
Abstract
To investigate the clinical characteristics, key diagnostic features, surgical management strategies, and postoperative outcomes of accessory cavitated uterine mass, with the aim of improving diagnostic accuracy and standardizing clinical management. A retrospective analysis was conducted on eight patients with accessory cavitated uterine mass who underwent surgical treatment at Gansu Provincial Maternity and Child Care Hospital between February 2023 and August 2025. Clinical presentation, imaging findings, surgical procedures, pathological results, and postoperative outcomes were systematically reviewed. The patient ages ranged from 19 to 39 years, and all presented with dysmenorrhea. Severe pain was reported in five patients (62.5%). Preoperative ultrasonography and pelvic magnetic resonance imaging suggested accessory cavitated uterine mass in all cases. Lesions were located on the left side in six patients (75%). The mean lesion diameter was 3.1 ± 0.62 cm. All patients successfully underwent laparoscopic excision without intraoperative or postoperative complications. During follow-up through October 2025, no recurrences were observed. Complete resolution of dysmenorrhea was achieved in seven patients. Accessory cavitated uterine mass primarily affects young women, with progressively worsening dysmenorrhea being the hallmark clinical presentation. Ultrasound combined with magnetic resonance imaging is the key diagnostic method. Laparoscopic excision is an effective, fertility-preserving treatment option with favorable postoperative outcomes.
Keywords
Introduction
Accessory cavitated uterine mass (ACUM) is a rare congenital obstructive malformation of the female reproductive tract. Although traditionally believed to be a subtype of Müllerian duct abnormalities, emerging evidence suggests that ACUM may originate from gubernacular dysfunction. The gubernaculum is the primitive structure that develops into the round ligament during embryogenesis and is responsible for guiding the descent and localization of the Müllerian duct. Impairment of this guiding function can lead to ectopic retention of local Müllerian duct tissue, which may ultimately differentiate into functional endometrium and smooth muscle-wrapping structures.1,2 ACUM was first formally described and named by Acién et al. 3 in 2010 based on previously reported similar cases and their summarized clinical characteristics. ACUM is characterized by an isolated, noncommunicating cavitated mass located within the myometrium, typically beneath the insertion of the round ligament, and lined by functional endometrial tissue. The inability to drain menstrual blood from the cavity leads to periodic increases in intracavitary pressure, resulting in progressively worsening dysmenorrhea and a substantial reduction in quality of life.4,5 However, because of its rarity and nonspecific clinical manifestations, ACUM is easily misdiagnosed as cystic adenomyosis or cystic degeneration of a myoma, resulting in delayed diagnosis and inappropriate management. Previous studies suggest that ACUM predominantly affects young women of reproductive age. Conservative medical treatments, including nonsteroidal anti-inflammatory drugs, oral contraceptives, and gonadotropin-releasing hormone agonists, may provide temporary symptom relief but are generally ineffective in achieving sustained pain control. Symptoms frequently recur after discontinuation of pharmacologic therapy. In contrast, surgical excision offers definitive symptom relief while preserving uterine integrity and reproductive potential.3,6 Despite increasing recognition of ACUM, the condition remains underdiagnosed in routine clinical practice. Most published data consist of isolated case reports or small case series, and standardized diagnostic and therapeutic strategies have yet to be established. In this study, we retrospectively analyzed the clinical characteristics, imaging findings, surgical management, and postoperative outcomes of eight patients with pathologically confirmed ACUM, aiming to enhance awareness of this rare entity and provide practical guidance for optimizing diagnosis and treatment.
Materials and methods
General information
Eight patients with ACUM who underwent surgical treatment at Gansu Provincial Maternal and Child Health Hospital (Gansu Provincial Central Hospital) from February 2023 to August 2025 were included. The patient ages ranged from 19 to 39 years, with a median age of 27 years; seven patients (87.5%) were younger than 30 years. All patients provided signed informed consent for the surgical procedure. Additionally, written informed consent for publication of clinical data and images was obtained from each patient. The study was approved by the Institutional Review Board of Gansu Provincial Maternity and Child Care Hospital (Approval No. 2020-SL-68; approval date: 8 November 2022). Diagnosis was established based on postoperative pathological confirmation in conjunction with preoperative clinical presentation and imaging findings, according to previously published diagnostic criteria: 3 (a) normal development of the uterine cavity, ovaries, and fallopian tubes; (b) an isolated, noncommunicating cystic lesion located beneath the uterine round ligament; (c) imaging demonstrating endometrioid echoes and hemorrhagic signals within the cyst cavity; and (d) postoperative pathology confirming that the cyst wall contains smooth muscle tissue and endometrial glands and stroma.
Data collection
Clinical data from the eight patients were collected, including age, gravidity and parity, clinical symptoms, preoperative tumor markers, ultrasonographic findings, pelvic magnetic resonance imaging (MRI) findings, hysteroscopic findings, surgical details, postoperative pathological outcomes, and prognosis. No notable findings were identified in the family, psychological, social, or genetic history.
