
Abstract
Objective
To identify factors associated with adalimumab response in patients with rheumatoid arthritis, particularly focusing on the clinical characteristics and neutrophil-to-lymphocyte ratio.
Methods
This prospective study included 189 patients with rheumatoid arthritis. Associations between treatment response and various demographic, clinical, therapeutic, disease activity, and serological parameters were analyzed, including serum concentrations of proinflammatory cytokines. Treatment response was assessed using the Disease Activity Score in 28 joints at week 24.
Results
Baseline neutrophil-to-lymphocyte (odds ratio = 3.1, 95% confidence interval: 1.04–7.50, p = 0.019) was identified as an independent predictor of favorable response to adalimumab. Among good responders, neutrophil-to-lymphocyte levels decreased significantly following initiation of tumor necrosis factor inhibitor treatment (p < 0.001). Patients achieving Disease Activity Score in 28 joints-defined remission at week 24 had significantly higher baseline neutrophil-to-lymphocyte values than non-remitters (p < 0.001). A significantly greater proportion of patients in the high-neutrophil-to-lymphocyte group attained remission compared with the low-neutrophil-to-lymphocyte group (62.1% vs. 39.2%, p < 0.001).
Conclusions
A higher baseline neutrophil-to-lymphocyte is associated with improved response to adalimumab therapy in rheumatoid arthritis. These findings support the potential use of baseline neutrophil-to-lymphocyte as a clinically applicable biomarker for predicting therapeutic outcomes following adalimumab treatment.
Introduction
Rheumatoid arthritis (RA)—a chronic systemic inflammatory condition primarily affecting the joints—can lead to persistent synovitis, bone erosion, and progressive articular damage.1,2 Additionally, RA may affect multiple organ systems, causing cardiovascular, ophthalmologic, or pulmonary complications. 3 In advanced stages, RA can cause permanent disability and interstitial lung fibrosis, substantially diminishing both quality of life and long-term survival. 4
The exact etiology of RA is not completely understood. Current evidence highlights the central role of chronic inflammation in disease progression, with key mediators such as tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6) contributing to clinical symptoms, including joint swelling, pain, and radiographic damage.2,4 Although biologic therapies targeting TNF-α have significantly advanced RA management, approximately 20%–40% of patients exhibit inadequate responses or experience loss of efficacy over time.5,6 Furthermore, some patients develop adverse events that limit the long-term use of these agents.
Substantial research has been devoted to identifying factors predicting the response to TNF-α inhibitors 5 ; certain clinical characteristics—including patient age, duration of illness, number of previously administered disease-modifying antirheumatic drugs (DMARDs), tender joint count, levels of acute-phase reactants, neutrophil percentage, and Disease Activity Score in 28 joints (DAS28)—may correlate with the treatment outcomes of TNF-α inhibitors, including adalimumab (ADA).3,5,7,8 Nonetheless, these associations are not consistently reproducible, which may be attributable to limitations such as small sample sizes, retrospective study designs, patient selection bias, variability in disease activity measures, and inconsistent assessment time points.
