
Abstract
Intracapsular hemorrhage occurs occasionally in acute pancreatitis complicated with pseudocyst that can be managed using laparoscopic gastric cyst anastomosis and drainage. However, cyst recurrence many years later and secondary splenic artery pseudoaneurysm rupture and hemorrhage leading to bloody vomiting and syncope are uncommonly reported. A woman in her late 40s was admitted for bloody vomiting, melena, anemia, and syncope. She underwent laparoscopic gastric cyst anastomosis and drainage for severe acute pancreatitis 3 years ago. Gastroscopy identified a bleeding gastric vascular malformation. Metal clips were used for endoscopic hemostasis. Abdominal enhanced computed tomography revealed a cystic lesion in the tail of the pancreas (4.2 × 3.9 cm) connected with the stomach wall and a splenic artery pseudoaneurysm in the cyst. Splenic artery pseudoaneurysm embolization was performed. The patient remains asymptomatic 2 years after embolization. Percutaneous selective embolization of a splenic artery pseudoaneurysm may be the preferred choice for patients with a pancreatic pseudocyst complicated by rupture and hemorrhage of the splenic artery pseudoaneurysm in the pancreatic pseudocyst. Clinicians should be alert regarding the possibility of recurrence after prior drainage, highlighting the importance of long-term follow-up.
Keywords
Introduction
Pancreatic pseudocyst (PPC) secondary to acute or chronic pancreatitis or pancreatic injury contains a large amount of pancreatic secretion that has leaked from the pancreatic ductal system.1,2 PPC is a self-limiting disease that can resolve on its own; however, treatment is required for symptomatic cases. The standard treatments include pharmacologic conservative treatment, internal drainage, external drainage, and cystectomy. 3 Pancreatic pseudoaneurysm (PA) is a rare but potentially life-threatening complication of acute and chronic pancreatitis, often associated with PPC. It arises when PPCs containing enzyme-rich fluid collections erode into adjacent blood vessels, most commonly the splenic artery, leading to the formation of a pseudoaneurysm.4–6 The present study reports a rare case of gastrointestinal hemorrhage caused by rupture of a splenic artery PA within a PPC 3 years after laparoscopic internal drainage of the PPC.
Case presentation
The reporting of this study conforms to the Case Report (CARE) guidelines. 7 Written informed consent to treatment was obtained from the patient. All patient details have been de-identified.
A woman in her late 40s was admitted to The Third People's Hospital of Datong (Datong, Shanxi, China) in March 2023 for intermittent blood vomiting and black stools for 6 days, accompanied with syncope. She had successfully undergone a laparoscopic cholecystectomy and PPC internal drainage 3 years ago at another hospital. The patient has no history of alcohol consumption, hypertension, or coagulation disorders.
Regarding patient history and previous interventions, in 2020, the patient was admitted to a local hospital for biliary severe acute pancreatitis, PPC, and cholelithiasis. A laparoscopic cholecystectomy combined with internal drainage of the pancreatic cyst had been performed. Intraoperative findings revealed a 7 × 8-cm cystic mass at the tail of the pancreas, with the anterior wall of the cyst densely adhering to the posterior wall of the stomach. The anterior gastric wall was incised to facilitate drainage, and a cystogastric anastomosis was created at the point of closest apposition between the posterior gastric wall and pancreatic cyst. The junction between the gastric and cystic walls was reinforced using interrupted sutures. Old blood clots were observed within the cyst; these were thoroughly cleared, and Gelfoam was applied to the internal cystic surface to achieve hemostasis. The procedure was completed successfully with minimal blood loss. The patient recovered well postoperatively with no significant discomfort. Follow-up abdominal computed tomography (CT) performed at the external hospital 3 months later indicated that the original PPC had significantly decreased in size (approximately 3 × 4 cm) and that there were no signs of pancreatitis. No further diagnostic or therapeutic interventions were pursued at that time.