Follow-up
Patients were followed through October 2025, with a median follow-up duration of 9.5 months (range: 2–32 months). Follow-up assessments included symptom relief and fertility outcomes.
Compliance with reporting guidelines
The reporting of this case series conforms to the CAse REport (CARE) guidelines. 7 All patient information was de-identified.
Results
Clinical symptoms
All patients presented with dysmenorrhea as the primary clinical symptom. Five patients (62.5%) reported progressively worsening dysmenorrhea, with symptom duration ranging from 1 to 12 years. One patient additionally reported intermittent unilateral lower abdominal pain lasting 4 years. Pain severity, assessed using the visual analog scale (VAS), ranged from 3 to 8. Severe pain (VAS ≥7) was observed in five patients (62.5%), all of whom had previously received nonsteroidal anti-inflammatory drugs with limited symptom relief. Four patients had no history of pregnancy and were relatively young (19–26 years), whereas the remaining four patients (27–39 years) had experienced at least one successful delivery (Table 1).
Characteristics of all patients.
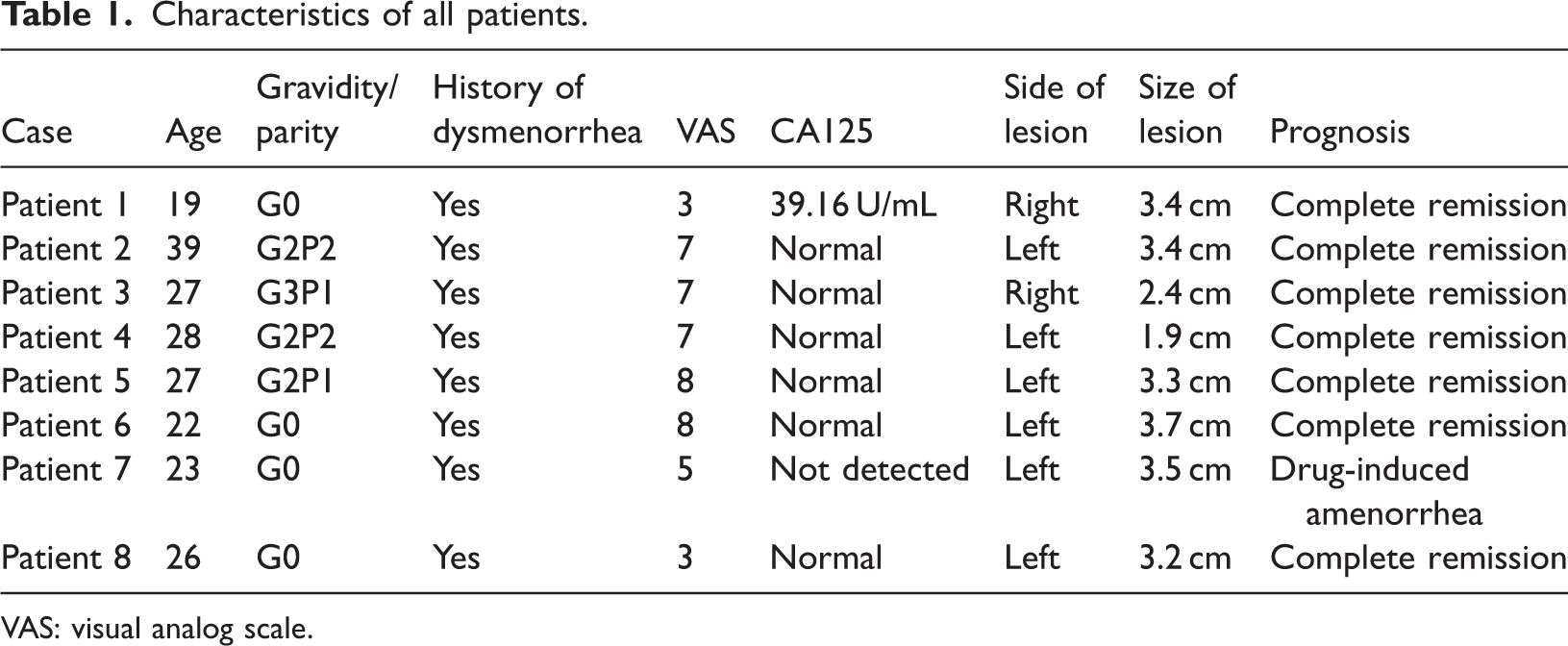
VAS: visual analog scale.
Timeline of diagnosis and treatment
The clinical course from symptom onset to surgical intervention and follow-up is summarized as follows (median values or ranges across the eight patients):
Onset of dysmenorrhea
All patients reported symptom onset 1–12 years before diagnosis (median, 4 years).
First medical consultation
Patients sought medical care at a median of 2 years after symptom onset (range: 0.5–8 years).
Preoperative imaging (ultrasound and MRI)
Preoperative imaging was performed within 1–3 months before surgery in all patients.
Laparoscopic excision
Surgery was performed between February 2023 and August 2025, when patients were aged 19–39 years.