The lack of reliable biomarkers capable of predicting treatment response remains a critical challenge in the current management of RA.8,9 The development of easily measurable stratification markers is warranted to improve patient selection and maximize the potential for favorable clinical outcomes. In standard RA care, peripheral blood is routinely assessed for total leukocyte counts and differentials, which include neutrophil measurement.3,10 As key mediators of acute inflammation, neutrophils release numerous proinflammatory cytokines upon activation. The neutrophil-to-lymphocyte ratio (NLR) serves as a practical metric for quantifying the circulating neutrophil compartment. 11 Elevated NLR levels are commonly observed in patients with RA compared with healthy individuals. 12
Numerous studies have highlighted the NLR as a useful, cost-effective biomarker in RA management.11–13 The NLR, calculated from routine complete blood counts, reflects the systemic inflammatory state by quantifying the balance between innate (neutrophil) and adaptive (lymphocyte) immune responses. 13 In RA, chronic inflammation often manifests as neutrophilia and relative lymphopenia, leading to an elevated NLR compared to that in healthy individuals. 11 Beyond its association with disease activity and severity, emerging evidence suggests NLR’s potential predictive value for treatment outcomes. For instance, a study has demonstrated that although patients with a high baseline NLR may have a lower likelihood of responding to conventional synthetic DMARDs such as methotrexate, they may show a better response to certain targeted therapies such as Janus kinase inhibitors. 12
ADA is a fully human immunoglobulin monoclonal antibody that functions by neutralizing both soluble and membrane-bound TNF-α, a key inflammatory cytokine. 14 This mechanism makes it an effective treatment for RA and other immune-mediated inflammatory diseases, including axial spondyloarthritis and inflammatory bowel disease. 15 Its efficacy and safety in RA treatment are well established, with 60%–70% of patients achieving a meaningful response based on DAS28-erythrocyte sedimentation rate (ESR) improvements at weeks 12 and 24 and reduced radiographic progression. 16 A 2019 meta-analysis of 13 studies, including over 1500 patients with RA, confirmed that the NLR was consistently elevated compared with that in healthy controls and was strongly associated with the presence of disease. 17 Further indications included methotrexate (MTX)-naïve patients with an NLR higher than 2.7 who were more likely to fail triple conventional synthetic DMARD therapy, while higher baseline NLR levels were associated with an improved response to filgotinib treatment. 18 However, the predictive value of NLR for TNF-α inhibitor response remains unclear. Given that clinical features alone are insufficient for guiding individualized therapy, it was hypothesized that specific biomarkers may offer improved predictive ability for treatment response to biological DMARDs.
In this exploratory analysis, data from 100 patients with RA were analyzed to investigate the association between baseline NLR and improved clinical response to ADA.
Patients and methods
Patients and treatments
A prospective cohort study was conducted involving patients with active RA who exhibited an inadequate response to MTX therapy. Participants were enrolled between February 2023 and December 2023 at Pingxiang People’s Hospital, China. The inclusion criteria comprised a confirmed diagnosis of RA according to the 2010 American College of Rheumatology/European League Against Rheumatism (EULAR) classification criteria. Exclusion criteria included active infections, current malignancies, or severe and unstable comorbid conditions affecting major organ systems.
Patients received 40 mg of subcutaneous ADA every 2 weeks over a 24-week period. Throughout the study, oral MTX (10–25 mg/week orally) was maintained at a stable dose for all participants. Corticosteroid regimens (kept stable at ≤10 mg/day) were also kept constant during the entire follow-up period. At baseline, 195 patients with RA met the predefined inclusion criteria. Six patients withdrew from the study due to adverse events (liver function abnormalities (n = 3), thrombocytopenia (n = 1), pneumonia (n = 1), and duodenal ulcer (n = 1)). A total of 189 patients completed the treatment course and were included in the final assessment of ADA therapeutic response. The study protocol was reviewed and approved by the Ethics Committee of Pingxiang People’s Hospital (Approval No. SW-2025Z070 -HS02, approved on 10 January 2023), and all procedures were performed in accordance with ethical standards for medical research involving human participants.
All eligible participants provided written informed consent before enrollment in the study, in compliance with both institutional regulations and international research governance frameworks. All patient data were anonymized, and confidentiality was strictly maintained.
Clinical data collection
Clinical and demographic data were carefully extracted from the electronic health record database, covering a broad spectrum of details related to the study cohort. The baseline demographic and clinical characteristics of all patients diagnosed with active RA were collected. These parameters included age, sex, disease duration, ESR (Westergren method, mm/h), C-reactive protein (CRP, Beckman Coulter AU 400 Unicel DXC 800 Synchron Clinical System, mg/L), and the counts of neutrophils, lymphocytes, and monocytes. Serum levels of key proinflammatory cytokines—TNF-α and interleukin (IL)-6—were recorded in all patients prior to treatment initiation and at week 24 following ADA therapy using a Luminex-based multiplex immunoassay platform that uses fluorescent bead technology (R&D Systems, Minneapolis, MN, USA, pg/mL). Cytokine concentrations were determined through interpolation from standardized calibration curves. The DAS28 using ESR was calculated with the aid of a visual analog scale, the number of tender and swollen joints, ESR, and the patient’s overall health assessment.
