
Abstract
Objective
Critically ill patients with septic shock frequently exhibit variability in antibiotic pharmacokinetics. We aimed to investigate the antibiotic concentration and time over minimum inhibitory concentration in patients with septic shock treated with prolonged and intermittent infusions.
Methods
We performed a post hoc analysis of a prospective study of patients with septic shock admitted to the intensive care unit at Helsingborg hospital from 2016 to 2018. Plasma samples were collected every 4 h for the initial 72 h following intensive care unit admission. We analyzed samples for cefotaxime (intermittent dosing), piperacillin–tazobactam (prolonged infusion), and meropenem (prolonged infusion) concentrations. Minimum inhibitory concentration values determined using epsilometer tests of bloodstream pathogens were collected, and corresponding epidemiological cut-off values were used for target attainment calculations. The primary outcome was percentage time over minimum inhibitory concentration or four times the minimum inhibitory concentration. We used linear mixed effects models for analyzing repeated measures of continuous variables.
Results
In total, 21 patients met the criteria for septic shock, and a total of 341 samples were analyzed (average 16 per patient). All patients achieved concentrations above the minimum inhibitory concentration for 100% of the time, and 83% of the patients achieved concentrations above 4 times the minimum inhibitory concentration for 100% of the time. We found an association between continuous renal replacement therapy and levels of antibiotics exceeding the upper therapeutic target (p = 0.021, odds ratio: 15, 95% confidence interval: 1 to 974).
Conclusion
Target attainment was high in this cohort study of critically ill patients with septic shock, with all patients achieving beta-lactam concentrations over the minimum inhibitory concentration 100% of the time.
Keywords
Introduction
Septic shock remains a significant global health concern and a leading cause of morbidity and mortality worldwide.1,2 Treatment of septic shock relies on prompt antimicrobial therapy. 3 Beta (ß)-lactams are the most used class of antibiotics in critically ill patients. They exhibit a time-dependent killing pattern, where the duration of exposure to antibiotics is important for their effectiveness.4,5 ß-lactams are generally known for their wide therapeutic index and few adverse effects; however, the increased use of therapeutic drug monitoring (TDM) has revealed abnormally high or low concentrations in several studies.6,7 This entails a risk of suboptimal therapy,6–9 potential toxicity, 10 and an increase in antibiotic resistance.4,11 Critically ill patients with septic shock are heterogeneous in age and comorbidities and often experience cardiovascular, liver, and renal organ dysfunction, 12 which contribute to pharmacokinetic (PK) variability.13,14 Dosing guidelines for adults are often extrapolated from studies on middle-aged healthy volunteers. 4 Several intensive care units (ICUs) have adopted continuous or extended infusion regimens instead of traditional intermittent dosing to optimize treatment. 3 Although extended or continuous infusions are theoretically appealing compared with intermittent dosing, their superiority seems difficult to prove with certainty or the benefit is small. 15 There may be added complicating factors associated with the use of continuous infusions such as intra-individual PK variability over time and durability or decomposition in vials. 16 We hypothesized that the unbound concentrations of ß-lactams in the blood of patients in the ICU with septic shock display important intra- and interindividual differences despite the use of prolonged infusions. We aimed to determine what proportion of patients with septic shock in the ICU attain an unbound ß-lactam concentration above the minimum inhibitory concentration (MIC) (free drug time over MIC (fT) > MIC) or four times the MIC (fT > 4x MIC) for 100% of the study period.