Following surgical treatment for the PPC, the patient experienced no recurrence of pancreatitis. The index admission was prompted by a sudden hemorrhage accompanied with syncope. Prior to this admission, the patient reported no symptoms of pancreatitis, such as abdominal pain or distension. Six days before admission, the patient had unexplained melena accompanied with dizziness and syncope. One day before her admission, the patient suffered from dizziness and syncope again, accompanied with bright red bloody vomiting without chest pain, shortness of breath, jaundice, fever, or other discomforts. Upon admission, her heart rate was 84 b/min, and blood pressure was 105/63 mmHg. Her white blood cell (WBC) count was 9.58 × 109/L, neutrophil percentage was 89.0%, hemoglobin level was 76.0 g/L (indicating anemia), platelet count was 229.0 × 109/L, and the vomitus occult blood test was positive. Abdominal color Doppler ultrasound showed gastrointestinal flatulence. Following admission, the patient reported dizziness. Symptomatic treatments were administered, including continuous oxygen therapy, acid suppression (proton pump inhibitors), hemostasis (anti-hemorrhagic agents), and fluid replacement therapy. Prior to the endoscopic evaluation, several differential diagnoses, including gastric fundal varices and peptic ulcer disease, were considered. However, these were ruled out following gastroscopy performed after admission. Gastroscopy on the second day showed linear scars on the anterior wall of the upper part of the gastric body, and the mucosa of the posterior wall of the greater curvature of the upper part of the gastric body was edematous and elevated, with central reddening and bleeding. Endoscopic ultrasonography (EUS) showed mucous and muscle layers thickening in the upper and posterior wall of the gastric body, while the rest of the gastric wall structure was normal. The initial endoscopic diagnosis was vascular malformation with bleeding (Dieulafoy's lesion) in the upper posterior wall of the gastric body, and the bleeding point of the gastric body was closed using three hemoclips (Figure 1) to manage the bleeding. This diagnosis was based on the local endoscopic appearance but was later found to be misleading as it represented secondary mucosal changes due to rupture of an adjacent splenic artery pseudoaneurysm, representing a classic diagnostic pitfall.
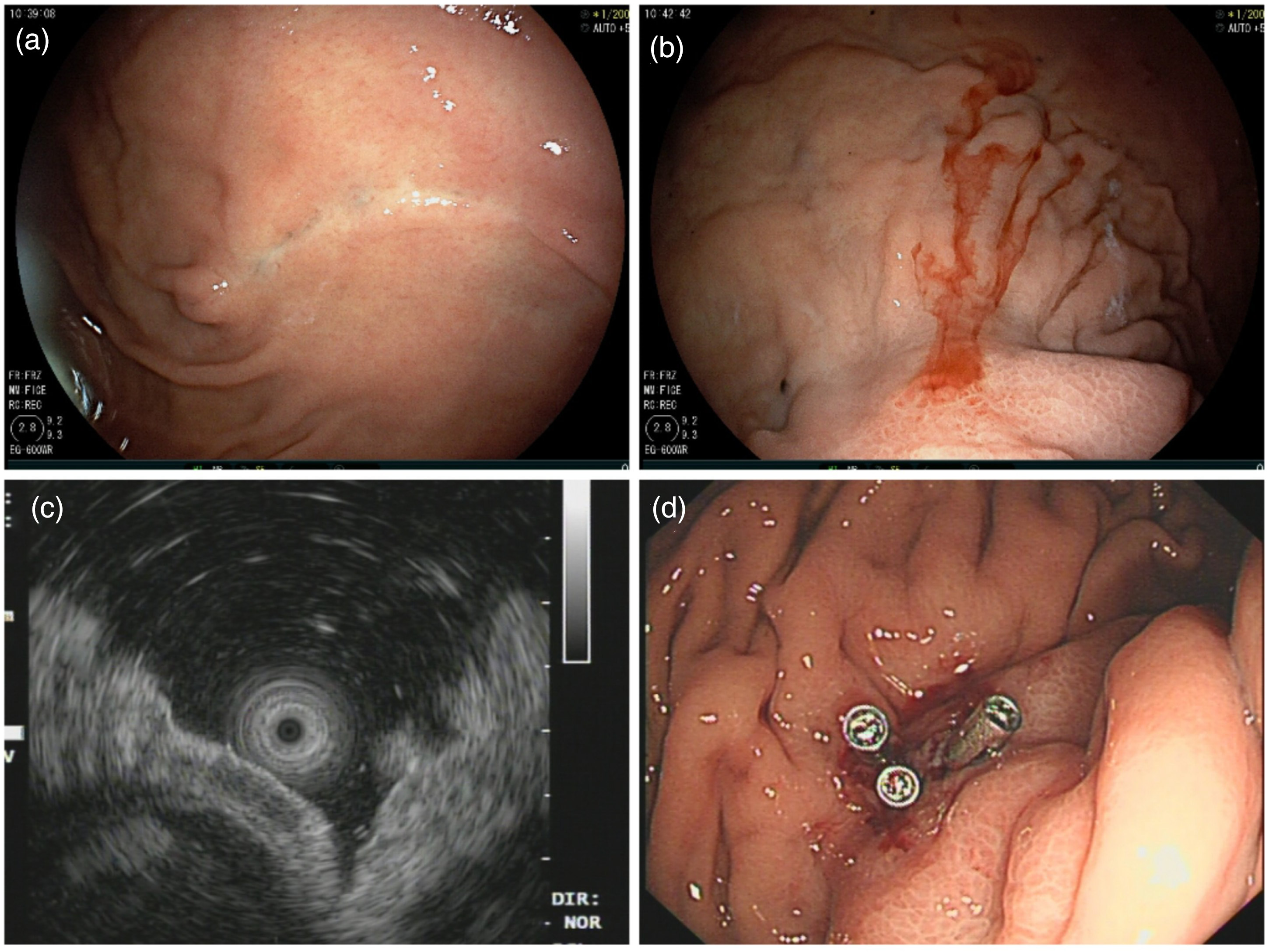
