
Abstract
Depth of anesthesia monitoring has become an important component of modern anesthetic practice. Electroencephalography-based technologies, such as the bispectral index, entropy, and Narcotrend, allow clinicians to assess the level of consciousness more objectively and guide anesthetic titration more precisely. This narrative review summarizes current evidence on the relationship between depth of anesthesia monitoring and major perioperative complications. Available evidence suggests that maintaining an appropriate depth of anesthesia reduces the risk of intraoperative awareness, hypotension associated with excessively deep anesthesia, postoperative delirium, and cognitive dysfunction. Electroencephalography-guided anesthesia appears particularly beneficial in older patients, individuals with cardiovascular disease, and other high-risk populations. Although several limitations remain, including algorithm variability and differential sensitivity to anesthetic agents, the integration of multimodal monitoring, brain network analysis, and artificial intelligence is expected to improve the accuracy and individualization of anesthesia management in the future.
Keywords
Introduction
The primary goal of general anesthesia is to maintain an appropriate depth of anesthesia (DOA), ensuring a delicate balance between “not too light” and “not too deep,” so that patients remain unconscious and pain-free, while stable physiological function is preserved throughout the surgery. 1 However, in clinical practice, deviations from the optimal DOA are common. Inadequate anesthesia may lead to intraoperative awareness, excessive sympathetic activation, hemodynamic instability, and increased postoperative pain, whereas excessively deep anesthesia may result in cardiovascular depression, organ hypoperfusion, delayed emergence, postoperative delirium (POD), and cognitive dysfunction, all of which may adversely affect patient outcomes.2–4
Traditional indicators used to estimate the DOA, such as blood pressure, heart rate, respiratory rate, and minimum alveolar concentration (MAC), are indirect surrogates of central nervous system (CNS) suppression and are readily influenced by individual variability, surgical stimulation, and pharmacologic factors, making them unreliable for real-time and accurate assessment of the brain’s anesthetic state. 5 In response, electroencephalography (EEG)-based monitoring technologies have been developed to provide a more objective assessment of the DOA. Tools such as the bispectral index (BIS), entropy, and Narcotrend analyze EEG signals to evaluate cortical activity and guide anesthetic titration more precisely.6,7
With increasing recognition of perioperative complications and the rise of precision anesthesia, EEG-based DOA monitoring has gained growing clinical relevance. It has shown potential for reducing intraoperative awareness, minimizing hypotension-related organ injury, improving emergence quality, and aiding in the prevention of POD and cognitive dysfunction.8,9 This narrative review aims to summarize current evidence regarding the relationship between DOA monitoring and perioperative complications, discuss its role and limitations in improving clinical outcomes, and highlight future directions for the development of individualized and multimodal anesthesia monitoring. This review was guided by the Scale for the Assessment of Narrative Review Articles (SANRA). 10
Literature search strategy
Given the broad scope of DOA monitoring across different perioperative outcomes, monitoring modalities, and patient populations, a narrative review approach was chosen to ensure a comprehensive and clinically oriented synthesis of the current evidence. Although this article is a narrative review, we performed a structured literature search to improve transparency and reproducibility. We searched the PubMed, Web of Science, Embase, and Cochrane Library databases for relevant studies. The main keywords included “DOA,” “bispectral index,” “BIS,” “processed electroencephalography,” “entropy,” “Narcotrend,” “intraoperative awareness,” “postoperative delirium,” “postoperative cognitive dysfunction,” “hypotension,” and “ICU sedation.” We prioritized systematic reviews, meta-analyses, randomized controlled trials, and major observational studies published in peer-reviewed journals. Reference lists of relevant articles were also manually screened to identify additional studies. Non-English articles, conference abstracts without full texts, duplicate publications, and studies with limited relevance to the clinical topic were generally excluded.
Concept and methods associated with DOA
Definition of DOA
DOA generally refers to the degree of CNS suppression induced by general anesthetics. It primarily encompasses two interrelated dimensions: hypnosis and analgesia. Hypnosis involves the loss of consciousness and responsiveness to external stimuli, while analgesia reflects the suppression of nociceptive perception and physiological reactions to noxious input. Together, these dimensions determine the overall functional state of the brain during anesthesia. Recent studies have shown that DOA is closely related not only to cortical EEG dynamics but also to alterations in brain network connectivity and responsiveness to surgical stimulation.11–13 Maintaining an appropriate DOA within a safe range is essential for ensuring surgical safety and minimizing perioperative complications.14–16
Traditional monitoring methods
Traditionally, in clinical practice, the DOA is inferred from physiological signs and observable responses such as blood pressure, heart rate, respiratory rate, pupillary reflexes, and MAC. Although these parameters can be readily obtained, they are only indirect indicators of CNS suppression and can be significantly influenced by multiple factors, including surgical stimulation, pain, anesthetic type, temperature, electrolyte imbalance, and concurrent medications. 17 For instance, increases in the heart rate or blood pressure do not necessarily indicate light anesthesia, while β-blockers may mask sympathetic responses. More importantly, these physiological indicators cannot directly reflect cortical activity, making it difficult to determine the precise moments of loss and recovery of consciousness.18,19 With the emergence of precision anesthesia, reliance solely on traditional vital signs is no longer sufficient for accurate, real-time, and objective evaluation of the DOA. 16
EEG-based DOA monitoring
To overcome the limitations associated with the use of conventional indicators, EEG-based DOA monitoring has gained widespread clinical use. The BIS remains the most commonly used tool; it analyzes EEG signals in both frequency and phase domains to derive a numerical index ranging from 0 to 100, with values between 40 and 60 generally considered optimal for surgical anesthesia.18,20 The entropy index—including state entropy and response entropy (RE)—quantifies the complexity of EEG signals to assess cortical inhibition while detecting changes in the electromyographic (EMG) activity that may indicate emerging arousal. 21 Narcotrend, another EEG-based system, classifies anesthesia depth into sleep-like stages, providing an intuitive display of the anesthetic state. 22
In recent years, quantitative electroencephalography (qEEG) analysis has allowed the extraction of advanced parameters such as phase synchronization, spectral power distribution, and functional connectivity metrics. These features enable more comprehensive characterization of neural dynamics under anesthesia and may better reflect the neurophysiological correlates of consciousness, representing an active area of current research. 23
Analgesia depth monitoring
DOA assessment should not focus solely on the hypnotic component; inadequate analgesia can trigger sympathetic overactivation, hemodynamic instability, intraoperative nociceptive memory formation, and increased postoperative pain. Consequently, monitoring the depth of analgesia has become an important complement to anesthetic management. 24
The Analgesia Nociception Index (ANI), derived from heart rate variability (HRV), evaluates autonomic nervous system responses to noxious stimuli and helps determine the sufficiency of analgesia.25,26 The Nociception Level Index (NOL) integrates multiple physiological signals, including photoplethysmography (PPG), skin conductance, and pulse wave amplitude, to provide a composite assessment of nociceptive balance.27,28 Combining hypnotic/sedative monitoring with analgesic depth monitoring allows a more comprehensive and individualized anesthesia management approach, reducing surgical stress and lowering the risk of perioperative complications.