Methods
Study design and population
This post hoc, retrospective, cohort study was conducted at the ICU of Helsingborg Hospital. Helsingborg emergency hospital is in southern Sweden and has an ICU with seven beds. The hospital serves an estimated population of 250,000. Study participants were recruited from September 2016 to February 2018 for an original study that aimed to investigate the prognostic performance of repeated measurements of heparin-binding protein (HBP) in the plasma, the results of which were published in 2020. 17 The Swedish Ethical Review Authority approved the study design of the original study in 2016 (Dnr 2016/271) and this post hoc analysis in 2020 (Dnr 2021–02692). Patients were evaluated for eligibility on arrival to the ICU by the attending intensive care physician. The inclusion criteria were as follows: (a) age ≥18 years and (b) suspected septic shock. Septic shock was suspected in patients with an acute increase of ≥2 points in the total sequential organ failure assessment (SOFA) score due to a suspected infection in addition to a need for vasopressors to maintain a mean arterial pressure (MAP) ≥65 mmHg despite adequate fluid resuscitation and a serum lactate level of ≥2 mmol/L. 18 No exclusion criteria were applied. Patients meeting the inclusion criteria were invited to participate in the study and asked to provide written informed consent. When patients were unable to provide consent, their next-of-kin was approached for permission. For the post hoc antibiotic concentration analysis, patients were excluded if insufficient samples were available or if MIC or epidemiological cut-off values (ECOFFs) data necessary for target attainment calculations could not be obtained. Patients included in the study received treatment with either cefotaxime given as intermittent doses (20 min infusions), piperacillin–tazobactam as a prolonged infusion (3-h infusions) or meropenem as a prolonged infusion, depending on clinical presentation. The continuous renal replacement therapy (CRRT) modality was continuous venovenous hemodialysis (CVVHD) with Prismaflex using regional citrate or heparin anticoagulation with Phoxilium or Hemosol solutions. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 19
Data and sample collection
A trained ICU nurse prospectively collected data at the time of plasma sampling using a study-specific case report form. Demographic characteristics, medical history, laboratory and microbiology results, monitoring parameters, physiological variables, and survival data were retrospectively extracted from electronic health records. Comorbidities were classified using the Charlson Comorbidity Index (CCI). 20 Renal function was assessed at the time of inclusion by determining the estimated glomerular filtration rate (eGFR) using serum creatinine values and the revised Lund–Malmö equation (LM-rev). 21 Serial plasma samples were collected starting within 2 h of ICU admission and subsequently every 4 h for up to 72 h or until death or ICU discharge. Arterial blood was drawn into 2.7-mL sodium citrate tubes, centrifuged, and the plasma aliquoted and frozen at −80°C within 1 h.
Analyses of ß-lactam concentrations
Samples from the HBP–Kinetics in Septic Shock (KISS) study were stored in a biobank at the Infection Clinic SUS Lund (BD-3) at −80°C for up to 5 years prior to analyses. 22 Antibiotic concentration analyses were performed at the Clinical Chemistry Department in Lund using liquid chromatography–mass spectrometry (LC–MS) with a coefficient of variation <15%. 23 An internal check was performed to compare analyses of sodium citrate and ethylenediaminetetraacetic acid (EDTA) plasma samples. Antibiotic concentrations were corrected for protein binding, and free concentrations were calculated. Concentrations of unbound piperacillin, cefotaxime, and meropenem were estimated to be 70%, 60%, and 98% of the total value, respectively.24–26 Tazobactam concentration was not analyzed. Epsilometer (E) tests were performed on saved samples from included patients unless an MIC value was already known and recorded in the database. The European Committee on Antimicrobial Susceptibility Testing (EUCAST) ECOFFs were used for all target attainment calculations, with individual MIC values presented alongside for reference. The toxicity analysis was restricted to piperacillin and meropenem, for which the upper therapeutic target thresholds were defined as 157 mg/L and 44 mg/L, respectively.10,27–29 However, there is no consensus, and some studies have suggested higher trough concentrations, especially for neurotoxic events. 30 The threshold for determining toxic levels of cefotaxime is not defined, although the French Societies of Pharmacology and Therapeutics (SFPT) and Anesthesia and Intensive Care Medicine (SFAR) have suggested an upper threshold for optimal treatment of 60 mg/L for cefotaxime.31,32
Outcome definition
Primary outcome. The primary outcome was the proportion of patients with unbound ß-lactam concentrations at or above MIC for 100% of the time (100% fT > MIC) or at or above 4 times the MIC (100% fT > 4x MIC) from the first to the last sampling time point (from ICU admission up to 72 h).
Secondary outcomes. The following two secondary outcomes were recorded:
Toxicity. Occurrence of ß-lactam concentrations above the upper therapeutic target thresholds and possibly related adverse events;
Clearance. Association between absolute unbound ß-lactam concentrations and individual eGFR or with use of CRRT.
Statistical analyses
All patient data were deidentified prior to analysis. Time over MIC was calculated using linear interpolation between measured concentrations obtained at 4-h intervals over 72 h. The percentage of time above MIC (fT > MIC) was determined as the proportion of the total observation period, during which free antibiotic concentrations exceeded the MIC, calculated as the sum of time intervals with concentrations above MIC divided by the total observation time. In addition to analyzing time over MIC, we recorded whether concentrations reached the upper therapeutic target levels, as defined by specific thresholds. The association between antibiotic toxicity and individual patient factors was performed using univariate and multivariate logistic regression modeling. Fisher's exact test was used for the comparison of proportions with less than five observations, such as for assessing the correlation between upper therapeutic target levels and CRRT. The secondary analysis regarding clearance was performed using linear mixed effects regression modeling, adjusting for repeated measurements within individuals using an identity link. Missing data were handled using a complete case approach. Statistical analyses were conducted using Stata MP 18.0 and R (version 2023.12.1 + 402). No sample size calculation was performed for this post hoc study.
