
Abstract
Objective
Glucagon-like peptide-1 receptor agonists are established for weight management and cardiovascular risk reduction, with emerging evidence for kidney protection. Whether albuminuria-lowering effects extend to nondiabetic chronic kidney disease remains uncertain.
Methods
We performed a Preferred Reporting Items for Systematic Reviews and Meta-Analyses–guided meta-analysis of randomized controlled trials comparing glucagon-like peptide-1 receptor agonists with placebo or standard care. Primary outcomes were change in body weight (kg) and percentage change in urinary albumin-to-creatinine ratio; change in estimated glomerular filtration rate was the secondary outcome. We conducted prespecified subgroup analyses (including glycemic status) and random-effects meta-regression to explore heterogeneity. Risk of bias assessment (2.0), small-study effects (funnel plot and trim-and-fill analyses), sensitivity analyses (leave-one-out and low-risk-only), and Grading of Recommendations Assessment, Development and Evaluation certainty ratings were applied.
Results
Ten trials (n = 26,088) were included. Glucagon-like peptide-1 receptor agonists reduced body weight (mean difference, −5.85 kg; 95% confidence interval: −7.78 to −3.92) with a consistent direction of effect across studies despite heterogeneity. Glucagon-like peptide-1 receptor agonists lowered urinary albumin-to-creatinine ratio overall (mean difference, −27.94%; 95% confidence interval: −37.72 to −18.15). Stratified analyses showed a precise reduction in type 2 diabetes mellitus (mean difference, −25.70%; I2 = 0%) and a directionally concordant but less precise reduction in populations without type 2 diabetes mellitus (mean difference, −30.93%; I2 = 96%). A modest between-group difference in estimated glomerular filtration rate was also observed (mean difference, −0.82 mL/min/1.73 m2; I2 = 0%). Meta-regression indicated attenuation with longer treatment duration and greater benefit with higher baseline albuminuria; drug class and glycemic status were not consistent moderators of urinary albumin-to-creatinine ratio in prespecified subgroups. Findings were robust to multiple sensitivity analyses. Certainty of evidence was high for weight and moderate for urinary albumin-to-creatinine ratio.
Conclusions
Glucagon-like peptide-1 receptor agonists were associated with clinically meaningful weight loss and lower urinary albumin-to-creatinine ratio across included trials. A directionally similar signal was observed in populations without type 2 diabetes mellitus, although interpretation of this subgroup remains limited by heterogeneity, imprecision, and the inability to evaluate intermediate glycemic phenotypes. Variability in urinary albumin-to-creatinine ratio estimates appears to reflect duration and baseline risk more than a lack of effect.
Keywords
Introduction
Chronic kidney disease (CKD) is a progressive and irreversible condition that has emerged as a major global public health challenge, associated with substantial morbidity, mortality, and healthcare expenditure.1,2 Albuminuria, typically quantified by the urinary albumin-to-creatinine ratio (UACR), is a cardinal sign of kidney damage and one of the most powerful predictors of both CKD progression to end-stage renal disease (ESRD) and incident cardiovascular events.3,4 Type 2 diabetes mellitus (T2DM) remains the leading cause of CKD worldwide, 5 with diabetic kidney disease (DKD) accounting for a significant proportion of patients requiring renal replacement therapy. 6
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) have fundamentally altered the treatment landscape for T2DM. 7 Beyond their robust glucose-lowering effects, this class of medications provides significant multisystem benefits, including substantial weight loss, blood pressure reduction, and proven cardiovascular protection, as demonstrated in large-scale cardiovascular outcome trials (CVOTs) such as REWIND and EXSCEL.8,9 A growing body of evidence from these trials has also highlighted the renoprotective potential of GLP-1RAs, primarily through secondary analyses showing a consistent reduction in the incidence or worsening of albuminuria.10,11
Evidence for kidney benefit in patients with T2DM and CKD was strengthened by the landmark FLOW trial, which was stopped early because of overwhelming efficacy. FLOW demonstrated that semaglutide reduced the risk of major kidney outcomes in patients with T2DM and established CKD. 12 However, whether similar benefit extends to nondiabetic populations remains uncertain. The mechanisms underlying this protection are thought to be multifactorial, including glucose-dependent pathways (improved glycemic control and weight loss) and, hypothetically, glucose-independent pathways (direct anti-inflammatory, antifibrotic, and renal hemodynamic effects). 13
However, the efficacy of GLP-1RAs in reducing albuminuria in patients without T2DM is far less established. 14 Clarifying this issue is important, as it may help determine whether the observed reduction in albuminuria extends beyond diabetic populations. Therefore, we conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) to quantify the overall effect of GLP-1RAs on UACR. The primary objective was to determine the magnitude of UACR reduction and, specifically, to investigate whether this effect is consistent across broad patient subgroups with and without T2DM and recognizing that intermediate glycemic phenotypes such as prediabetes could not be examined using the available trial-level data.
Methods
Τhis systematic review and meta-analysis was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement. 15 This study was registered post-study at INPLASY (Registration Number: INPLASY202650012).
Search strategy
We performed a comprehensive search of PubMed/MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL) from their inception to October 2025. The search strategy combined Medical Subject Headings (MeSH) and free-text keywords for “GLP-1 receptor agonists” (e.g. “semaglutide,” “liraglutide,” “dulaglutide,” “exenatide”) and terms related to renal outcomes (e.g. “albuminuria,” “Urine Albumin-to-Creatinine Ratio,” “UACR,” “chronic kidney disease,” “renal function”). We also manually screened the reference lists of included articles and relevant systematic reviews to identify additional eligible studies. The detailed search strategy is shown in Supplementary Table S1.
Study selection
Two independent reviewers (Jun Xu and Zhen Wang) screened all retrieved titles and abstracts. Full texts of potentially relevant articles were then assessed for final inclusion based on predefined criteria. Disagreements were resolved by consensus or consultation with a third reviewer (Qingshen Gao). Inclusion criteria were as follows: 1. The study design was an RCT. 2. Participants were adults with CKD or at high risk for renal or cardiovascular events. 3. The intervention was a GLP-1RA compared with placebo or standard/active care. 4 The outcome of interest, change in UACR, was reported. Exclusion criteria were as follows: (a) nonrandomized or observational studies; (b) case reports, reviews, or animal studies; (c) studies that did not report UACR data; and (d) duplicate publications.
Data extraction
The two reviewers independently extracted data using a standardized form. Extracted data included the following: (a) study characteristics (first author, publication year, and study design); (b) participant demographics (sample size, mean age, T2DM status, baseline eGFR (estimated glomerular filtration rate), and baseline UACR); (c) intervention details (drug type, dose, and duration); and (d) outcome data (mean change in UACR and its measure of dispersion, such as the 95% confidence interval (CI), SD, or standard error (SE)). The Cochrane Risk of Bias 2 (RoB 2) tool was used to assess the quality and risk of bias for each included RCT.