Postoperative follow-up
Follow-up was conducted through October 2025, with a median duration of 9.5 months (range: 2–32 months). No recurrences or pregnancies were recorded during this period.
Auxiliary inspection
Tumor markers
Serum CA125 levels were assessed in seven patients. Mild elevation (39.16 U/mL; normal reference value ≤35 U/mL) was observed in one patient, whereas levels in the remaining patients were within the normal range (Table 1).
Ultrasound examination
All eight patients underwent ultrasonography. Of these, two underwent transvaginal ultrasonography, one underwent transabdominal ultrasonography, and five underwent three-dimensional (3D) ultrasonography. The principal ultrasonographic finding was blood accumulation within the accessory cavity, which appeared predominantly hypoechoic or anechoic; fluid–fluid levels were occasionally visible. Coronal images obtained by 3D ultrasonography demonstrated an oval accessory cavity adjacent to the triangular uterine cavity, with no communication between the two structures (Figure 1).

Ultrasound image of all patients. (a) Patient 2, transvaginal ultrasound, arrow indicating hypoechoic nodule in the left uterine wall. (b) Patient 3, three-dimensional (3D) ultrasound, arrow indicating hypoechoic nodule in the right myometrial wall. (c) Patient 6, 3D ultrasound, arrow indicating hypoechoic nodule in the left myometrial wall.
MRI examination
Pelvic MRI was performed in all eight patients. The cystic lesions demonstrated high signal intensity on T1-weighted imaging (T1WI), suggestive of old hemorrhage. On T2-weighted imaging (T2WI), the cyst walls exhibited low signal intensity, consistent with smooth muscle tissue. A thin high-signal layer within the cavity was also observed, corresponding to endometrial tissue (Figure 2). Among the eight patients, the mean lesion diameter was 3.1 cm, and six lesions (75%) were located on the left side of the uterus (Table 1).