Intraoperative awareness
Intraoperative awareness is one of the most concerning complications associated with general anesthesia and remains a major issue in anesthetic safety. It refers to the patient’s recall of events during the surgery, such as sounds, touch, or even pain, despite intended general anesthesia. For some patients, this can be a deeply distressing experience and may be followed by lasting psychological consequences, including anxiety, insomnia, nightmares, avoidance behavior, and post-traumatic stress disorder. 29 Because of its potential impact on both perioperative experience and long-term mental health, intraoperative awareness is widely regarded as one of the most serious adverse events in anesthesia.
The risk of accidental awareness is higher in several well-recognized clinical situations. One of the most important is total intravenous anesthesia (TIVA), wherein there is no continuously measurable end-tidal anesthetic concentration (ETAC) comparable with MAC. Awareness may also occur when drug infusion is interrupted or when the anesthetic dose is insufficient. In addition, the use of neuromuscular blocking agents can make inadequate hypnosis harder to detect because patient movement is suppressed. The risk may be even greater in patients with hemodynamic instability who require vasopressor support as anesthetic doses are often deliberately reduced to maintain cardiovascular stability.30–32
With the increasing use of EEG monitoring in clinical anesthesia, DOA management based on processed EEG parameters, particularly strategies targeting a BIS of 40–60, has been examined in several clinical studies. Overall, the main trial-based evidence supporting the use of the BIS to prevent the risk of intraoperative awareness comes from two settings: (a) high-risk cases and (b) TIVA. In the landmark B-Aware trial, 2463 adult patients at high risk of intraoperative awareness were enrolled, and the incidence of definite awareness was lower in the BIS-guided group than in the routine care group (2/1225 vs. 11/1238), suggesting that BIS-guided anesthesia reduces the risk of definite awareness in high-risk patients. 33 In addition, a multicenter randomized double-blind trial focused on TIVA, which included 5228 patients (2919 in the BIS group and 2309 in the control group), confirmed awareness among 4/2919 patients in the BIS group and 15/2309 in the control group; both possible awareness and dreaming were also less frequent in the BIS group. 34
Available evidence also suggests that the clinical benefit of BIS is not consistent across all anesthetic settings. In the B-Unaware trial, Avidan and colleagues compared a BIS-guided protocol with a protocol based on end-tidal anesthetic gas (ETAG) concentrations. In total, 967 patients were included in the BIS group and 974 in the ETAG group for the final analysis; definite awareness occurred in 2 patients in each group, with no significant difference between the groups. 35 This was followed by the Bispectral Index or Anesthetic Gas to Reduce Explicit Recall (BAG-RECALL) trial, in which BIS-guided management was compared with a protocol based on age-adjusted ETAC. Among patients who completed postoperative interviews, definite awareness was reported in 7/2861 patients (0.24%) in the BIS group and 2/2852 patients (0.07%) in the ETAC group, reiterating no clear advantage of BIS over ETAC-guided management. 36 Similar results were reported by Mashour et al. 37 in their large comparative-effectiveness randomized trial involving an unselected surgical population that analyzed 18,836 patients, including 9376 in the BIS protocol group and 9460 in the anesthetic concentration protocol group. Definite awareness occurred in two patients in each group, with no significant difference observed. Taken together, these studies suggest that under inhalational anesthesia, when ETAG or ETAC is already being monitored in a structured and rigorous manner, there is limited benefit offered by the additional use of the BIS. Overall, the BIS may be more useful in specific high-risk situations, particularly in patients at increased risk of intraoperative awareness and those receiving TIVA; however, its added clinical value appears less consistent when anesthetic concentration is already being carefully monitored. Key clinical trial evidence has been summarized in Table 1.
Key clinical trials of BIS-guided anesthesia for prevention of intraoperative awareness.