Quality assessment
Methodological quality was assessed using the Cochrane Risk of Bias tool (RoB 2.0), considering the randomization sequence, allocation concealment, blinding, attrition, outcome measurement, and reporting. Certainty of evidence was graded using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework (domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias), with ratings assigned for each outcome (body weight, UACR, and eGFR).
Outcomes
Co-primary outcomes were (a) mean difference (MD) in body weight (kg) and (b) percentage change in UACR. Secondary outcomes were MD in eGFR, systolic blood pressure (SBP), and glycated hemoglobin (HbA1c). UACR was synthesized as percent change; when appropriate, log-transformed ratios were harmonized back to percent change for interpretation.
Statistical analysis
Random-effects meta-analysis (restricted maximum likelihood (REML)) was performed to pool MDs with 95% CIs; heterogeneity was quantified using τ2 and I2, and 95% prediction intervals were reported. Prespecified subgroup analyses tested interaction by glycemic status (T2DM vs non-T2DM), drug class (semaglutide vs exenatide), treatment duration (≤ vs > prespecified threshold), ethnicity proportion, baseline eGFR (>60 vs ≤60 mL/min/1.73 m2), baseline UACR (>300 vs ≤300 mg/g), and prevalence of lipid-lowering or antihypertensive therapy. To further explore heterogeneity, random-effects meta-regression (REML with Knapp–Hartung adjustment) was performed to evaluate study-level moderators (e.g. duration of treatment, baseline UACR burden, glycemic status, and concomitant therapies). Small-study effects were assessed using funnel plots and trim-and-fill analysis; where applicable, Egger's test was considered. Sensitivity analyses included leave-one-out influence diagnostics, restriction to low-risk-of-bias studies, and exclusion of T2DM trials to verify the nondiabetic signal. Analyses used two-sided α of 0.05; computations were conducted in R (‘metafor’ package).
Results
Literature search and study selection
A comprehensive literature search was conducted in PubMed, Embase, and the Cochrane Library from inception to October 2025, using combinations of the terms “GLP-1 receptor agonist,” “dual agonist,” “type 2 diabetes,” “chronic kidney disease,” “UACR,” and “weight change.” Reference lists of relevant reviews and clinical trials were also screened to identify additional eligible studies. After removing duplicates and excluding reviews, observational studies, and reports without extractable data, a total of 10 RCTs met the inclusion criteria and were included in the quantitative synthesis (Figure 1).
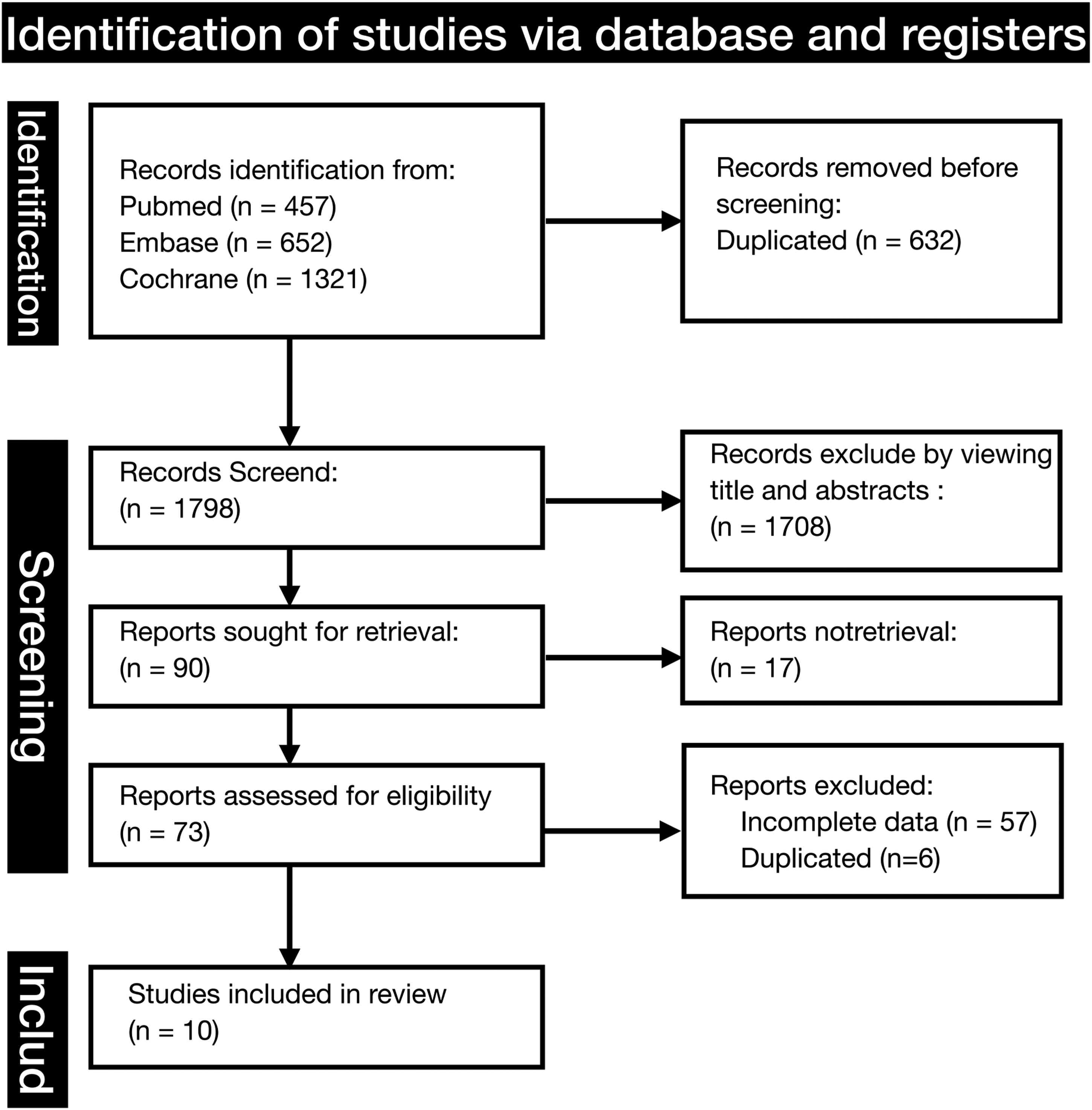
PRISMA flow diagram of the literature search and study selection process.
Study and participants characteristics
Ten RCTs comprising 26,088 participants were included. The mean age was 61.2 years, 31.7% of participants were women, and baseline body mass index (BMI) averaged 33.1 kg/m2. Kidney function at entry was moderately reduced overall (mean eGFR, 76.8 mL/min/1.73 m2). Trial sample sizes ranged from 33 to 17,604 participants. Seven studies enrolled participants with T2DM and three enrolled nondiabetic cohorts. Interventions predominantly evaluated GLP-1RAs (mainly semaglutide; several trials used exenatide) versus placebo or standard care. Baseline characteristics were generally balanced across treatment arms (Table 1).16–25
Baseline characteristics of the included randomized controlled trials and study participants.