MRI image of the pelvis. (a) Patient 1, the arrow indicates a circular mass in the wall of the right uterine muscle layer; (A1) T1 weighted imaging; (A2) T2 weighted imaging. (b) Patient 5, the arrow represents a circular mass in the wall of the left anterior muscle layer; (B1) T1 weighted imaging; (B2) T2 weighted imaging. (c) Patient 6, the arrow indicates a circular mass in the left uterine muscle layer wall; (C1) T1 weighted imaging; (C2) T2 weighted imaging. MRI: magnetic resonance imaging.
Hysteroscopy
Hysteroscopy was performed in six patients and revealed a normal uterine cavity with clearly visible bilateral tubal ostia (Figure 3). The procedure was performed to confirm a normal uterine cavity and exclude communication between the lesion and the cavity, which is critical for differentiating ACUM from Robert's uterus or a noncommunicating functional uterine horn.
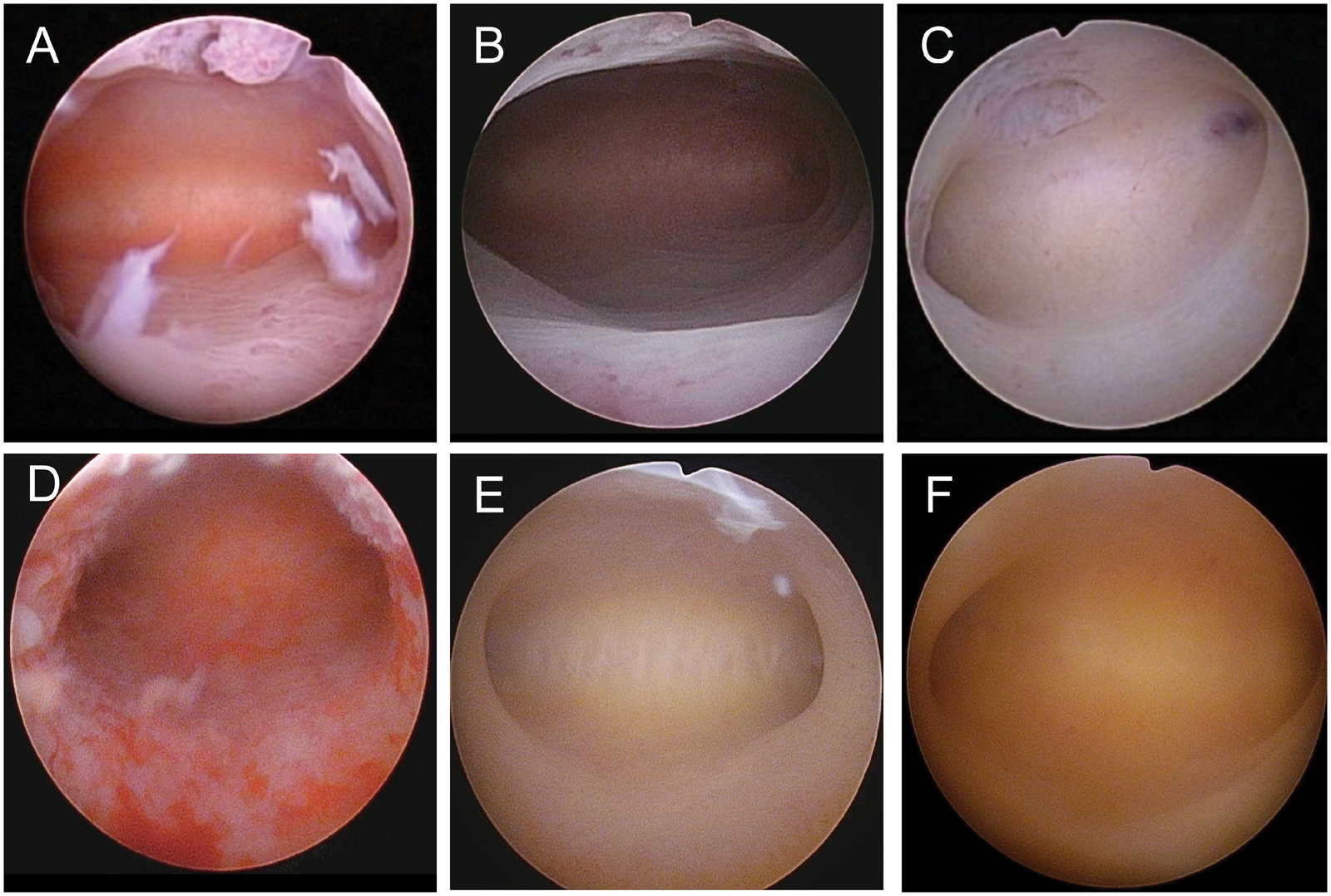
Hysteroscopic examination. Hysteroscopy of six patients showed a normal uterine cavity configuration with clearly visible bilateral tubal ostia. (a) Patient 1; (b) Patient 2; (c) Patient 3; (d) Patient 4; (e) Patient 6; and (f) Patient 7.
Surgery and pathology
Surgical method
All eight patients underwent laparoscopic excision of the lesion. The surgical procedure was as follows: 1.Using an electric hook, the surgical route was planned with the lesion as the center and the normal uterine muscle layer as the boundary. 2. A layered resection was then performed from shallow to deep tissue planes, ensuring that all steps were carried out under direct visualization to minimize damage to healthy myometrium. 3. During resection, spoon forceps were employed to provide serosal counter-traction, thereby avoiding the use of toothed graspers and minimizing the risk of lesion rupture. 4. The residual cavity was copiously irrigated with normal saline and subsequently closed in layers using a continuous 0-gauge absorbable suture to reconstruct the uterine wall. 5. The resected lesion was placed into a disposable sealed retrieval bag and removed through the puncture site (Figure 4).
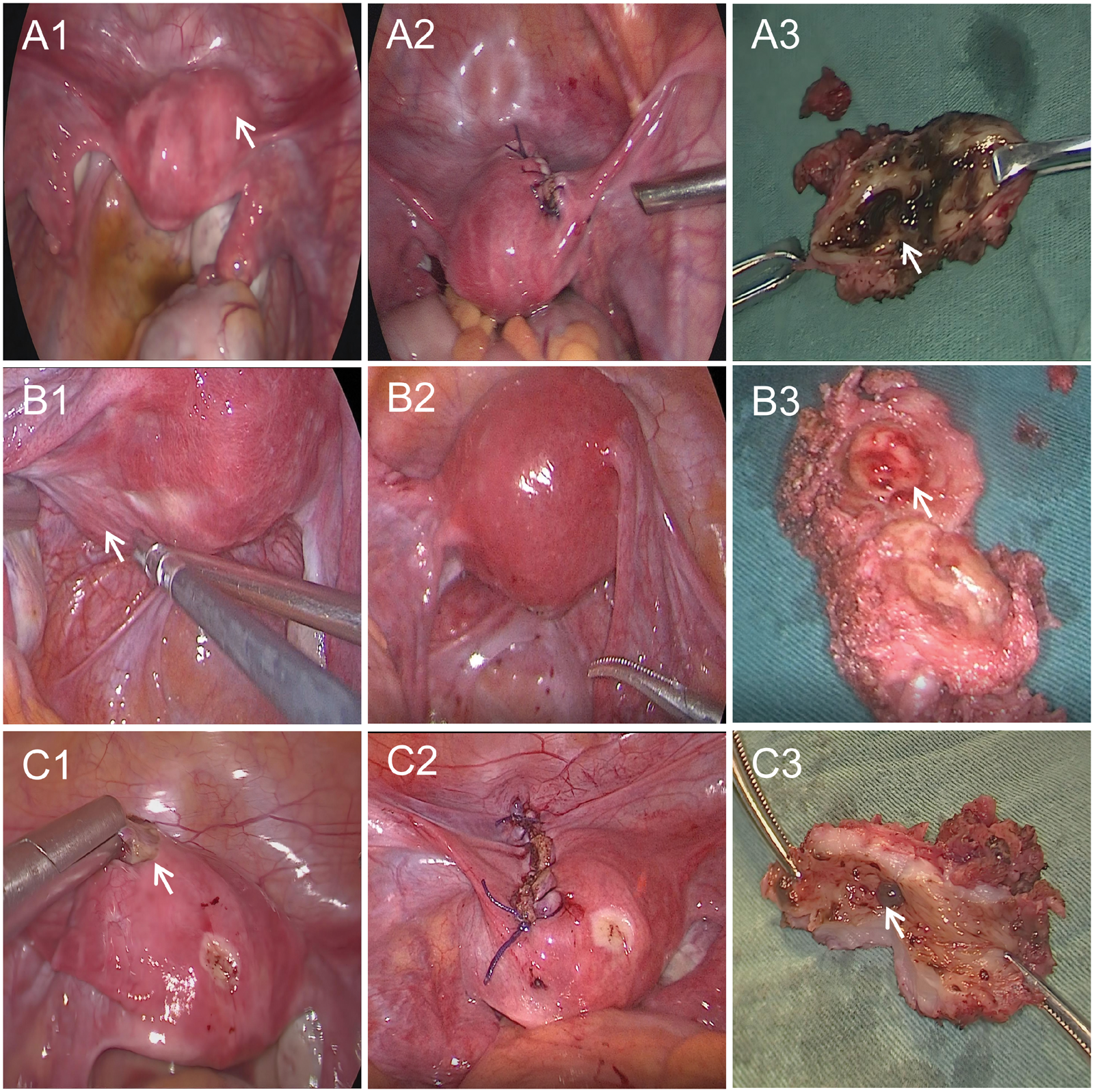