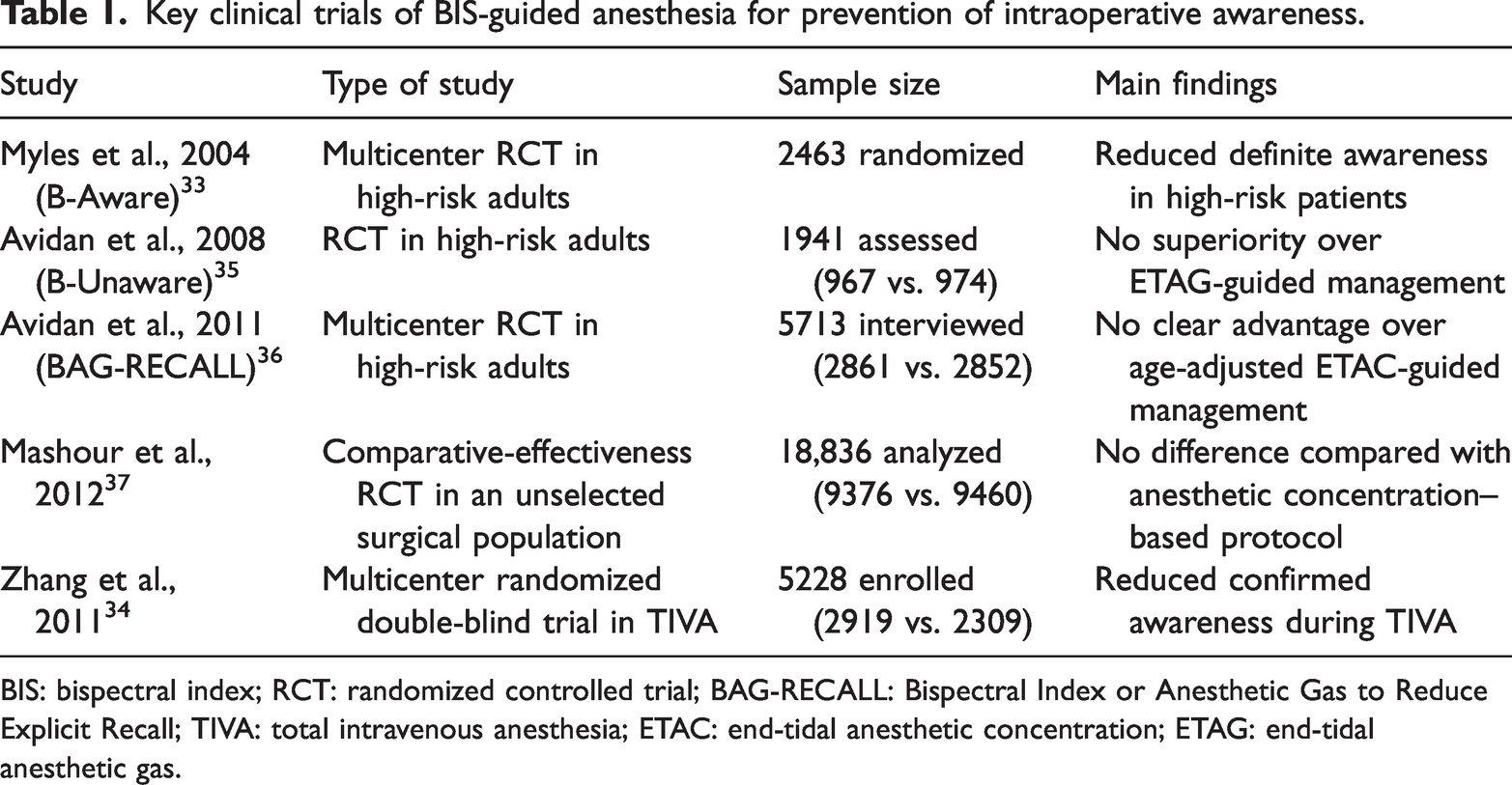
BIS: bispectral index; RCT: randomized controlled trial; BAG-RECALL: Bispectral Index or Anesthetic Gas to Reduce Explicit Recall; TIVA: total intravenous anesthesia; ETAC: end-tidal anesthetic concentration; ETAG: end-tidal anesthetic gas.
Excessive anesthesia, hypotension, and organ hypoperfusion
Excessive anesthesia is an important cause of intraoperative hypotension and organ hypoperfusion. It is usually reflected by persistently low BIS values, especially <40, or by obvious EEG suppression such as burst suppression. 38 These findings suggest excessive cortical depression and are often accompanied with anesthetic overdose. In this setting, myocardial contractility may be reduced, peripheral vascular tone may decrease, and both mean arterial pressure (MAP) and cardiac output may reduce, ultimately compromising tissue and organ perfusion. 39 This problem is particularly relevant in older patients and those with poor cardiovascular reserve, both of whom exhibit poor tolerance to perfusion-related insults. 29
Current evidence suggests that hypotension associated with excessively deep anesthesia is not merely a transient intraoperative fluctuation but is also be associated with worse postoperative outcomes. Based on their large, perioperative cohort study, Sessler et al. reported that the simultaneous presence of low MAP, BIS, and anesthetic concentration—the so-called “triple low” state—is associated with prolonged hospital stay and increased 30-day mortality, indicating the potential harm caused by deep hypnosis combined with hypotension. 40 Monk et al. also reported that cumulative deep hypnotic time, reflected by low BIS values, together with intraoperative hypotension, independently predicts 1-year mortality after non-cardiac surgery. 41 In addition, large observational analyses have shown a dose–response relationship between the depth and duration of intraoperative hypotension and major organ injury, including acute kidney injury and myocardial injury. In particular, the risk appears to increase further when the MAP remains <55 mmHg for a prolonged period. 42 Taken together, these findings suggest that hypotension during excessively deep anesthesia contributes to inadequate perfusion of vital organs and poorer perioperative outcomes.
In this context, the main value of BIS monitoring is in helping anesthesiologists identify excessive anesthesia early and adjust the anesthetic dosing accordingly, thereby reducing unnecessary drug exposure and preventing further deterioration in blood pressure and organ perfusion. Compared with reliance on indirect signs such as blood pressure and heart rate alone, BIS provides a more direct reflection of the brain’s response to anesthetic agents and is therefore more useful for preventing excessively deep anesthesia. Some clinical studies support this view. Nair et al. also reported that compared with standard clinical management, BIS monitoring is associated with lower sevoflurane consumption, shorter emergence and extubation times, and more stable MAP. 43 Overall, the clearest advantage of BIS is in its ability to reduce anesthetic overdose and prevent excessively deep anesthesia, while any protective effect on hypotension and organ hypoperfusion is probably best understood as a downstream consequence of its primary role. Key clinical evidence has been summarized in Table 2.
Summary of studies on anesthesia depth monitoring and intraoperative hypotension.
