
Abstract
Objective
To evaluate the efficacy and safety of novel targeted drugs in patients with human epidermal growth factor receptor 2-positive breast cancer and their impact on clinical outcomes, including overall survival and progression-free survival.
Methods
This systematic review was registered with PROSPERO (CRD420261383276). A systematic search of PubMed, Embase, Cochrane Library, Web of Science, and ClinicalTrials.gov was conducted for randomized controlled trials and prospective cohort studies published between January 2000 and March 2024. Participants were adult females diagnosed with human epidermal growth factor receptor 2-positive breast cancer who were treated with novel agents (e.g. T-DXd, margetuximab, and tucatinib). Primary outcomes included overall survival, progression-free survival, objective response rate, and disease control rate. Statistical analyses were performed using RevMan 5.4 and Stata 16.0 with random-effects models.
Results
Eight studies were included from 2567 identified records. Novel human epidermal growth factor receptor 2-targeted drugs significantly improved overall survival (hazard ratio = 0.73, 95% confidence interval: 0.68–0.79) and progression-free survival (hazard ratio = 0.65, 95% confidence interval: 0.60–0.71) compared with standard treatments. The objective response rate (50% vs. 35%) and disease control rate (80% vs. 60%) were also significantly higher in the novel drug group. Subgroup analyses revealed greater benefits among patients with hormone receptor-negative disease (progression-free survival, hazard ratio = 0.58, 95% confidence interval: 0.50–0.67) and those with brain metastases (progression-free survival, hazard ratio = 0.52, 95% confidence interval: 0.45–0.60). Furthermore, novel drugs were associated with lower incidences of cardiotoxicity (5% vs. 15%) and gastrointestinal reactions (10% vs. 25%).
Conclusions
Novel targeted drugs demonstrate superior efficacy and a more favorable safety profile than traditional therapies in patients with human epidermal growth factor receptor 2-positive breast cancer. These findings provide a clinical basis for optimizing individualized treatment, particularly for high-risk subgroups.
Keywords
Introduction
Significant advances have been made in the treatment of breast cancer in recent decades, particularly in the field of human epidermal growth factor receptor 2 (HER2)-positive breast cancer. HER2-positive breast cancer is a distinct subtype of breast cancer caused by amplification or overexpression of the HER2 gene and accounts for approximately 15%–20% of all breast cancer cases. 1 This type of breast cancer is characterized by an abnormally increased number of HER2 receptors on the cell surface, leading to accelerated proliferation and dissemination of tumor cells. 2 Traditional chemotherapy has limited efficacy for this type of tumor; therefore, HER2-targeted therapy has become an important breakthrough in this field. Since 2000, the clinical application of HER2-targeted therapies, such as Herceptin and Perjeta, has achieved significant success and greatly improved the prognosis of patients with HER2-positive breast cancer. 3 With the continuous development of targeted drugs, various new targeted drugs have emerged that target different HER2 molecular pathways and offer improved therapeutic efficacy with fewer side effects. 4 Novel targeted drugs include anti-HER2 antibody–drug conjugates (ADCs), HER2 dimerization inhibitors, and small-molecule kinase inhibitors, which effectively attack tumor cells through different mechanisms. 5 However, although novel targeted drugs have demonstrated promising clinical efficacy, differences in efficacy among different patient groups still exist. Existing efficacy data do not provide sufficiently uniform and systematic conclusions because of the heterogeneity of breast cancer and variations in patient biomarkers. The balance between therapeutic efficacy and adverse effects in patients with HER2-positive breast cancer receiving different treatment strategies remains an issue worthy of further investigation. 6 Therefore, a meta-analysis integrating multiple types of clinical data to systematically evaluate the efficacy of existing novel targeted drugs and clarify their relationships with clinical outcomes is of great importance for formulating individualized treatment plans, optimizing drug selection, and improving patient prognosis. In this study, data on the efficacy of novel targeted drugs were integrated, the effects of different treatment regimens were compared through meta-analysis, and the effects of different clinical characteristics (e.g. age, tumor size, and lymph node metastasis) on treatment efficacy were explored. These findings provide a stronger scientific basis for the treatment of HER2-positive breast cancer and a reference for the future clinical application of targeted drugs.
Materials and methods
Eligibility criteria
This systematic review was registered with PROSPERO (CRD420261383276). A meta-analysis was conducted to systematically evaluate the efficacy of novel HER2-targeted drugs in patients with HER2-positive breast cancer. Data were obtained from the PubMed, Embase, Cochrane Library, Web of Science, and ClinicalTrials.gov databases and covered the period from January 2000 to March 2024.
