
Abstract
Chronic obstructive pulmonary disease is a prevalent chronic respiratory disorder that often coexists with multidrug-resistant bacterial infections in the lungs, significantly increasing treatment complexity and patient mortality. Consequently, research on the prevention and management of chronic obstructive pulmonary disease complicated by pulmonary multidrug-resistant bacterial infections has attracted increasing attention. Establishing predictive models for chronic obstructive pulmonary disease complicated by multidrug-resistant bacterial infections based on clinical risk factors has become a crucial direction in current clinical research. This narrative review summarizes the limitations of currently available predictive models, particularly in the selection of major risk factors and model construction. It aims to provide guidance for the selection and optimization of future predictive model development methods. The goal is to enhance the predictive performance and clinical applicability of these models while laying a theoretical foundation for the transformation of diagnostic and therapeutic paradigms.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic heterogeneous disease characterized by persistent airflow limitation, mainly caused by airway remodeling and alveolar structural abnormalities, and manifested as chronic cough, sputum production, and progressive dyspnea. 1 The pathogenesis of COPD primarily involves several core mechanisms, including chronic inflammation and immune dysregulation, which interact and promote each other, ultimately leading to lung tissue destruction and airflow limitation.2–4 Due to population aging, the global prevalence of COPD has reached 10.3%. 1 Patients with COPD have reduced physical activity and limited social functioning, often accompanied by severe complications and comorbidities, leading to significantly impaired health-related quality of life.1,5,6 It is estimated that more than 3 million people die from COPD each year, 7 and by 2050, COPD is predicted to become one of the top four causes of disability-adjusted life years (DALYs), 8 posing a serious threat to human health.
Due to irrational antibiotic use, bacterial resistance has become a global crisis,9,10 and according to the University of Washington in the United States, approximately 4.95 million people died from bacterial resistance in 2019 alone. 11 With declining lung function, the incidence of multidrug-resistant (MDR) bacterial pulmonary infections gradually increases,12–14 resulting in an elevated risk of death. 11 Therefore, early identification of high-risk patients and prevention of MDR bacterial infections are critical to improving patient outcomes.15–17
Given the adverse impact of MDR bacterial infections in patients with COPD, an increasing number of prediction models have been applied in clinical research.17,18 Existing prediction models are mainly built by analyzing patient demographic characteristics and clinical data using statistical methods, aiming to accurately identify high-risk patients and enable early intervention, thereby reducing the emergence and spread of MDR bacteria.19–21 However, the performance of current models varies, and their generalizability needs improvement. Future research should focus on integrating multidimensional data from clinical, microbiological, and molecular fields, combined with artificial intelligence and large-scale data analytics, to establish more accurate and effective prediction models.22–24
This review is a narrative review. Through a comprehensive analysis of the risk factors and predictive models for MDR bacterial infection in patients with COPD, especially by comparing the advantages and limitations of machine learning models with those of traditional models, it aims to provide theoretical guidance for the selection of predictive factors and modeling methods in future predictive model development.
Methods
Search scope
A comprehensive search of the PubMed and Web of Science databases was conducted. The search period spanned from the establishment of the databases to 1 October 2025.
Search terms used
A strategy combining subject headings and free-text terms was adopted. The English search terms included the following: “Chronic Obstructive Pulmonary Disease,” “COPD,” “Acute Exacerbation of Chronic Obstructive Pulmonary Disease,” “Multiple Resistant Bacteria,” “Infection by Multi-drug Resistant Bacteria,” “Multi-drug Resistant,” “Pulmonary Infection,” “Resistance Mechanism,” “Pathomechanism,” “Hazard,” “Prediction Model,” “Machine Learning,” “Regression Model,” and “Model Limitations.”
Inclusion and exclusion criteria
The inclusion criteria were as follows:
Study types include cohort studies, case-control studies, cross-sectional studies, randomized controlled trials, meta-analyses, and systematic reviews. The focus of the studies is the construction and validation of prediction models for MDR bacterial infections in patients with COPD. The study subjects are patients aged 18 years or older with COPD or pulmonary infection. The predicted outcome is MDR bacterial infection in the lungs.