Evaluation criteria for efficacy
The criteria for assessing therapeutic efficacy were categorized into clinical response and non-clinical response. In all patients with RA, DAS28 scores were measured prior to the initiation of treatment and 24 weeks after the commencement of treatment. Following EULAR guidelines, a clinical good response is defined as either a reduction of at least 1.2 points in the DAS28 score and a post-treatment score below 3.2. Remission was defined as a DAS28‑ESR score <2.6 at week 24.
Statistical analysis
Data analysis was performed using SPSS version 23.0 (IBM Corp., Armonk, NY), and graphical visualization was conducted using GraphPad Prism 8. Continuous variables that adhered to a normal or approximately normal distribution are presented as mean ± standard deviation. Independent samples t-tests were employed to assess intergroup differences. For variables that violated the assumption of normality, the non-parametric Wilcoxon rank-sum test was used. Categorical variables are summarized as frequencies and percentages, and the chi-square test was applied to compare proportions across groups. Pearson’s correlation analysis was conducted to evaluate the strength and direction of linear relationships between continuous variables. A binary logistic regression model, adjusted for baseline DAS28, disease duration, and ESR, was used to identify independent predictors of a good clinical response to adalimumab, with results expressed as odds ratios (OR) and 95% confidence intervals (CIs). Receiver-operating characteristic (ROC) curve analysis was performed to assess the predictive accuracy of NLR and other markers for treatment response. The area under the curve (AUC), sensitivity, and specificity are reported. The optimal cut-off value for baseline NLR was determined by maximizing the Youden index (Youden index = Sensitivity +Specificity - 1). Statistical significance was set at a two-tailed p-value of <0.05.
Results
Predictors of treatment response to ADA
This prospective cohort study evaluated 189 patients with RA undergoing ADA therapy, stratified by treatment outcomes. At week 24, treatment response assessed by DAS28 was classified as “good” in 100 patients (52.9%) and “non-good” in 89 patients (47.1%). The good response cohort demonstrated statistically significant baseline disparities versus non-good responders, including shorter disease duration (p < 0.001), lower ESR (p = 0.038), and high inflammatory markers (NLR, p < 0.001) (Table 1). Good responders exhibited significantly higher NLR than poor responders.
Characteristics of the good response group and non-good response group.

Welch two sample t-test.
Pearson’s chi-squared test.
Data are presented as the mean ± SD unless otherwise indicated.
RA: rheumatoid arthritis; bDMARDs: biological disease-modifying antirheumatic drugs; ADA: adalimumab; NLR: neutrophil-to-lymphocyte ratio; MTX: methotrexate; ESR: erythrocyte sedimentation rate; JAKi: Janus kinase inhibitor; RF: rheumatoid factor; ACPA: anti-cyclic citrullinated peptide antibody; DAS28: Disease Activity Score in 28 joints; TNF-α: tumor necrosis factor-α; IL-6: interleukin-6.
Baseline NLR as a strong predictor of ADA response at week 24
The associations between clinical and laboratory parameters and the likelihood of achieving a good response at week 24 are presented in Table 2. When patients treated with adalimumab were stratified by baseline NLR using the median value of 2.7 as the cut-off (based on the previously established threshold of >2.7 for elevated NLR), 19 those with high baseline NLR had 3.1-fold higher odds of being good responders compared with those with low baseline NLR (OR = 3.1, 95% CI 1.04–7.50; p = 0.019; R2 = 0.075).
Changes in NLR levels after 24 weeks of treatment with adalimumab.
Data are presented as the mean ± SD unless otherwise indicated.
NLR: neutrophil-to-lymphocyte ratio.
