
Abstract
Barium-associated intestinal ischemia is a rare but life-threatening complication following upper gastrointestinal barium contrast examinations, with an incidence of less than 0.01%. Hepatic portal venous gas is a condition secondary to intra-abdominal lesions, such as intestinal ischemia and intestinal necrosis. When complicated by intestinal necrosis, the mortality rate of this condition can be as high as 50%–90%. Cases involving both barium-associated intestinal ischemia and hepatic portal venous gas are even rarer. We report the case of a 62-year-old male patient who underwent upper gastrointestinal barium contrast examination for evaluating potential gastrointestinal disorder. Eight hours after the procedure, he developed clinical symptoms, including abdominal pain, decreased blood pressure, and increased heart rate. Abdominal computed tomography revealed enteritis, with gas detected in the hepatic portal vein, superior mesenteric vein, and intestinal wall. After 12 h of active anti-infective treatment, the gas in the hepatic portal vein was absorbed, and the symptoms improved by the second day. The patient’s condition improved on the fourth day of treatment, and follow-up at 1 month confirmed complete recovery. Barium-associated intestinal ischemia is a medical emergency characterized by rapid infection and multiorgan involvement. Hepatic portal venous gas is an important indicator of underlying intra-abdominal pathology. Early anti-infective treatment and intensive care unit monitoring are critical for favorable outcomes.
Keywords
Introduction
Barium contrast studies are widely used in clinical practice for evaluating gastrointestinal (GI) disorders and are generally regarded as safe, noninvasive procedures. However, barium-associated intestinal ischemia, an inflammatory response induced by barium-related intestinal mucosal injury or impaired perfusion, remains a rare but potentially fatal complication. Barium peritonitis, defined as peritonitis caused by the extravasation of barium sulfate into the peritoneal cavity, has a reported mortality rate of approximately 30%–50%, and some studies suggest that the rate may exceed 60% without timely treatment. 1 Although barium sulfate is chemically inert, animal studies have shown that sterile intraperitoneal infusion of barium does not directly induce inflammation. 2 Nevertheless, it can lead to peritoneal adhesions and granuloma formation, eventually progressing to sepsis. 3
Hepatic portal venous gas (HPVG) is most commonly associated with intestinal ischemia, intra-abdominal infection, or abdominal trauma. Historically, the mortality rate of HPVG was extremely high, reaching 75% in 1978. However, advances in abdominal computed tomography (CT) and intensive care management have reduced the mortality rate to approximately 20%–30%. Nevertheless, HPVG remains a marker of severe abdominal pathology, and its co-occurrence with barium-associated