
Abstract
Objective
To compare the predictive performance of quick Sequential Organ Failure Assessment, National Early Warning Score 2, Shock Index, and Modified Shock Index for in-hospital mortality in adult emergency department patients with sepsis.
Methods
This retrospective observational study included 187 adult patients who presented to the emergency department and met the Sepsis-3 definition of sepsis between January 2022 and December 2023. The predictive performance of quick Sequential Organ Failure Assessment, National Early Warning Score 2, Shock Index, and Modified Shock Index was evaluated using receiver operating characteristic curve analysis, DeLong’s test, and diagnostic performance metrics, including sensitivity, specificity, positive predictive value, and negative predictive value. Multivariable logistic regression was performed as an exploratory secondary analysis.
Results
Among 187 patients, 37 (19.8%) died during hospitalization. Non-survivors showed greater physiological derangement at emergency department presentation, including higher respiratory rate, heart rate, and lactate levels and lower oxygen saturation. National Early Warning Score 2 demonstrated the highest discriminatory performance for in-hospital mortality (area under the curve, 0.94), followed by quick Sequential Organ Failure Assessment (area under the curve, 0.82), Modified Shock Index (area under the curve, 0.79), and Shock Index (area under the curve, 0.77). Pairwise comparisons using DeLong’s test showed that National Early Warning Score 2 performed significantly better than the other evaluated tools. In exploratory multivariable analysis, quick Sequential Organ Failure Assessment ≥2, Modified Shock Index ≥1.3, lactate >2.0 mmol/L, and chronic kidney disease were independently associated with in-hospital mortality.
Conclusions
National Early Warning Score 2 showed the best predictive performance for in-hospital mortality in adult emergency department patients with sepsis and may be a useful tool for early risk stratification in this setting.
Keywords
Introduction
Sepsis remains a leading cause of morbidity and mortality in emergency departments (EDs) worldwide. Globally, it affects an estimated 49 million people annually and is responsible for 11 million deaths, accounting for approximately 20% of all deaths worldwide.1–4 Prompt identification and risk stratification of patients with sepsis are crucial for initiating timely interventions and improving outcomes. However, the heterogeneous nature of sepsis poses challenges for early risk prediction and clinical decision making.2,5–8
To address this challenge, several rapid bedside scoring systems have been developed and validated across various settings. Among them, the quick Sequential Organ Failure Assessment (qSOFA) score was introduced by the Sepsis-3 task force to identify patients at high risk of mortality outside the intensive care unit (ICU).3,8–10 The National Early Warning Score 2 (NEWS2), widely implemented in the UK and increasingly adopted globally, integrates multiple physiological parameters to detect clinical deterioration.11–13 In addition, the Shock Index (SI) and its modification, the Modified Shock Index (MSI), provide simple hemodynamic markers based on vital signs and have shown promise in predicting adverse outcomes across a range of acute illnesses, including sepsis.1,14,15
Although each of these tools has demonstrated prognostic value, direct comparisons of their predictive performances in the emergency setting, particularly in the context of sepsis, remain limited. Furthermore, their relative utility in predicting short-term adverse outcomes, such as ICU admission or in-hospital mortality, continues to be debated.3,16–18
Therefore, this study aimed to compare the predictive performance of qSOFA, NEWS2, SI, and MSI in assessing the risk of adverse outcomes among patients with sepsis presenting to the ED. By identifying the most accurate and practical tool, we aimed to provide evidence that may guide frontline clinicians in the early recognition and management of high-risk sepsis patients.
Methods
Study design and setting
This was a retrospective observational study conducted in the ED of Rudong County People’s Hospital, a tertiary care academic medical center, between January 2022 and December 2023.