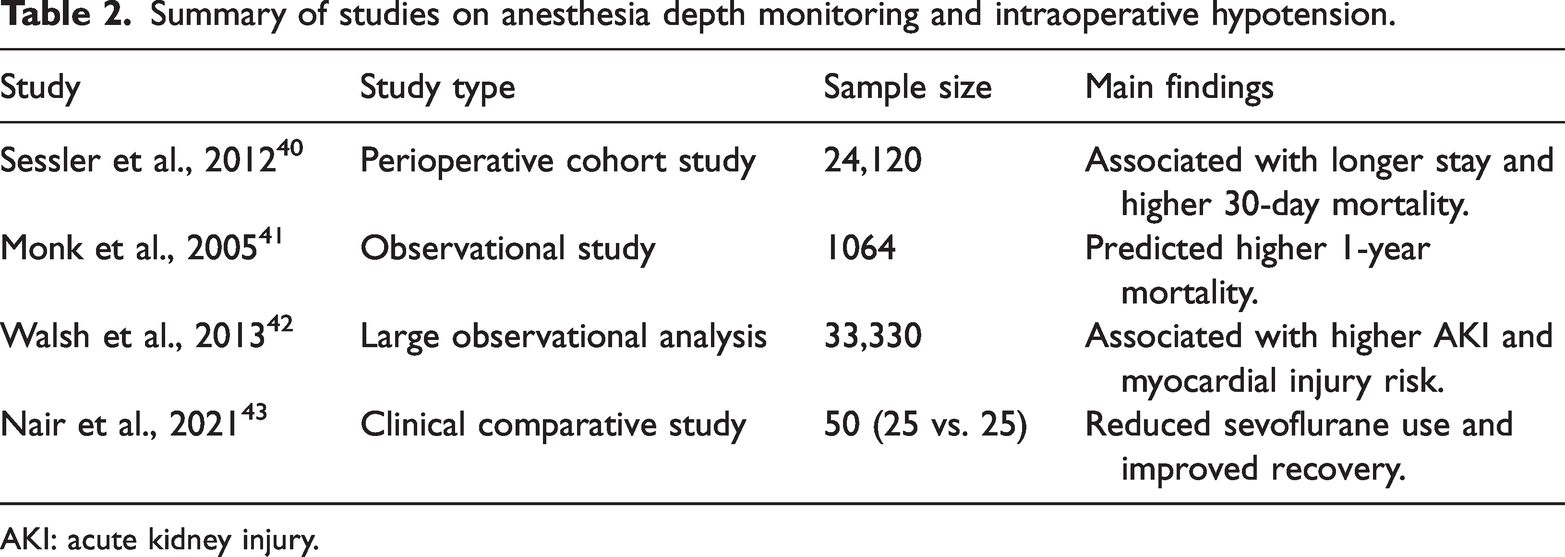
AKI: acute kidney injury.
POD and postoperative cognitive dysfunction (POCD)
POD and POCD are among the most common and consequential neurological complications in the perioperative period, particularly prevalent among older surgical patients. POD typically occurs within hours to days after surgery and is characterized by acute fluctuations in consciousness, inattention, and cognitive disorganization, whereas POCD manifests weeks to months postoperatively, presenting as impairments in memory, attention, and executive function. 44 These complications not only prolong hospitalization and increase healthcare costs but are also strongly associated with higher risks of postoperative falls, long-term functional decline, and mortality. 8
A growing body of evidence has established a close link between the DOA and postoperative neurocognitive outcomes. Excessive anesthesia can markedly reduce cerebral blood flow and impair oxygen metabolism, resulting in cerebral hypoperfusion and metabolic suppression, both of which increase the risk of neuronal dysfunction and injury. The occurrence of EEG burst suppression has been associated with a higher risk of POD in pooled clinical evidence, indicating profound cortical inhibition and low cerebral metabolic activity. 45 Furthermore, anesthetic exposure and surgical trauma can induce central neuroinflammation, impairing neuronal connectivity, reducing synaptic plasticity, and promoting inflammatory-mediated cognitive dysfunction. 46
Recent clinical evidence supports the protective role of EEG-guided anesthesia in reducing the incidence of postoperative neurocognitive complications. Based on their systematic review and meta-analysis, Bocskai et al. reported that BIS-guided anesthesia is associated with a lower risk of POD on postoperative day 1 and a reduced incidence of POCD at 12 weeks postoperatively. 47 In addition, a systematic review and meta-analysis focusing on processed EEG–guided general anesthesia has reported a reduction in POD compared with usual care across pooled trials. 48 Chen et al. conducted a randomized controlled trial in which maintaining BIS values between 40 and 60 decreased the incidence of delayed neurocognitive recovery (DNR) and postoperative neurocognitive disorder (PND), although it did not significantly change the POD incidence. 49
A larger meta-analysis by Ling et al. involving 5392 patients further suggested that lighter anesthesia (higher BIS targets) was associated with a lower risk of POD and POCD at 3 months postoperatively compared with deeper anesthesia; however, the authors noted heterogeneity and limited certainty for some endpoints. 2 Consistent with these findings, the results of a randomized trial conducted by Radtke et al. 50 demonstrated that DOA monitoring reduced the incidence of POD; however, no significant differences were observed in the POCD outcomes between the groups. 51
These studies collectively suggest that EEG monitoring reduces neurocognitive complications by avoiding excessively deep anesthesia and limiting EEG suppression while improving hemodynamic and cerebral perfusion stability. Clinically, intraoperative EEG suppression itself has been shown to predict POD risk. Fritz et al. reported that greater duration of intraoperative EEG suppression was independently associated with higher odds of POD in an observational cohort. 52 These findings are consistent with the key clinical evidence summarized in Table 3.
Summary of studies on EEG/BIS monitoring and postoperative neurocognitive outcomes (POD/POCD).

BIS: bispectral index; DNR: delayed neurocognitive recovery; PND: postoperative neurocognitive disorder; EEG: electroencephalography; POD: postoperative delirium; POCD: postoperative cognitive dysfunction; RCT: randomized controlled trial.