Laparoscopic resection. (a) Patient 1; (A1) A mass was seen below the round ligament of the right anterior uterine wall; (A2) Myometrial defect sutured; (A3) Sectioned specimen showed the lesion to be lined by endometrium and filled with chocolate-like fluid. (b) Patient 5; (B1) A mass was seen below the round ligament of the left posterior uterine wall; (B2) Myometrial defect sutured; (B3) Sectioned specimen showed the lesion to be lined by endometrium and filled with chocolate-like fluid. (c) Patient 6; (C1) A mass was seen below the round ligament of the left anterior uterine wall; (C2) Myometrial defect sutured; (C3) Sectioned specimen showed the lesion to be lined by endometrium and filled with chocolate-like fluid.
Pathological results
Pathological examination of all eight surgical specimens showed chocolate-like fluid within the accessory cavity on gross examination. Microscopically, the cavity was lined with functional endometrium and surrounded by regularly arranged smooth muscle tissue (Figure 5).
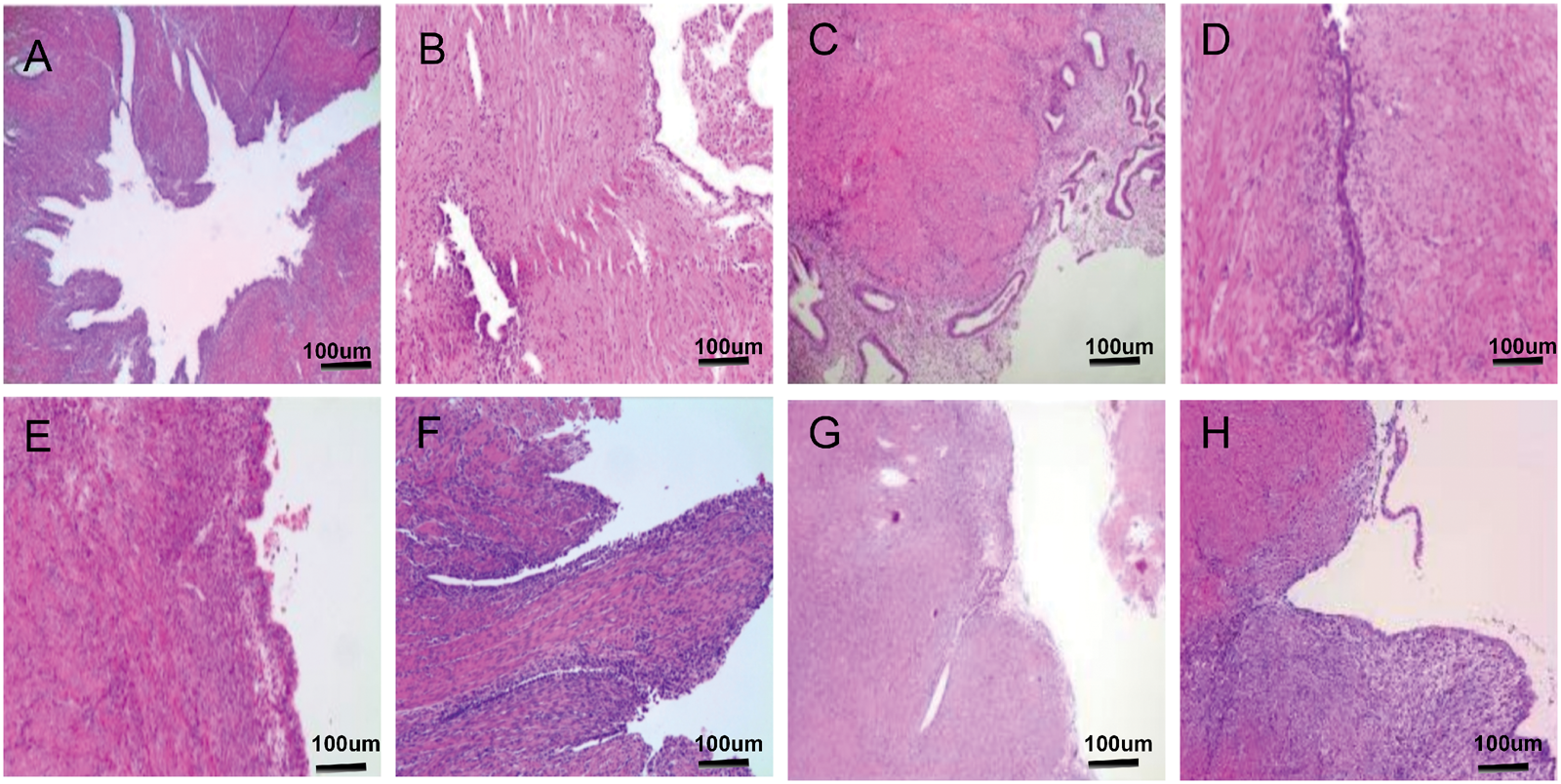
Pathological images of all patients. Histological examination with hematoxylin and eosin (HE) staining and immunohistochemistry demonstrated that the ACUM was histologically composed of endometrial epithelium surrounded by myometrial tissue. (a) Patient 1; (b) Patient 2; (c) Patient 3; (d) Patient 4; (e) Patient 5; (f) Patient 6; (g) Patient 7; (h) Patient 8. ACUM: accessory cavitated uterine mass.
Prognosis
During follow-up, no recurrences were observed. Complete resolution of dysmenorrhea was achieved in seven patients. One patient received a levonorgestrel-releasing intrauterine system postoperatively and subsequently developed drug-induced amenorrhea (Table 1). No pregnancies occurred during the follow-up period.
Discussion
Epidemiology and clinical characteristics
In the present case series, the median age of patients was 27 years, which is consistent with the median age of 29 years reported by Naftalin et al. 8 in their cohort of 20 patients. These findings further support that ACUM predominantly affects young women of reproductive age. The clinical presentation of ACUM is often nonspecific, which contributes substantially to delayed or incorrect diagnosis. Progressively worsening dysmenorrhea is the hallmark symptom of ACUM and is frequently accompanied by chronic pelvic pain. The underlying mechanism is cyclic bleeding of functional endometrial tissue within the accessory cavity, resulting in progressive intracystic pressure accumulation and stimulation of surrounding pain-sensitive structures. 