
Abstract
Objective
Although the non–high-density lipoprotein cholesterol-to-high-density lipoprotein cholesterol ratio (NHHR) has emerged as a novel indicator of lipid metabolism, its specific correlation with cognitive function remains unclear. This study aimed to comprehensively explore this association in an aging population.
Methods
This prospective cohort study comprised both cross-sectional (2015, n = 4605) and longitudinal (2018, n = 2362) analyses using data from the China Health and Retirement Longitudinal Study. Regression analysis was performed to assess the association of the NHHR with cognitive performance and cognitive impairment. Restricted cubic spline models explored potential nonlinear associations. A logistic regression model was employed in the longitudinal research to examine the correlation between baseline NHHR levels and cognitive impairment during follow-up.
Results
NHHR was positively correlated with episodic memory (regression coefficient = 0.23, p < 0.01) and total cognition (regression coefficient = 0.28, p < 0.01) and inversely correlated with cognitive impairment (odds ratio = 0.89, p = 0.013). Restricted cubic spline analysis confirmed significant nonlinear relationships for these outcomes (p < 0.05). The protective effect of an elevated NHHR was most pronounced in prediabetic individuals, showing improved memory (regression coefficient = 0.33), total cognition (regression coefficient = 0.42), and reduced cognitive impairment (odds ratio = 0.79) (all p < 0.01). Longitudinal associations with incident cognitive impairment lost significance after full covariate adjustment.
Conclusions
NHHR exhibits a nonlinear association with cognitive function in older Chinese adults. Maintaining optimal NHHRs may benefit cognitive health, particularly in prediabetic individuals.
Keywords
Introduction
With rapid aging of the global population, cognitive impairment has become a significant public health concern. 1 Currently, more than 55 million people worldwide live with dementia, a number projected to triple by 2050. In China, the burden is particularly heavy; recent epidemiological data estimate the prevalence of mild cognitive impairment and dementia among adults aged ≥60 years to be approximately 15.5% and 6.0%, respectively. 2 Dementia leads to profound loss of functional independence, increased caregiver burden, and substantial pressure on health care systems. Common risk factors for cognitive decline in older adults include advancing age; genetic susceptibility; and a cluster of modifiable cardiometabolic conditions, including hypertension, diabetes, and dyslipidemia. 3 Consequently, elucidating modifiable risk and protective factors for cognitive impairment is essential for developing effective prevention strategies.
Lipid metabolism dysregulation, a common pathological feature of chronic diseases, has garnered increasing attention because of its possible association with cognitive function.4–6 Studies have suggested that elevated low-density lipoprotein cholesterol (LDL-C) levels promote amyloid plaque formation by impairing amyloid clearance, whereas lower high-density lipoprotein cholesterol (HDL-C) levels might reduce the transport of lipophilic molecules, disrupting neuronal homeostasis. 7 Lower HDL-C levels can also damage cerebrovascular integrity through oxidative stress and endothelial dysfunction, driven by mechanisms such as lipid peroxidation and accumulation of oxidized lipoproteins. These processes compromise blood–brain barrier (BBB) function, thereby increasing the risk of neurodegeneration and cognitive impairment. 8
Although numerous studies have investigated the relationships between conventional lipid markers and cognitive function, the findings remain inconsistent. Most evidence suggests that elevated total cholesterol (TC) and LDL-C levels increase the risk of cognitive decline and dementia.9–11 However, some studies have reported either a protective association or null effects. Notably, a study involving 3467 participants has demonstrated that higher LDL-C levels significantly reduce dementia risk with a demonstrable dose–response relationship, 12 highlighting the complexity of these associations.
The NHHR, a novel indicator that comprehensively reflects lipid metabolism, can better illustrate the balanced relationship within lipid metabolism.13,14 Substantial evidence confirms the superior predictive value of the NHHR over traditional indicators for cardiovascular events, diabetes, sleep-disordered breathing, and kidney disease.15,16 The NHHR represents the balance between pro-atherogenic lipoproteins, including LDL-C, very low-density lipoprotein cholesterol (VLDL-C), remnant lipoproteins, and anti-atherogenic HDL-C particles. This balance is critical for assessing lipid metabolism and atherogenesis. High NHHRs indicate a dominance of pro-atherogenic lipoproteins over protective HDL particles, which may exacerbate neurovascular damage. Given the high prevalence of metabolic syndrome and mixed dyslipidemia in the aging Chinese population, a composite index such as the NHHR offers a more robust and clinically accessible tool than isolated lipid parameters in the evaluation of cognitive vulnerability. Nevertheless, evidence regarding the association of the NHHR with cognitive function remains scarce. Notably, recent studies have identified nonlinear relationships between composite lipid indicators and cognitive function.17,18 Relying on high-quality cohort data from the China Health and Retirement Longitudinal Study (CHARLS), the current study comprehensively examined the relationship between the NHHR and cognitive performance in older Chinese individuals by integrating cross-sectional and longitudinal analyses and analyzed whether there was a nonlinear relationship between them. The study also explored how different glucose metabolism states affect this association.
Materials and methods
Study population
The CHARLS, which began in 2011 with Wave 1, is a poll that is representative of the entire country’s population. Subsequent survey Waves were performed in 2013, 2015, 2018, and 2020 and were called Waves 2 through 5, respectively. The baseline survey included 150 counties and 450 villages across 28 provincial-level administrative divisions in China. 19 This study was conducted in accordance with the Declaration of Helsinki (as revised in 2024). The study protocol was approved by the Ethical Review Committee of Peking University, Beijing, China (Approval Number: IRB00001052-11015), and written informed consent was obtained from all participants. All data used in this study were fully deidentified. Additionally, the reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 20
This prospective cohort study comprises both cross-sectional analysis (performed utilizing data from the CHARLS 2015) and longitudinal cohort follow-up analysis (using data from the CHARLS 2018). The following exclusion criteria were enforced: (a) age <60 years; (b) lack of cognitive assessment data; (c) lack of lipid data; and (d) prior diagnosis of memory-related disease. Ultimately, 4605 participants were included. For the longitudinal analysis, we excluded individuals who met any of the following criteria: (a) total cognitive score <11 at Wave 3; (b) loss to follow-up; and (c) missing cognitive data at Wave 4. This process ultimately yielded a final analytical sample consisting of 2362 eligible participants. The participant selection process is detailed in Figure S1.