Study population
Adult patients (≥18 years) who presented to the ED and met the Sepsis-3 definition of sepsis were eligible for inclusion. Eligible patients were consecutively identified from the electronic medical records during the study period according to the predefined inclusion and exclusion criteria. Sepsis was defined as suspected or documented infection accompanied by an acute increase in Sequential Organ Failure Assessment (SOFA) score of ≥2 points compared with baseline. Patients were excluded if key clinical data required to calculate the risk scores or ascertain outcomes were missing or if sepsis onset occurred after hospital admission (Figure 1). Approximately 10% of initially screened patients were excluded because of missing data.

Patient enrollment and study flow diagram.
Data collection
Electronic medical records were reviewed to collect demographic data, comorbidities, vital signs, laboratory parameters, and clinical outcomes. The physiological variables used to calculate qSOFA, NEWS2, SI, and MSI were obtained from the first recorded vital signs within the first hour of ED arrival. Laboratory parameters, including lactate, were based on the initial blood tests obtained within the first hour of ED presentation, where available. Dichotomized variables were defined as follows: qSOFA ≥2, 19 NEWS2 ≥ 7, 20 SI ≥0.9, and MSI ≥1.3, 21 based on previous literature.
Outcome measures
The primary outcome was in-hospital mortality during the index hospitalization. Patients were classified into survivors and non-survivors accordingly.
Statistical analysis
Continuous variables were presented as mean ± SD or median (interquartile range), and categorical variables were presented as counts and percentages. Group comparisons were performed using the unpaired Student’s t-test or Mann–Whitney U test for continuous variables and chi-squared or Fisher’s exact test for categorical variables. Univariate logistic regression was performed to explore variables associated with in-hospital mortality. Variables with clinical relevance and p <0.1 in univariate analysis were entered into a multivariate logistic regression model as an exploratory secondary analysis. The primary comparative analysis of the scoring systems focused on diagnostic performance metrics, including the area under the receiver operating characteristic (ROC) curve (AUC-ROC), sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). Odds ratios (ORs) with 95% confidence intervals (CIs) were reported. The discriminatory performance of each scoring system was assessed by calculating the AUC-ROC with 95% CIs. Sensitivity, specificity, PPV, and NPV were also calculated for the predefined cutoff values of qSOFA, NEWS2, SI, and MSI. Comparisons between AUCs were performed using the DeLong test. In addition, forest plots were generated to visualize the strength of association between risk factors and outcomes. Statistical analyses were performed using R software (version 4.3.2). A two-sided p-value <0.05 was considered statistically significant.
Ethics statement
This retrospective observational study was conducted in accordance with the Declaration of Helsinki of 1975, as revised in 2024. The study was reviewed by the Ethics Committee of Rudong County People’s Hospital, Rudong, China, and a waiver of ethical approval and written informed consent was granted on 23 December 2021 because the study used anonymized data collected during routine clinical care and posed minimal risk to participants. No separate exemption number was issued for this waiver. All patient details were deidentified before analysis. The reporting of this study conforms to the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guideline. 22
Results
Baseline characteristics
A total of 187 adult patients meeting the Sepsis-3 definition of sepsis were included, of whom 37 (19.8%) died during hospitalization. Compared with survivors, non-survivors were older and showed more severe physiological disturbance at ED presentation, including higher heart rate and respiratory rate, lower oxygen saturation, and more frequent altered mental status and supplemental oxygen use. Non-survivors also had higher qSOFA, NEWS2, SI, and MSI values as well as higher lactate levels. In addition, comorbidities such as diabetes mellitus, chronic kidney disease, chronic lung disease, and active malignancy were more common among non-survivors. Detailed baseline characteristics are shown in Table 1.
Baseline characteristics of the study population.

BMI: body mass index; BP: blood pressure; bpm: beats per minute; SpO2: peripheral oxygen saturation; GCS: Glasgow Coma Scale; qSOFA: quick Sequential Organ Failure Assessment; NEWS2: National Early Warning Score 2.