Respiratory and emergence-related complications
Excessive DOA not only affects the cardiovascular system but also produces significant respiratory depression. Overdosage of anesthetic agents reduces ventilatory drive, which may lead to diminished minute ventilation and carbon dioxide (CO2) retention in the early postoperative period. 53 Simultaneously, the tone of respiratory and upper airway muscles decreases, diaphragmatic motion becomes restricted, and residual neuromuscular blockade may further exacerbate respiratory suppression, impairing the recovery of spontaneous ventilation. 54 This effect is particularly pronounced in older patients and those with limited pulmonary reserve who are at a higher risk for delayed respiratory recovery, extubation difficulty, and postoperative hypoxemia. 53
In recent years, the association between the DOA and postoperative pulmonary complications (PPCs) has drawn increasing attention. Several clinical studies have demonstrated that perioperative respiratory impairment is often accompanied with reduced tidal volume and alveolar hypoventilation, which contribute to atelectasis formation, impaired oxygenation, and a higher incidence of PPCs. Based on their randomized controlled trial, Cheng et al. reported that applying moderate positive end-expiratory pressure (PEEP, 5 cmH2O) improves lung mechanics and reduces atelectasis during robot-assisted laparoscopic prostatectomy. 55 Similarly, Li et al. reported that high-flow nasal cannula oxygen inhalation during anesthesia recovery improves oxygenation and reduces hypoxemia in older patients. 56
EEG-based DOA monitoring may help reduce respiratory depression during emergence and facilitate earlier recovery of spontaneous breathing. In a randomized controlled trial involving 45 patients undergoing major abdominal surgery, Persec et al. reported that BIS-guided anesthesia significantly shortens the extubation time compared with routine care (17.5 vs. 75 min, p < 0.001), although no significant difference was observed in the total anesthetic consumption. 57 Similarly, in a randomized study involving 60 patients undergoing sevoflurane-based general anesthesia, Shukla et al. found that the time to tracheal extubation was shorter in the BIS group than in the ETAG-guided group (308.77 ±20.48 s vs. 377.90 ± 25.06 s, p < 0.001), with lower sevoflurane concentrations used in the BIS group at multiple time points (p = 0.001). 58
More recent evidence has also suggested that BIS-guided management improves the quality of emergence. Based on their randomized controlled trial, Zhang et al. reported that BIS-guided sedation with dexmedetomidine and propofol reduces coughing and airway reactions during extubation and lowers the peak expiratory flow during recovery, resulting in smoother emergence. 59 These findings are consistent with the key clinical evidence summarized in Table 4.
Clinical evidence on anesthesia monitoring and prevention of respiratory and emergence-related complications.
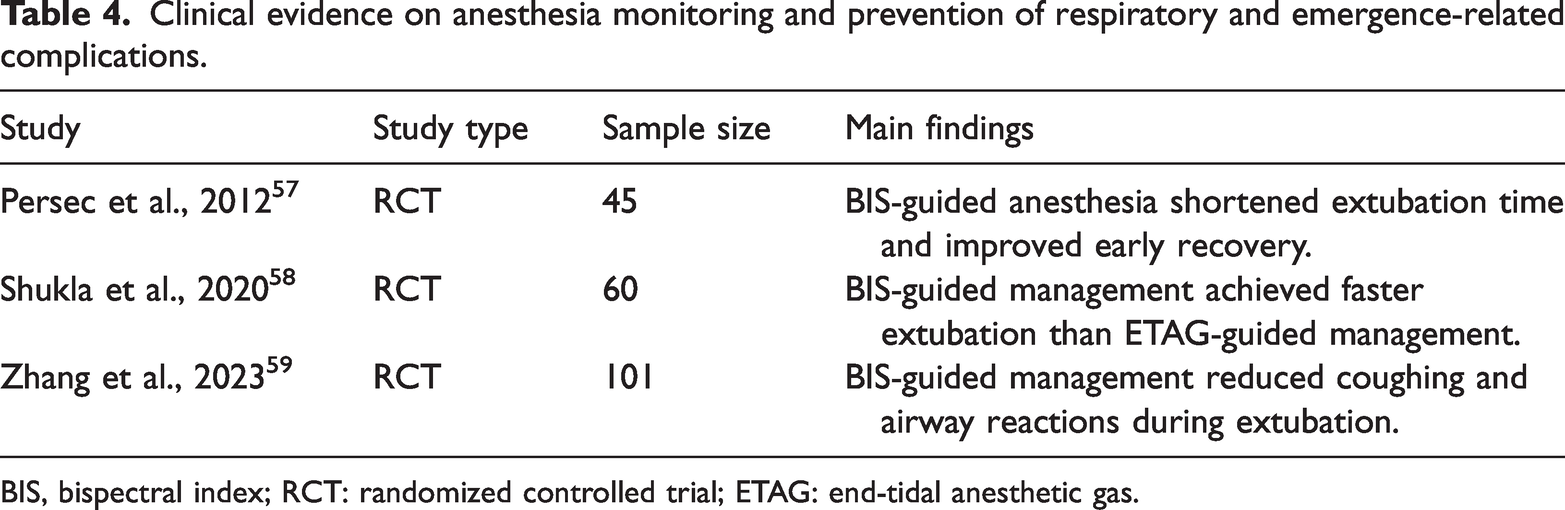
BIS, bispectral index; RCT: randomized controlled trial; ETAG: end-tidal anesthetic gas.
Intensive care unit (ICU) sedation–related complications
In the ICU, sedation is an essential component of patient management, enabling mechanical ventilation, relieving anxiety and pain, and maintaining physiological stability during life support. However, deep or excessive sedation remains common in clinical practice and is closely associated with multiple serious complications. Deep sedation can obscure neurological changes, delaying recognition of consciousness disorders or brain injury, and has been identified as an independent risk factor for ICU delirium. ICU delirium is an acute form of brain dysfunction linked to increased in-hospital mortality, long-term cognitive decline, and deterioration in quality of life. 60
Studies have consistently shown that early deep sedation is associated with higher mortality, prolonged mechanical ventilation, and extended ICU length of stay. A systematic review and meta-analysis involving mechanically ventilated patients conducted by Stephens et al. has demonstrated that deeper (or early deep) sedation strategies are associated with worse clinical outcomes, whereas lighter sedation is linked to shorter ventilation time and ICU stay and lower mortality risk. 60 In addition, a prospective ICU cohort study has suggested that profound EEG suppression (e.g. burst suppression) during propofol-based deep sedation is associated with subsequent delirium and increased longer-term mortality, supporting the concept that excessive cortical suppression reflects harmful brain-state vulnerability in critical illness. 61
In recent years, EEG-based monitoring of sedation depth has been increasingly used in ICU sedation management. EEG provides an objective assessment of cortical suppression induced by sedative agents, thereby helping clinicians avoid empirically driven overdosing and unnecessary deep sedation. Based on their randomized clinical trial, Huespe et al. reported that compared with usual care, BIS-guided deep sedation reduces the overall sedative exposure, including exposure to propofol and/or benzodiazepines. Although the overall difference in delirium- and coma-free days was not statistically significant, the study supports BIS/EEG monitoring as a practical strategy to reduce sedative burden and help prevent inadvertent over-sedation, particularly in patients who require prolonged deep sedation. 62 Similarly, a randomized study by Olson et al. has demonstrated that in critically ill ICU patients, BIS-assisted sedation monitoring reduces the total amount of sedatives required to achieve the same clinical level of sedation and shortens recovery time, suggesting that BIS use helps optimize sedative use. 63 Consales et al. further reported that in deeply sedated ICU patients, BIS use is able to distinguish different degrees of cortical suppression even when clinical sedation scores are similar, indicating an added value in identifying excessive sedation that may not be readily recognized with bedside clinical assessment alone. 64 Wang et al. 65 also reported that in mechanically ventilated patients, the actual occurrence of deep sedation is often greater than expected clinically, and that BIS, particularly when combined with post-stimulation assessment, aids in the detection of unintentional over-sedation. Overall, the main value of BIS in the ICU is in helping clinicians recognize and prevent excessive sedation and reducing unnecessary sedative exposure, whereas its direct impact on longer-term clinical outcomes requires further investigation. These findings are consistent with the key clinical evidence summarized in Table 5.