Endoscopic view. (a) Linear scar on the anterior wall of the upper part of the gastric body. (b) Edema and elevation of the lateral mucosa of the posterior wall of the upper greater curvature of the gastric body, with central reddening and fresh bleeding. (c) Thickening of the mucous and muscular layers of the mucous membrane at the elevation of the posterior wall of the upper part of the gastric body, as seen using a small intragastric ultrasound probe. (d) Metal clip closure of the gastric body at the bleeding point.
Considering the history of PPC, the possibility that the bleeding event was related to the original PPC and surgery could not be excluded. Contrast-enhanced abdominal CT revealed a lesion in the tail of the pancreas connected to the gastric wall, consistent with a PPC. Within the pseudocyst, a splenic artery pseudoaneurysm was strongly suspected. Other findings included post-cholecystectomy changes, bilateral renal cysts, a cystic lesion in the right iliac fossa, possibly a lymphangioma, a small amount of pelvic effusion, hemoclips on the greater curvature of the gastric body (post-procedural changes), and significant high-density material in the colon (possible post-surgical changes), suggesting PPC recurrence and PA (Figure 2(a) to (d)). On day 6, a consultation was held with the Department of Hepatobiliary Surgery. The assessment concluded that the PPC, measuring approximately 4 cm, did not currently meet the criteria for surgical indications. A referral to the Interventional Radiology department was recommended for the management of the splenic artery pseudoaneurysm. Over the first 8 days of hospitalization, her hemoglobin levels fluctuated from 71 to 81 g/L. During this hospitalization, the patient's vital signs remained relatively stable, and no blood transfusion was performed.

Enhanced abdominal computed tomography and follow-up abdominal computed tomography 3 months after discharge. (a) A metal-like hyperdense shadow is visible in the stomach. (b–c) A splenic artery pseudoaneurysm is present within a pseudocyst cavity in the tail of the pancreas (approximately 4.2 × 3.9 cm), communicating with the gastric wall and demonstrating moderate enhancement of the wall thinness. (d) The splenic artery is partially involved in the lesion and demonstrates localized enlargement. (e) The metal clips visible in the stomach. (f) The splenic artery pseudoaneurysm within the pseudocyst cavity in the tail of the pancreas connected to the gastric wall, reduced in size compared with that during the previous examination. (g–h) Dense clips visible along the course of the splenic artery, and radial artifacts observed in the surrounding area.