This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines for observational studies.
Measurement of the NHHR and cognitive function
The NHHR was calculated as (TC (mg/dL) − HDL-C (mg/dL))/HDL-C (mg/dL).21,22 Fasting venous blood samples were collected from participants in the morning after an overnight fast of at least 8 h.
Cognitive performance in the CHARLS cohort was assessed across two primary domains: (a) episodic memory and (b) executive function. 23 Executive function evaluation comprised three components: (a) temporal orientation (naming the current year, month, date, day of week, and season, with 1 point awarded for every correct item and a maximum of 5 points); (b) serial subtraction (five consecutive subtractions of 7 from 100, with 1 point per correct calculation and a maximum of 5 points); and (c) figure drawing (reproducing interlocking pentagons from a displayed image, with 1 point awarded for accurate reproduction). These components collectively yielded a maximum executive function score of 11 points. 24
Episodic memory was primarily assessed through immediate and delayed recall tasks. In this procedure, a set of 10 words was presented orally to each participant who was then instructed to recall them immediately. Following a 10-min delay, participants recalled the same list. The total cognition score combines episodic memory (0–20 points) with executive function (0–11 points), resulting in a maximum composite score of 31 points. Elevated scores correspond to superior cognitive performance. 25 On the basis of prior research, cognitive impairment is typically characterized by a total cognition score <11.26,27
Covariates
The inclusion of covariates in this study accounted for a variety of demographic and health-related variables. The demographic variables included sex, age, educational level, marital status, and residence. Health-related factors included common comorbidities (hypertension, diabetes, heart disease, and stroke), alcohol consumption, smoking status, body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting blood glucose (FBG), glycosylated hemoglobin (HbA1c), triglyceride (TG), TC, LDL-C, and HDL-C.
Hypertension was characterized by an SBP ≥40 mmHg and/or a DBP ≥90 mmHg (based on the average of the second and third blood pressure measurements), the utilization of antihypertensive medication, or self-reported hypertension by individuals. Diabetes was classified as self-reported, FBG level ≥126 mg/dL, HbA1c level ≥6.5%, or use of glucose-lowering drugs. Prediabetes was defined as an FBG level between 100 and 125 mg/dL or an HbA1c level between 5.7% and 6.4%. Normal glucose regulation (NGR) was defined as an FBG level <100 mg/dL and an HbA1c level <5.7%. 28
Statistical analyses
Analyses of quantitative variables that followed a normal distribution are presented as the means and SD values. Differences between the groups were assessed using analysis of variance (ANOVA). For quantitative variables that did not conform to a normal distribution, we provided the median and interquartile range values and evaluated differences among groups by performing the Kruskal–Wallis test. Categorical variables were described using counts and percentages, with statistical evaluations conducted using the chi-square test. To assess the link between continuous NHHR levels and cognitive performance, linear regression analyses were conducted; moreover, multivariable logistic regression models were used to investigate the association between the NHHR and cognitive impairment.
To investigate potential collinearity between the NHHR and other covariates, tolerance values and variance inflation factors (VIFs) were examined. The analysis indicated that all VIFs were <5, suggesting no severe multicollinearity among the covariates (Table S1). To examine the potential nonlinear association between the NHHR and cognitive outcomes, we fitted restricted cubic spline (RCS) functions in multivariable regression models. Threshold effect analysis revealed inflection points where associations changed significantly. To investigate possible effect modification, we performed subgroup analyses stratified by a series of variables. Interaction effects were tested using likelihood ratio tests.
Prospective comparisons between baseline NHHRs (2015) and incident cognitive impairment (2018) were made using logistic regression with the same adjustment model. The statistical analyses were conducted with R (version 4.4.3) and Statistical Package for Social Sciences (SPSS) software (version 25.0), employing a two-tailed test, with statistical significance set at p <0.05.
Results
Participant characteristics based on NHHR quartiles
This study included 4605 participants (Figure S1), with a mean age of 67.42 years; females comprised 45.02% of the study population. Table 1 presents the baseline characteristics of participants from Wave 3. Compared with those in Q1, participants in the higher NHHR quartiles (Q2–Q4) were more likely to be females, rural residents, and people who had never smoked or consumed alcohol; they also had higher prevalences of hypertension, diabetes, heart disease, and stroke as well as elevated blood pressure, FBG levels, and HbA1c levels (all p < 0.01). Age and marital status did not significantly differ between the quartiles (p > 0.05). Cognitively, participants in the higher NHHR quartiles had better episodic memory and total cognition scores (Q2–Q4 vs. Q1) and lower cognitive impairment prevalence (Q3–Q4 vs. Q1) (all p < 0.01). Executive function showed no significant differences across quartiles (p > 0.05).
Baseline characteristics of the participants.