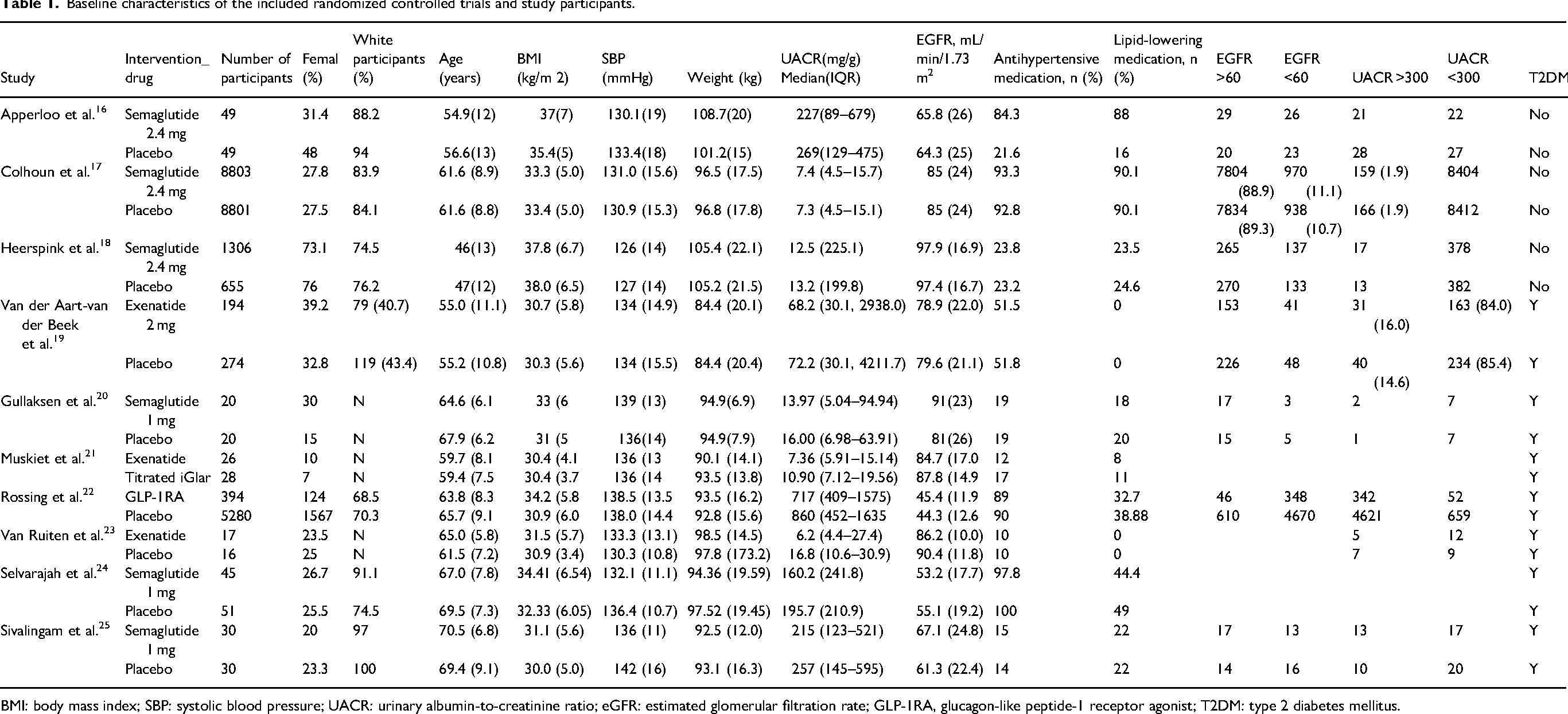
BMI: body mass index; SBP: systolic blood pressure; UACR: urinary albumin-to-creatinine ratio; eGFR: estimated glomerular filtration rate; GLP-1RA, glucagon-like peptide-1 receptor agonist; T2DM: type 2 diabetes mellitus.
UACR was reported in all trials, with participant-level distributions available in 8 studies covering 25,938 participants. Across these studies, 72.5% of participants had a UACR <300 mg/g at baseline, indicating that most had normal to moderately increased albuminuria at enrollment; the remainder had higher albuminuria. These UACR profiles were broadly comparable between intervention and control groups within each trial, supporting valid between-group comparisons for renal outcomes.
Efficacy of GLP-1RAs on body weight
In the pooled analysis of 10 RCTs, GLP-1RA therapy demonstrated a significant reduction in body weight compared with placebo or standard care (MD, −5.85 kg, 95% CI: −7.78 to −3.92; P < 0.0001; Figure 2). Despite substantial heterogeneity (I2 = 86%, τ2 = 5.25; P < 0.0001), the direction of effect was consistent across studies, and the prediction interval (−11.4 to −0.3) supported generalizability.
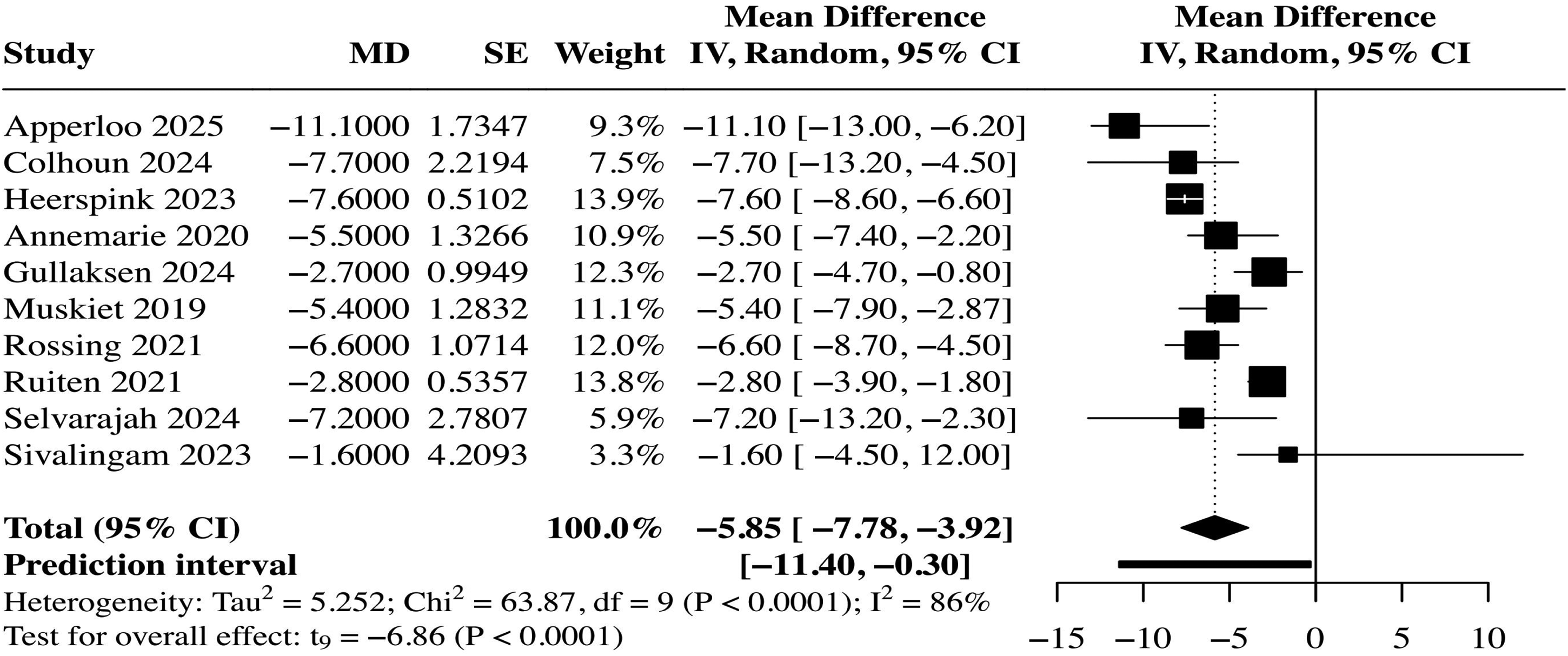
Forest plot of the effect of GLP-1 receptor agonists versus control on body weight (kg).