Key clinical studies evaluating EEG/BIS-guided sedation and ICU sedation-related complications.

BIS: bispectral index; EEG: electroencephalography; ICU: intensive care unit; RR: relative risk
Clinical value of DOA monitoring in unique populations
Different patient populations exhibit substantial variations in anesthetic drug metabolism, physiological reserve, and neural vulnerability, making them more sensitive to changes in the DOA. Therefore, DOA monitoring has clinical importance in these high-risk or physiologically distinct groups.
In older patients, reduced cerebral reserve and weakened neural network connectivity increase susceptibility to deep anesthesia and EEG burst suppression—patterns strongly associated with POD and POCD. In their systematic review and meta-analysis, Shi et al. reported that BIS- and Narcotrend-guided anesthesia is associated with a lower risk of POCD in older patients (reported pooled effect size indicating benefit). 66 Similarly, Qi et al. reported that Index of Consciousness (IoC) monitoring during general anesthesia in older patients is associated with better postoperative rehabilitation-related outcomes, supporting the value of processed EEG guidance in this population. 8 A recent study by Shi et al. has also suggested that BIS-targeted anesthetic management can improve early recovery quality, as measured using the Quality of Recovery-15 (QoR-15) scale, in older patients undergoing laparoscopic surgery without significant safety concerns. 67 Furthermore, a randomized trial by Evered et al. (BALANCED substudy) evaluated DOA strategies in older adults and has provided clinical evidence linking depth-targeted management to postoperative neurocognitive outcomes. 68
In patients with cardiovascular disease, maintaining appropriate DOA is critical to prevent excessive myocardial depression and peripheral vasodilation. Evidence from cardiac-surgical populations indicates that very deep hypnotic states (as indicated by low BIS values)—especially when combined with hypotension—are associated with worse postoperative outcomes, highlighting the importance of depth monitoring in hemodynamically fragile patients. 69 In older adults undergoing cardiac surgery, the ENGAGES-Canada randomized trial tested processed EEG–guided strategies and has provided high-quality evidence supporting the feasibility and clinical impact of EEG-guided care in this high-risk cardiovascular setting. 70 Additionally, BIS-guided titration approaches during cardiac anesthesia induction/maintenance have been investigated as a method of optimizing dosing and hemodynamic stability in patients with limited cardiac reserve. 71
In pediatric patients whose neural systems are still developing, sensitivity to the DOA is markedly heightened. Beekoo et al. compared EEG/BIS–related characteristics across age groups and highlighted that pediatric EEG patterns differ substantially, implying that processed indices may need age-specific interpretation and that direct EEG information can be valuable. 72 Moreover, the GAS trial (Davidson et al.) has provided landmark randomized evidence on neurodevelopmental outcomes after early-life anesthesia exposure, underscoring the importance of careful anesthetic management in pediatric patients. 73
In obese individuals, increased drug distribution volume and accumulation make conventional dosing models prone to excessive anesthesia. In a randomized controlled trial, Zhang et al. compared deeper and lighter hypnotic targets (BIS ∼35 vs. 50) in obese surgical patients and have reported differences in postoperative pain and recovery-related outcomes, supporting the concept that depth targeting may influence patient-centered endpoints. 74 From a pharmacologic and dosing standpoint, Ingrande and Lemmens summarized how morbid obesity alters anesthetic dosing requirements, providing the rationale for objective monitoring to avoid over- or under-dosing. 75 Finally, Gaszynski et al. studied the DOA and anesthetic requirements in obese patients under different anesthetic techniques with BIS-based assessment and have provided evidence supporting the clinical relevance of depth monitoring in this group. 76 These findings are consistent with the key clinical evidence summarized in Table 6.
Key clinical studies evaluating the value of anesthesia depth monitoring in unique patient populations.