Interventional embolization was performed on day 11 after admission. Intraoperatively, an irregular cord-like enlargement was seen 3 cm from the beginning of the splenic artery, and the distal branches were normal, consistent with a splenic artery pseudoaneurysm. The coaxial microcatheter technique was used to superselect the distal part of the splenic artery pseudoaneurysm, and two spring coils (10 × 30 mm and 8 × 20 mm, Boston Scientific Corporation) were released. The microcatheter was placed in the aneurysm, and 7 spring coils (2 × 5 mm, Boston Scientific Corporation) were released. The microcatheter was placed in the proximal part of the aneurysm, and 1 spring coil (6 × 20 mm, Boston Scientific Corporation) was released. Repeat angiography revealed preservation of the main trunk of the splenic artery, with no demonstration of the aneurysm or distal end (Figure 3). Postoperatively, the patient recovered well without complications and was discharged 5 days later.
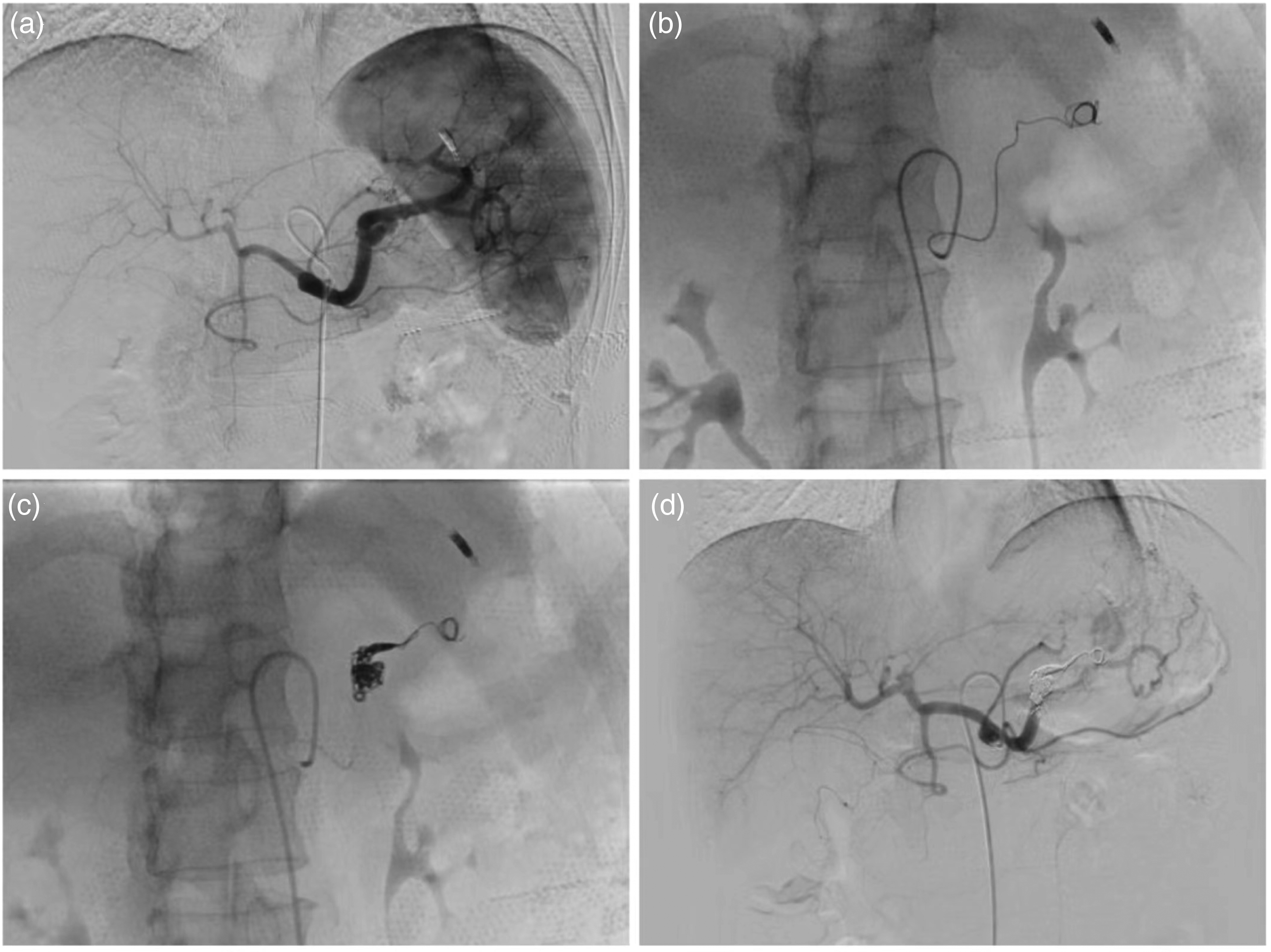
Percutaneous selective abdominal angiography and splenic artery pseudoaneurysm embolization. (a) A splenic artery pseudoaneurysm visible on abdominal angiography. (b) Splenic artery pseudoaneurysm distal to the release of the spring coil. (c) Splenic artery pseudoaneurysm and its proximal release of the spring coil. (d) Reimaging of the distal splenic artery trunk occlusion demonstrates splenic artery pseudoaneurysm tamponade and a small, residual collateral supply to the spleen.