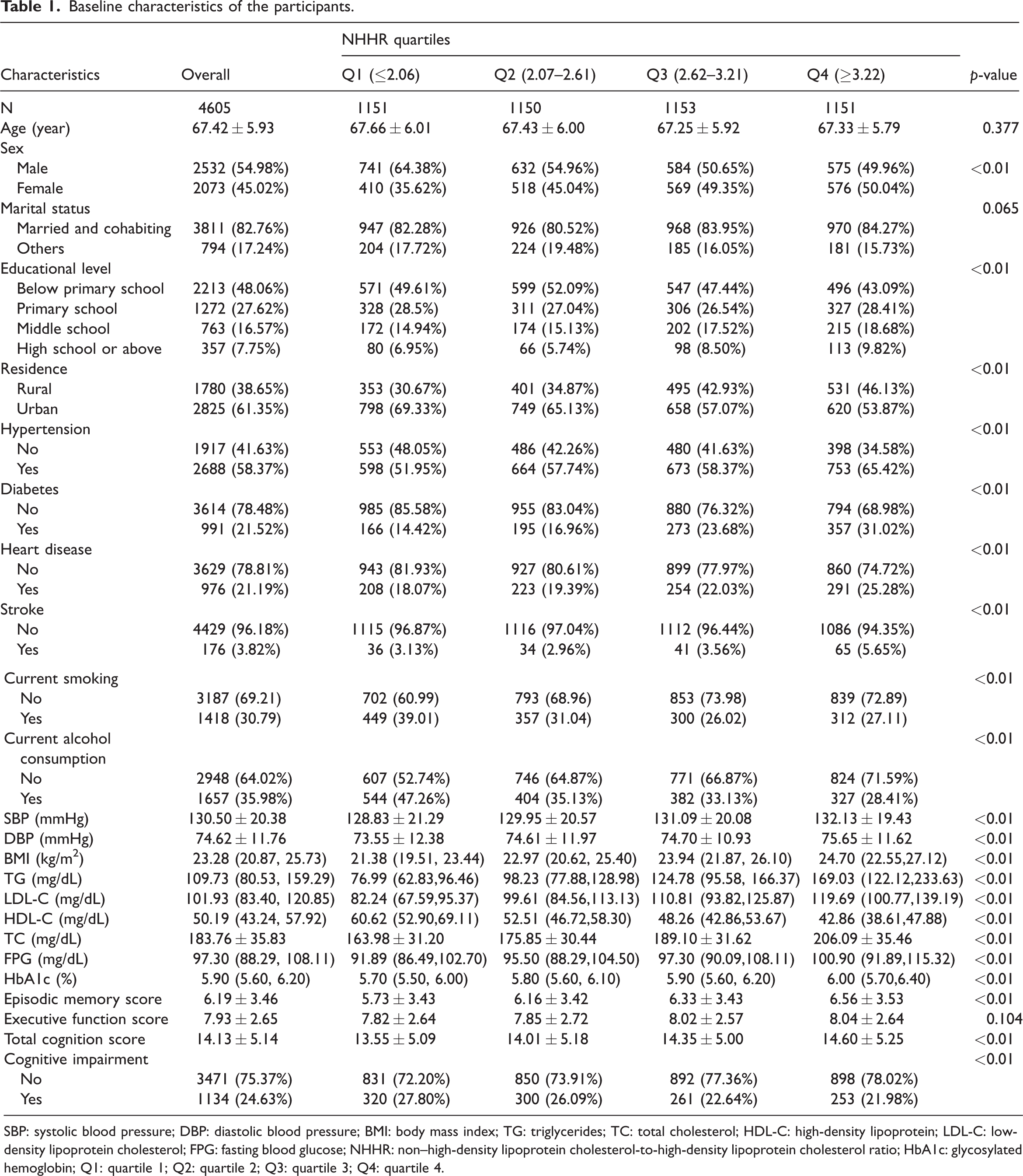
SBP: systolic blood pressure; DBP: diastolic blood pressure; BMI: body mass index; TG: triglycerides; TC: total cholesterol; HDL-C: high-density lipoprotein; LDL-C: low-density lipoprotein cholesterol; FPG: fasting blood glucose; NHHR: non–high-density lipoprotein cholesterol-to-high-density lipoprotein cholesterol ratio; HbA1c: glycosylated hemoglobin; Q1: quartile 1; Q2: quartile 2; Q3: quartile 3; Q4: quartile 4.
Associations between the NHHR and cognitive performance
Table 2 displays the associations between the NHHR and cognitive performance derived from multivariable logistic regression models. In Model 1, the NHHR was positively correlated with the episodic memory, executive function, and total cognition scores (p < 0.01). In Model 2, this association remained statistically significant (p < 0.01). Following full adjustment for covariates (Model 3), the NHHR maintained a significant positive association with the episodic memory and total cognition scores. Specifically, for each 1-unit increase in the NHHR, the episodic memory score increased by 0.23 points (regression coefficient (β) = 0.23; 95% confidence interval (CI): 0.12, 0.34; p < 0.01), and the total cognition score increased by 0.28 points (β = 0.28; 95% CI: 0.12 to 0.43; p < 0.01). However, no significant correlation was found with the executive function score. When the NHHR was analyzed as a categorical variable in Model 3, participants in the other quartiles exhibited higher episodic memory and total cognition scores than those in the first quartile; however, no such differences were observed for the executive function score (p > 0.05).
Associations between the NHHR and cognitive performance.