Univariate logistic regression analysis
The results of the univariate logistic regression analysis for predicting in-hospital mortality are summarized in Table 2. Several demographic, physiological, laboratory, and comorbidity variables were significantly associated with mortality. Older age, higher body mass index (BMI), higher temperature, elevated heart rate and respiratory rate, lower oxygen saturation, altered mental status, and supplemental oxygen use were all associated with increased odds of in-hospital death. Among the evaluated scoring systems, qSOFA ≥2, NEWS2 ≥7, SI ≥0.9, and MSI ≥1.3 were all significantly associated with mortality. Elevated lactate levels and comorbidities including diabetes mellitus, chronic kidney disease, chronic lung disease, and active malignancy were also significant predictors.
Univariate analysis of factors associated with in-hospital mortality.
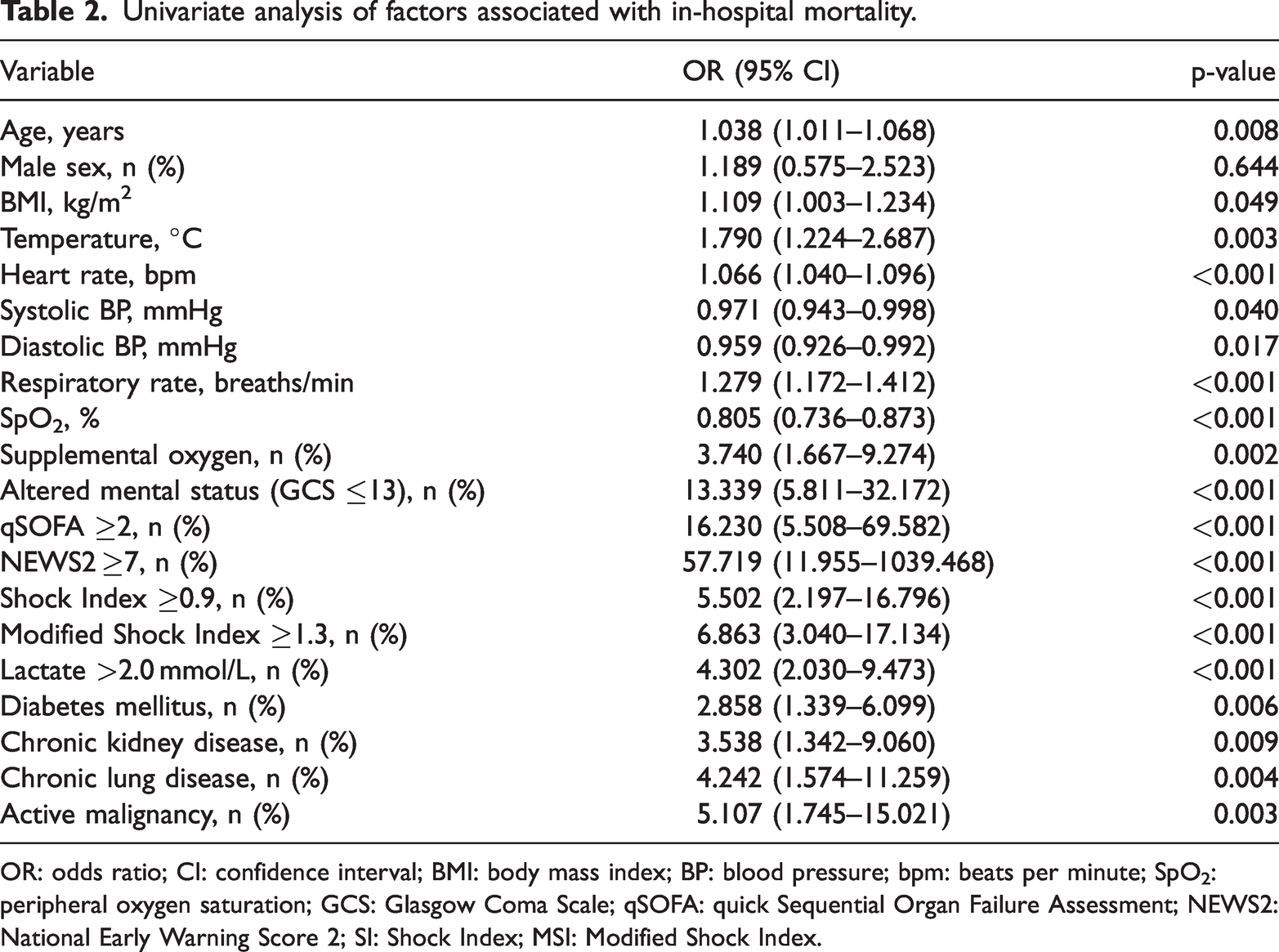
OR: odds ratio; CI: confidence interval; BMI: body mass index; BP: blood pressure; bpm: beats per minute; SpO2: peripheral oxygen saturation; GCS: Glasgow Coma Scale; qSOFA: quick Sequential Organ Failure Assessment; NEWS2: National Early Warning Score 2; SI: Shock Index; MSI: Modified Shock Index.