The exclusion criterion was studies for which full text cannot be obtained or from which relevant data cannot be extracted.
This review is guided by the Scale for the Assessment of Narrative Review Articles (SANRA). 25
Mechanisms and classification of antimicrobial resistance
Mechanisms and characteristics of MDR bacteria
MDR bacteria refer to bacterial strains resistant to three or more classes of antibiotics. 26 The emergence of MDR bacteria substantially increased treatment difficulty and posed serious challenges to clinical practice,11,27 especially in intensive care units (ICUs) and among immunosuppressed patients, where infection rates have risen significantly and markedly increased the healthcare burden and mortality.28–31
Bacteria develop resistance through multiple mechanisms, disseminating resistance genes among strains via horizontal gene transfer mediated by plasmids, transposons, and integrons,32–39 and their resistance mechanisms are complex (Table 1), especially in chronic respiratory diseases such as COPD, where they often lead to lower respiratory tract colonization and recurrent infections, severely affecting patient outcomes. 13
Mechanisms of antimicrobial resistance in MDR bacteria.
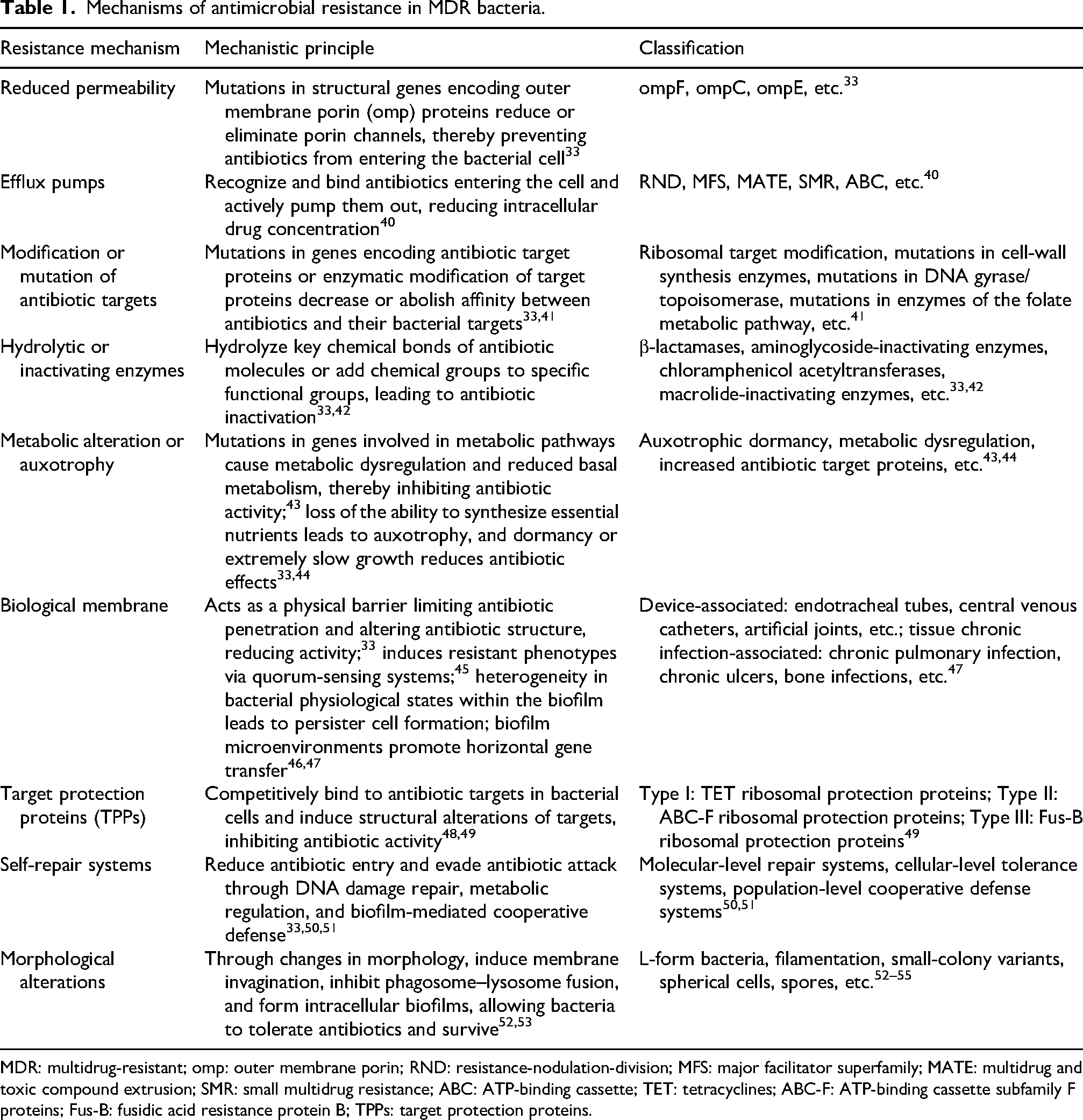
MDR: multidrug-resistant; omp: outer membrane porin; RND: resistance-nodulation-division; MFS: major facilitator superfamily; MATE: multidrug and toxic compound extrusion; SMR: small multidrug resistance; ABC: ATP-binding cassette; TET: tetracyclines; ABC-F: ATP-binding cassette subfamily F proteins; Fus-B: fusidic acid resistance protein B; TPPs: target protection proteins.
MDR bacteria, with their complex mechanisms and broad resistance spectrum, pose significant challenges to clinical diagnosis and treatment and have become a serious public health threat, 56 making in-depth investigation of resistance mechanisms essential for developing early prevention strategies and improving outcomes.
Common types of MDR bacteria
Common MDR bacteria in COPD included Pseudomonas aeruginosa (PA), Escherichia coli, Klebsiella pneumoniae, Acinetobacter baumannii, and methicillin-resistant Staphylococcus aureus (MRSA).4,57 Among these, PA was the most common and was closely associated with frequent acute exacerbations and mortality58–61 Due to its genetic characteristics, PA tended to persist within the same clonal lineage during repeated infections, promoting the development of resistance genes. 