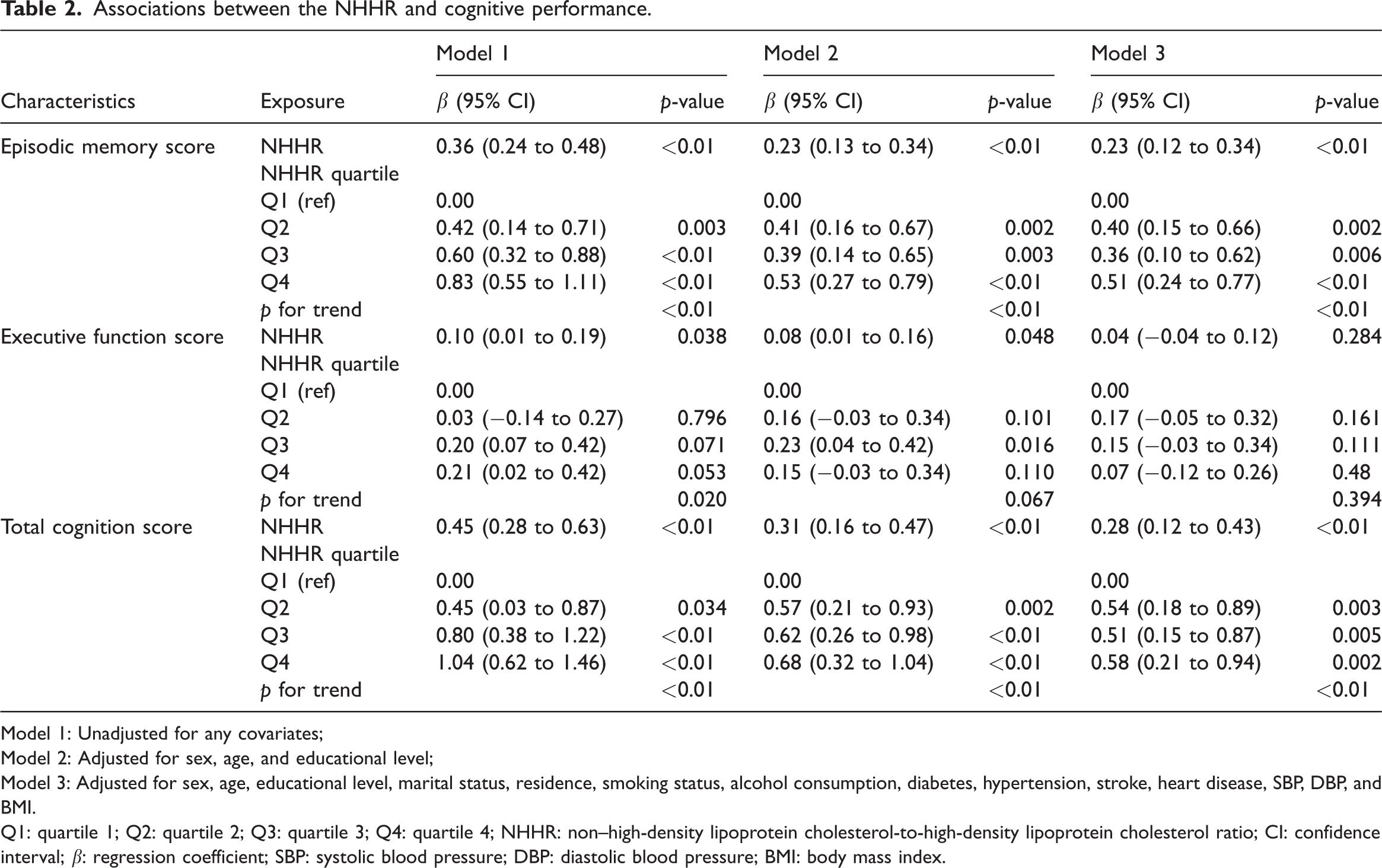
Model 1: Unadjusted for any covariates;
Model 2: Adjusted for sex, age, and educational level;
Model 3: Adjusted for sex, age, educational level, marital status, residence, smoking status, alcohol consumption, diabetes, hypertension, stroke, heart disease, SBP, DBP, and BMI.
Q1: quartile 1; Q2: quartile 2; Q3: quartile 3; Q4: quartile 4; NHHR: non–high-density lipoprotein cholesterol-to-high-density lipoprotein cholesterol ratio; CI: confidence interval; β: regression coefficient; SBP: systolic blood pressure; DBP: diastolic blood pressure; BMI: body mass index.
Fully adjusted RCS analysis revealed significant nonlinear associations of the NHHR with episodic memory (nonlinear p = 0.015) and total cognition (nonlinear p = 0.004) (Figure 1(a) to (c)); inflection points emerged at NHHRs of 2.42 and 2.53, respectively. Below these thresholds, a 1-unit increase in the NHHR significantly improved episodic memory (β = 0.64, 95% CI: 0.23 to 1.03; p < 0.01) and total cognition (β = 0.85, 95% CI: 0.36 to 1.34; p < 0.01). Above these points, associations became non-significant (episodic memory, p = 0.597; total cognition, p = 0.821). Executive function showed no significant correlation (p > 0.05) (Table S2).
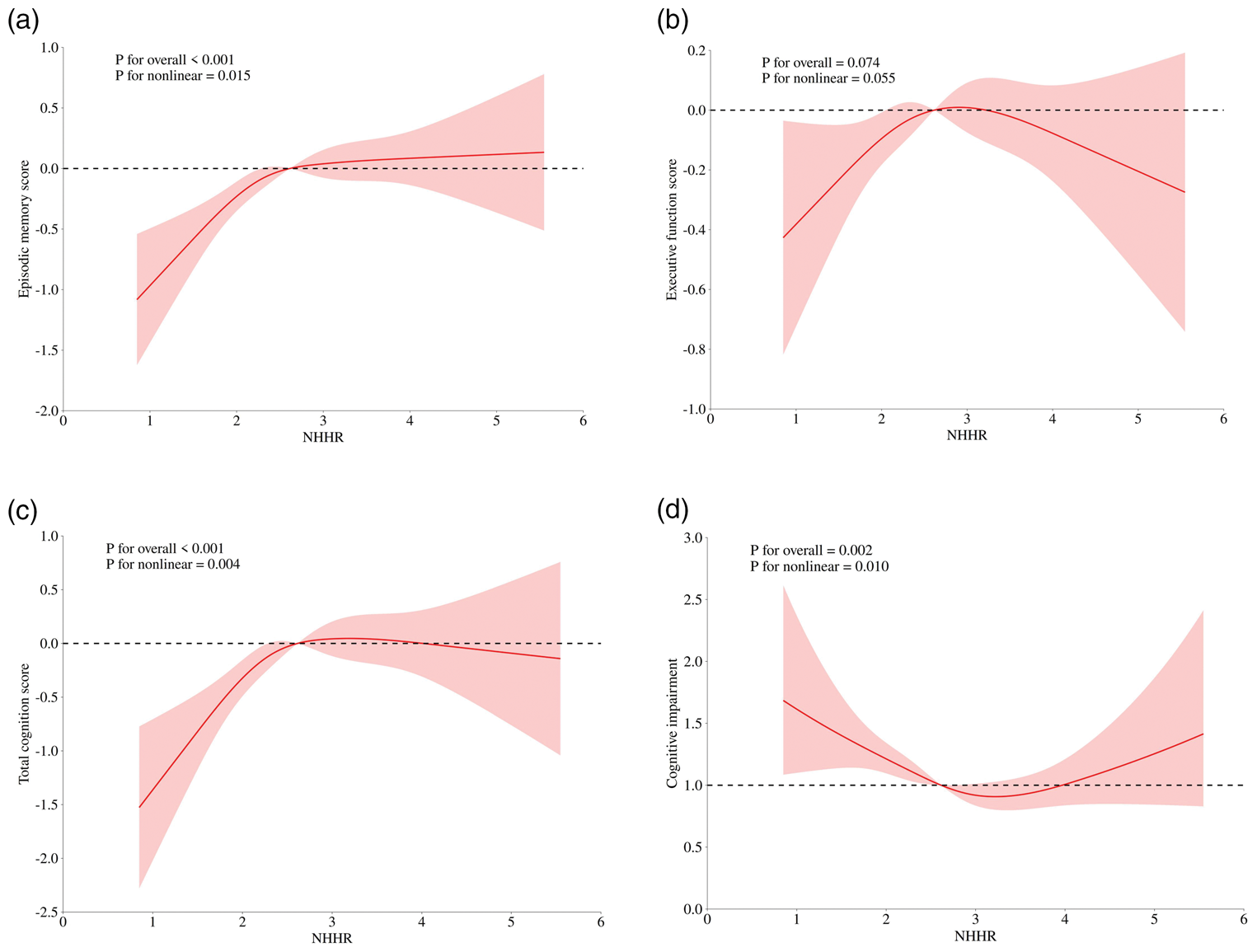
Dose–response relationship between the NHHR and cognitive function. (a) Episodic memory score; (b) executive function score; (c) total cognition score; (d) cognitive impairment. Adjusted for sex, age, educational level, marital status, residence, smoking status, alcohol consumption, diabetes, hypertension, stroke, heart disease, SBP, DBP, and BMI. NHHR: non–high-density lipoprotein cholesterol-to-high-density lipoprotein cholesterol ratio; SBP: systolic blood pressure; DBP: diastolic blood pressure; BMI: body mass index.