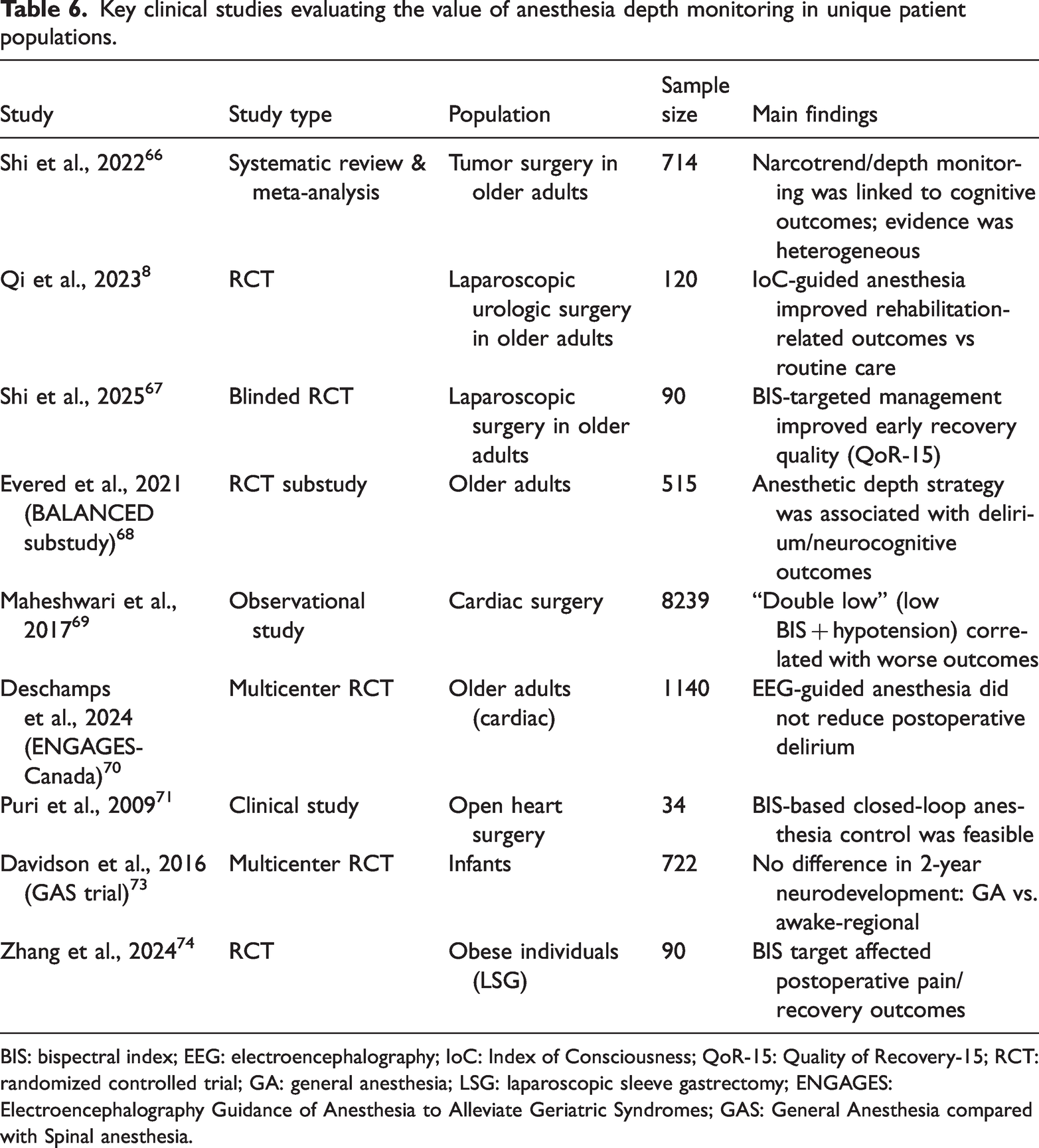
BIS: bispectral index; EEG: electroencephalography; IoC: Index of Consciousness; QoR-15: Quality of Recovery-15; RCT: randomized controlled trial; GA: general anesthesia; LSG: laparoscopic sleeve gastrectomy; ENGAGES: Electroencephalography Guidance of Anesthesia to Alleviate Geriatric Syndromes; GAS: General Anesthesia compared with Spinal anesthesia.
Compared with previous reviews that have often focused on a single monitoring modality or a specific perioperative outcome, this narrative review provides a broader synthesis of current evidence on DOA monitoring across multiple clinically relevant domains, including intraoperative awareness, hypotension-related organ injury, postoperative neurocognitive complications, respiratory events, and ICU sedation-related adverse outcomes. In addition, this review emphasizes the relevance of DOA monitoring in high-risk populations and discusses emerging directions such as multimodal monitoring, brain network analysis, and artificial intelligence. Therefore, this review adds to the literature by offering a more integrated clinical perspective on the current value, limitations, and future developments in DOA monitoring.
Limitations and controversies
Although DOA monitoring is being become increasingly used in clinical practice to reduce intraoperative awareness and optimize anesthetic dosing, certain limitations and controversies remain.
First, EEG-based DOA indices—such as the BIS, entropy, and Narcotrend—reflect only the statistical features of cortical electrical activity. However, consciousness arises from complex interactions across cortical and subcortical neural networks. Consequently, EEG-derived indices may not always accurately represent the true state of consciousness. 77 In addition, signal artifacts caused by EMG interference, electrocautery, and environmental noise remain major technical challenges during monitoring. Kim et al. compared the BIS and phase lag entropy (PLE) and found that BIS readings were more susceptible to EMG artifacts following neuromuscular blockade reversal, whereas PLE demonstrated greater stability. 78 Moreover, the depth of neuromuscular blockade and analgesia may further complicate the interpretation of EEG-based DOA monitoring. Neuromuscular blockade can reduce EMG activity and thereby alter processed EEG-derived indices, whereas insufficient analgesia may increase sympathetic responses and affect physiological parameters despite apparently adequate hypnotic depth. Therefore, EEG-based DOA values should not be interpreted as a direct measure of overall anesthetic adequacy, particularly when hypnotic depth, analgesic balance, and neuromuscular blockade are changing simultaneously.79,80
In addition, studies conducted in sedation-only or pre-induction monitoring settings may provide useful information on how sedative depth affects vital signs before the confounding effects of full general anesthesia, neuromuscular blockade, and surgical stimulation become prominent. Evidence from procedural sedation suggests that EEG-based monitoring helps assess the adequacy of sedation and reduced excessive sedative exposure. However, its interpretation should be combined with respiratory and hemodynamic parameters, such as oxygen saturation, respiratory rate, blood pressure, and heart rate. Therefore, findings from sedation-only settings further support the view that DOA monitoring should be used as an adjunctive tool rather than as an isolated indicator of anesthetic adequacy.81,82
Second, EEG signal patterns vary substantially among different anesthetic agents, limiting the generalizability of EEG-based indices. Beekoo et al. reported distinct EEG spectral characteristics between inhalational anesthesia (sevoflurane) and intravenous anesthesia (propofol) and have noted that BIS values differ significantly between pediatric and older patients—suggesting that the algorithm does not fully account for physiological diversity. 83 Furthermore, certain agents such as ketamine, dexmedetomidine, and nitrous oxide can produce paradoxical EEG patterns—where the patient remains sedated but displays high-frequency “wake-like” EEG activity—leading to overestimation of the patient’s consciousness level using the BIS. 84
Third, discrepancies among monitoring devices due to proprietary algorithms compromise result consistency and standardization. Shepherd et al. reported significant heterogeneity between BIS, entropy, and Narcotrend readings under comparable anesthetic conditions, raising concerns about inter-device reliability. 85 Similarly, Abdelrahman et al. reported that electrode placement (frontal vs. postauricular) could alter BIS readings by as much as ±9%, underscoring the influence of hardware configuration on measurement accuracy. 86
From a clinical perspective, the evidence regarding whether DOA monitoring improves long-term outcomes remains inconsistent. Kettner concluded that BIS-guided anesthesia significantly reduces the risk of intraoperative awareness in high-risk patients (odds ratio = 0.24, 95% confidence interval: 0.12–0.48); however, it does not significantly improve mortality or postoperative cognitive outcomes under standard anesthetic care. 87 In a multicenter randomized controlled trial, Gruber et al. found that anesthesiologists who directly interpreted raw EEG waveforms titrated propofol more accurately and achieved higher postoperative QoR-15 scores than those relying solely on numerical BIS feedback. 88
Emerging research has suggested that artificial intelligence (AI) and multimodal monitoring approaches overcome some of these limitations. Li et al. developed a random forest model based on EEG complexity and spectral features, achieving a correlation coefficient of 0.84 with BIS values and demonstrating improved real-time stability and resistance to artifacts. 87