62 MDR A. baumannii was commonly found in patients with prior endotracheal intubation.63,64 Resistant E. coli and K. pneumoniae often displayed resistance to various β-lactams and quinolones, and their production of β-lactamases and carbapenemases further complicated treatment.59,65 MRSA was resistant to methicillin and several other antibiotics, greatly increasing treatment difficulty and mortality. 66
Studies have shown that MDR bacterial infections are independent risk factors for COPD progression and poor prognosis 15 ; therefore, early identification and targeted antimicrobial strategies are important for improving patient outcomes.15,67
Relationship between COPD and MDR bacterial infections
Pathophysiological mechanisms of COPD
The central mechanism of COPD is chronic inflammation, triggered mainly by smoking and environmental pollution, leading to epithelial hyperplasia, basement membrane thickening, and smooth muscle proliferation, which cause small airway remodeling and progressive decline in lung function.68–70 Chronic inflammation also results in lung tissue destruction and loss of elastic recoil, leading to emphysema and further aggravating airflow limitation.68,69
Another mechanism is immune dysregulation, as chronic inflammation activates immune cells such as neutrophils, lymphocytes, and macrophages, causing them to release large amounts of inflammatory mediators, triggering oxidative stress and lung tissue injury.71,72 Chronic inflammation and oxidative stress accelerate lung aging and disease progression. 69 Immune dysregulation also induces systemic inflammation, contributing to cardiovascular disease, osteoporosis, and metabolic syndrome.73,74 Additionally, COPD is often accompanied by lower airway microbiome alterations and chronic infections, which exacerbate airway inflammation and impair barrier defense, making patients more vulnerable to pathogen invasion.75,76 Inflammation and infection also cause mucus hypersecretion, worsening airway obstruction and ventilatory dysfunction.77,78
Thus, the pathophysiological mechanisms of COPD involved multiple interacting processes that not only lead to airway narrowing and tissue destruction but also weaken immunity, providing favorable conditions for MDR colonization and infection.