ROC curve analysis was used to quantify the prognostic utility of pretreatment biomarkers in predicting therapeutic responsiveness (Figure 1). Analysis of circulating inflammatory indices revealed that the NLR achieved superior prognostic differentiation (AUC: 0.830, 95% CI: 0.772–0.888; p = 0.004) compared with conventional disease activity measures. Composite scoring systems demonstrated moderate predictive capacity: ESR (AUC 0.671; 95% CI: 0.595–0.747), CRP (AUC 0.673; 95% CI: 0.595–0.750), and DAS28 (AUC: 0.692; 95% CI: 0.616–0.768; p = 0.015).
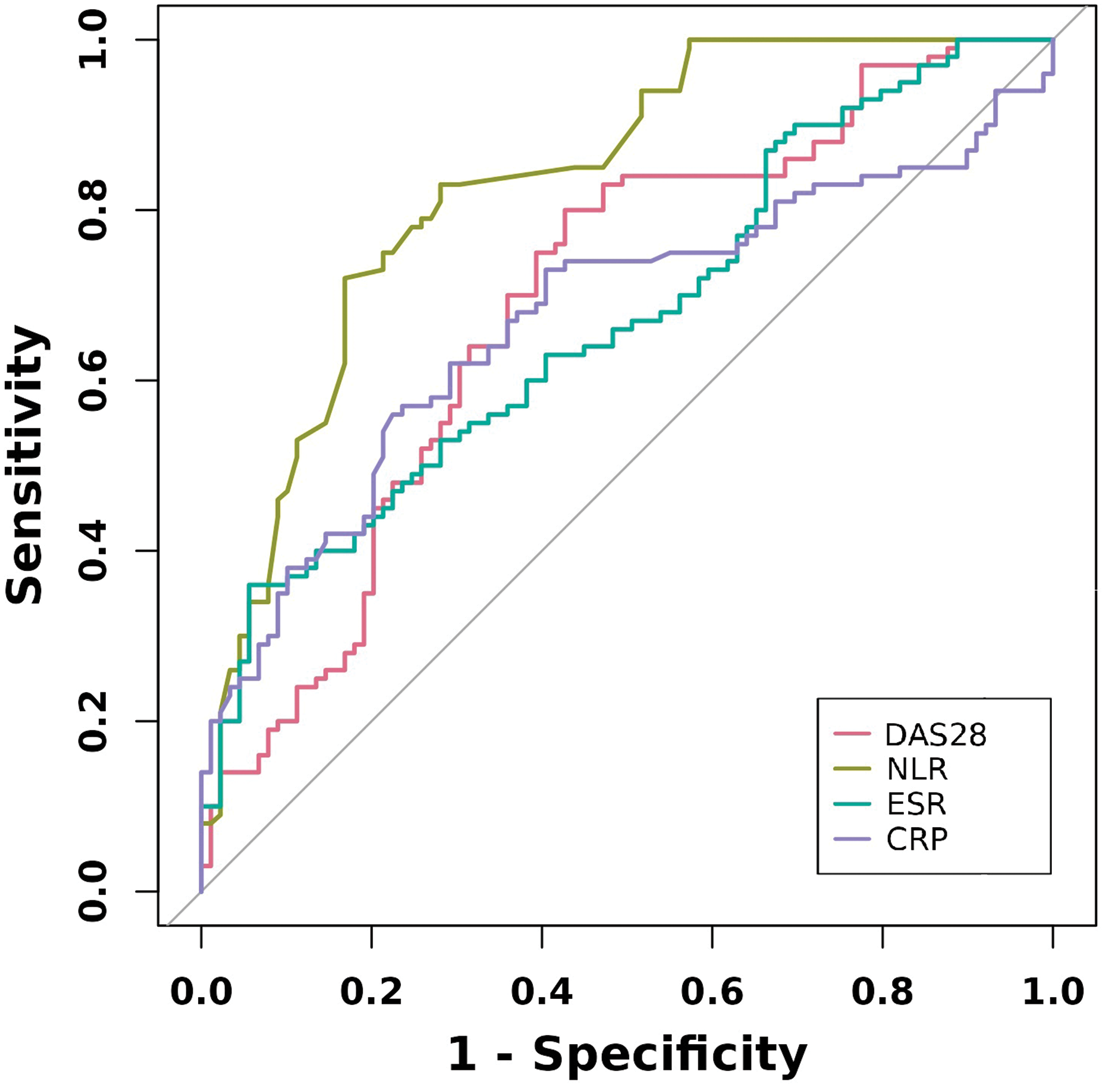
The receiver-operating characteristic (ROC) curve and the predictive ability for good response to adalimumab at week 24. The ROC curve analysis for good response, neutrophil-to-lymphocyte ratio (area under the curve (AUC) = 0.830), Disease Activity Score in 28 joints (AUC = 0.692), erythrocyte sedimentation rate (AUC = 0.671), C-reactive protein (AUC = 0.673).