Multivariate logistic regression analysis
The results of the multivariate logistic regression analysis are shown in Table 3 and Figure 2. After adjustment for potential confounders, BMI, qSOFA ≥2, MSI ≥1.3, lactate >2.0 mmol/L, and chronic kidney disease remained independently associated with in-hospital mortality. Among these variables, qSOFA ≥2 demonstrated the strongest association with mortality (OR: 29.2, 95% CI: 6.478–226.581, p < 0.001). Diabetes mellitus, chronic lung disease, and active malignancy showed elevated ORs but did not reach statistical significance.
Multivariate logistic regression analysis for predicting in-hospital mortality.
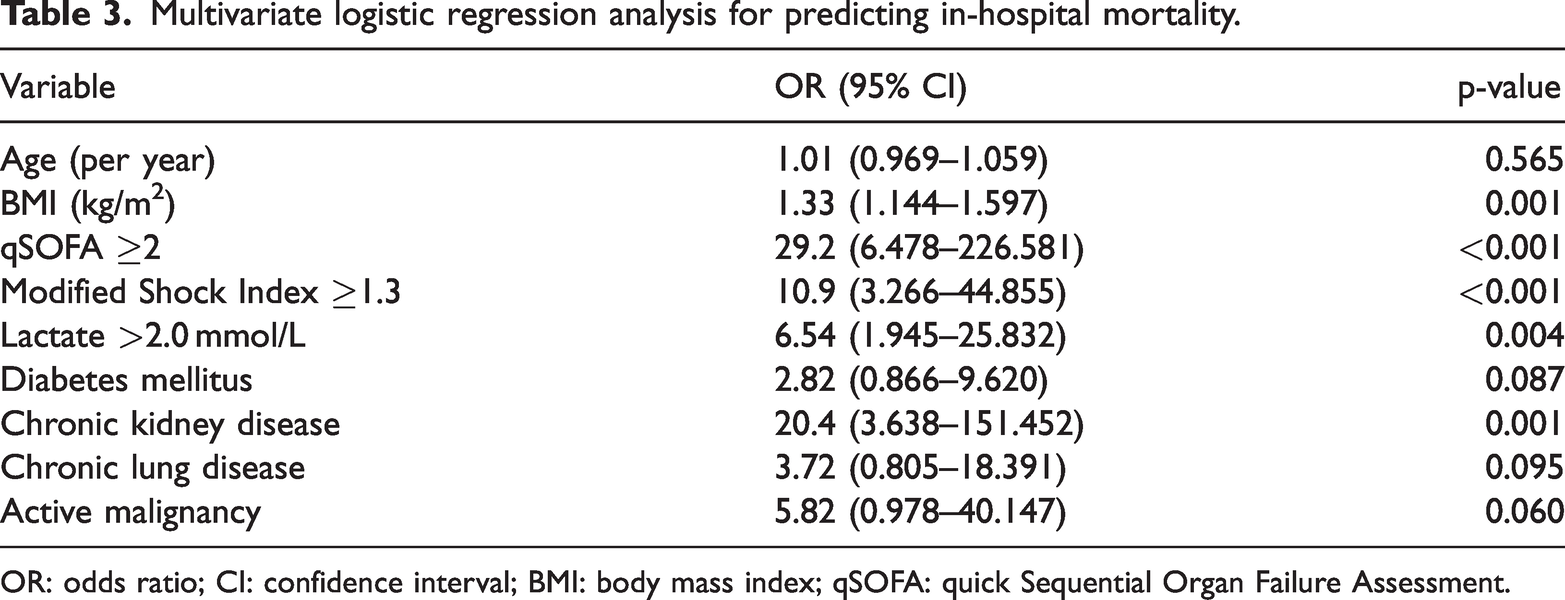
OR: odds ratio; CI: confidence interval; BMI: body mass index; qSOFA: quick Sequential Organ Failure Assessment.