Epidemiological characteristics
Epidemiological data showed that patients with COPD have significantly higher MDR infection rates than individuals without COPD, which are associated with frequent hospitalizations, antibiotic exposure, and invasive procedures.79–81 A case-control study reported that severe COPD was an independent risk factor for MDR infections, and that patients infected with carbapenem-resistant bacteria had a 30-day mortality rate as high as 37.6%. 82 Therefore, the epidemiological characteristics of COPD with MDR infections include a high incidence and high mortality, which are closely related to disease severity and clinical management.
Risk factors for MDR bacterial infections in COPD
Patient-related factors
Age and sex
Studies indicate that older patients are more susceptible to MDR bacteria because of immune senescence, reduced physiological barrier function, and a higher prevalence of comorbidities.38,83 Men have a higher risk of MDR colonization and infection than women, mainly because of androgen-related immunosuppression and higher rates of smoking, alcohol use, and occupational exposure.83,84
COPD classification and disease duration
Alexopoulos Evangelos et al. found that, compared with patients with GOLD stage I, the frequency of acute exacerbations increased by 40% and 74.5% in patients with GOLD stage III and IV disease, respectively, and that patients with a disease duration of >10 years had 54.3% higher hospitalization rates and 75.5% higher ICU admission rates than those with a disease duration of <5 years. 85 Therefore, due to frequent antibiotic and glucocorticoid exposure, patients with GOLD stage III or higher disease or a disease duration of >10 years had an increased risk of MDR infection.78,86
Comorbidities
Diabetes
Hyperglycemia in diabetes causes vascular changes, tissue ischemia, and impaired defense function while simultaneously providing nutrients for bacterial growth and impairing immune responses. Therefore, recurrent infections may facilitate MDR development and progression.87,88
Malignancy
Malignancy is often associated with malnutrition and immune impairment, and antitumor therapies cause bone marrow suppression and damage to local defense barriers, increasing the risk of MDR infection. 89
Immunodeficiency
Patients with human immunodeficiency virus (HIV) or organ transplantation often exhibit immune deficiency, making them prone to frequent infections and MDR development.90–92 A meta-analysis of patients with HIV and bacterial infections reported an MDR detection rate of up to 58.02%, 90 and immunodeficient patients with MDR infections had a significantly higher mortality risk. 93
Others
Studies have also found that patients with congestive heart failure, chronic renal failure, or cerebrovascular accidents have significantly higher risks of MDR pulmonary infections. 94
Malnutrition
Studies show that 30% of patients with COPD have malnutrition, especially those aged >60 years and those with severe lung impairment. 95 Malnutrition leads to protein deficiency and impaired immunity, increasing the risk of infection. Due to micronutrient deficiency and reduced nutrient intake, intestinal microbiota imbalance occurs, increasing the prevalence of intestinal MDR bacteria. Based on the gut–lung axis and the vicious cycle between malnutrition and infection, the risk of MDR pulmonary infections increases. 96
Clinical factors
Hospitalization frequency
MDR bacteria are widely present in hospitals, especially ICUs. Studies show that patients with COPD hospitalized ≥2 times because of acute exacerbations within 1 year have an increased risk of MDR infection.18,97
Antibiotics
A retrospective study by Fang Ding et al. reported that frequent antibiotic use was an independent risk factor for MDR infections in patients with COPD. 15 Frequent antibiotic use induces gene mutation and expression, promotes biofilm formation, 35 and facilitates the horizontal transfer of resistance genes, exacerbating the spread of MDR bacteria.81,98
Glucocorticoids
Glucocorticoids have anti-inflammatory and immunosuppressive effects; long-term use suppresses innate and adaptive immunity, increasing infection risk. They also promote biofilm formation and horizontal gene transfer, inducing the emergence of MDR bacteria. 99
Invasive procedures
Invasive mechanical ventilation
Invasive mechanical ventilation is the main cause of ventilator-associated pneumonia (VAP). Studies show that when ventilation exceeds 48 h, the incidence of VAP reaches 27.7%, with MDR bacteria accounting for 43.65%. 100 Multiple studies have identified invasive mechanical ventilation as an independent risk factor for MDR infection.101–103 Endotracheal intubation causes mucosal injury and impairs ciliary clearance, disrupting defense barriers; the tube serves as a site for colonization and biofilm formation, while the open airway increases the risks of aspiration, bacterial translocation, and cross-infection, leading to MDR development.104,105