Subgroup analyses identified several potential effect modifiers (Table 2). The magnitude of weight reduction was significantly greater in trials enrolling non-T2DM participants (MD, −8.49 kg, 95% CI: −13.07 to −3.91) compared with those including participants with T2DM (MD, −4.50 kg, 95% CI: −6.24 to −2.75; seven studies; I2 = 64%; P for interaction = 0.002). Furthermore, larger reductions were observed in studies with a higher proportion of White participants (MD, −9.18 vs −4.96 kg; P for interaction = 0.005) and those with more prevalent use of concomitant lipid-lowering therapy (MD, −9.68 vs −5.10 kg; P for interaction = 0.013) or antihypertensive therapy (MD, −7.41 vs −3.21 kg; P for interaction < 0.001). In contrast, drug class (semaglutide vs. exenatide; P for interaction = 0.275) and treatment duration (P for interaction = 0.961) did not materially modify efficacy. Baseline renal function measures (UACR, P for interaction = 0.136; eGFR, nominal P for interaction = 0.013) also did not consistently influence weight outcomes. Because these subgroup findings were derived from aggregate trial-level characteristics rather than individual patient data, they should be interpreted as exploratory rather than definitive evidence of treatment interaction.
Subgroup analyses of body weight reduction and secondary outcome analysis for eGFR.
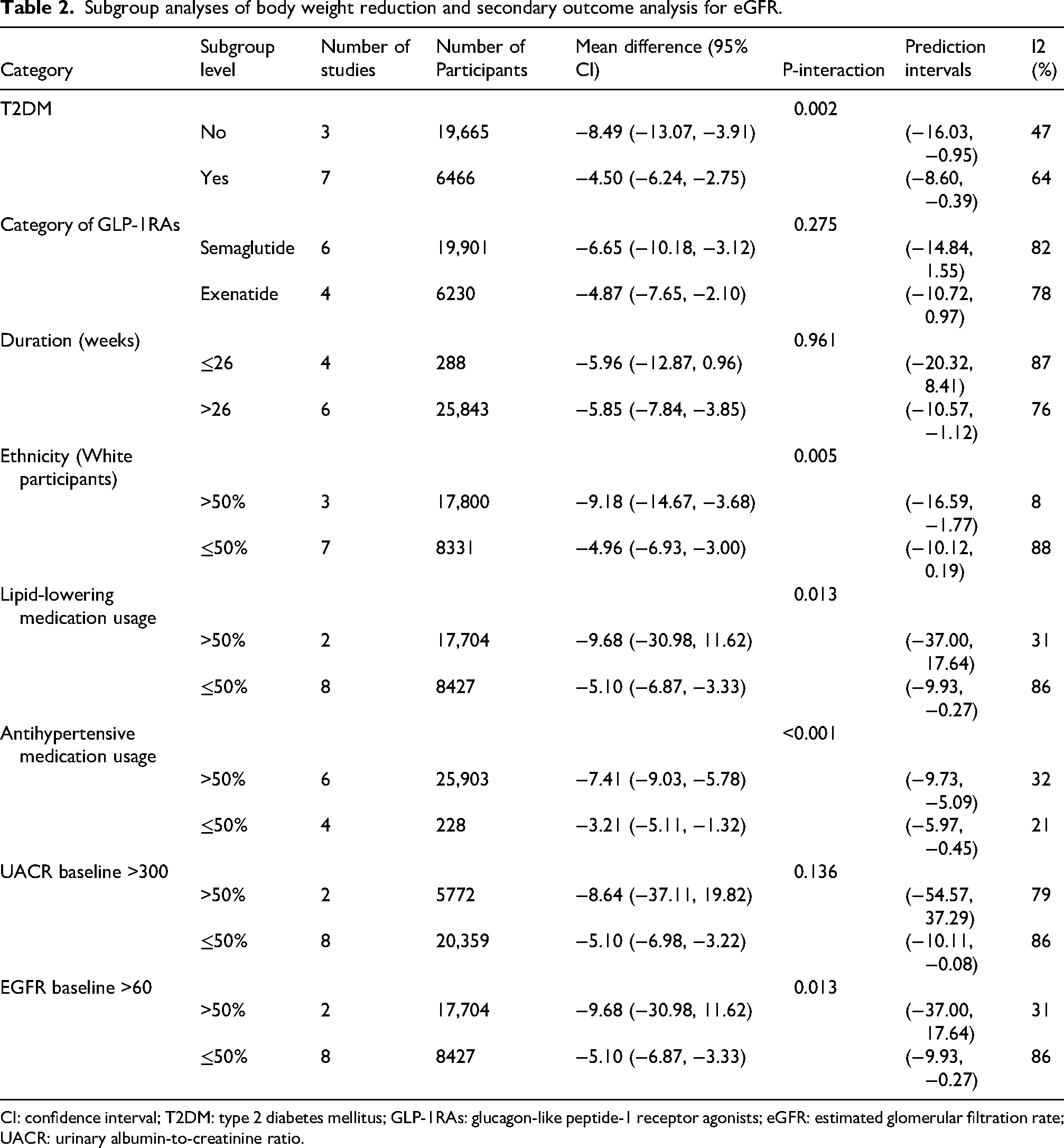
CI: confidence interval; T2DM: type 2 diabetes mellitus; GLP-1RAs: glucagon-like peptide-1 receptor agonists; eGFR: estimated glomerular filtration rate; UACR: urinary albumin-to-creatinine ratio.
Efficacy of GLP-1RAs on UACR (primary renal outcome)
GLP-1RA therapy significantly reduced the primary renal outcome, UACR, in the overall pooled analysis (MD, −27.94%, 95% CI: −37.72 to −18.15; P = 0.0002; Figure 3), with a consistent direction of effect and moderate heterogeneity (I2 = 26%, τ2 = 132.87; P < 0.0001). Stratification by glycemic status suggested that the albuminuria-lowering effect may also be present in nondiabetic populations. As shown in Figure 4, the effect was observed in both subgroups. The T2DM subgroup (seven studies) showed a precise and highly consistent reduction (MD, −25.70%, 95% CI: −29.42 to −21.97; I2 = 0%). Concurrently, the non-T2DM subgroup (three studies) exhibited a numerically larger, albeit less precise, decrease (MD, −30.93%, 95% CI: −82.25 to 20.39; I2 = 96%).