Associations between the NHHR and cognitive impairment
To evaluate the link between the NHHR and cognitive impairment, we performed multivariate logistic regression analysis (Table 3). In Model 3, each 1-unit increase in the NHHR was associated with an 11% reduction in cognitive impairment (odds ratio (OR) = 0.89, 95% CI: 0.81 to 0.98; p = 0.013). When the NHHR was analyzed as quartiles in the fully adjusted model (Model 3), compared with Q1, cognitive impairment was reduced by 16% in Q2 (OR = 0.84; 95% CI: 0.68 to 1.03; p = 0.090), 24% in Q3 (OR = 0.76; 95% CI: 0.61 to 0.94; p = 0.013), and 23% in Q4 (OR = 0.77; 95% CI: 0.62 to 0.97; p = 0.024), demonstrating a notable dose–response trend across quartiles (p trend = 0.039). Furthermore, after additional adjustment for lipid-lowering medications as well as both lipid-lowering and antihyperglycemic drugs, the association between the NHHR and a reduced risk of cognitive impairment remained statistically significant (Model 5: OR = 0.82, 95% CI: 0.74 to 0.91, p < 0.001) (Table S3).
Relationship between the NHHR and cognitive impairment.
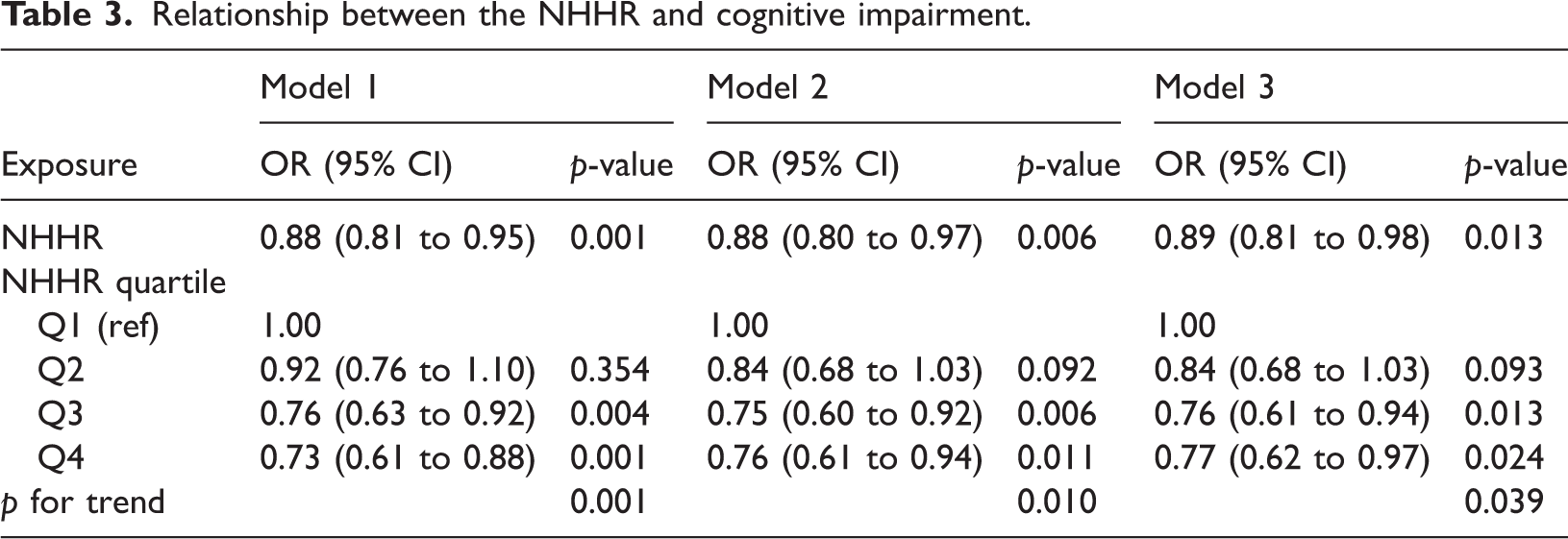
Model 1: Unadjusted for any covariates;
Model 2: Adjusted for sex, age, and educational level;
Model 3: Adjusted for sex, age, educational level, marital status, residence, smoking status, alcohol consumption, diabetes, hypertension, stroke, heart disease, SBP, DBP, and BMI.