After 3 months of follow-up, the patient's hemoglobin level normalized. She remained in good general condition following the interventional embolization therapy. There was no recurrence of gastrointestinal bleeding symptoms, such as hematemesis or melena, and the patient reported no abdominal pain or fever. Based on the clinical presentation, post-interventional complications, specifically splenic infarction or abscess, were ruled out. Abdominal CT showed the metal clips in the stomach, a cystic lesion (2.4 × 2.0 cm) in the tail of the pancreas communicating with the gastric wall, with a thickened wall demonstrating moderate enhancement and no enhancement within the capsule, as well as splenic artery coils (Figure 2(e) to (h)). CT also confirmed the absence of complications. In May 2025, the patient had been followed up for 2 years, and no discomfort had been reported. The comprehensive clinical course, including prior interventions, recurrence, and current treatment, is summarized in the timeline shown in Figure 4.
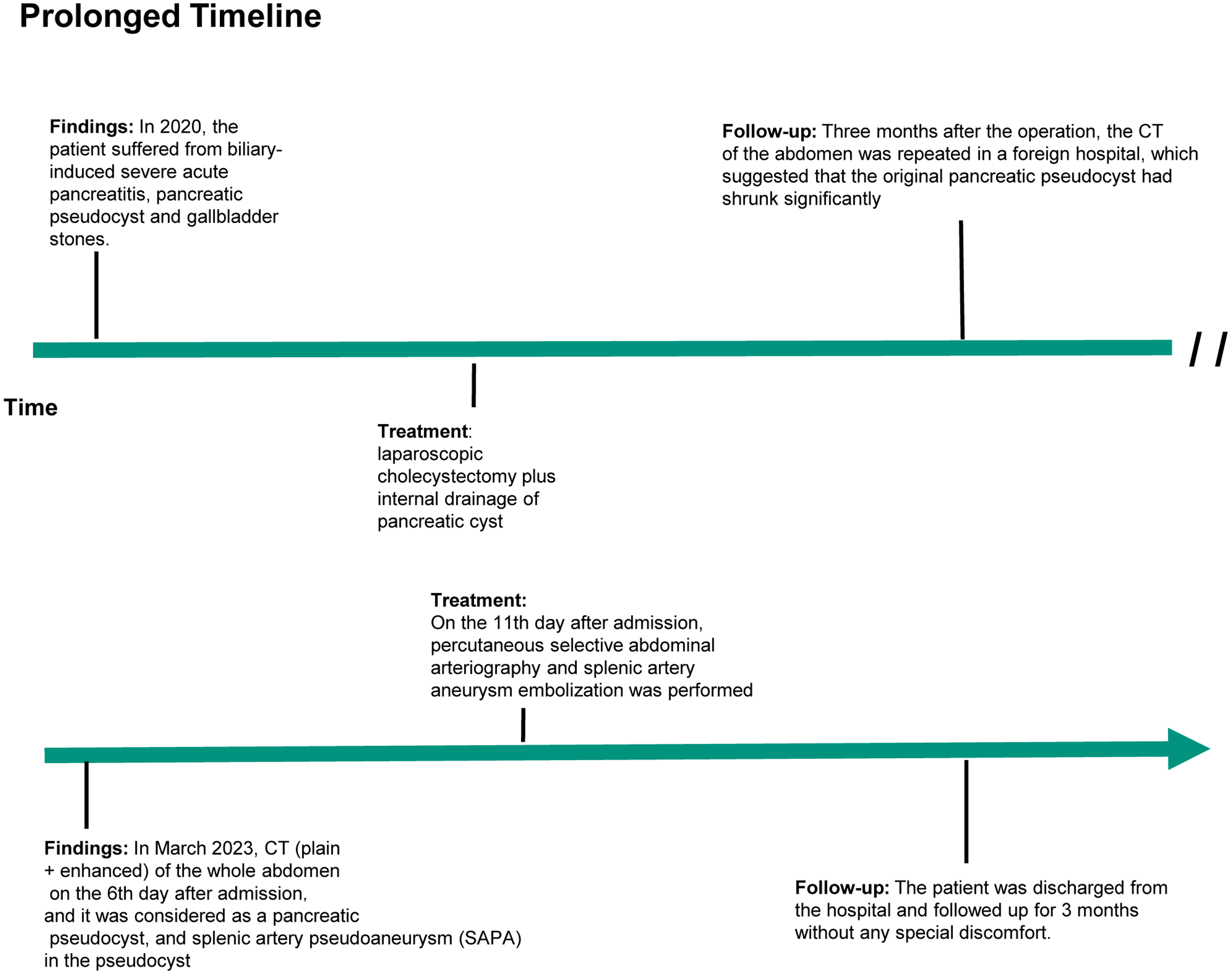
Timeline of the patient's clinical history and therapeutic interventions.
Discussion
The patient in this report experienced severe acute pancreatitis of biliary origin 3 years before the index admission, leading to a PPC that was treated with laparoscopic cholecystectomy and pancreatic cyst internal drainage at another hospital; the 3-month postoperative review demonstrated a shrunken PPC. For the index admission, the patient was admitted as an emergency case of upper gastrointestinal hemorrhage with melena, blood vomiting, and syncope. Anemia was confirmed after admission. Gastroscopy showed that the mucosa of the upper posterior wall of the gastric body was swollen with localized blood seepage. Endoscopic metal clip hemostasis was performed. CT and angiography revealed splenic artery PA, which was managed using coils. The patient remained asymptomatic for at least 2 years.