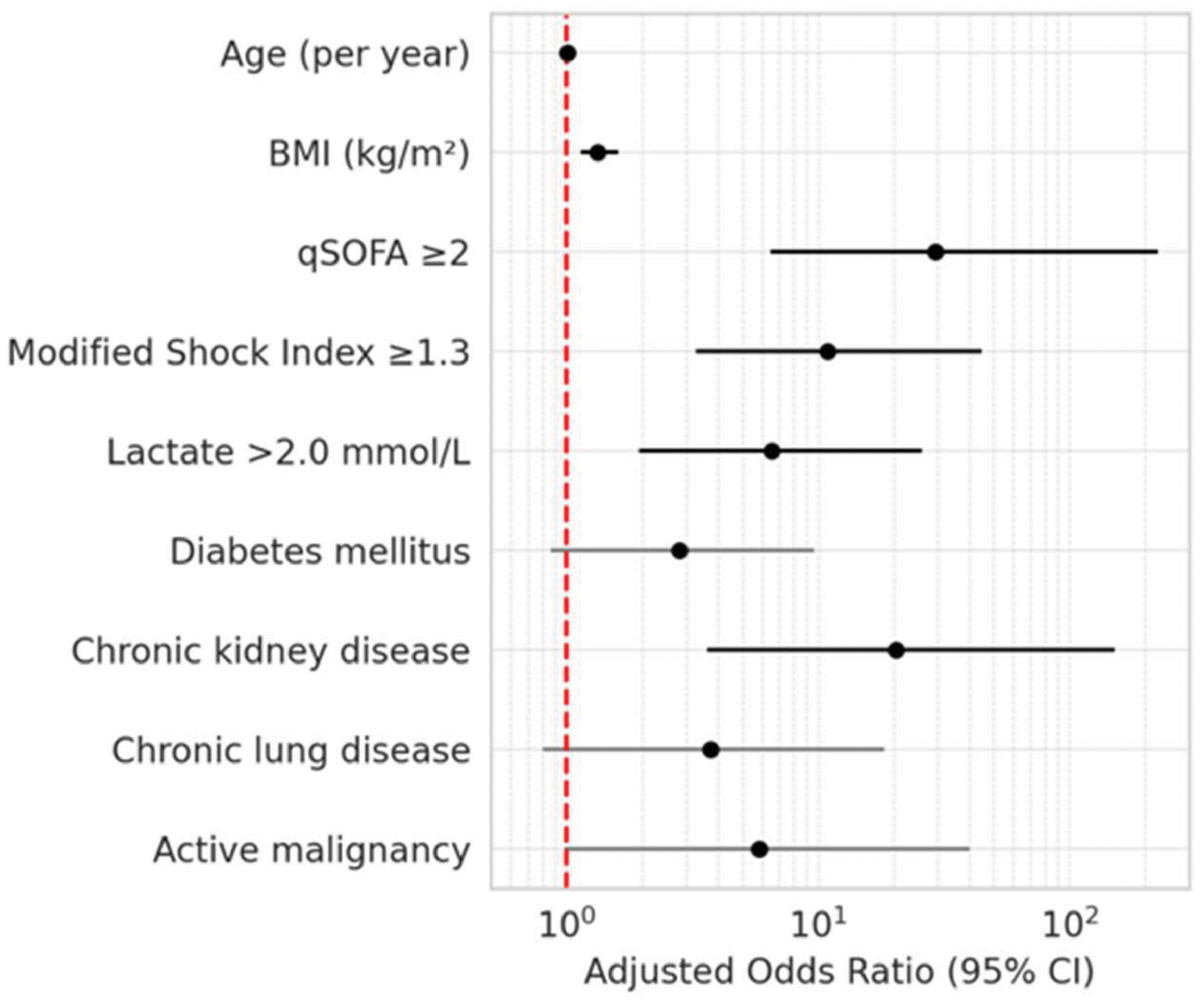
Forest plot of the exploratory multivariable logistic regression analysis for in-hospital mortality. Adjusted odds ratios (ORs) with 95% confidence intervals are shown for variables included in the multivariable model. The dashed vertical line indicates an OR of 1.0. This analysis was performed as an exploratory secondary analysis.
Predictive performance of qSOFA, NEWS2, SI, and MSI
The predictive performance of qSOFA, NEWS2, SI, and MSI for in-hospital mortality was evaluated using ROC curve analysis. Among the evaluated tools, NEWS2 showed the highest discriminatory performance, followed by qSOFA, whereas SI and MSI showed lower predictive ability. Detailed diagnostic performance metrics, including AUC with 95% CIs, sensitivity, specificity, PPV, and NPV at the predefined cutoff values, are presented in Table 4. Pairwise comparisons of AUCs using DeLong’s test showed that NEWS2 performed significantly better than qSOFA, SI, and MSI, whereas no significant differences were observed among qSOFA, SI, and MSI (Table 5). The ROC curves are illustrated in Figure 3(a), and the forest plot of AUCs with 95% CIs is presented in Figure 3(b).
Diagnostic performance of qSOFA, NEWS2, Shock Index, and Modified Shock Index for predicting in-hospital mortality.