4 According to previous research, 9 dysmenorrhea and chronic pelvic pain often exhibit primary or secondary resistance to common pharmacotherapies—including nonsteroidal anti-inflammatory drugs, combined oral contraceptives, and gonadotropin-releasing hormone agonists—resulting in poor analgesic efficacy. In our cohort, all eight patients presented with dysmenorrhea, including one patient who primarily experienced intermittent unilateral lower abdominal pain. Five patients (62.5%) reported progressively worsening symptoms, and five patients (62.5%) experienced severe pain (VAS ≥ 7) with limited response to nonsteroidal anti-inflammatory drugs. These results are consistent with the literature reported above. The fundamental cause of pain is the periodic shedding of functional endometrium within the lesion, which prevents menstrual blood from being discharged and increases intracavitary pressure, thereby stimulating surrounding pain-sensitive nerves. 10 Notably, no apparent correlation was observed between lesion size and pain severity in this series. However, this observation should be interpreted cautiously given the limited sample size and warrants further investigation in larger cohorts. In this series, 75% of ACUM lesions were located on the left side. The mechanism underlying this asymmetry is not fully understood but may be related to embryological differences in the development of the bilateral gubernaculum or degeneration of the mesonephric duct. Further research is needed to clarify the developmental basis of this lateralization. Although ACUM was initially thought to occur only in nulliparous women, our series confirms its presence in women with multiple pregnancies. Importantly, half of the patients had a history of at least one successful delivery, indicating that ACUM does not necessarily impair fertility prior to surgical intervention. This observation expands the clinical spectrum of ACUM and highlights that this diagnosis should also be considered in patients with progressive dysmenorrhea who are multiparous.