CI: confidence interval; OR: odds ratio; NHHR: non–high-density lipoprotein cholesterol-to-high-density lipoprotein cholesterol ratio; Q1: quartile 1; Q2: quartile 2; Q3: quartile 3; Q4: quartile 4; SBP: systolic blood pressure; DBP: diastolic blood pressure; BMI: body mass index.
To further investigate the nonlinear relationships between the NHHR and cognitive impairment, RCS analysis revealed a significant nonlinear association in Model 3 (overall p = 0.002, nonlinear p = 0.010; Figure 1(d)). Threshold analysis (Table S4) revealed an inflection point at an NHHR of 3.2. Under this threshold, each 1-unit increase in the NHHR was related to a 25% decrease in cognitive impairment (OR = 0.75, 95% CI: 0.64 to 0.88; p < 0.01). Above this inflection point, each 1-unit increase in the NHHR showed a non-significant association (OR = 1.31, 95% CI: 0.97 to 1.75; p = 0.076).
Associations between the NHHR and cognitive function according to glucose metabolism status
Tables S5 and S6 present the associations between the NHHR and cognitive function across different glucose metabolism states. In patients with prediabetes, an increase in the NHHR was significantly linked to improvements in the episodic memory and total cognition scores (p < 0.01 for both), and these associations remained robust after covariate adjustment. In contrast, in the NGR group, associations were observed only for episodic memory and total cognition scores in Model 1; after controlling for relevant factors, these results were no longer statistically significant, and no significant associations were detected in the diabetes mellitus (DM) group across all the models (all p > 0.05). Specifically, in Model 3, a 1-unit increase in the NHHR was associated with a 21% decrease in the probability of cognitive impairment in the prediabetes group (OR = 0.78; 95% CI: 0.68 to 0.90; p < 0.001); however, in the NGR and DM groups, no direct associations between the NHHR and cognitive impairment were observed in any model (all p > 0.05)
Subgroup analysis
To further elucidate the link between the NHHR and cognitive impairment, we performed several subgroup analyses. In analyses stratified by sex, educational level, residence, marital status, hypertension, stroke history, heart disease, and BMI categories (Figure S2), the relationships between the NHHR and cognitive impairment remained consistent, except for age and heart disease status (interaction p > 0.05 for sex, residence, marital status, educational level, hypertension, and BMI). Interaction tests revealed significant effect modifications for heart disease (p for interaction = 0.007) and age group (p for interaction = 0.046). Subgroup analysis specifically focusing on participants with heart disease revealed a potential threshold effect of the NHHR on cognitive impairment. Although the standard linear regression model showed a significant protective association (OR = 0.60, 95% CI: 0.46 to 0.79, p < 0.001), the two-piecewise linear regression identified an inflection point at 1.50 (Table S7).
Longitudinal analysis for the association between NHHR and cognitive impairment based on data from Waves 3 and 4
Among the 2362 participants in 2015 (Wave 3), 368 individuals (15.58%) developed new-onset cognitive impairment by 2018 (Wave 4). The incidence rates of cognitive impairment across the NHHR quartiles were 18.23% (105/576) in Q1, 17.23% (97/563) in Q2, 15.24% (91/597) in Q3, and 11.98% (75/626) in Q4, demonstrating a statistically significant decreasing trend (p < 0.05) (Figure S3). Table 4 presents the longitudinal association between the NHHR and cognitive impairment according to logistic regression models. In Model 1, a 1-unit increase in the NHHR was linked to an 18% reduction in the odds of cognitive impairment (OR = 0.82; 95% CI: 0.72 to 0.93; p = 0.025). The association remained stable in Model 2; however, after full adjustment in Model 3, no significant association was found.
Longitudinal analysis of the association between NHHR and cognitive impairment utilizing data from Waves 3 and 4.