intestinal ischemia further complicates prognosis.4–6 The combination of barium-associated intestinal ischemia and HPVG substantially increases the complexity of clinical diagnosis and treatment. To date, literature reports of barium-associated intestinal ischemia complicated by massive HPVG remain extremely limited. Most published case reports and retrospective studies have focused either on isolated barium-associated intestinal ischemia or HPVG resulting from other etiologies, such as bowel obstruction or mesenteric ischemia. Consequently, understanding of the clinical course, optimal diagnostic strategies, and therapeutic outcomes in patients with both conditions remains limited. Additionally, emphysematous gastritis should be considered in the differential diagnosis of this clinical presentation. 7 Emphysematous gastritis is a rare, life-threatening condition characterized by intramural gastric gas formation and may also be accompanied by HPVG, thereby mimicking the clinical manifestations observed in our patient. Furthermore, HPVG may occur in gastric disorders such as spontaneous gastric necrosis, which should also be considered during differential diagnosis. 7
Herein, we report a rare case of successful survival in a patient with barium-associated intestinal ischemia complicated by massive HPVG, with the aim of providing additional diagnostic and therapeutic evidence for clinicians managing similar cases. The reporting of this study conforms to the Case Report (CARE) guideline. 8
Case presentation
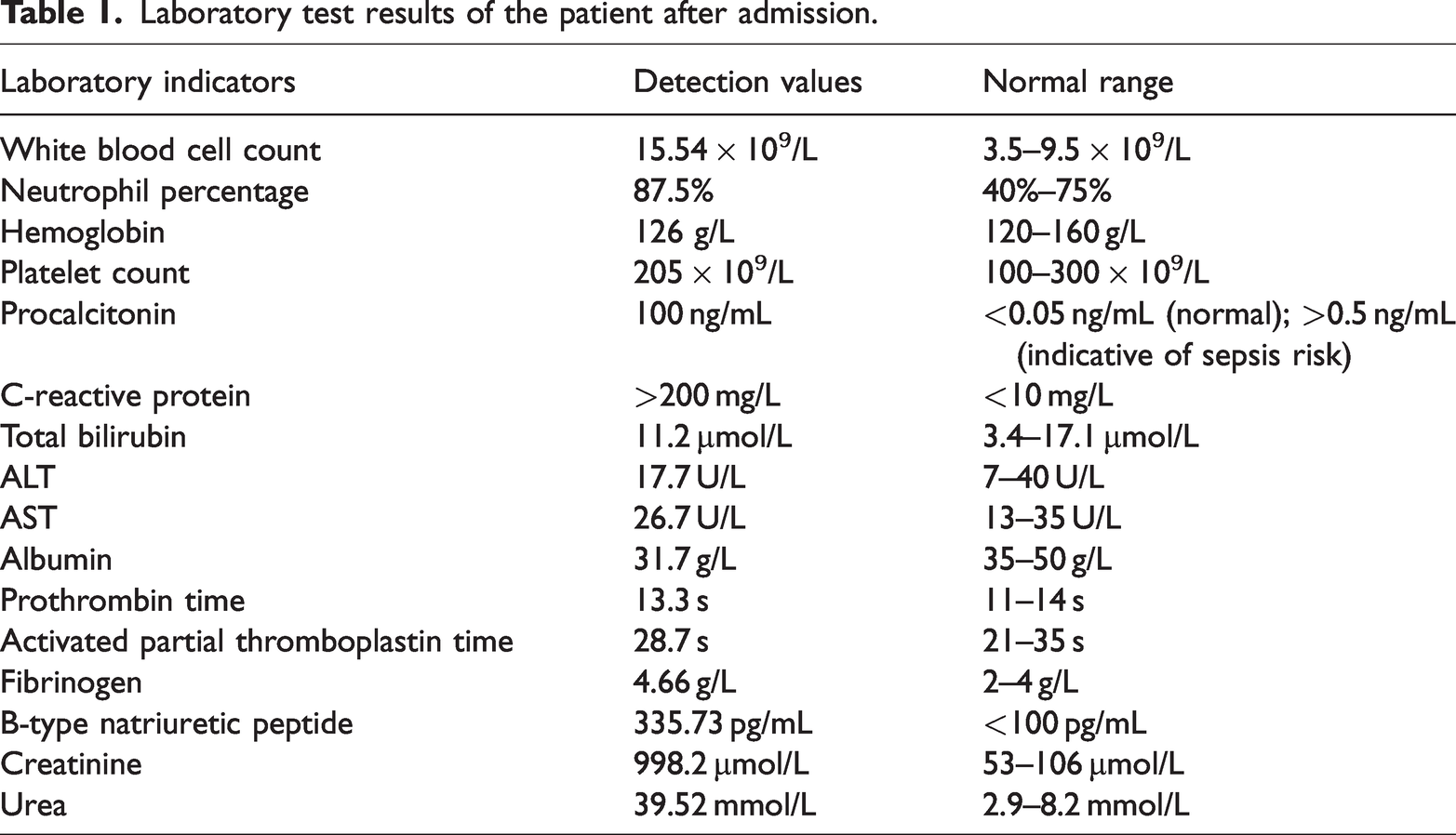
A patient in their early 60s was admitted to the Department of Critical Care Medicine, Daping Hospital, Army Medical University (Chongqing, China), in mid-2024 with a sudden onset of severe epigastric pain that occurred 8 h after undergoing an oral barium meal examination (performed to evaluate persistent upper abdominal discomfort of unknown etiology). On presentation, the patient appeared restless and in significant distress. Vital signs revealed a temperature of 37.0°C, heart rate of 99 bpm, respiratory rate of 18 breaths per minute, and blood pressure of 104/55 mmHg. The blood pressure before vasopressor administration was 74/37 mmHg. Oxygen saturation was 98% while receiving oxygen via nasal cannula with an FiO2 of 45%. Physical examination revealed marked epigastric tenderness with guarding and rebound tenderness in the periumbilical region. The patient’s laboratory test results on admission are presented in Table 1. The APACHE II score was calculated as 23, indicating severe illness. Abdominal CT (Figure 1(a) and (b)) revealed multiple strip-shaped hypodense lesions within the liver, with a CT attenuation value of −174 HU and a characteristic “tree-branch-like” morphology. Additionally, extensive gas accumulation was identified in the superior mesenteric vein and its distal branches in the mid-abdomen.
Laboratory test results of the patient after admission.