Other invasive procedures
Urinary catheterization was an independent risk factor for MDR infections, especially MRSA infection. 94 Destruction of urinary tract defenses and biofilm formation promote MDR bacterial growth, which may lead to bacteremia and pulmonary infection. 106 Nasogastric tube placement causes aspiration, intestinal dysbiosis, and bacterial translocation, significantly increasing the risk of pulmonary E. coli infection. 107 Continuous renal replacement therapy and central venous or arterial catheterization increase the risk of MDR bacteremia and secondary pulmonary infections.97,108
Biomarkers
In recent years, multiple biomarkers have been identified as predictive factors for MDR infections and have been used in the construction of clinical prediction models. These biomarkers mainly include peripheral blood neutrophils, lymphocytes, the platelet-to-lymphocyte ratio (PLR), the neutrophil-to-lymphocyte ratio (NLR), eosinophils, C-reactive protein (CRP), procalcitonin (PCT), interleukin-6 (IL-6), and albumin.97,109–113 The detection results of these biomarkers are more objective, and prediction models developed by integrating them with machine learning techniques often show better predictive performance. 113
Lifestyle and environmental factors
Smoking
Smoking is closely associated with lung function decline, COPD exacerbations, and infections. 15 Smoking damages the airway mucosa and lowers local defense function, promotes chronic airway and systemic inflammation, and increases the risk of lower airway MDR colonization and infection, especially in adolescents.114,115
Air pollution
Inhalation of particulate matter and harmful gases aggravates inflammation and oxidative stress, damaging lung barrier function and immunity and creating favorable conditions for MDR invasion and colonization. 116 Hospitals and waste treatment facilities provide environmental reservoirs for MDR bacteria, which spread through aerosols.116,117
In summary, the co-occurrence of COPD and MDR bacterial infections results from the interplay of multiple risk factors, including host-related factors, clinical diagnosis and treatment, and environmental influences. The precise identification of high-risk patients and the early formulation of prevention and intervention strategies are pivotal to reducing the emergence of MDR bacteria and improving patient outcomes.
Socioeconomic factors
Studies indicate that the risk of MDR bacterial infections in patients with COPD is closely associated with socioeconomic factors. 118 Populations with low socioeconomic status often live in substandard conditions with inadequate sanitation, which increases exposure to and the transmission of pathogens. Meanwhile, financial constraints may prevent patients from completing a full course of treatment. Low educational attainment leads to insufficient awareness of the disease and antimicrobial agents, predisposing patients to antibiotic misuse or premature treatment discontinuation and thereby facilitating the emergence of drug-resistant bacteria. Furthermore, economically underdeveloped regions typically face resource scarcity and inconsistent clinical diagnostic and therapeutic standards. This may result in delayed or nonstandardized care, which elevates the risk of infection and antibiotic exposure. These factors often act synergistically to further increase patients’ susceptibility to infections.118,119
Current status of prediction model development
Common types of prediction models
Logistic regression models
Logistic regression is a classification model used to estimate event probability based on multiple independent variables. Model discrimination is typically evaluated using the area under the receiver operating characteristic curve, calibration using the Hosmer–Lemeshow test or calibration curves, internal validation using bootstrap or cross-validation, and external validation using datasets from other institutions or time periods; results are interpreted using odds ratios (ORs). A systematic review on acute exacerbation of COPD (AECOPD) prognosis prediction reported that 41 of 53 models used logistic regression, making it one of the most traditional and commonly used clinical modeling methods. 21 It is widely applied to construct nomograms, model equations, and scoring systems.115–117
Cox proportional hazards models
The Cox model identifies relationships between variables and time-to-event outcomes. Discrimination is evaluated using the concordance index, and calibration using calibration curves; results are interpreted using hazard ratios and 95% confidence intervals, and nomograms or survival curves are used to build prediction tools. A multicenter retrospective study used a Cox model and nomogram to predict the prognosis of elderly patients with pulmonary MDR infections, 118 and Graul EL et al. used a Cox model and forest plot to assess the risk of nonfatal cardiovascular events after COPD exacerbation, 119 with both studies showing satisfactory prediction performance.