NLR levels decrease after TNF inhibitor therapy in responders
Post-treatment biomarker levels at week 24 following the initiation of ADA therapy were systematically assessed and compared with baseline values, as summarized in Table 2. In the good responder group, statistically significant reductions were observed in NLR (p < 0.001). In contrast, among non-good responders, NLR levels remained largely unchanged (p = 0.067). These results indicate a differential inflammatory response to ADA therapy between responders and nonresponders, underscoring the potential use of NLR as a biomarker for predicting treatment response.
High baseline levels of NLR were associated with a better clinical response to ADA treatment
Stratification based on pretreatment NLR > 2.7 versus ≤2.7 revealed distinct therapeutic outcomes among ADA-treated patients. The high NLR cohort exhibited superior 24-week DAS28-ESR remission rates compared with the low NLR group (62.1% vs. 39.2%, p < 0.001), as shown in Figure 2(a). Although both NLR-low and NLR-high patients receiving ADA achieved greater improvements in DAS28 from baseline, NLR-high patients exhibited significantly greater improvements than NLR-low patients at earlier time points (Figure 2(b) and (c)). Notably, despite a similar initial trend in both groups, NLR-low patients did not exhibit such pronounced DAS28 improvements compared with their NLR-high counterparts over time. The improvement in DAS28 ESR from baseline was significantly greater in the NLR-high group than in the NLR-low group at this time point, with a mean change of 3.02 ± 0.09 versus 2.23 ± 0.10 (p < 0.001), as shown in Figure 2(c).
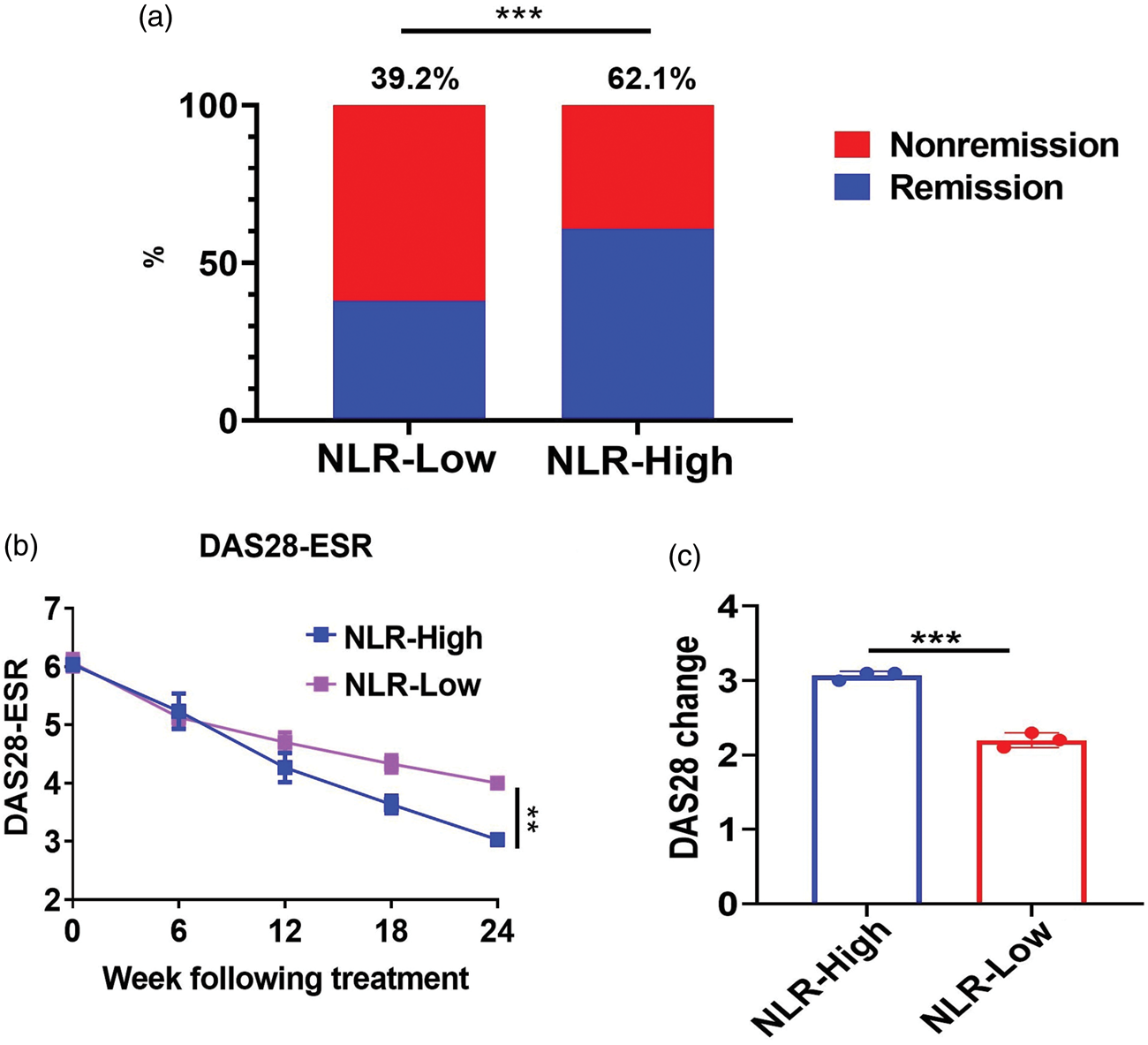
(a): A significantly higher proportion of patients in the high neutrophil-to-lymphocyte ratio (NLR) group achieved Disease Activity Score in 28 joints (DAS28) remission at 24 weeks compared to the low NLR group (62.1% vs. 39.2%, P = 0.032) following adalimumab (ADA) treatment. (b): The improvement in the DAS28 erythrocyte sedimentation rate was better in the high NLR group than in the low NLR group at 24 weeks following ADA treatment. (c): The changes in the DAS28 from baseline to 24 weeks of treatment following adalimumab therapy were assessed in the low and high NLR groups. *p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