Acute pancreatitis is often accompanied with PPC, which can lead to corrosion of the blood vessel wall and PA formation.8,9 PA formation can also be associated with arterial blood pressure. PA often involves the splenic, gastroduodenal, pancreaticoduodenal, right gastric, left gastric, gastric, omental, and gallbladder arteries,4,10–13 with vein involvement also reported. 14 Due to their thin and fragile wall, PAs are highly prone to rupture and potentially life-threatening hemorrhage.15,16
The patient had undergone internal drainage of PPC 3 years prior. The cyst had shrunk in the 3-month postoperative review; however, no further follow-up had been performed. The PPC recurrence in this case may be related to gradual closure of the cyst-gastrostomy over time leading to poor pancreatic juice drainage; however, this conclusive remains speculative. Under the long-term erosion effect of the pancreatic fluid in the PPC, the wall of the adjacent splenic artery thinned to form a PA, which ruptured into the cyst, leading to a sharp increase in pressure within the cyst and gastrointestinal bleeding after blood and pancreatic fluid leaked from the cyst into the gastric cavity. However, pancreatic duct imaging (e.g. MRCP/ERCP) was unavailable; therefore, persistent ductal disruption or chronic pancreatitis could not be confirmed. Therefore, alternative explanations for recurrence include de novo splenic artery pseudoaneurysm formation, subclinical ductal leak, and post-surgical vascular vulnerability.