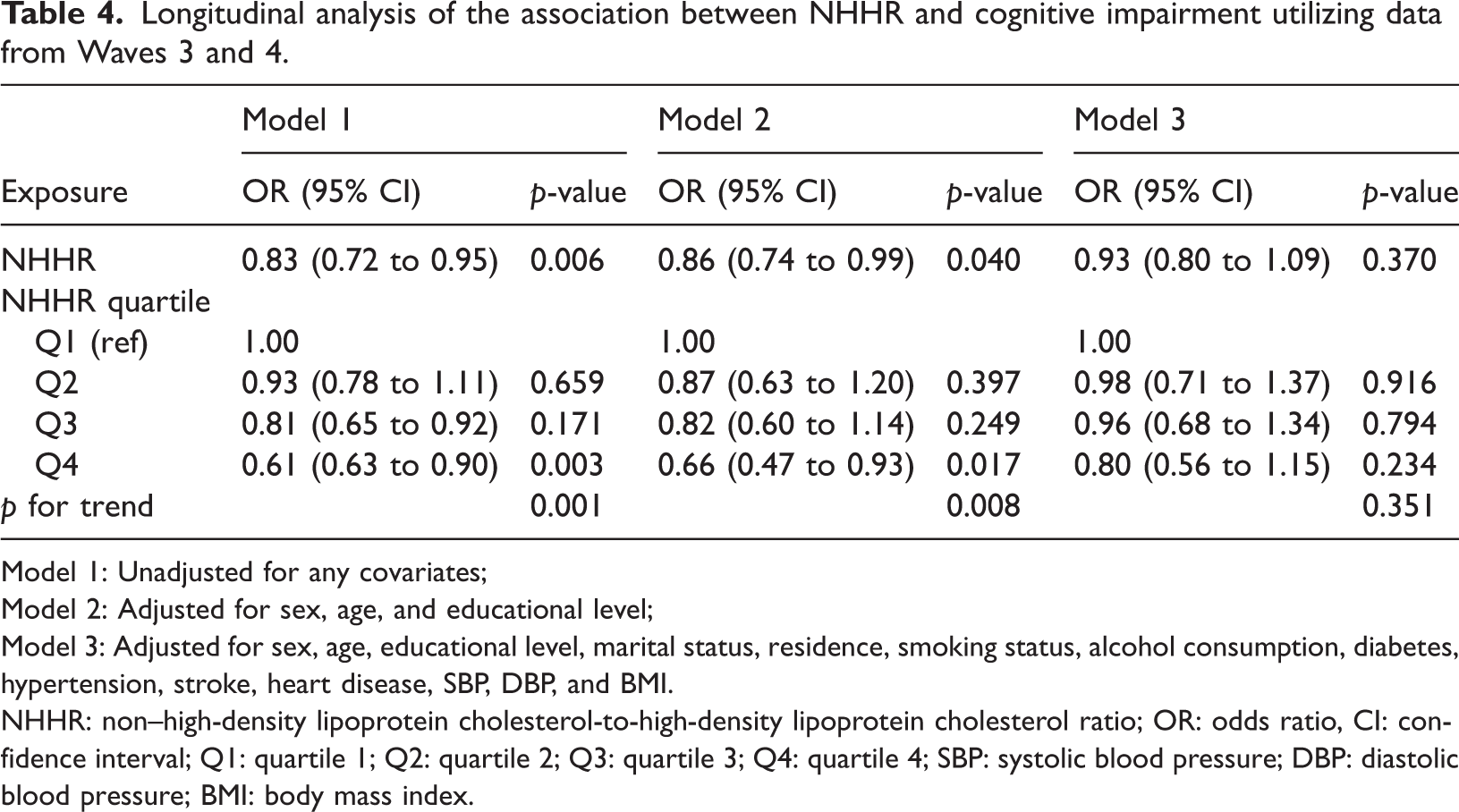
Model 1: Unadjusted for any covariates;
Model 2: Adjusted for sex, age, and educational level;
Model 3: Adjusted for sex, age, educational level, marital status, residence, smoking status, alcohol consumption, diabetes, hypertension, stroke, heart disease, SBP, DBP, and BMI.
NHHR: non–high-density lipoprotein cholesterol-to-high-density lipoprotein cholesterol ratio; OR: odds ratio, CI: confidence interval; Q1: quartile 1; Q2: quartile 2; Q3: quartile 3; Q4: quartile 4; SBP: systolic blood pressure; DBP: diastolic blood pressure; BMI: body mass index.
RCS analysis was performed to further investigate the association between baseline NHHR and incident cognitive impairment (Figure S4). The results demonstrated a significant overall association (p for overall = 0.024), characterized by a largely linear decrease in the risk of cognitive impairment as the NHHR increased (p for nonlinear = 0.366).
Discussion
Our data revealed a positive correlation between elevated NHHRs and better episodic memory and total cognitive scores. In contrast, lower NHHRs were correlated with higher odds of cognitive impairment. These relationships remained strong even after several variables were adjusted for. Notably, the relationship between the NHHR and cognitive function exhibited a nonlinear pattern and demonstrated population-specific effects, particularly in individuals with prediabetes. Furthermore, a longitudinal follow-up over 3 years revealed that those in the lower quartiles of the NHHR had a greater likelihood of developing new-onset cognitive impairment than those in the highest quartile. These findings underscore the dual role of lipid metabolism in cognitive aging and imply that the NHHR might be a valuable indicator of cognitive susceptibility stratification.
The relationship between conventional lipid markers and cognitive function remains controversial. High lipid levels can promote atherosclerosis, impair cerebral vascular integrity, and reduce cerebral blood flow perfusion, thereby affecting the energy supply and metabolic homeostasis of neurons and leading to cognitive decline and dementia risk.29,30 Ma et al. have reported that a 1-mmol/L increase in TC and LDL-C levels is correlated with a significant deterioration in cognitive function, with an estimated yearly decrease ranging from 0.28 to 0.42 points. 31 Two longitudinal studies have also reported that individuals with higher levels of LDL-C and TC are at an increased risk of dementia.32,33 However, conflicting evidence exists. TC levels were observed to be lower in those with cognitive impairment, and TC levels were positively correlated with Mini-Mental State Examination scores, according to studies conducted in China among older individuals and centenarians. 34
This study utilized the NHHR, which is a comprehensive indicator reflecting the balance of lipid metabolism and is computationally simple and clinically accessible.35,36 Some studies have suggested a nonlinear relationship between the NHHR and lipid metabolism. For example, Zhang et al. 17 and Zhou et al. 18 have reported a nonlinear relationship between composite lipid markers such as non–HDL-C and TC/HDL-C and cognitive function, with dose–response effects observed in different populations. Compared with previous studies examining lipid ratios and cognitive outcomes,37,38 the present work extends the literature in several important directions. First, by applying RCS and two-piecewise regression models, we demonstrated a relationship between the NHHR and cognitive function, identifying inflection points that suggest a threshold effect. Second, stratified analyses revealed that the protective effect of a higher NHHR was most pronounced among individuals with prediabetes, indicating a possible interaction between the lipid–glucose metabolism and cognitive vulnerability. Third, the inclusion of both cross-sectional and longitudinal analyses provides stronger support for the temporal relevance of the NHHR in the context of cognitive decline.