Diagnosis
The diagnosis of ACUM relies on an integrated assessment of clinical presentation, imaging findings, and pathological confirmation, with imaging playing a pivotal role in preoperative evaluation. Transvaginal ultrasonography serves as the preferred initial diagnostic modality because of its accessibility, noninvasiveness, and ability to accurately localize the lesion beneath the round ligament. Typical findings include an isolated cystic mass with hemorrhagic content and no communication with the uterine cavity. 8 MRI serves as a crucial supplementary technique for definitive diagnosis, particularly in differentiating ACUM from cystic adenomyosis or cystic degeneration of myoma. Owing to its high soft-tissue resolution and multisequence capabilities, MRI accurately characterizes lesion composition: high T1WI signal indicates hemorrhagic content, a low-T2WI-signal cyst wall suggests smooth muscle, and an internal thin layer of high T2 signal corresponds to the endometrial lining. These features are central to distinguishing ACUM from cystic adenomyosis. 10
In the present study, six patients underwent hysteroscopic examination, which demonstrated normal uterine cavity morphology with clearly identifiable bilateral tubal ostia. Hysteroscopy can assess the configuration of the uterine cavity and exclude abnormalities that communicate with the uterine cavity, thereby helping distinguish ACUM from other obstructive uterine malformations such as Robert's uterus and a type II rudimentary horn uterus.
Serum CA125 levels were measured in most patients as part of routine preoperative screening for gynecologic tumor markers. As a common nonspecific biomarker elevated in epithelial ovarian cancer, endometriosis, pelvic inflammatory disease, and other benign gynecologic conditions, CA125 may assist in differentiating abdominal pain caused by endometriosis or degenerating uterine fibroids. Consistent with previous reports, serum CA125 levels were normal or only mildly elevated, confirming its limited diagnostic value in ACUM. 4 This finding further underscores the limited utility of CA125 in diagnosing the condition.
The differential diagnosis of a cavitated uterine mass is broad and includes several entities. Cystic adenomyosis is usually characterized by indistinct borders, multiple small cysts, and diffuse involvement of the myometrium without specific anatomical features and may occur in any part of the uterus. Robert’s uterus is a rare asymmetric septate uterus with a septum extending from the fundus to above the internal os and deviating to one side to form a blind noncommunicating hemicavity. The obstructed cavity communicates with the ipsilateral fallopian tube, the external uterine contour remains normal, and hysteroscopy typically demonstrates only one visible tubal ostium. A type II rudimentary horn uterus may also contain chocolate-like fluid; however, the key distinction from ACUM is that the rudimentary horn communicates with one fallopian tube, whereas the contralateral side exhibits a unicornuate uterine configuration, and only one tubal ostium is visualized on hysteroscopy. Cystic degeneration of uterine fibroids usually does not cause cyclic pelvic pain. MRI may demonstrate a central cystic cavity, although hemorrhagic content is uncommon, the cyst wall lacks an endometrial lining, fibroids may be multiple, and lesions can occur anywhere in the uterus. These differential diagnoses can often be distinguished through a combination of clinical history, imaging findings, and, when necessary, hysteroscopy.
Treatment options and prognosis
The treatment of ACUM aims to alleviate symptoms and preserve fertility. Current evidence supports surgical excision of the lesion as the preferred treatment option.5,9
Pharmacological therapy
Pharmacological treatment should be considered only as a temporary measure for preoperative symptom control. The literature indicates that although oral contraceptives and gonadotropin-releasing hormone agonists (GnRH-a) can transiently suppress endometrial shedding and provide temporary pain relief, symptoms rapidly recur after treatment discontinuation.9,11 Nonsteroidal anti-inflammatory drugs (NSAIDs) act by inhibiting cyclooxygenase and reducing prostaglandin-mediated pain and inflammation. In this study, five patients with severe pain experienced poor symptom relief with ibuprofen before surgery. Therefore, long-term pharmacological therapy is not recommended.
Surgical treatment
Laparoscopic excision is currently regarded as the first-line treatment for ACUM, offering definitive symptom relief while preserving uterine anatomy and reproductive potential. 5 This approach offers the advantages of minimal invasiveness, rapid recovery, and excellent visualization, allowing complete excision of the lesion while preserving the surrounding myometrium. 12 It is particularly suitable for patients with fertility requirements. Three key surgical principles should be emphasized: (a) complete excision of the lesion while preserving as much normal myometrium as possible; (b) meticulous handling to avoid intraoperative rupture and spillage of cystic contents; and (c) careful multilayer reconstruction of the uterine wall to ensure structural integrity for future pregnancy. In this study, all eight patients successfully underwent laparoscopic resection. Postoperatively, complete relief of dysmenorrhea was achieved in seven patients. The remaining patient, who had no fertility desire, developed drug-induced amenorrhea following placement of a levonorgestrel-releasing intrauterine system, making further evaluation of dysmenorrhea impossible. In the present series, all patients underwent laparoscopic resection without complications. During follow-up, no recurrences were observed, and complete resolution of dysmenorrhea was achieved in most patients, confirming the effectiveness of surgical management.
