomes ranged from low to very low, primarily due to high heterogeneity, small sample sizes across included studies, and high risk of bias in most studies (largely driven by the inherent lack of blinding in rehabilitation trials) as well as the extreme sensitivity of pooled estimates to individual trials. Consequently, confidence in these findings is limited, and they should be interpreted with caution.
Our results demonstrating the superiority of telerehabilitation over self-managed home exercise are consistent with previous meta-analyses in other chronic conditions. For instance, Bonnevie et al. 39 reported that advanced telehealth technology exercise therapy (ATT-ET) yielded superior outcomes in objective physical activity and quality of life compared with home-based exercise therapy without ATT. Similarly, Lin et al. 40 found that telerehabilitation significantly reduced pain and improved range of motion in nonoperative shoulder conditions compared with home-based conventional therapy. A possible mechanism for this superiority lies in remote supervision and feedback, which are often absent in standard home exercise programs.41,42 In the included studies, control groups typically received static home programs, often delivered via printed materials or verbal instructions. In contrast, telerehabilitation interventions provided structured guidance. For instance, Malliaras et al. 34 used real-time video conferencing to correct exercise techniques, whereas Pak et al. 35 employed an app with sensor-based biofeedback to ensure movement quality. This “guided self-management” approach ensures that progressive loading, crucial for tendon remodeling, is performed consistently and correctly, thereby maximizing clinical benefits compared with independent exercise.
Furthermore, our analysis confirms that telerehabilitation serves as an effective alternative to in-person physical therapy, yielding comparable clinical outcomes. This is consistent with the findings of Suso-Martí et al., 43 whose umbrella review and meta-meta-analysis concluded that telerehabilitation offers comparable physical function outcomes to conventional in-person rehabilitation for musculoskeletal conditions, and Zou et al., 44 who reported that telerehabilitation for nonspecific neck pain resulted in similar pain reduction compared with conventional care. This similarity suggests that the critical factor for tendinopathy recovery is the content of the rehabilitation protocol (e.g. progressive loading) rather than the mode of delivery. Evidence from the included studies supports this interpretation. For instance, Pak et al. 35 used motion-tracking sensors to provide real-time biofeedback, allowing patients with shoulder pain to self-correct movements without direct therapist supervision. Similarly, Turkmen et al. 37 demonstrated that a video-based rehabilitation program was as effective as a physiotherapist-supervised program in improving shoulder function and quality of life in patients with rotator cuff tears. These findings suggest that telerehabilitation technologies can effectively replicate key supervisory components of in-person care, thereby enabling patients to manage chronic symptoms independently and reducing the logistical burden of frequent clinic visits. 45
Further exploration reveals that intervention characteristics, particularly duration and delivery modality, play a pivotal role in the observed heterogeneity. Regarding the comparison with home exercise, sensitivity analysis identified Çil et al. 38 as a source of heterogeneity. Unlike other included trials, such as Inal et al., 21 which reported large effect sizes for pain reduction, this study observed a more modest benefit. A key factor likely contributing to this discrepancy is the mode of delivery: Çil et al. 38 employed a web-based asynchronous system in which patients logged in to view videos at their own pace. The lack of active human “coaching” or real-time supervision in this passive asynchronous model may have resulted in lower adherence or engagement compared with interventions involving synchronous, direct therapist contact (as seen in Inal et al.). 21 The accountability provided by human interaction appears to be a crucial driver of efficacy when the digital platform lacks advanced interactive features. 46 In the comparison with in-person therapy, sensitivity analysis identified Ferner et al. 20 as the primary source of heterogeneity. This divergence is likely driven by differences in intervention duration and modality. Ferner et al. 20 employed a 90-day digital therapeutic application, which was substantially longer than the intervention periods in other included studies. The superior outcomes suggest that structured, asynchronous applications with extended durations may be particularly effective in fostering long-term self-management and progressive loading, key components of tendinopathy recovery that are highly amenable to remote delivery. 47 This contrasts with synchronous video conferencing or simple video-instruction models used in other studies. 36 Unlike episodic interventions, which are constrained by appointment availability, app-based approaches allow for continuous adherence monitoring and algorithmic adjustments to exercise intensity, ensuring that the loading stimulus remains optimal throughout rehabilitation. 20