qSOFA: quick Sequential Organ Failure Assessment; NEWS2: National Early Warning Score 2; AUC: area under the curve; CI: confidence interval; PPV: positive predictive value; NPV: negative predictive value.
Pairwise comparison of AUCs using DeLong’s test.

AUC: area under the curve; qSOFA: quick Sequential Organ Failure Assessment; NEWS2: National Early Warning Score 2.

Comparative diagnostic performance of qSOFA, NEWS2, Shock Index, and Modified Shock Index for predicting in-hospital mortality. (a) Receiver operating characteristic (ROC) curves of qSOFA, NEWS2, Shock Index, and Modified Shock Index for predicting in-hospital mortality; (b) Forest plot showing the area under the ROC curve with 95% confidence intervals for each scoring system. qSOFA: quick Sequential Organ Failure Assessment; NEWS2: National Early Warning Score 2; AUC: area under the curve.
Discussion
In this retrospective observational study of ED patients with suspected sepsis, we compared the predictive performance of qSOFA, NEWS2, SI, and MSI for in-hospital mortality. NEWS2 demonstrated the highest discriminatory performance, followed by qSOFA, whereas SI and MSI showed lower predictive ability. These findings suggest that NEWS2 may be a more useful early warning tool for risk stratification in patients with sepsis presenting to the ED.