Results
Patient characteristics
During the original prospective study period, there were a total of 88 eligible patients, out of which 22 were included. The mean age of the 22 included patients was 66.5 (range: 34–84) years; 9 patients were female (41%), and 7 were surgical admissions (32%). The median Simplified Acute Physiology Score 3 (SAPS 3) score was 70 (range: 47–100) points, and the median SOFA score on the first day was 12.5 (range 6–18). Twenty-one out of the 22 patients received a final diagnosis of septic shock, whereas one patient (ID: 18) experienced circulatory failure due to a severe episode of inflammatory bowel disease. The 28-day mortality rate was 23% (n = 5), and the 90-day mortality rate was 27% (n = 6). Figure 1 illustrates the patient selection flowchart, and Table 1 includes information about patient characteristics.
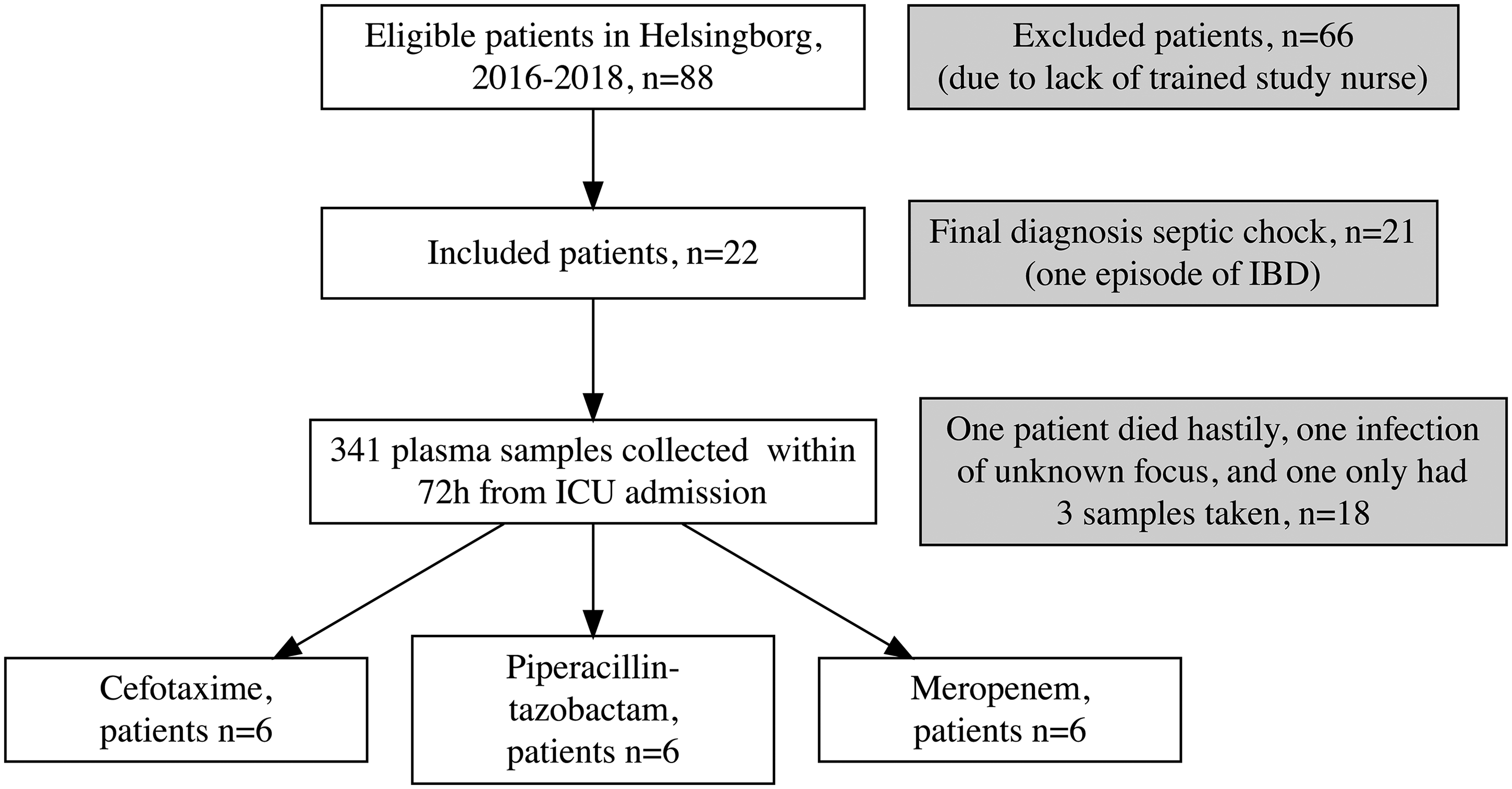
Flow chart depicting the selection process of eligible patients for the study conducted in Helsingborg from 2016 to 2018, along with subsequent exclusions and reasons.