The contemporary management of RA has shifted from palliative care to a target-driven therapeutic strategy, with randomized controlled trials consistently demonstrating improved clinical outcomes under this approach. 20 Nevertheless, a significant proportion of patients remain refractory to treatment, failing to achieve established disease activity thresholds such as DAS28 ≤ 3.2. Currently, there are two major limitations to clinical decision-making:21,22 (a) lack of reliable biomarker signatures to guide therapeutic interventions and (b) lack of standardized protocols for personalizing treatment based on the molecular characteristics of RA pathology. This gap in clinical tools is significant in light of the increasing availability of biologic agents and small-molecule DMARDs, alongside advancing precision medicine efforts aimed at tailoring therapies through a deeper understanding of interpatient heterogeneity in immune cell function and cellular interactions. 23 To the best of our knowledge, this is one of the first studies to specifically evaluate the association between baseline NLR and treatment response in a cohort of MTX-inadequate responder RA patients receiving ADA in combination with stable MTX.
This prospective cohort study identified NLR as a potential predictor of treatment response to ADA in patients with RA with inadequate response to MTX.11–13,24 Consistent with previous studies, 23 shorter disease duration, 21 higher NLR levels, 18 lower ESR, and higher baseline DAS28 were significantly associated with a good response to ADA therapy in patients with RA at week 24. 25 Critically, this study found that a high baseline NLR strongly predicted a good response to ADA therapy by week 24. Patients with high baseline NLR levels exhibited significantly elevated DAS28 and serum cytokines (IL-6 and TNF-α).