Machine learning models
Machine learning, a subset of artificial intelligence, uses computer algorithms to analyze data, learn patterns, and make predictions or decisions. Common clinical machine learning models include random forests, support vector machines (SVMs), deep learning, and extreme gradient boosting (XGBoost). In elderly patients with COPD, SVMs achieved training and testing accuracies of 93.82% and 90.07%, respectively, effectively capturing nonlinear relationships. 120 Deep learning, based on multilayer neural networks, has shown strong predictive performance in studies using chest X-rays and pulmonary function data to predict COPD. 121 Random forests outperformed traditional models in predicting in-hospital mortality among patients with AECOPD. 122 In multiple studies predicting bacterial resistance, XGBoost demonstrated higher accuracy and predictive performance in both the training and validation sets.123–125 These studies collectively demonstrated the superiority and potential of machine learning models in clinical practice.
Comparison of prediction models
Different prediction models exhibit significant differences in effectiveness and accuracy, especially between traditional statistical models and machine learning models, each with its own strengths and limitations (Table 2). Model selection and optimization should consider clinical requirements and data characteristics.
Comparison between traditional prediction models and machine learning models.
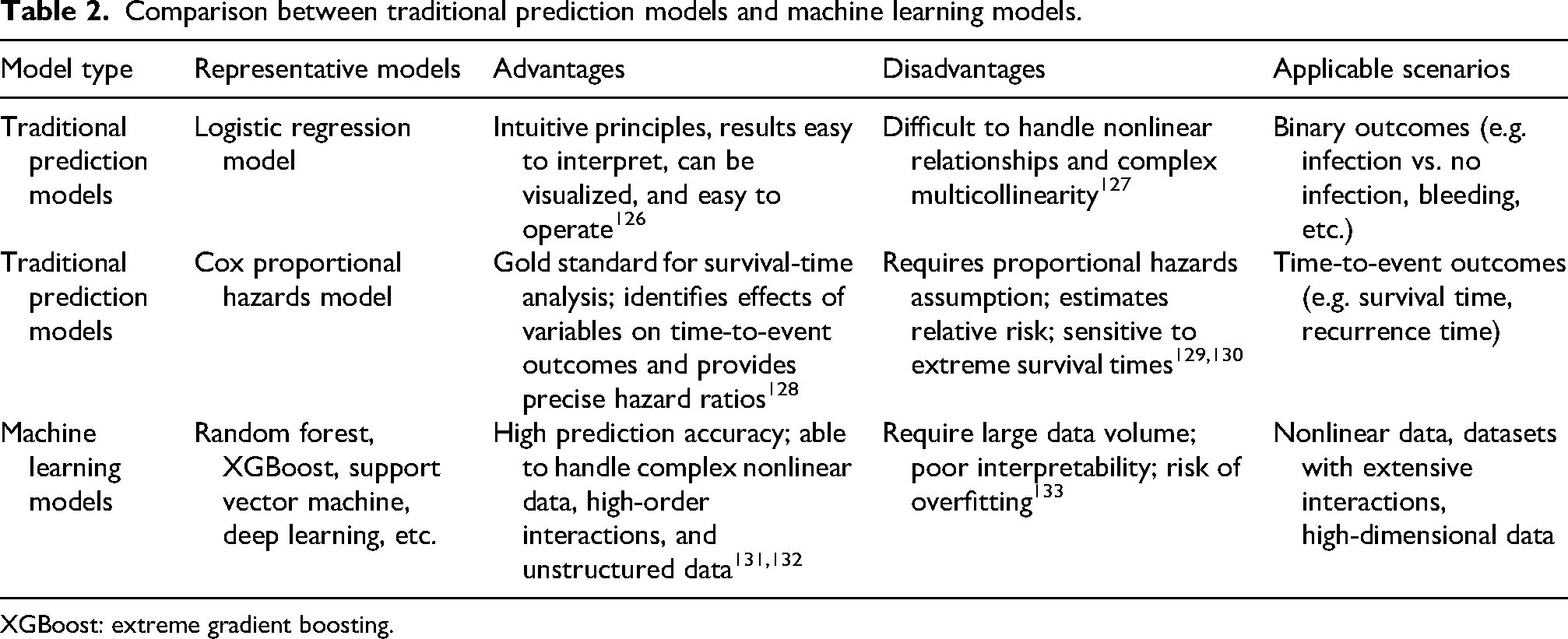
XGBoost: extreme gradient boosting.