Our findings are consistent with previous studies that have highlighted the superior performance of NEWS2 over qSOFA in predicting adverse outcomes in sepsis. Several large-scale prospective studies and meta-analyses have demonstrated that NEWS2 offers higher sensitivity and better early warning capability compared with qSOFA, particularly in non-ICU settings.11,18,19 Although qSOFA was originally designed for use outside of the ICU as a quick bedside tool, its limited sensitivity has raised concerns in clinical settings where early identification is critical. 23 In contrast, NEWS2 incorporates more comprehensive physiological parameters, including oxygen saturation and supplemental oxygen use, which may contribute to its enhanced discriminative ability in identifying high-risk patients.24,25
In the present study, the superiority of NEWS2 was further supported by pairwise comparisons using DeLong’s test, which showed that NEWS2 performed significantly better than qSOFA, SI, and MSI, whereas the differences among qSOFA, SI, and MSI were not statistically significant. In addition to AUC-ROC, sensitivity and specificity should also be considered when evaluating the clinical usefulness of early warning scores. In our cohort, NEWS2 showed the highest sensitivity and NPV, supporting its role as a potentially useful early screening tool in the ED, whereas qSOFA provided lower sensitivity despite acceptable overall discrimination. These findings are broadly consistent with previous studies,26–28 which also suggested that NEWS2 may offer a more favorable balance of discrimination and early detection in patients with sepsis or suspected sepsis.
Although SI and MSI are simple and quick to calculate, our results indicate that their predictive performance was inferior to that of NEWS2 and not significantly different from that of qSOFA. This is consistent with previous reports, which concluded that although SI and MSI have prognostic value in acute care settings, they are less accurate than composite scoring tools for sepsis mortality prediction.1,14,15,29 This may be due to their limited scope, as they rely only on heart rate and systolic blood pressure, and may not capture other key physiological disturbances in patients with sepsis. Nonetheless, SI and its modified versions remain useful in certain clinical contexts, especially for their simplicity in triage environments.
In multivariate analysis, qSOFA ≥2, MSI ≥1.3, elevated lactate, and comorbidities such as chronic kidney disease were independently associated with in-hospital mortality. These findings reinforce the multifactorial nature of sepsis-related mortality and underscore the importance of considering both physiological scores and underlying comorbidities in clinical decision making.
This study has several strengths, including the use of real-world ED data and head-to-head comparison of widely adopted risk scores. However, several limitations must also be acknowledged. First, the sample size was relatively small and drawn from a single-center, which may limit generalizability. Second, the retrospective design may have introduced selection and information bias. Approximately 10% of initially screened patients were excluded because of missing data, which may have further introduced selection bias and limited the generalizability of the findings. Third, the diagnostic classification of sepsis was based on clinical assessment rather than strictly confirmed infection with organ dysfunction, which may have led to misclassification in some cases. Finally, although NEWS2 showed strong discriminatory performance in our cohort, this finding should be interpreted cautiously given the relatively small sample size and lack of external validation. Despite these limitations, our findings provide useful insights into the comparative performance of early warning scores in the emergency setting. Future studies with larger multicenter cohorts and prospective designs are warranted to validate and expand upon these results.
Conclusion
Among qSOFA, NEWS2, SI, and MSI, NEWS2 showed the best predictive performance for in-hospital mortality in ED patients with suspected sepsis. Although qSOFA, SI, and MSI were also associated with mortality risk, their overall predictive performance was lower than that of NEWS2. These findings suggest that NEWS2 may be a more useful tool for early risk stratification in this setting, although further validation in larger prospective multicenter studies is needed.
Footnotes
Acknowledgments
The authors thank the staff of Rudong County People’s Hospital for their support in clinical data management.
Author contributions
Xiao Wang and Hua Miao conceived and designed the study. Xiao Wang collected the data, performed the statistical analysis, and drafted the manuscript. Yan Wang and Jie She contributed to data interpretation and critically revised the manuscript for important intellectual content. Hua Miao supervised the study and revised the manuscript. All authors read and approved the final manuscript.
Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by the Nantong Municipal Health Commission Scientific Research Project (Project No. MSZ2025098).