Emerging research has increasingly emphasized hematologic biomarkers, particularly the NLR, as clinically relevant indicators for both diagnosing RA and evaluating disease activity and severity.26–28 Although systemic inflammation in RA induces morphological and quantitative alterations in peripheral blood cells, these cellular components also actively participate in key pathophysiological processes.29,30 In the synovial microenvironment of inflamed joints, neutrophils contribute to disease progression through the secretion of TNF-α and release of chemokines such as chemokine (C-C motif) ligand 18 and B-cell activating factors, which facilitate the recruitment and activation of B and T lymphocytes, perpetuating chronic inflammation.16,26
Clinically, neutrophilia and thrombocytosis are frequently observed during active disease phases,28,31 whereas lymphopenia often accompanies disease progression, although its precise molecular mechanisms remain incompletely understood. 32 Given this reciprocal shift in myeloid and lymphoid lineages, the NLR is emerging as a robust composite marker reflecting systemic inflammatory burden in RA.11,33 Multiple studies have consistently demonstrated elevated granulocyte and platelet counts alongside reduced lymphocyte levels in patients with RA.13,34 The expansion of neutrophil populations is primarily attributed to enhanced cell survival mediated by upregulated anti-apoptotic proteins (e.g. Bcl-2 family members), increased stimulation of bone marrow hematopoietic precursors, and elevated granulocyte colony-stimulating factor levels. 24 Conversely, lymphocyte depletion is largely driven by apoptosis triggered by inflammatory cytokines through intrinsic and extrinsic signaling pathways, a hallmark of RA immunopathology.
Taylor et al. underscored NLR as a robust prognostic biomarker for predicting clinical response to Janus kinase inhibitor therapy in patients with RA. 18 In the study by Lee et al., elevated baseline levels of NLR and platelet-to-lymphocyte ratio (PLR) were significantly associated with an increased risk of non-response to anti-TNF-α agents at week 12, while a high pretreatment NLR independently predicted a greater likelihood of early treatment discontinuation. 24 Sargin et al. reported that changes in NLR and PLR levels before and after rituximab therapy were strongly correlated with DAS28-ESR fluctuations, revealing significant reductions in both ratios among responders, which indicates their importance as dynamic indicators of therapeutic efficacy. 35 Similarly, Boulos et al. demonstrated that baseline NLR levels effectively stratified outcomes in patients with RA receiving triple DMARD therapy, with nonresponders exhibiting significantly higher NLR values. 36 These findings are further corroborated by Lee et al., who showed that elevated baseline NLR levels are linked to diminished responsiveness to TNF antagonists, highlighting the role of systemic inflammation, as reflected by myeloid-to-lymphoid cell ratios, in modulating treatment outcomes across diverse RA therapeutic regimens. 24
The study results are consistent with those of previous research, demonstrating that a higher NLR level is significantly associated with a favorable clinical response to ADA therapy. Nevertheless, some studies present contradictory results. Koiwa et al. reported that pretreatment NLR lacked predictive utility for response to biologic agents in patients with RA, despite a confirmed correlation between NLR and DAS28. 13 These inconsistencies may arise from differences in study design and patient population characteristics. Koiwa et al. evaluated the association between baseline NLR and EULAR response at 6 months, whereas this study did not find a significant link between baseline NLR and EULAR-defined response to anti-TNF-α therapy at week 24. 13 This implies that the NLR may reflect rapid, transient changes in systemic inflammatory status, thereby limiting its predictive capacity to earlier treatment phases (e.g. within 12 weeks). Furthermore, Koiwa et al.’s study encompassed heterogeneous RA populations receiving various biologic therapies—including TNF inhibitors and abatacept—but did not adjust for key confounding variables such as disease duration, concomitant medications, or prior treatment exposure, which may have affected the strength of observed associations. 13 The NLR is correlated with disease activity in RA, potentially explaining the association between higher baseline NLR levels and enhanced short-term response to anti-TNF-α agents.12,18,37 Therefore, in addition to conventional markers of inflammation, the NLR may serve as a clinically accessible and dynamic prognostic indicator for early treatment response and long-term therapeutic persistence, although the underlying immunobiological mechanisms warrant further mechanistic investigation.