Regarding follow-up strategies after PPC drainage, this case highlights the importance of long-term monitoring. The patient underwent only one CT scan 3 months postoperatively, with no further surveillance for 3 years until the major hemorrhage occurred. Although cyst shrinkage is generally a positive sign, relying on size reduction alone may be insufficient to assess long-term risks, particularly in patients at risk of vascular erosion. Individualized long-term follow-up plans, potentially including periodic imaging, should be considered for patients who have undergone pseudocyst drainage, especially those with a complex initial etiology, large cysts, or risk factors for persistent ductal abnormalities, to monitor for recurrence or complications.
Endoscopic clipping serves as a delaying and diagnostic measure that can stop blood from leaking into the gastric lumen and may help stabilize the patient and preliminarily localize the bleeding site while awaiting definitive therapy. However, it is a short-term management method as the cyst may rupture. The pseudocyst wall is often thin and friable, making it difficult to achieve durable hemostasis using clips alone. Recurrent bleeding is common because the clip may dislodge or fail to occlude the entire vessel, especially if the rupture site is deep or obscured by ongoing hemorrhage.17,18 Endoscopic clips are designed for superficial mucosal or submucosal lesions, such as ulcers or diverticula, where the bleeding source is accessible and localized. In vascular pseudocyst rupture, the bleeding originates from a large, pulsatile artery, often behind or within the pseudocyst wall. Clips cannot reliably compress or occlude such high-flow arterial sources, and the risk of rebleeding is substantial. Additionally, the pseudocyst itself may continue to erode adjacent vessels, leading to further hemorrhage after initial endoscopic control.17,19 Definitive management of vascular pseudocyst rupture usually requires a combination of endoscopic, radiological, and surgical interventions. Endovascular embolization is often necessary to occlude the bleeding artery, while surgical resection may be required in case of extensive vascular destruction or embolization failure. Endoscopy can serve as a temporizing measure to stabilize the patient and localize the bleeding site; however, it is inadequate for long-term control. The use of clips may also help mark the site for subsequent interventions; however, they do not eliminate the need for definitive vascular control. 17 In this case, the absence of rebleeding after clipping demonstrated its role as a short-term measure; however, definitive treatment required endovascular embolization. Therefore, the patient underwent splenic artery embolization to eliminate the rebleeding risk.
Dual embolization of the proximal and distal portions of the aneurysm-bearing splenic artery is necessary and effective. After main splenic artery occlusion, the spleen can receive partial blood supply from collateral branches such as the short gastric artery, preventing splenic infarction. If only the proximal splenic artery is embolized at this time, the splenic artery PA may receive blood via reverse flow, leading to rebleeding. The wall of the splenic artery in patients with PA after pancreatitis is fragile; therefore, the intervention should be performed with minimum manipulation and technical complexity. Therefore, a thin, soft catheter should be used, along with spring coils that match the diameter of the splenic artery. In cases where this is not followed, entrapment, rupture of the arterial wall, or displacement of the spring coil may occur. In the present case, the patient remained in good general condition after interventional embolization, achieved favorable results and did not experience further gastrointestinal bleeding, abdominal pain, abdominal distension, fever, or other discomfort.