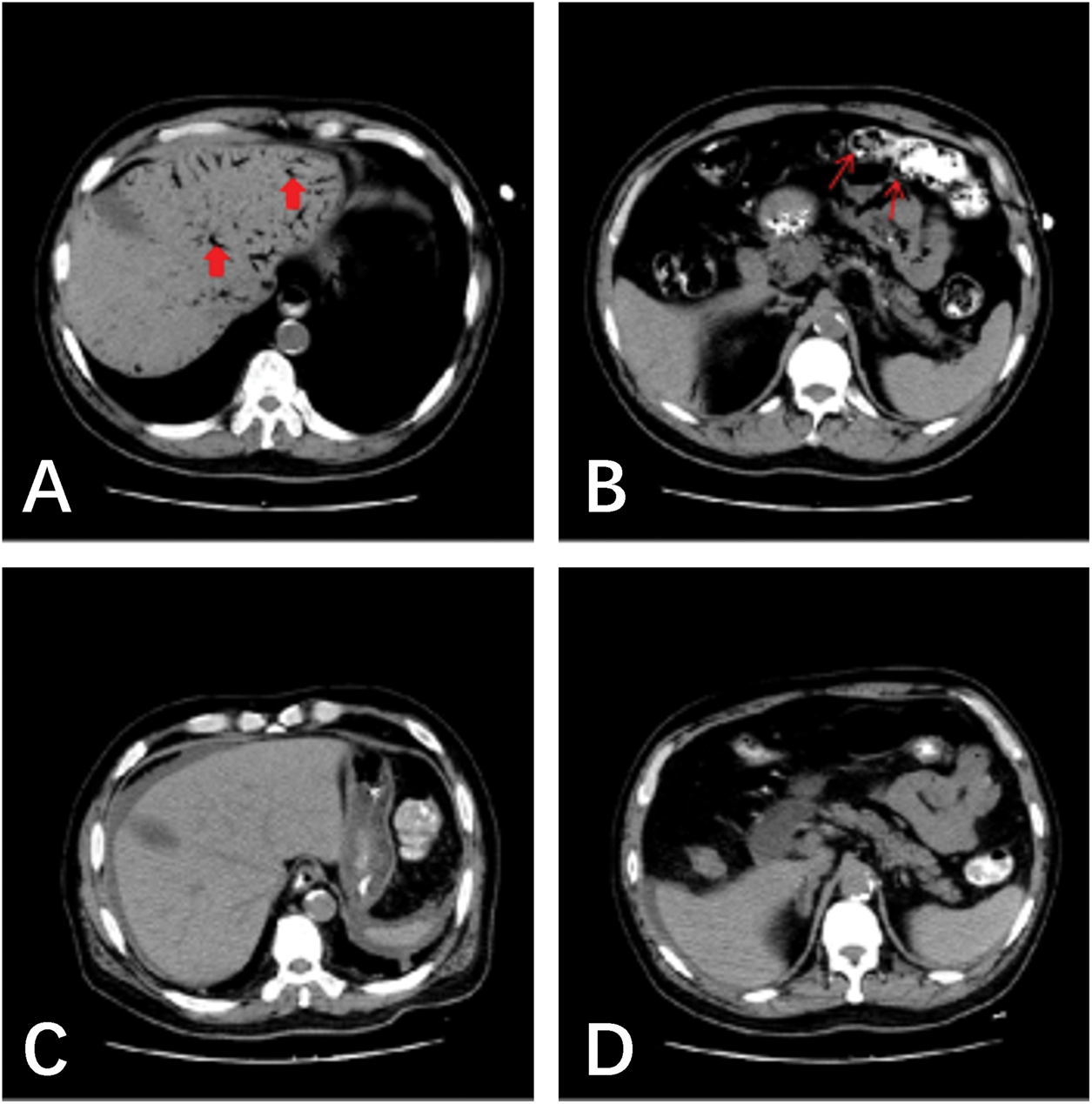
(a, b) Small bowel enteritis with gas in the portal vein, superior mesenteric vein, and intestinal wall (the “tree-branch” sign); (c, d) follow-up CT at 12 h showing resolution of pneumatosis.
Based on the clinical presentation, imaging findings, and laboratory data, the preliminary diagnoses included the following: (a) barium-associated intestinal ischemia; (b) HPVG and mesenteric venous gas; and (c) septic shock. Comorbidities included coronary heart disease, type 2 diabetes mellitus, stage 5 chronic kidney disease, grade 1 hypertension (high-risk group), and arteriosclerotic occlusive disease of both lower extremities.