Patient characteristics.
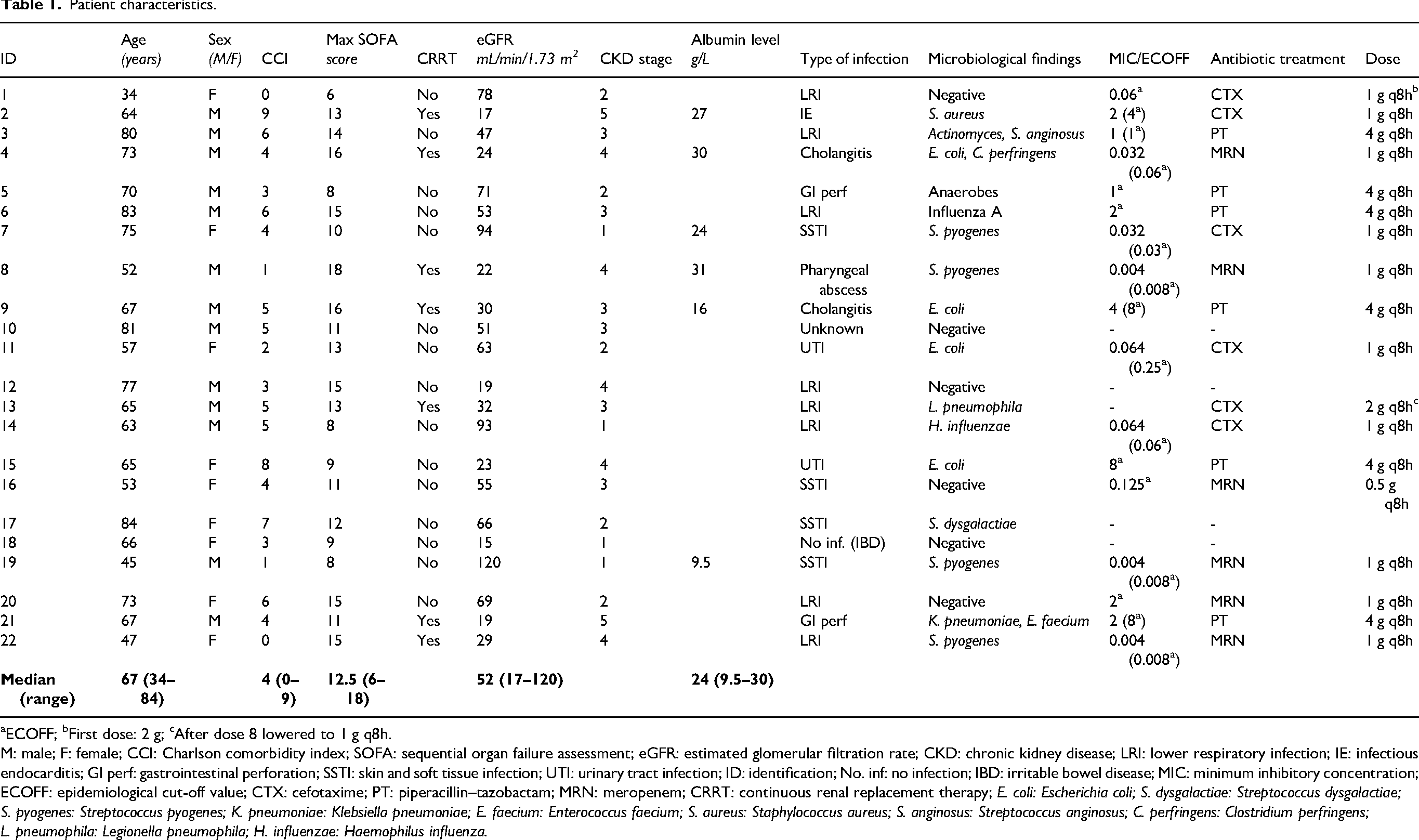
ECOFF; bFirst dose: 2 g; cAfter dose 8 lowered to 1 g q8h.
M: male; F: female; CCI: Charlson comorbidity index; SOFA: sequential organ failure assessment; eGFR: estimated glomerular filtration rate; CKD: chronic kidney disease; LRI: lower respiratory infection; IE: infectious endocarditis; GI perf: gastrointestinal perforation; SSTI: skin and soft tissue infection; UTI: urinary tract infection; ID: identification; No. inf: no infection; IBD: irritable bowel disease; MIC: minimum inhibitory concentration; ECOFF: epidemiological cut-off value; CTX: cefotaxime; PT: piperacillin–tazobactam; MRN: meropenem; CRRT: continuous renal replacement therapy; E. coli: Escherichia coli; S. dysgalactiae: Streptococcus dysgalactiae; S. pyogenes: Streptococcus pyogenes; K. pneumoniae: Klebsiella pneumoniae; E. faecium: Enterococcus faecium; S. aureus: Staphylococcus aureus; S. anginosus: Streptococcus anginosus; C. perfringens: Clostridium perfringens; L. pneumophila: Legionella pneumophila; H. influenzae: Haemophilus influenza.