Surgery offers direct visualization and repair or resection of the bleeding vessel and pseudocyst and is generally reserved for hemodynamically unstable patients, those for whom endovascular therapy has failed, and in cases of extensive pancreatic necrosis or infection requiring debridement or drainage.17,20 Endovascular therapy (embolization or stenting) is favored for hemodynamically stable patients due to its minimally invasive nature, lower perioperative morbidity, and shorter recovery time.20–22 Surgery is associated with a higher complication rate (especially in emergency cases and severe pancreatitis patients); however, it provides definitive control, while endovascular therapy offers a favorable safety profile but is associated with a higher risk of rebleeding or need for repeat intervention if the lesion is not fully excluded or collaterals are present.20,23 Mortality rates are higher for emergent surgery, especially if performed before stabilization or in the setting of uncontrolled infection or necrosis. 20 Coil embolization is preferred for small, discrete pseudoaneurysms where the feeding vessel can be selectively catheterized and occluded without compromising major arterial flow.24–26 Covered stents are used when the parent vessel supplies critical blood flow (e.g. major arteries such as the superior mesenteric or splenic arteries) and preservation of vessel patency is crucial or when the pseudoaneurysm has a wide neck and not ideal for coiling alone.24,25,27 Covered stents require relatively straight, large, and accessible vessels and may not be feasible for use in small, tortuous, or distal branches. They prevent the need for vessel sacrifice; however, they involve a risk of stent thrombosis and require long-term antiplatelet therapy, which may not be ideal in patients with ongoing bleeding.24,25,27 Importantly, treatment should be tailored according to the patient's anatomy, clinical stability, and available expertise.20,24,25,27
This case is characterized by apparent gastric bleeding secondary to rupture into a pseudocyst communicating with the stomach and by the fact that gastroscopy suggested localized gastric mucosal exudate; the true site of bleeding was not in the stomach but in the PPC adjacent to it. The patient's 3-year history of internal drainage of the PPC provided an important clue to the correct diagnosis; contrast-enhanced abdominal CT confirmed the diagnosis and enabled successful splenic artery PA embolization. However, the exact reason for PPC recurrence remains unknown. The patient remains under surveillance, and surgical intervention is not currently indicated. The literature reports two cases of massive hemorrhage caused by splenic artery aneurysm 3 years after traumatic pancreatitis in one case and 10 years after necrotizing pancreatitis in the other, highlighting the need for considering recurrence after treatments.28,29
Pseudocyst recurrence years after initial resolution remains uncommon; however, the literature supports several plausible pathophysiological mechanisms. Chronic pancreatitis, ongoing ductal abnormalities, and fibrosis increase vulnerability to late recurrence, especially if underlying inflammatory or ductal processes persist or reactivate.30–32 Chronic pancreatitis can cause progressive ductal fibrosis, strictures, and protein plugs or calculi, which disrupt pancreatic juice flow and favor new cyst formation, even years after prior episodes.3,30 Acute exacerbations or new injuries (alcohol, stones, trauma) may trigger fresh leakage of pancreatic juice into the peripancreatic tissues, recreating a pseudocyst.30,32 Blockage or incomplete healing of previous duct–cyst communications can eventually reopen or lead to new fistulae, resulting in recurrence.3,33 Some reports have noted extremely delayed recurrence (up to 9 years post-treatment), emphasizing the importance of considering the chronic pathology and excluding neoplasm through biochemical and imaging workup. 31 Hence, the literature supports the notion that recurrence after several years is more likely attributable to chronic disease or incomplete initial ductal healing than to true primary formation.
Thus, percutaneous selective embolization of the splenic artery PA may be a favorable treatment option for patients with PPC complicated by rupture and hemorrhage of the splenic artery PA in the PPC. It is noteworthy that upper gastrointestinal hemorrhage has diverse etiologies, including PA within a PPC. When endoscopy reveals suspected gastric mucosal lesions, the possibility of adjacent vascular pathology, especially in patients with a history of PPC, should be considered. Another important clinical implication is the possibility of recurrence after prior drainage, warranting appropriate long-term follow-up.
Footnotes
Ethics approval and consent to participate
The study was approved by the Ethics Committee of The Third People's Hospital of Datong (Approval number: (2024) Research Paper Review No. 01). All participants were informed about the study protocol and provided written informed consent to participate in the study. I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards set in the 1964 Declaration of Helsinki and its subsequent amendments.
Consent for publication
Informed consent was obtained from the patient's family prior to the drafting and submission of this manuscript; the family has granted full permission for its submission and publication. While the text may include the patient's medical history, laboratory findings, and imaging data, all personally identifiable information has been redacted to ensure the protection of patient privacy.
Authors’ contributions
Jiandong Liu and Min Liang conducted the studies, collected data, and drafted the manuscript. Jinhong Yu and Yanglin Pan performed the statistical analysis and participated in its design. Zhigao Xu and Dahai Shi participated in the acquisition, analysis, or interpretation of data. All authors read and approved the final manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.