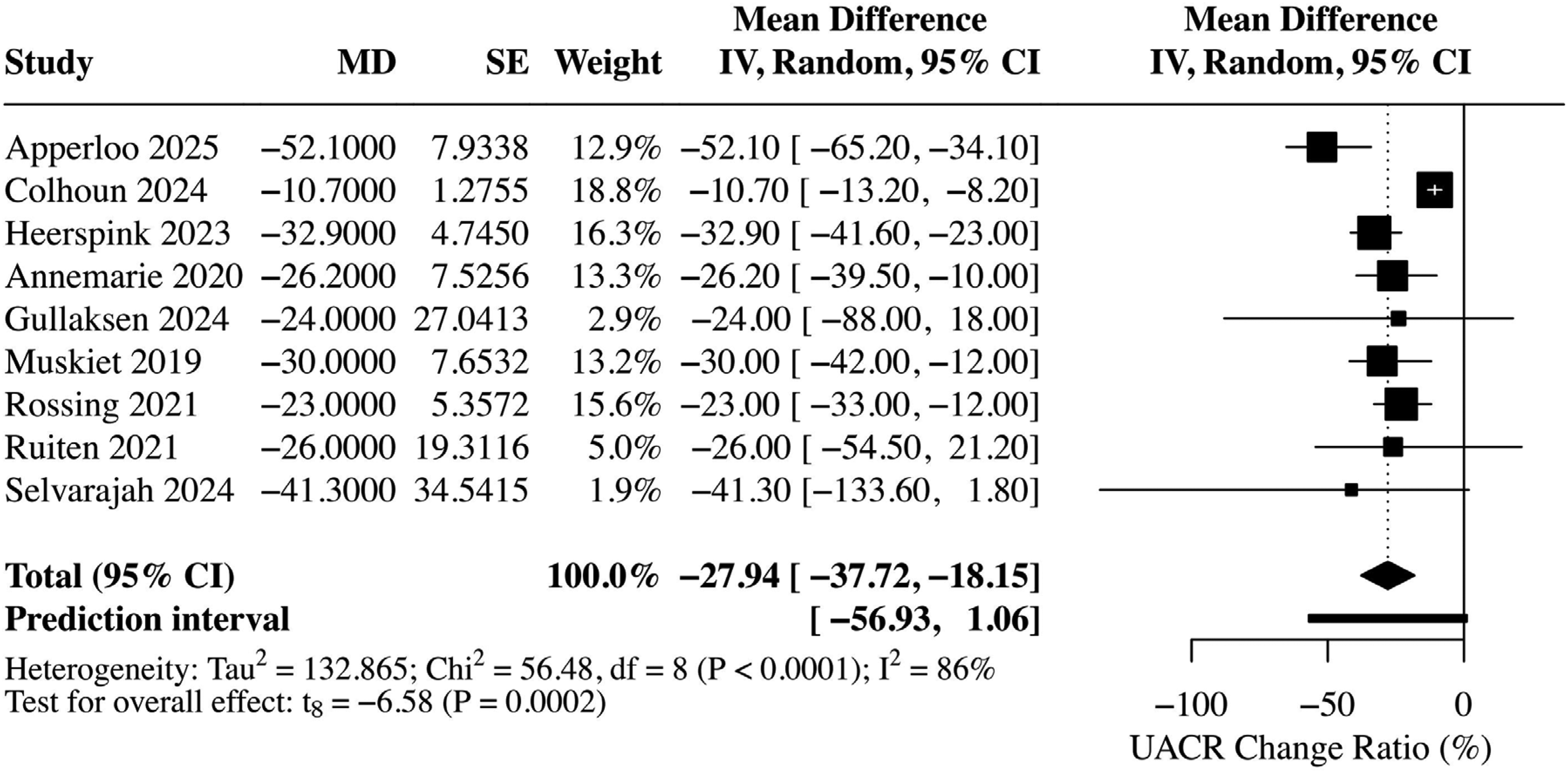
Forest plot of the effect of GLP-1 receptor agonists on percentage change in urinary albumin-to-creatinine ratio (UACR).
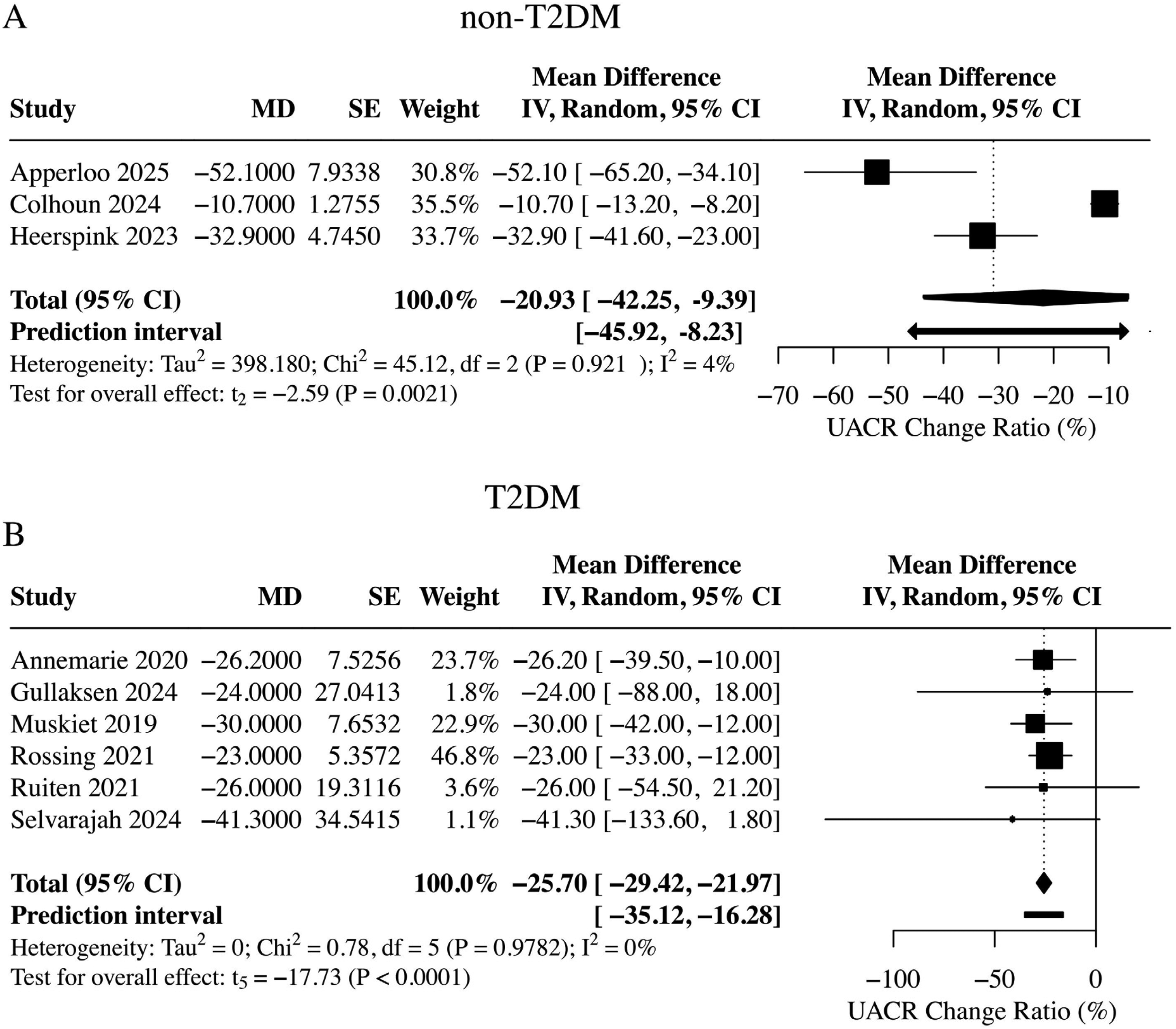
Forest plot of UACR reduction stratified by glycemic status (T2DM vs. non-T2DM).