Sample, blood culture, and antimicrobial dosing characteristics
In total, 341 plasma samples were collected. Thus, an average of 16 samples per patient were collected every 4 h during the first 3 days at the ICU. Four patients (IDs: 10, 12, 17, and 18) were excluded from the antibiotic concentration analysis. One patient (ID: 12) was excluded due to early death. Only three samples were collected from another patient (ID: 17) at the start of treatment. One patient (ID: 10) had an infection of unknown origin, whereas another (ID: 18) experienced acute severe exacerbation of irritable bowel disease, rendering analysis unfeasible due to the lack of MIC or ECOFF data. Patients undergoing cefotaxime treatment were administered intermittent doses, whereas those being administered piperacillin–tazobactam or meropenem received prolonged infusion. One patient (ID: 10) accidentally received four doses of cefotaxime at once. Five patients (IDs: 2, 15, 16, 18, and 19) received less than five doses of the ß-lactam antibiotics analyzed. Eleven patients had positive blood cultures (50%). The most common blood culture finding was Escherichia coli and Streptococcus pyogenes, accounting for 36% each out of positive blood cultures. In 16 patients (73%), cultures from other sites such as the respiratory tract, urinary tract, wound site, and abdominal abscess were positive. All identified pathogens were susceptible to the administered ß-lactam antibiotics. Figure 2 provides an overview of the antibiotic concentrations in individual patients over time compared with the MIC or ECOFF. Table 1 presents a list of estimated MICs.
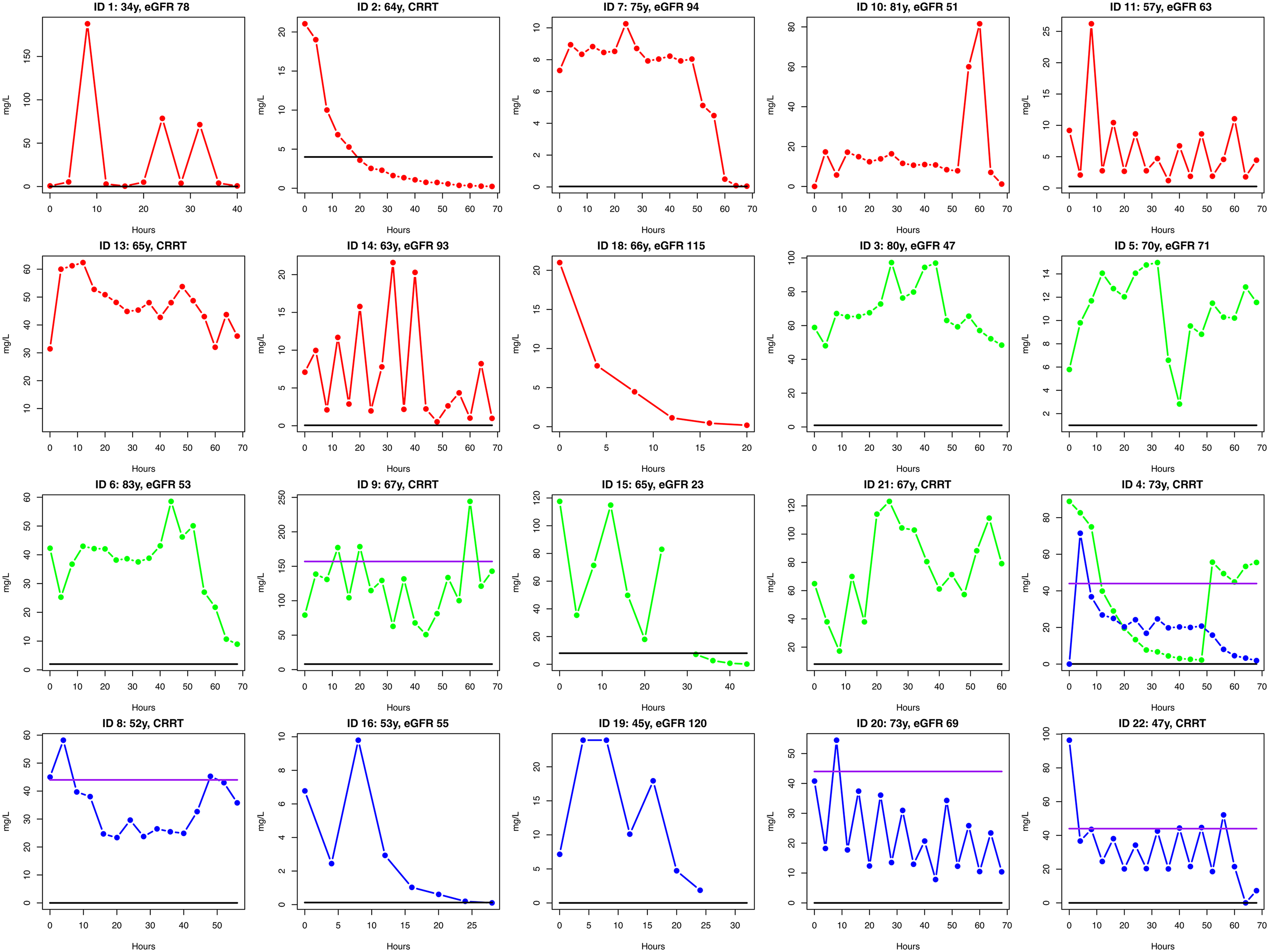
Graphs illustrating antibiotic concentrations over time for each patient. Cefotaxime was administered intermittently, whereas piperacillin–tazobactam and meropenem, administered as prolonged infusions. Line styles and point shapes for each antibiotic as well as for the epidemiological cut-off value (ECOFF) and the upper threshold for extended infusion are defined in the legend. Additional patient information can be found in Table 1.