Telerehabilitation appears to offer a promising alternative to traditional in-person rehabilitation or home-based therapy for patients with nonoperatively managed tendinopathy. First, the observed clinical advantage of telerehabilitation over independent home exercise suggests a potential role for remote supervision in conservative management. Although standard home exercise programs are frequently used as low-cost interventions, our analysis suggests they often result in suboptimal outcomes in pain relief and functional recovery due to a lack of professional guidance. 48 Telerehabilitation effectively addresses this supervisory gap by providing structured monitoring and feedback, ensuring that progressive loading protocols, crucial for tendon remodeling, are executed with the necessary precision and consistency. Furthermore, the comparable efficacy of telerehabilitation relative to in-person physical therapy suggests it may be considered a potential standalone option, particularly when patients are unable to attend physical therapy sessions due to logistical constraints. By shifting the center of care from the clinic to the patient’s home, this modality overcomes barriers such as geographical isolation, financial limitations, and time constraints without compromising quality of care. The feasibility of this approach is reinforced by the successful implementation of “self-manual therapy” in Çelik et al. 31 and app-guided biofeedback in Pak et al., 35 demonstrating that even complex rehabilitation tasks can be effectively managed remotely when supported by appropriate technology. From a health policy perspective, integrating telerehabilitation into routine care pathways offers a strategic avenue for optimizing resource allocation. The broad spectrum of effective delivery methods identified in this review, ranging from simple telephone coaching 21 to advanced digital therapeutics, 20 enables clinicians to tailor interventions according to patient needs and available infrastructure. We propose a stratified care model in which telerehabilitation is used to enhance the standard of care for patients who would otherwise receive only static home exercise instructions and also served as a primary alternative for those unable to access traditional clinics.
Limitation
Despite the promising findings, this review is subject to several limitations. First, considerable statistical heterogeneity was observed in some comparisons. Although sensitivity analyses identified specific outliers, the limited number of included trials precluded formal meta-regression and subgroup analyses (by tendinopathy type, delivery modality, synchronicity, or intervention duration) to fully explore clinical heterogeneity arising from diverse interventions and anatomical sites. This ultimately necessitates cautious interpretation of the pooled effect estimates. Second, sample sizes in the included RCTs were generally small, with most experimental groups containing fewer than 20 participants. This limited sample size may reduce statistical power and the precision of effect estimates. Third, the majority of included studies focused on rotator cuff tendinopathy, which may limit the generalizability of findings to other tendon types, such as elbow or Achilles tendinopathy. Fourth, sensitivity analyses indicated that pooled effect sizes were appreciably influenced by individual studies. Although the direction of effects remained qualitatively stable across leave-one-out iterations, the magnitude of SMDs changed substantially when specific trials were excluded (e.g. from 0.99 to 1.23 for pain in the home exercise comparison and from −0.34 to −0.14 in the in-person therapy comparison). These variations underscore that the current summary estimates lack robust stability and should be interpreted with caution. Finally, as highlighted in the GRADE assessment, the certainty of evidence for primary outcomes ranged from low to very low. This was largely driven by high risk of bias across several domains, particularly the lack of blinding of participants and therapists, an inherent challenge in rehabilitation trials. Furthermore, publication bias cannot be excluded given potential small-study effects, the limited number of included trials, and the unretrieved reports.