The concordant direction of effect across these strata, further corroborated by Table 3, suggests that the albuminuria-lowering effect of GLP-1RAs may not be limited to patients with T2DM. However, the wide CI and substantial heterogeneity in the non-T2DM group warrant cautious interpretation. A small but statistically significant between-group difference in eGFR was also observed (MD, −0.82 mL/min/1.73 m2, 95% CI: −0.92 to −0.72; P < 0.001; I2 = 0%; Table 2). However, because eGFR was a secondary outcome and hard renal outcomes were not assessed, this finding should be interpreted cautiously. In parallel, BMI decreased markedly (MD, −24.92%, 95% CI: −28.13 to −21.71; I2 = 0%), SBP fell modestly (MD, −4.03 mmHg, 95% CI: −5.05 to −3.02; I2 = 0%), and HbA1c showed a non-significant trend toward reduction (MD, −0.80%, 95% CI: −1.70 to 0.09; P = 0.072; I2 = 97%) (Table 3). Taken together, these metabolic and hemodynamic improvements provide biological plausibility for the observed reduction in albuminuria and indicating that the observed effect may not be exclusively mediated by glycemic control.
Pooled analysis of secondary metabolic and hemodynamic outcomes: BMI, systolic
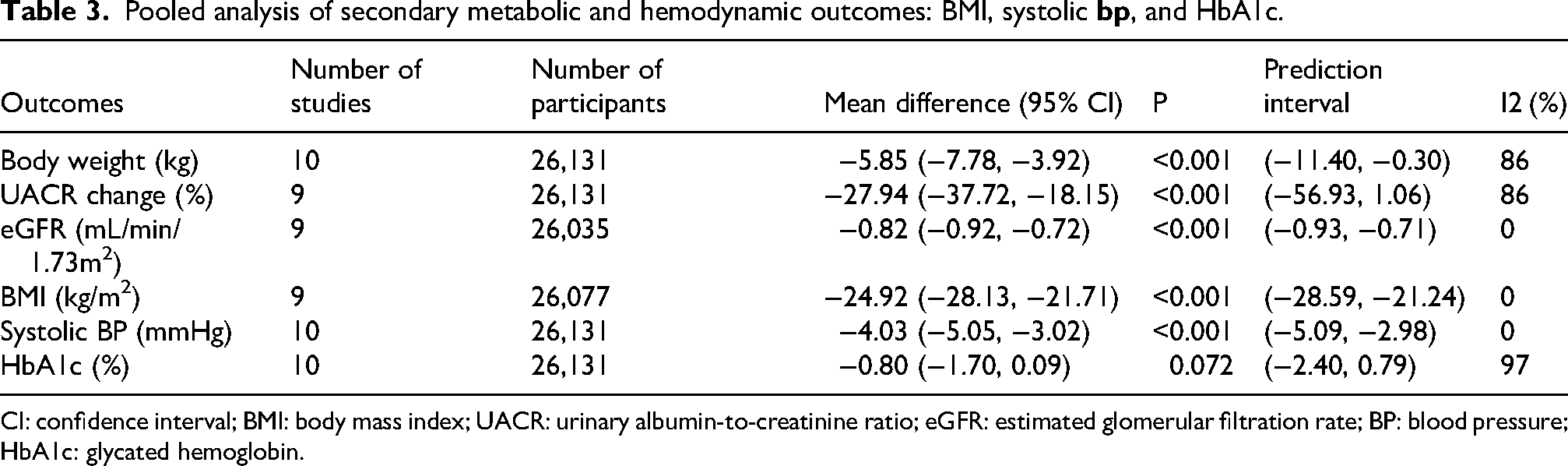
CI: confidence interval; BMI: body mass index; UACR: urinary albumin-to-creatinine ratio; eGFR: estimated glomerular filtration rate; BP: blood pressure; HbA1c: glycated hemoglobin.
Subgroup analysis of UACR effect modifiers
Based on the subgroup analysis (Table 4), treatment duration appeared to influence the magnitude of albuminuria reduction, with shorter trials showing greater decreases (MD, −34.1%, 95% CI: −48.7 to −19.5) than longer trials (MD, −23.4%, 95% CI: −39.8 to −7.1; P for interaction = 0.16). However, this trend did not reach statistical significance. T2DM status likewise did not significantly modify the effect (P for interaction = 0.65): both T2DM and non-T2DM groups showed reductions in UACR, with a numerically larger but less precise effect in non-T2DM. No significant differences were found across drug class, ethnicity, concomitant lipid-lowering or antihypertensive therapy, baseline eGFR, or baseline UACR strata. Although negative, these findings are clinically informative because they suggest that the albuminuria-lowering signal was not obviously restricted to a single study-defined subgroup. Overall, these findings suggest that GLP-1RAs reduce albuminuria across diverse study populations. However, the estimate in the non-T2DM subgroup was less precise and should be interpreted cautiously because of the limited number of studies, substantial heterogeneity, and the inability to assess intermediate glycemic phenotypes such as prediabetes.
Subgroup analyses of effect modifiers for the change in UACR.