Primary outcome: Target attainment
All assessable patients (n = 18) achieved 100% fT >MIC. In total, 83% of patients achieved 100% fT >4x MIC (n = 15) (Table 2).
Summary of results for primary and secondary outcomes.
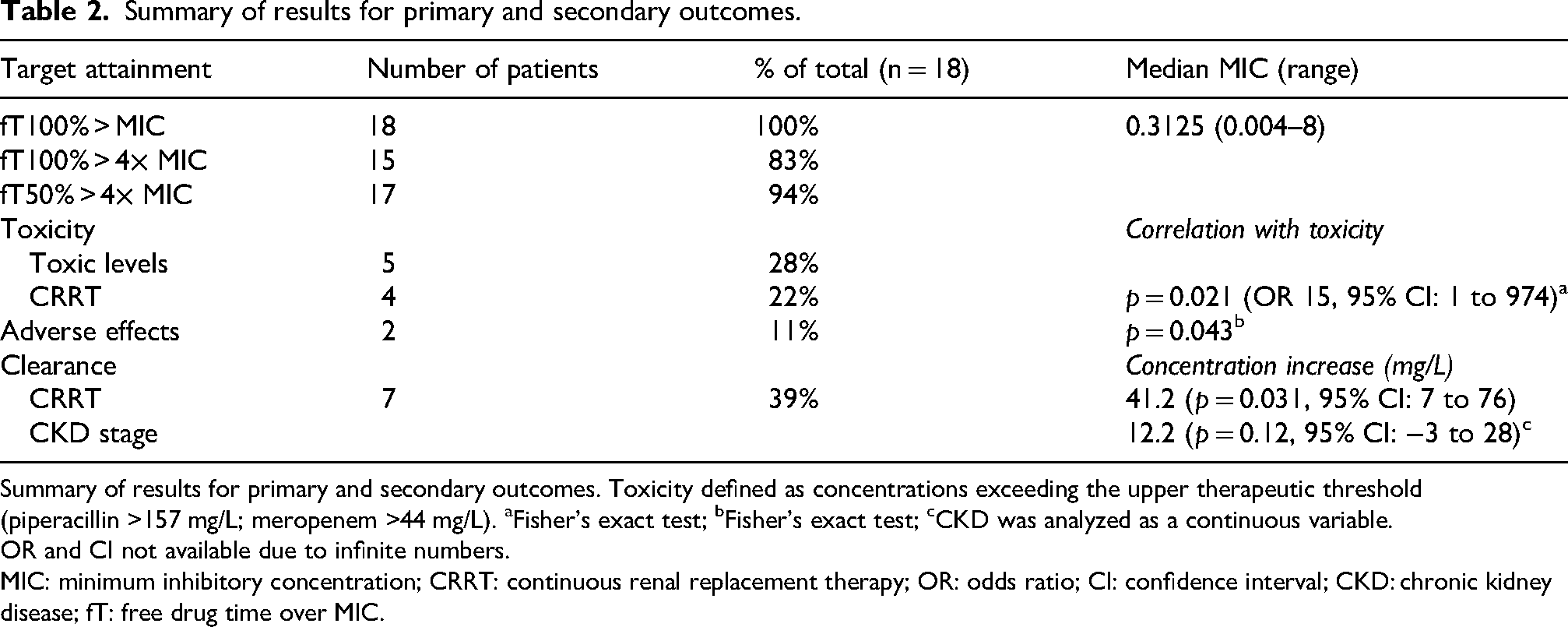
Summary of results for primary and secondary outcomes. Toxicity defined as concentrations exceeding the upper therapeutic threshold (piperacillin >157 mg/L; meropenem >44 mg/L). aFisher's exact test; bFisher's exact test; cCKD was analyzed as a continuous variable.