Discussion
Current predictive models still have numerous shortcomings. For example, data from different hospitals display heterogeneity, which makes them difficult to merge and standardize. Specimens for microbiological tests, such as sputum cultures, vary in quality and are easily contaminated by respiratory colonizing bacteria, resulting in false-positive results. Predictive factors also have limitations; critical information, such as a history of antibiotic exposure and medical contact, may be incompletely or inaccurately recorded.
Moreover, patients’ clinical status and the risk of MDR infection change dynamically, and predictive models have difficulty capturing this dynamic process. The models are mainly constructed based on single-center retrospective studies, leading to a high risk of bias. Most models lack adequate external validation, resulting in poor clinical generalizability. 134
Additionally, some studies indicate that differences in socioeconomic and demographic characteristics may affect model fairness. This suggests that these factors should be considered during model construction and evaluation to avoid introducing racial or socioeconomic biases. 135
Since machine learning models have demonstrated better predictive performance than traditional prediction models in predicting the risk of MDR bacterial infections in patients with COPD, future research should focus on multicenter external validation of these models, the scientific rigor of variable selection, and the introduction of calibration methods. Leveraging the advantages of artificial intelligence and big data analysis to apply machine learning models to clinical diagnosis and treatment may become key to overcoming the bottleneck in the prevention and control of MDR bacterial infections.
In summary, this review comprehensively analyzes the risk factors of COPD complicated by MDR bacterial infections, specifically covering biomarkers and socioeconomic factors. Moreover, the review systematically examines predictive models, with an emphasis on machine learning models. It compares the advantages and limitations of traditional models with those of machine learning models and identifies current research gaps. This provides researchers with a reference for selecting appropriate modeling methods. However, as a narrative review, this study has potential risks of subjective bias. Moreover, because the primary source of the literature was the PubMed database, the conclusions may lack sufficient representativeness.
Conclusion
The risk factors for COPD complicated by MDR infections span multiple dimensions, including patient characteristics, clinical diagnosis and treatment, the living environment, and socioeconomic status. Establishing scientifically accurate and clinically applicable predictive models is essential for the targeted management of COPD patients and MDR infections. Future research should utilize multidimensional data and incorporate artificial intelligence technologies into model development to enhance model accuracy and generalizability, thereby facilitating early disease prevention and control and improving patient outcomes.
Footnotes
Acknowledgments
The authors extend their sincere gratitude to all participating patients, whose contributions have greatly advanced the field of COPD and MDR research.
The authors used ChatGPT (OpenAI; GPT-4o, accessed September 2025) solely for language polishing. All content was verified and edited by the authors, who bear full responsibility for the final manuscript.
Ethical considerations
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Contributions
(I) Conception and design: Deng Haibo, Luo Wei;
(II) Literature screening: Deng Haibo, Wu Yonghong;
(III) Data analysis and interpretation: Deng Haibo, Wu Yonghong, Yan Min, Luo Wei;
(IV) Writing – original draft: Deng Haibo;
(V) Final approval of manuscript: All authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data sharing statement
This article does not contain any unpublished data.