Conclusion
This meta-analysis suggests that telerehabilitation may offer potential benefits for patients with nonoperatively managed tendinopathy, with pooled estimates indicating possible advantages over home exercise in reducing pain intensity and improving functional outcomes. Furthermore, telerehabilitation may provide clinical efficacy comparable to conventional in-person physical therapy, suggesting it could serve as a promising option for patients facing barriers to traditional care. However, confidence in these findings is limited, with the certainty of evidence remaining low to very low due to substantial heterogeneity, small sample sizes, risk of bias, and the high sensitivity of pooled estimates to individual studies. Therefore, although these findings highlight the potential of digital care models, future high-quality RCTs with adequate power and standardized protocols are necessary to robustly confirm these conclusions.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605261456510 - Supplemental material for Effectiveness of telerehabilitation versus home exercise and in-person therapy for nonoperatively managed tendinopathy: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605261456510 for Effectiveness of telerehabilitation versus home exercise and in-person therapy for nonoperatively managed tendinopathy: A systematic review and meta-analysis by Shijie Fan, Sehrish Noor, Yuvathi Arunkumar, Zhaodong Bi, Yongle Guo and Longguo Zhang in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605261456510 - Supplemental material for Effectiveness of telerehabilitation versus home exercise and in-person therapy for nonoperatively managed tendinopathy: A systematic review and meta-analysis
Supplemental material, sj-pdf-2-imr-10.1177_03000605261456510 for Effectiveness of telerehabilitation versus home exercise and in-person therapy for nonoperatively managed tendinopathy: A systematic review and meta-analysis by Shijie Fan, Sehrish Noor, Yuvathi Arunkumar, Zhaodong Bi, Yongle Guo and Longguo Zhang in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_03000605261456510 - Supplemental material for Effectiveness of telerehabilitation versus home exercise and in-person therapy for nonoperatively managed tendinopathy: A systematic review and meta-analysis
Supplemental material, sj-pdf-3-imr-10.1177_03000605261456510 for Effectiveness of telerehabilitation versus home exercise and in-person therapy for nonoperatively managed tendinopathy: A systematic review and meta-analysis by Shijie Fan, Sehrish Noor, Yuvathi Arunkumar, Zhaodong Bi, Yongle Guo and Longguo Zhang in Journal of International Medical Research
Supplemental Material
sj-pdf-4-imr-10.1177_03000605261456510 - Supplemental material for Effectiveness of telerehabilitation versus home exercise and in-person therapy for nonoperatively managed tendinopathy: A systematic review and meta-analysis
Supplemental material, sj-pdf-4-imr-10.1177_03000605261456510 for Effectiveness of telerehabilitation versus home exercise and in-person therapy for nonoperatively managed tendinopathy: A systematic review and meta-analysis by Shijie Fan, Sehrish Noor, Yuvathi Arunkumar, Zhaodong Bi, Yongle Guo and Longguo Zhang in Journal of International Medical Research
Supplemental Material
sj-pdf-5-imr-10.1177_03000605261456510 - Supplemental material for Effectiveness of telerehabilitation versus home exercise and in-person therapy for nonoperatively managed tendinopathy: A systematic review and meta-analysis
Supplemental material, sj-pdf-5-imr-10.1177_03000605261456510 for Effectiveness of telerehabilitation versus home exercise and in-person therapy for nonoperatively managed tendinopathy: A systematic review and meta-analysis by Shijie Fan, Sehrish Noor, Yuvathi Arunkumar, Zhaodong Bi, Yongle Guo and Longguo Zhang in Journal of International Medical Research
Footnotes
Acknowledgments
Not applicable.
Author contributions
Longguo Zhang and Shijie Fan contributed to study conception and design. Longguo Zhang, Sehrish Noor, Yuvathi Arunkumar, Zhaodong Bi, and Yongle Guo performed data collection and statistical analysis. Longguo Zhang, Shijie Fan, and Sehrish Noor critically revised the manuscript. Shijie Fan supervised the project and approved the final version. All authors read and approved the final manuscript.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Data availability statement
All relevant data have been provided in the manuscript. Supplementary datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
Not applicable.
Funding
None.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.