Before treatment, written informed consent for treatment was obtained from the patient’s legal representative. Written informed consent for publication of this case report and the accompanying images was also obtained from the patient’s legal representative. We have de-identified all patient details to protect privacy.
After admission to the intensive care unit (ICU), the patient received a norepinephrine infusion at 0.2 µg/kg/min and empirical broad-spectrum antibiotic therapy with imipenem/cilastatin and teicoplanin. Supportive management included aggressive fluid resuscitation, anticoagulation, bowel rest (nil per os), and continuous gastrointestinal decompression. Given the patient’s multiple comorbidities and poor surgical tolerance, conservative treatment was initially pursued. After 12 h of supportive treatment in the ICU, repeat abdominal CT was performed to further assess the presence of intestinal ischemia or necrosis and determine whether surgical intervention was required. The imaging demonstrated a marked reduction in intraluminal barium and complete resolution of gas in the portal venous system and mesentery (Figure 1(c) and (d)). Over the next 4 days, the patient’s hemodynamic status gradually stabilized, and the abdominal pain improved significantly. The patient was subsequently transferred to another institution for continued treatment. Follow-up at 1 month confirmed complete recovery.
Discussion
Barium contrast studies are widely utilized in clinical practice for evaluating GI disorders and are generally regarded as safe and noninvasive procedures. However, barium-associated intestinal ischemia, an inflammatory response of the peritoneum resulting from barium-induced intestinal ischemia or perforation, remains a rare but potentially fatal complication. It occurs in approximately 0.02%–0.08% of lower GI barium enema cases, with a reported mortality rate of up to 50% when complicated by septic shock. In contrast, intestinal ischemia following upper GI barium studies is exceedingly rare, with an incidence of less than 0.01%. 9 Nevertheless, when it occurs, it represents a medical emergency requiring prompt ICU-level care and, in some cases, surgical intervention if there is extensive barium leakage.
The precise pathophysiologic mechanism by which barium sulfate induces intestinal ischemia or perforation remains incompletely understood. When barium enters the peritoneal cavity, it can lead to severe consequences. Animal studies have demonstrated that barium contamination is associated with significantly higher mortality rates than contamination with other water-soluble contrast agents, such as meglumine iothalamate, air, or normal saline. 10 This is believed to result from barium’s ability to cause hyperosmotic dehydration and chemical irritation and facilitate bacterial peritonitis. 11 Further investigations have shown that barium sulfate is a potent activator of phagocytes. Interestingly, although it activates resting phagocytes, it paradoxically impairs their bactericidal and fungicidal functions during active infection, thereby compromising host defenses. 12 Consequently, barium-associated intestinal ischemia may initially present with dehydration, intra-abdominal infection, and septic shock. If not thoroughly removed from the peritoneal cavity, residual barium can persist and trigger chronic inflammation, ultimately leading to fibrous adhesions, granuloma formation, and, in severe cases, mechanical intestinal obstruction. 13 However, in the absence of barium leakage into the peritoneal cavity, the risk of chronic sequelae such as fibrous adhesions or granuloma formation is relatively low, which supports the choice of conservative management in our patient.
The diagnosis of barium-associated intestinal ischemia is relatively straightforward and is primarily based on clinical findings. Patients typically present with acute abdominal symptoms, such as pain, vomiting, and distension, immediately after undergoing a barium contrast study. These symptoms are often accompanied by clinical signs of peritonitis and hemodynamic instability. Radiographic findings on abdominal X-ray or CT scan usually confirm the diagnosis. In the present case, although no intestinal perforation was detected on CT, the liver demonstrated the characteristic “tree-branch” sign, indicative of portal venous gas (PVG). First described in 1955, HPVG is an uncommon but serious radiologic finding associated with various intra-abdominal pathologies and carries a mortality rate of approximately 27.3%. The most common etiologies include intestinal ischemia or necrosis (53%–61.4%), GI obstruction or distension (9.0%–10.3%), GI infections (8.3%), and peptic ulcer disease (4.5%).14,15 Two primary mechanisms have been proposed to explain the formation of PVG. The first involves transmural invasion of gas-producing bacteria into the intestinal wall and mesenteric veins during episodes of intestinal ischemia or necrosis, leading to direct gas entry into the portal circulation. The second mechanism suggests that elevated intraluminal pressure, resulting from intestinal obstruction, overdistension, or trauma, causes mucosal injury and disruption of the epithelial barrier, thereby allowing gas to infiltrate the mesenteric venous system and reflux into the portal vein.6,16 Interestingly, despite its alarming radiographic appearance, the prognosis of PVG is often favorable. This may be attributable to the rapid absorption of intravascular gas and resolution of the underlying cause, with some reports describing complete disappearance of PVG within 3 h. 17