RCS and threshold analysis revealed a nonlinear association between the NHHR and cognitive function. These findings were consistent across episodic memory and total cognitive scores. This discovery challenges the traditional assumption of linear relationships and suggests that the effect of lipid metabolism on cognitive function exhibits a “threshold effect.” Moderate elevations in the NHHR may be more protective against cognitive function decline, whereas extreme elevations may result in the loss of protective effects or even become detrimental. The underlying mechanism may involve moderate NHHRs, reflecting a dynamic balance in lipid metabolism, preventing the excessive accumulation of atherogenic lipids, 39 and thereby supporting cerebral vascular homeostasis and neuronal function. Conversely, an excessively high or low NHHR may disrupt this balance. Neuronal cell membranes rely on cholesterol as a key component to maintain membrane integrity and fluidity; 40 low cholesterol levels may impair neurotransmitter and synaptic functions, 41 whereas high levels of cholesterol, particularly non–HDL-C, may indirectly affect cognitive function via pathways such as endothelial injury, neuroinflammation, and β-amyloid deposition.42–44
We additionally examined the correlation between the NHHR and cognitive function across various glucose metabolic statuses. In the prediabetes group, after full adjustment, an increase in the NHHR was substantially related to improved performance in terms of episodic memory and total cognitive scores as well as a 22% reduction in cognitive impairment. However, no similar relationship was observed in patients with NGR or diabetes. This finding could be attributable to the fact that in individuals with diabetes, microvascular complications and excessive oxidative stress may override the regulatory effects of the NHHR, thereby masking its potential protective effects on cognitive function.45,46 In the NGR group, the metabolic state was relatively stable, and the regulatory mechanisms of lipid metabolism and neurofunction may have been more balanced, potentially mitigating the effect of the NHHR on cognitive function without other metabolic or pathological disturbances. In individuals with prediabetes, the brain is subjected to early-stage metabolic stress; however, the structural integrity of the microvasculature remains relatively preserved. At this stage, higher lipid reserves may serve as a critical defense mechanism. 47
The protective effect of the NHHR against cognitive impairment in the cardiac disease subgroup was significantly stronger than that in individuals without cardiac disease, stemming primarily from the dual effects of biological mechanisms and clinical characteristics. Mechanistically, cardiac disease induces cerebral hypoperfusion, neuroinflammation, and oxidative stress, exacerbating cognitive damage. By balancing lipid metabolism, the NHHR enhances the vasodilatory, anti-inflammatory, and antioxidant functions of HDL-C, specifically improving cerebral blood flow, inhibiting the neuroinflammatory cascade, and reducing neuronal oxidative damage—this protective effect is more prominent under pathological conditions.48,49
The longitudinal analysis in this study indicated that individuals with higher baseline NHHRs exhibited a reduced incidence of new-onset cognitive impairment over a 3-year follow-up period. However, after full adjustment for confounding factors, the association lost statistical significance. These findings indicate that the short-term relationship between the NHHR and cognitive impairment could be affected by uncontrollable variables, including long-term dietary patterns and the apolipoprotein E genotype. The long-term predictive value of the NHHR may require validation in longer-term cohort studies.
Furthermore, lifestyle modifications such as structured exercise can significantly improve lipid profiles and cognitive outcomes in older adults with metabolic syndrome.50,51 This suggests that managing composite lipid indicators such as the NHHR through targeted lifestyle strategies offer synergistic benefits for neurovascular health.
The findings regarding the nonlinear association between the NHHR and cognitive function in older Chinese adults have clear practical implications for real-world applications. Specifically, individuals with an NHHR <3.2, particularly those with prediabetes, should be prioritized for more frequent follow-ups.
Strengths and limitations
This study has several key strengths. First, the CHARLS involves a nationally representative cohort and features comprehensive cognitive assessments. We rigorously adjusted for confounding factors and validated the findings through longitudinal analysis. Second, this study examined the relationship between the NHHR and cognitive impairment across different glucose metabolic states. Finally, the NHHR is a clinically accessible indicator, which enhances its applicability.
Certain study limitations must be acknowledged. First, the cross-sectional design inhibits the ability to draw causal conclusions, as longitudinal analysis revealed attenuated associations after full covariate adjustment, possibly because of insufficient follow-up duration or cognitive assessment sensitivity. Second, despite comprehensive covariate control, confounding from unknown factors cannot be excluded. Third, the lack of APOE4 genetic data in the CHARLS database is a notable constraint, as APOE4 is a major genetic determinant of both lipid metabolism and Alzheimer’s disease risk. Finally, the study was limited to older Chinese adults; therefore, caution is warranted when extrapolating these results to other ethnic groups or younger populations.
Conclusion
This study offers novel evidence regarding the association between lipid metabolism and cognitive function, revealing a nonlinear association between the NHHR and cognitive function in older Chinese adults. The findings indicate that maintaining an optimal NHHR may exert a protective effect against cognitive impairment, particularly among individuals with prediabetes. In the future, longer-term studies are necessary to verify the long-term predictive value of the NHHR and explore its underlying mechanism of action to provide more precise strategies for the prevention and management of cognitive impairment.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605261457282 - Supplemental material for Nonlinear association of the non–high-density lipoprotein cholesterol-to-high-density lipoprotein cholesterol ratio with cognitive function in older Chinese adults: A prospective cohort study
Supplemental material, sj-pdf-1-imr-10.1177_03000605261457282 for Nonlinear association of the non–high-density lipoprotein cholesterol-to-high-density lipoprotein cholesterol ratio with cognitive function in older Chinese adults: A prospective cohort study by Xiangguo Cong, Sijue Yang, Yiwen Chen and Yan Bi in Journal of International Medical Research
Footnotes
Acknowledgments
We extend our appreciation to the participants and staff of the CHARLS for their efforts.
Author contributions statement
Xiangguo Cong: Conceptualization, Methodology, Formal analysis, and Writing-Original Draft. Sijue Yang: Conceptualization, Methodology, Formal analysis, and Writing-Original Draft. Yiwen Chen: Formal analysis and Data Curation. Yan Bi: Funding acquisition, Supervision, and Writing-Review & Editing.
Consent for publication
All the authors have given their approval for publication.
Data availability
Declaration of conflicting interests
The authors declare that they have no competing interests.
Ethics statement
The study involving human participants was approved by the Ethical Review Committee of Peking University, Beijing, China (Approval number: IRB00001052-11015) in compliance with local legislation and institutional requirements. All the participants provided signed informed consent.
Funding
This work was supported by the Noncommunicable Chronic Diseases-National Science and Technology Major Project (2024ZD0523200), the National Chinese–Western Medicine Clinical Collaboration Project for Major Difficult Diseases (2024–92), and the Multidisciplinary Joint Innovation and Tackling New Technology Project from the Affiliated Drum Tower Hospital, Medical School of Nanjing University.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.