Although not used in our cases, robotic-assisted laparoscopy offers potential advantages for ACUM excision, including enhanced 3D visualization (10–15× magnification), wristed instruments with seven degrees of freedom, tremor filtration, and improved ergonomics. These features facilitate precise dissection, reduce the risk of cyst rupture, and enable superior myometrial reconstruction, which may be particularly beneficial for fertility preservation. However, higher costs and longer operative times limit its widespread use, and conventional laparoscopy remains the first-line treatment in most cases.
Sclerotherapy
Ultrasound-guided sclerotherapy has been proposed as a minimally invasive alternative for ACUM management. 13 One study reported that among seven patients with ACUM, six experienced significant symptom relief after treatment, with gradual shrinkage of the mass and no recurrence. Only one patient experienced initial symptom improvement and lesion shrinkage after 1 month, but recurrence occurred 3 months later. Under local anesthesia, sclerosing agents such as 95% ethanol or polidocanol can be injected directly into the cystic cavity. This technique induces chemical inflammation, epithelial destruction, and subsequent fibrosis of the cyst wall, potentially leading to permanent obliteration of the cavity. A key advantage of this method is its minimal invasiveness—it preserves myometrial integrity, causes no muscular injury, and can be performed under local anesthesia. Although preliminary reports suggest symptom improvement and lesion regression in selected cases, recurrence has also been documented. At present, evidence remains limited, and standardized protocols regarding sclerosant type, dosage, and long-term safety—particularly with respect to fertility—are lacking. 8
Direct comparisons between surgical excision and sclerotherapy are currently unavailable, highlighting the need for future multicenter studies to clarify optimal treatment strategies, particularly in women desiring fertility preservation.
Fertility management and prognosis
Following laparoscopic excision, individualized contraceptive counseling is recommended for 6–12 months, depending on the extent of myometrial reconstruction, with close obstetric surveillance advised in subsequent pregnancies. In this study, four patients expressed future reproductive desires. To date, none have attempted conception. Notably, postoperative live births without uterine rupture were reported in 8 of the 95 patients by Timmerman et al., 6 demonstrating the feasibility of fertility following surgical intervention. Future multicenter prospective studies are essential to validate the long-term reproductive prognosis and clarify the impact of ACUM on fertility.
Study contributions and limitations
Our findings confirm that the age at onset, clinical presentation, and surgical outcomes of ACUM are consistent with previous reports.5,8,9 Importantly, we demonstrate that ACUM also occurs in multiparous women (50% of our cohort), challenging the early assumption that the condition is confined to nulliparous patients. Furthermore, we provide a detailed, standardized laparoscopic resection procedure with direct comparison of surgical techniques, offering practical guidance for gynecologists. This study adds valuable evidence to the limited global literature on ACUM and raises awareness of this underdiagnosed entity. Several limitations should be acknowledged. This was a retrospective, single-center case series with a small sample size (n = 8), which may limit generalizability. The follow-up period was relatively short (median 9.5 months), and no pregnancies occurred during this time. Therefore, the direct impact of surgery on fertility could not be evaluated. Robotic surgery was not performed in our cohort, precluding direct comparison with conventional laparoscopy. Finally, the embryological mechanism underlying the left-sided predominance remains theoretical and requires further basic research.
In summary, ACUM is a rare obstructive malformation affecting young women and is characterized by progressive dysmenorrhea, often involving left-sided lesions. Transvaginal ultrasonography combined with MRI is key to diagnosis. Laparoscopic resection effectively relieves symptoms and preserves fertility, yielding excellent outcomes. Improved clinical recognition is essential to avoid misdiagnosis and facilitate individualized treatment.
Footnotes
Acknowledgments
The successful completion of this study would not have been possible without the support and assistance of multiple parties. We sincerely thank the Natural Science Foundation of Gansu Province (Project No. 23JRRA1379) for its financial support, which was essential for clinical data collection, imaging analysis, and follow-up. We also thank the Ethics Committee of Gansu Maternal and Child Health Hospital (Gansu Provincial Central Hospital) for its review and guidance (Approval No. 2020-SL-68), which ensured that this study was conducted in accordance with ethical standards and protected the rights and interests of the participants.
Author contributions
Fang Wang and Qing Liu conceived and designed the study. Fang Wang drafted the manuscript. Jing Zheng subsequently revised the manuscript. Qing Liu and Huiling Wang performed the surgical procedures and recruited patients. Yaqin Zhao, Futang Ma, Zhenqiang Gong, and Jing Zheng collected and organized the clinical data. All authors reviewed and approved the final manuscript.
Availability of data and materials
All data supporting the findings of this study are available within the paper and its supplementary information.
Consent for participation
Written informed consent for participation was obtained from all patients or their parents/legal guardians, as appropriate.
Declaration of conflicting interests
The authors declare no conflicts of interest.
Ethics approval
This study was conducted in accordance with the Declaration of Helsinki. All procedures involving human participants were approved by the Human Investigation Committees of Gansu Provincial Maternity and Child Care Hospital (Approval No. 2020-SL-68).
Funding
This study was supported by the Natural Science Foundation of Gansu Province (23JRRA1379).