Taken together, although EEG-based DOA monitoring provides valuable neurophysiological insights, its limitations—including algorithmic variability, drug dependency, and signal artifacts—necessitate cautious interpretation. DOA indices should be regarded as adjunctive tools rather than definitive measures, and their use should be integrated with hemodynamic parameters, pharmacokinetic modeling, and clinical judgment to achieve truly individualized and precision-guided anesthesia management.
Future perspectives
With ongoing advances in anesthesiology, neuroscience, and biomedical engineering, research on DOA monitoring is gradually shifting from single-signal EEG assessment toward multidimensional integration and precision-oriented management. Traditional EEG-based monitoring methods remain limited in their ability to accurately reflect the full spectrum of consciousness states and predict postoperative complications. In recent years, multimodal monitoring has emerged as a promising direction. By integrating EEG with HRV, PPG, electromyography (EMG), and near-infrared spectroscopy (NIRS), clinicians can obtain a more comprehensive assessment of central and autonomic nervous system activity, thereby improving the sensitivity and stability of DOA evaluation. 89 Evidence suggests that combining EEG and HRV analysis provides superior performance in detecting intraoperative stress responses and fluctuations in consciousness compared with the use of EEG alone. 90
Monitoring approaches based on brain functional connectivity also show growing potential. Using EEG-derived measures such as functional connectivity and graph theory analysis, researchers have observed marked reductions in network integration and information transfer efficiency during deep anesthesia, suggesting that brain network indices better represent the neurophysiological basis of consciousness. 91 Moreover, the incorporation of EEG-derived parameters such as signal entropy and variability has enabled more precise dynamic quantification of transitions in consciousness. 92
Rapid advances in the fields of AI and machine learning are also reshaping anesthetic monitoring. Sharma et al. developed an interpretable AI model (XAI-VSDOA) that integrates multiple physiological parameters to predict the DOA with an accuracy of 99% and has demonstrated robustness across datasets. 93 Similarly, Madanu et al. applied convolutional neural networks combined with empirical mode decomposition (EEMD) for EEG analysis, achieving higher classification accuracy than conventional BIS-based systems. 94 A systematic review by Lopes et al. has concluded that AI-assisted anesthesia management outperforms traditional empirical methods in DOA evaluation, drug infusion control, and perioperative risk prediction. 95
The Closed-loop Anesthesia Delivery System (CLADS) represents another significant step forward. This system automatically adjusts anesthetic drug infusion in real time using EEG or AI–based feedback, improving control accuracy and hemodynamic stability. 96 Multiple clinical trials have shown that AI-driven closed-loop systems effectively reduce the duration of intraoperative hypotension, minimize drug consumption, and enhance recovery quality. 97
With the widespread adoption of personalized medicine, the concepts of precision anesthesia and goal-directed anesthesia are becoming increasingly prominent. Zeng et al. proposed integrating genetic information, neurophysiological parameters, and AI modeling to dynamically tailor anesthetic strategies based on patients’ metabolic and neural response profiles. 98 According to a bibliometric analysis by Ou and Hu, current research hotspots in anesthetic AI focus on multimodal depth monitoring, automated drug infusion, perioperative risk prediction, and individualized interventions. 99
Conclusion
DOA monitoring is closely related to several perioperative complications, including intraoperative awareness, hypotension and organ hypoperfusion associated with excessively deep anesthesia, POD and cognitive dysfunction, respiratory complications, and ICU sedation-related adverse events. Current evidence suggests that EEG-based monitoring supports more precise anesthetic titration and may be particularly valuable in high-risk populations, such as older patients, patients with cardiovascular disease, and those with limited physiological reserve. Although important limitations remain, ongoing advances in multimodal monitoring, brain network analysis, and AI may further improve the precision and clinical applicability of DOA monitoring in anesthesia management. In daily clinical practice, DOA monitoring should be interpreted together with clinical signs, hemodynamic status, anesthetic dosage, and patient-specific risk factors. It should be used as an adjunctive tool to support individualized anesthetic management rather than as a replacement for clinical judgment.
Footnotes
Acknowledgements
The authors used artificial intelligence (AI)–assisted tools for language improvement during the preparation of this manuscript. All the manuscript content has been reviewed and approved by the authors who take full responsibility for the final manuscript.
Author contributions
Huisen Yu contributed to the conception and design of the review, performed the literature search, drafted the manuscript, and contributed to manuscript revision. Bin Gao contributed to the literature analysis, interpretation of the evidence, and critical revision of the manuscript. Yuanyuan Li supervised the study, contributed to the conception and design of the review, and revised the manuscript for important intellectual content. All authors have read and approve the final manuscript.
Declaration of conflicting interests
The authors declare that there are no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.