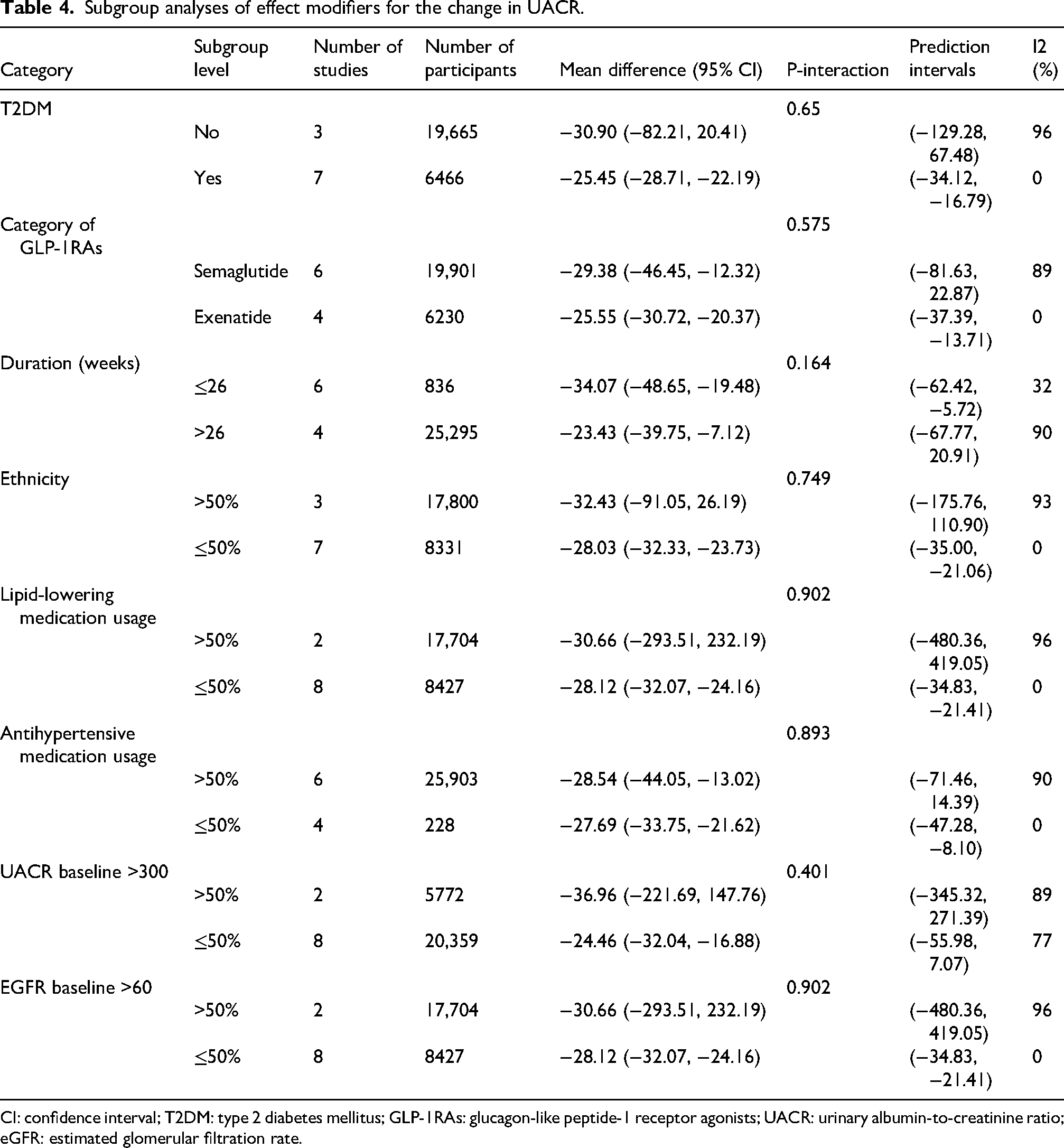
CI: confidence interval; T2DM: type 2 diabetes mellitus; GLP-1RAs: glucagon-like peptide-1 receptor agonists; UACR: urinary albumin-to-creatinine ratio; eGFR: estimated glomerular filtration rate.
To further explore sources of heterogeneity, we performed a random-effects meta-regression, which identified several study-level moderators of UACR change. Trials enrolling participants with T2DM exhibited attenuated albuminuria reduction relative to non-T2DM (coefficient, +51.69%; 95% CI: 20.84–82.54), and longer treatment duration was likewise associated with a smaller reduction (+19.67%, 8.70–30.63). In contrast, a higher baseline UACR burden was associated with greater reductions in albuminuria (coefficient, −19.37%, −30.92 to −7.82). A higher prevalence of antihypertensive therapy was also linked to attenuation (+21.55%, 4.75–38.36). Drug category (semaglutide vs exenatide), ethnicity, and lipid-lowering therapy were not significant moderators (95% CIs crossed 0). These model-based results align with the subgroup analyses by duration and glycemic status, although interpretation of glycemic-status subgroup differences remains limited by the lack of patient-level glycemic phenotyping (Figure S1 and Table S2).
Heterogeneity and sensitivity analyses
Across outcomes, heterogeneity was generally moderate to substantial. For the renal endpoint (UACR), a leave-one-out analysis confirmed a stable direction and significance of the pooled effect (overall MD, approximately −27% with t9 = −7.04, P < 0.0001), despite high between-study variability (overall I2, approximately 84%, τ2, approximately 120.6) (Figure S2). Sensitivity analyses restricted to low-risk-of-bias trials (Table S3) yielded consistent results for both primary endpoints, with slightly reduced heterogeneity and unchanged directionality, confirming methodological stability. Similarly, exclusion of T2DM studies (Table S4) did not materially affect the pooled estimates, supporting the robustness of the overall albuminuria-lowering signal, and not eliminating uncertainty in the nondiabetic subgroup.
Collectively, these findings indicate that the overall albuminuria-lowering effect of GLP-1RAs was robust to influential-study removal. However, uncertainty remained regarding the magnitude and interpretation of the effect in the non-T2DM subgroup because of the limited number of studies, substantial heterogeneity, and the absence of patient-level glycemic phenotyping.
Assessment of bias and evidence certainty
The overall risk of bias across the included studies was judged to be low to moderate (Table S1). Random sequence generation and allocation concealment were adequately reported in nearly all trials (Figure S3 to S4). Blinding of participants, investigators, and outcome assessors was clearly described in more than 80% of studies. No major concerns were identified regarding attrition or selective reporting, and all primary outcomes were prespecified in the trial protocols.
According to the GRADE framework, the certainty of evidence was rated as high for body weight reduction and moderate for UACR outcomes, with the latter downgraded for minor imprecision and inter-study heterogeneity. Overall, these findings indicate high-quality and consistent evidence for metabolic benefit and moderate-certainty evidence for reduction in UACR. Interpretation of kidney-related benefit across populations, particularly in non-T2DM groups, should remain cautious because the renal analyses relied primarily on surrogate outcomes and the nondiabetic subgroup was imprecise.
Begg's funnel plot suggested asymmetry (Figure S5), and Egger's test was significant (P = 0.022). Using Duval and Tweedie's trim-and-fill method, the adjusted pooled effect indicated a slightly larger weight reduction (MD, −11.32 kg, 95% CI: −13.30 to −9.34; Figure S6), without changing the direction of effect. These findings suggest potential small-study effects; however, the primary conclusions remain robust.