OR and CI not available due to infinite numbers.
MIC: minimum inhibitory concentration; CRRT: continuous renal replacement therapy; OR: odds ratio; CI: confidence interval; CKD: chronic kidney disease; fT: free drug time over MIC.
Secondary outcomes
Toxicity (piperacillin and meropenem). In five patients (IDs: 4, 8, 9, 20, and 22), concentrations were intermittently above the upper therapeutic target levels for extended infusions. All these patients were on CRRT, and two eventually died. Both deceased patients (IDs: 9 and 20) had received CRRT due to renal failure. Two patients had documented adverse effects potentially attributable to ß-lactam antibiotics, including one with concentrations exceeding the upper therapeutic threshold for piperacillin and thrombocytopenia (ID: 9) and another with ß-lactam fever (ID: 22). Out of five patients with concentrations exceeding the upper therapeutic threshold, four had received CRRT, versus one out of seven patients who had not received CRRT (p = 0.021, odds ratio (OR): 15, 95% confidence interval (CI): 1 to 974; Table 2). Our analysis revealed no additional significant predictors for concentrations exceeding the upper therapeutic threshold. Neither chronic kidney disease (CKD) (p = 0.996, 95% CI −448 to 318) nor eGFR (p = 0.996, 95% CI: −3 to 653) were associated with exceeding of this threshold.
Clearance. In total, 13 individuals had CKD stage >2 (59%). No patients demonstrated augmented renal clearance (creatinine clearance > 130 mL/min). 33 Among the 22 patients, 7 required CRRT. Among the 7 patients receiving CRRT, effluent rates at initiation ranged from 23 to 29 mL/kg/h. Dialysate flow rates ranged from 1000 to 1200 mL/h, and replacement fluid flow rates ranged from 600 to 1000 mL/h, with fluid removal between 0 and 100 mL/h. Data were unavailable for two patients (IDs: 2 and 4) due to missing records.
Patients had on average 0.62 mg/L lower antibiotic concentration for every 1-mL/min increase in the eGFR (p = 0.023, 95% CI: 1.1 to 0.092). Patients on CRRT had on average 41.2-mg/L higher antibiotic concentration than those not receiving CRRT (p = 0.031, 95% CI: 6.6 to 76). Albumin levels were measured for 6 patients during the collection period, with a median value of 27 g/L (interquartile range (IQR): 16–30 g/L; Table 1). The antibiotic concentration was estimated to decrease by 1.87 mg/L for every 1-g/L increase in the albumin level; however, this effect was not statistically significant (p = 0.634, 95% CI: −75 to 259).
Discussion
Main findings
The antibiotic concentration target achievement was very high among 21 ICU patients with septic shock, revealing unbound ß-lactam concentrations at or above MIC for 100% of the observation period. Additionally, augmented levels of antibiotic concentrations were common and could be related to CRRT rather than eGFR.
Comparison with other studies
We observed an association between CRRT and augmented concentrations, contrary to the prevailing emphasis on the risk of underdosing antibiotics during CRRT in some previous studies.34–37 Our findings suggest that CRRT leads to elevated concentrations of ß-lactam antibiotics, potentially due to the overestimation of drug clearance, which contrasts with previous ex vivo studies demonstrating rapid antibiotic removal via CRRT circuits.36,37 Studies have shown that the clearance of meropenem and piperacillin–tazobactam is influenced by various CRRT modalities and prescriptions as well as effluent flow rates and residual renal function.34,38 Our study revealed overdosing rather than underdosing with CRRT, challenging the existing consensus on antibiotic dosing in this context. Notably, Swedish guidelines do not recommend adjusting dosage in patients with CRRT and severe infections. 39 The significant interindividual and intra-individual variability in concentrations further complicates dosing predictions. The wide variability in drug exposure observed, independent of the prescribed dosing regimen, is consistent with previously published data. Roberts et al. have documented up to 6.7-fold variability in meropenem trough concentrations in CRRT patients receiving empirical dosing, despite relatively standardized regimens. 40 The subsequent multinational Sampling Antibiotics in Renal Replacement Therapy (SMARRT) study confirmed this finding, demonstrating that neither the CRRT prescription nor the dosing regimen alone could reliably predict trough concentrations and that estimated total renal clearance (eTRCL) was insufficient as a sole dosing guide. 29 The heterogeneity of CRRT practices and pathophysiology results in substantial intra- and interpatient PK variability. Our data extend these observations to the setting of extended infusion, where the relationship between dose and exposure remains similarly unpredictable, reinforcing the case for individualized TDM-guided dosing in this population. In the recently published multicenter randomized controlled trial, BLING III, no significant difference was observed in the 90-day mortality between groups receiving intermittent versus continuous infusions. 15
Interpretation
By visualizing the substantial PK variability observed in septic ICU patients even when antibiotics are administered via prolonged infusion, this study underscores the complex nature of hydrophilic antibiotic dosing in critically ill individuals. The presence of higher concentrations, possibly due to prolonged infusion, in many patients with acute kidney injury (AKI) and undergoing CRRT, indicates a potential overestimation of clearance. Prolonged dosing strategies may require lower doses, and it is conceivable that the combination of prolonged antibiotics and CRRT contributes to higher doses. Furthermore, the absence of augmented renal clearance in this cohort may have contributed to the high degree of target attainment observed. In this context, concentrations above the target may partly be a consequence of insufficient dose reduction rather than inherent PK variability.