It is important to differentiate this condition from emphysematous gastritis, a rare entity that can present with similar clinical and radiologic features, including HPVG. 16 Emphysematous gastritis is characterized by intramural gastric gas formation, usually caused by gas-producing bacteria, and is associated with a high mortality rate. However, in our patient, CT showed no intramural gas within the stomach, and the primary abnormalities were localized to the small bowel and mesenteric veins, making emphysematous gastritis less likely. In addition, HPVG can occur in patients with gastric wall necrosis, which should also be excluded during differential diagnosis. 7
This patient had multiple underlying comorbidities, including long-term renal dialysis, malnutrition, and extensive arterial calcification, all indicative of a severely compromised systemic condition. The administration of barium likely precipitated intestinal ischemia, which was radiologically manifested as enteritis and impaired mucosal barrier function on CT. This disruption of the intestinal barrier may have facilitated the translocation of gas-producing bacteria into the intestinal wall and vasculature, resulting in intramural and mesenteric venous gas, which subsequently entered the hepatic portal circulation. The clinical triad of abdominal pain, septic shock, and peritoneal signs supported the diagnosis of severe intestinal ischemia and secondary peritonitis. Remarkably, this case captured imaging evidence of gas within the intestinal wall, mesentery, and hepatic portal vein, providing valuable diagnostic information. In clinical practice, however, such findings may be transient because intravascular gas can be rapidly absorbed. Consequently, repeat CT performed within a short interval may fail to detect PVG. For critically ill patients, point-of-care abdominal ultrasonography may serve as a valuable adjunctive tool for the early detection of intra-abdominal gas. 18
Management of barium-associated intestinal ischemia centers on three key principles: (a) early administration of broad-spectrum antibiotics, aggressive fluid resuscitation to correct circulatory shock, and organ-protective strategies to prevent multiorgan dysfunction; (b) surgical intervention to remove barium when significant peritoneal contamination is evident; and (c) meticulous postoperative care, including infection surveillance, hemodynamic stabilization, organ support, and nutritional therapy, all of which are critical determinants of patient survival.6,11,16 In the present case, prompt medical intervention enabled the early initiation of broad-spectrum antimicrobial therapy before overt intestinal perforation occurred, thereby effectively containing the infection. Intensive hemodynamic monitoring and carefully tailored fluid resuscitation helped maintain adequate tissue perfusion without exacerbating intestinal wall edema. Continuous renal replacement therapy was employed to remove circulating toxins and inflammatory mediators, thereby supporting homeostasis and mitigating the systemic inflammatory response. Concurrently, plaque stabilization and anticoagulation therapies may have contributed to the prevention of mesenteric and peripheral arterial thrombosis. Early ICU admission and comprehensive multidisciplinary management were instrumental in achieving a favorable clinical outcome in this critically ill patient. During follow-up, the patient was closely monitored for potential long-term complications, such as intestinal adhesions or granuloma formation; however, no such complications were identified at the 1-month follow-up.
Barium-associated intestinal ischemia (without overt perforation) is a medical emergency characterized by rapidly developing infection, a severe systemic inflammatory response, and frequent multiorgan involvement. Early recognition, timely initiation of broad-spectrum antimicrobial therapy, and coordinated multidisciplinary management in the ICU are critical for improving clinical outcomes and survival. It is important to emphasize that true barium peritonitis, which involves leakage of barium into the peritoneal cavity, typically requires surgical intervention. In the absence of frank perforation, however, early aggressive medical management may prevent the need for surgery and result in favorable outcomes.
Conclusion
Barium-associated intestinal ischemia is a medical emergency characterized by rapid-onset infection, a severe systemic inflammatory response, and frequent multiorgan involvement. Early recognition, timely initiation of broad-spectrum antimicrobial therapy, and coordinated multidisciplinary management in the ICU are critical for improving clinical outcomes and survival rates.
Footnotes
Acknowledgments
None.
Author contributions
Peng Xu contributed to the conceptualization of the study, data collection, and manuscript drafting. Xiaoyu Peng contributed to study supervision, data analysis, and manuscript revision. All authors have read and approved the final manuscript.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available because of privacy and ethical restrictions.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research was funded by the Chongqing Traditional Chinese Medicine Advantageous Specialty Program (Project No. 2025795).