Discussion
This meta-analysis confirms that GLP-1RAs provide a statistically significant and clinically meaningful reduction in UACR. This finding aligns with previous meta-analyses and secondary analyses of major CVOTs, including REWIND and EXSCEL, supporting a favorable effect of this drug class on albuminuria.26,27 The landmark FLOW trial, which studied semaglutide in T2DM with CKD, provides evidence of hard kidney outcome benefit in a diabetic CKD population. 28 However, because our analysis primarily focused on UACR and did not assess hard renal outcomes, our findings should not be interpreted as direct evidence of renal protection at the level of kidney failure events or sustained kidney function decline.
An important finding from our subgroup analysis was that a directionally similar reduction in UACR was also observed in patients without T2DM. This is a crucial distinction, as benefits were often presumed to be secondary to glycemic control. However, this subgroup included only a limited number of studies and showed substantial heterogeneity; therefore, the non-T2DM findings should be interpreted cautiously. Moreover, this comparison represents a broad clinical subgroup analysis rather than a definitive separation across the full glycemic continuum, because prediabetes and related intermediate phenotypes could not be assessed using the available trial-level data. Thus, the non-T2DM findings should be considered suggestive and hypothesis-generating rather than definitive evidence of benefit. Nevertheless, the biological plausibility of this observation remains considerable. GLP-1 receptors are present in kidney cells, and GLP-1RAs may exert hemodynamic, anti-inflammatory, and anti-oxidative effects that could contribute to lower albuminuria. However, our results do not allow us to distinguish direct renal effects from indirect effects mediated through changes in body weight, glycemia, blood pressure, insulin sensitivity, or systemic inflammation.
Our analysis also aligns with evidence of heterogeneity among agents. Newer drugs such as semaglutide may offer superior UACR reduction compared with older agents,29,30 although this should be regarded as exploratory rather than definitive evidence of potency-dependent renal benefit. Although the magnitude of albuminuria reduction appeared attenuated in longer-duration studies, the direction of effect remained favorable, suggesting that the observed benefit was not merely a transient hemodynamic phenomenon. 31 Our subgroup analyses did not find that baseline eGFR or UACR levels significantly modified the effect, suggesting benefits across a wide spectrum of CKD severity. This contrasts with post hoc analyses such as EXSCEL, which found greater benefits at higher baseline UACR. 32 An additional clinically relevant question is whether baseline kidney disease may attenuate the metabolic efficacy of GLP-1RAs. In our study-level subgroup analysis, baseline renal function measures did not consistently modify the body weight effect of GLP-1RAs; however, the impact of CKD severity on glycemic efficacy could not be robustly evaluated because HbA1c was analyzed only as a secondary outcome and renal-stratified glycemic data were not consistently available across the included trials. Our pooled data suggest that the albuminuria-lowering effect may extend across a broad range of populations, although the evidence in nondiabetic populations remains less precise and should be interpreted cautiously. Taken together, these subgroup and meta-regression analyses provide clinically relevant context regarding where the observed effects appeared more or less pronounced, but they do not establish patient-level interaction effects because detailed adiposity measures and concomitant medication data were not uniformly available across the included trials. Even the absence of significant subgroup modification is informative, as it suggests that the albuminuria-lowering signal was not clearly confined to a single narrow clinical context.
Strengths include our robust subgroup analyses, especially the comparison between T2DM and non-T2DM populations. Several limitations must be acknowledged. First, the analysis was constrained by inter-study heterogeneity and the use of UACR as a surrogate endpoint. Second, hard renal outcomes were not available for pooled analysis. Third, the non-T2DM subgroup included relatively few studies and showed marked heterogeneity, limiting the precision of inference. Fourth, eGFR was a secondary outcome and should not be overinterpreted. Finally, this study relied on study-level rather than patient-level data, which limited more detailed exploration of patient-level effect modifiers, including intermediate glycemic phenotypes such as prediabetes, and reduced the precision of subgroup inference. This also prevented a more robust assessment of whether baseline renal impairment modifies the glycemic efficacy of GLP-1RAs.Additionally, because this study was registered post hoc at INPLASY, post-study registration may have introduced bias and should be considered a limitation.
In conclusion, this meta-analysis provides consolidated evidence that GLP-1RAs significantly reduce albuminuria. A directionally similar effect was also observed in nondiabetic patients; however, this subgroup finding was based on a limited number of studies and showed substantial heterogeneity and should therefore be interpreted cautiously. Taken together, these results support a favorable effect on albuminuria but do not establish definitive renoprotective effects in the absence of hard renal outcomes. Trials evaluating hard renal outcomes in nondiabetic CKD are warranted.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605261458641 - Supplemental material for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605261458641 for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis by Rong Huang and Bin Wang in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605261458641 - Supplemental material for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis
Supplemental material, sj-pdf-2-imr-10.1177_03000605261458641 for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis by Rong Huang and Bin Wang in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_03000605261458641 - Supplemental material for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis
Supplemental material, sj-pdf-3-imr-10.1177_03000605261458641 for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis by Rong Huang and Bin Wang in Journal of International Medical Research
Supplemental Material
sj-pdf-4-imr-10.1177_03000605261458641 - Supplemental material for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis
Supplemental material, sj-pdf-4-imr-10.1177_03000605261458641 for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis by Rong Huang and Bin Wang in Journal of International Medical Research
Supplemental Material
sj-pdf-5-imr-10.1177_03000605261458641 - Supplemental material for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis
Supplemental material, sj-pdf-5-imr-10.1177_03000605261458641 for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis by Rong Huang and Bin Wang in Journal of International Medical Research
Supplemental Material
sj-pdf-6-imr-10.1177_03000605261458641 - Supplemental material for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis
Supplemental material, sj-pdf-6-imr-10.1177_03000605261458641 for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis by Rong Huang and Bin Wang in Journal of International Medical Research
Supplemental Material
sj-png-7-imr-10.1177_03000605261458641 - Supplemental material for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis
Supplemental material, sj-png-7-imr-10.1177_03000605261458641 for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis by Rong Huang and Bin Wang in Journal of International Medical Research
Supplemental Material
sj-png-8-imr-10.1177_03000605261458641 - Supplemental material for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis
Supplemental material, sj-png-8-imr-10.1177_03000605261458641 for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis by Rong Huang and Bin Wang in Journal of International Medical Research
Supplemental Material
sj-png-9-imr-10.1177_03000605261458641 - Supplemental material for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis
Supplemental material, sj-png-9-imr-10.1177_03000605261458641 for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis by Rong Huang and Bin Wang in Journal of International Medical Research
Supplemental Material
sj-png-10-imr-10.1177_03000605261458641 - Supplemental material for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis
Supplemental material, sj-png-10-imr-10.1177_03000605261458641 for Effect of glucagon-like peptide-1 receptor agonists on body weight and urinary albumin-to-creatinine ratio in patients with and without type 2 diabetes: A systematic review and meta-analysis by Rong Huang and Bin Wang in Journal of International Medical Research
Footnotes
Acknowledgments
Not applicable.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
Rong Huang performed the literature search, data extraction, and quality assessment. Bin Wang supervised the study and resolved disagreements. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.