An interesting finding was that good responders had significantly lower baseline ESR but higher baseline NLR than nonresponders. This dissociation suggests that NLR may capture a different dimension of the inflammatory burden than conventional acute-phase reactants. Although ESR/CRP reflects systemic cytokine levels, NLR might more directly reflect the cellular immune phenotype, particularly the balance between innate (neutrophil-driven) and adaptive (lymphocyte-mediated) inflammation. The superior predictive value of NLR over ESR/CRP in our cohort may indicate that patients whose RA inflammation is more “neutrophil-centric” derive greater benefit from TNF-α blockade.
Notably, baseline serum levels of IL-6 and TNF-α were not significantly associated with treatment response. This is consistent with previous studies reporting that circulating concentrations of TNF-α and IL-6 lack reliability as predictive biomarkers for clinical outcomes following tocilizumab therapy.38,39 This contrasts with studies suggesting that elevated IL-6 levels may be linked to either improved therapeutic efficacy or poorer responses. 40 The discrepancies observed in the literature may stem from methodological heterogeneities, particularly the reliance on DAS28—a composite index with known psychometric and biological limitations—as a primary endpoint, as well as potential selection biases in patient enrollment.41,42 In this study, the majority of patients exhibited high disease activity at baseline, and IL-6 and TNF-α levels remained comparable across response strata both prior to ADA initiation and following treatment. These results reinforce the hypothesis that TNF-α is robustly expressed in both resolving and persistent synovitis, underscoring the pathophysiological significance of dysregulated prolonged TNF-α signaling in driving and sustaining acute and chronic immune-mediated inflammatory processes.
This study has several limitations. First, although it was a prospective study, the sample size was limited, and larger cohorts are needed to validate these findings. In this single-center prospective cohort, baseline NLR predicted 24-week ADA response with high accuracy (AUC: 0.830), outperforming DAS28, ESR, and CRP. However, these findings warrant cautious interpretation due to potential cohort-specific bias or overfitting. External validation in diverse, multi-center cohorts is essential to confirm NLR’s generalizability and robustness. Future work should explore combining NLR with clinical variables or other biomarkers in a composite score to improve prediction. Second, the low proportion of male participants limits the generalizability of the results with respect to sex-specific effects. Although the underlying mechanisms of RA remain unclear, previous studies have reported higher NLR levels in male patients with rheumatic diseases than in female patients. Therefore, the underrepresentation of males in this cohort may have constrained the statistical power to detect sex-based differences in treatment response. Furthermore, the absence of a control group restricts the ability to determine whether the identified predictive characteristics are specific to the ADA + MTX treatment regimen or applicable across other therapeutic approaches.
Conclusions
The findings of this study highlight NLR as a practical predictive biomarker for ADA response in patients with RA. Patients with high baseline NLR levels are more likely to respond well to TNF-α inhibitors than those with low baseline NLR levels, supporting its use for patient stratification. The NLR is calculated from routine blood tests, indicating that it can be easily adopted in clinical practice without additional diagnostics. Incorporating the NLR into regular assessments may improve treatment personalization, clinical outcomes, and patient-reported outcomes in RA.
Footnotes
Acknowledgments
Authors’ contributions
Jingru Zhu and Jiankang Hu conceived and designed the study. Senhua Dai and Yuhang Liu collected the data and performed the literature search. The clinical data analysis was conducted by Hu Na and Wei Peng.
Dening He and Chao He were involved in the writing of the manuscript. All authors have read and approved the final manuscript.
Availability of data and materials
The data generated in the present study will be made available upon reasonable request to the corresponding author.
Declaration of conflicting interest
The authors declare that they have no competing interests.
Funding
The study was supported by the Jiangxi Provincial Health Commission science and technology project plan (NO.202510929).