This study sheds light on the issue of antibiotic toxicity. Two patients in the cohort developed adverse effects. Two patients had documented adverse effects of ß-lactam antibiotics, including one who developed thrombocytopenia and another who experienced with ß-lactam fever; both patients had received CRRT. The patient who developed thrombocytopenia exhibited intermittent episodes in which the piperacillin level exceeded the upper therapeutic target for extended infusion, indicating that the thrombocytopenia was caused by bone marrow toxicity caused by piperacillin–tazobactam. Considering these observations, the study highlights the potential value of TDM as a tool to optimize dosing and prevent toxic concentrations, particularly in patients undergoing CRRT where the actual drug clearance may be overestimated leading to augmented antibiotic concentrations.
Strengths
One strength of this study is the frequent sampling regimen, with measurements taken every 4 h over a span of 3 days, including a comprehensive visualization of drug kinetics and the ability to evaluate time over MIC. Additionally, although this was a retrospective study, the initial samples were collected in a prospective manner, featuring broad inclusion criteria and a well-defined cohort, where 21 out of 22 patients were diagnosed with septic shock.
Limitations
The study has certain limitations. First, this retrospective study was based on previously collected samples. In the initial HBP-KISS study, there was no sample size calculation or prespecified analysis plan as antibiotic concentration measurements were not originally intended.
Additionally, only 25% of eligible patients with signs of septic shock were enrolled. This yielded a relatively small sample size, making it challenging to draw definitive conclusions.
Furthermore, data collection and analysis were performed well after the patients were admitted and treated in the ICU, making it challenging to establish direct correlations between observations and the clinical setting. Sampling was not planned in relation to antibiotic administration, which is an inherent limitation of the post hoc study design. Finally, toxicity could not be formally assessed in this study, as trough concentrations were not available for patients on intermittent dosing, and validated steady-state toxicity thresholds remain poorly defined in the literature for patients receiving extended infusion.
Conclusion
This small observational study indicates adequate levels of unbound ß-lactam antibiotic concentration can be achieved in most patients with septic shock using either intermittent or prolonged infusion. However, the level of concentration varies considerably between individuals and, in the same individual over time, with an associated risk of toxicity. This provides weak support for the use of TDM in clinical practice, particularly in patients undergoing CRRT.
Supplemental Material
sj-docx-1-imr-10.1177_03000605261457800 - Supplemental material for Time over minimum inhibitory concentration and variations in beta-lactam concentrations during prolonged and intermittent infusions in patients with septic shock: A post hoc observational study
Supplemental material, sj-docx-1-imr-10.1177_03000605261457800 for Time over minimum inhibitory concentration and variations in beta-lactam concentrations during prolonged and intermittent infusions in patients with septic shock: A post hoc observational study by Ylva Mattisson and Jonas Tverring in Journal of International Medical Research
Footnotes
Ethics considerations
The study was conducted in accordance with the Declaration of Helsinki of 1975, as revised in 2024. The Swedish Ethical Review Authority approved the study design of the original study in 2016 (Dnr 2016/271) and this post hoc analysis in 2020 (Dnr 2021–02692), with the need for written informed consent waived.
Consent to participate
In the original study, patients were asked to participate and provide written informed consent. If they were unable to provide consent, their next-of-kin was asked permission. In this post hoc analysis, the need for written informed consent was waived.
Author contributions
Jonas Tverring conceived the study. Jonas Tverring and Ylva Mattisson collected data from medical records and sample analyses. Ylva Mattisson drafted the manuscript and created the figures, which Jonas Tverring revised. Ylva Mattisson performed the statistical analyses. All authors approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Stig & Ragna Gorthon's Foundation (2022–2816 to YM, grant number 2022-2816).
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data are available upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.