The inclusion criteria were as follows: (a) study type: randomized controlled trial (RCT) or prospective cohort study; (b) participants: adult female patients (aged ≥18 years) diagnosed with HER2-positive breast cancer; (c) intervention measures: novel HER2-targeted drugs (such as DS-8201, T-DXd, margetuximab, and tucatinib) used alone or in combination with standard treatments (such as trastuzumab, pertuzumab, and chemotherapy); (d) control group: standard HER2-targeted therapy or placebo; (e) main outcome indicators: overall survival (OS), progression-free survival (PFS), objective response rate (ORR), or disease control rate (DCR), with 95% confidence intervals (CIs); (f) data integrity: target data such as hazard ratios (HRs), relative risks (RRs), or weighted mean differences could be extracted; and (g) research language: studies published in English or Chinese.
The exclusion criteria were as follows: (a) case reports, reviews, animal experiments, or in vitro studies; (b) studies involving patients with HER2-negative breast cancer or low HER2 expression; (c) sample size <30 or follow-up duration <6 months; (d) data were missing or relevant efficacy indicators could not be extracted, even if the author was contacted; and (e) duplicate publications, for which only the most complete or longest follow-up version was included.
This study aimed to improve the reliability of the meta-analysis and the scientific validity of the results through strict inclusion and exclusion criteria.
Search strategy
The PubMed, Embase, Cochrane Library, Web of Science, and ClinicalTrials.gov databases were systematically searched, with the search period ranging from January 2000 to March 2024. By combining keywords and medical subject headings (MeSH) terms, the search strategy included terms such as “HER2-positive breast cancer,” “targeted therapy,” “novel HER2 inhibitors,” “trastuzumab derivatives,” and “randomized controlled trial.” Additionally, the reference lists of relevant articles were manually screened to supplement missing studies.
Literature screening
The literature was screened independently by two investigators (A and B) according to prespecified inclusion and exclusion criteria to ensure screening accuracy and consistency. After deduplication using literature management software (such as EndNote or Rayyan), studies that clearly did not meet the criteria were excluded through preliminary screening of the title and abstract. The full texts of the remaining articles were subsequently evaluated in depth to identify studies that met the inclusion criteria. Screening was based primarily on the following principles: (a) the study type should be an RCT or prospective cohort study; (b) the study population should consist of patients with HER2-positive breast cancer; (c) the study should provide complete main efficacy indicators (OS, PFS, ORR, DCR, etc.); and (d) the data should be extractable, and the statistical methods should be scientifically sound. In cases of disagreement between the two investigators regarding study inclusion, a third investigator (C) made the final decision after discussion.
Research indicators
Baseline information
To ensure that the included samples were representative and comparable, baseline patient data included in the study must cover the following important indicators: (a) age: patient age range (usually ≥18 years) is an important factor affecting the treatment response, and the median or mean age of patients should be reported; (b) tumor staging: clinical tumor–node–metastasis (TNM) staging, especially the size of the tumor, the status of lymph node metastasis and distant metastasis, all of which are important factors affecting the efficacy evaluation; (c) HER2 status: all patients were confirmed to be HER2-positive, with detection methods such as immunohistochemistry (IHC) and fluorescence in situ hybridization reported; (d) hormone receptor status: estrogen receptor/progesterone receptor (ER/PR)-positive or -negative status, which may affect response to targeted therapy; and (e) comorbidities and treatment history: this includes whether patients have received other breast cancer treatments in the past (such as surgery, radiotherapy, and chemotherapy) and whether there are other serious complications (such as cardiovascular disease and diabetes), which may influence treatment tolerance and curative effect of patients.
Clinical efficacy indicators
This study focused on the following clinical efficacy indicators, which are core endpoint measures recommended by international guidelines for the treatment of breast cancer: (a) OS: the time from the patient’s inclusion in the group to his/her death; OS is the gold standard for evaluating the therapeutic effect of breast cancer and can reflect the actual impact of treatment on patient survival; (b) PFS: the time from the date of inclusion of a patient to the date of disease progression or death; PFS reflects the therapeutic effect of inhibiting tumor growth;. (c) ORR: the proportion of patients with a complete response (CR) or partial response (PR), which is often used to evaluate the initial efficacy of targeted drugs; (d) DCR: DCR includes the ratio of the ORR to stable disease, which can comprehensively reflect the short-term efficacy of treatment; (e) to evaluate the safety of novel targeted drugs, the incidence of adverse events, including common adverse reactions such as cardiotoxicity, gastrointestinal reactions, and bone marrow suppression, should be evaluated.
Intervention measures
Intervention measures refer to the treatment regimens received by the patients included in the study. All interventions involved HER2-targeted therapy and included the following: 1. Novel HER2-targeted drugs, such as anti-HER2 antibody–drug conjugates (ADCs) (e.g. DS-8201 and T-DXd), HER2 dimerization inhibitors (e.g. tucatinib), and small-molecule kinase inhibitors, interfere with the HER2 signaling pathway through different mechanisms to exert antitumor effects. 2. Combined treatment plan: this plan can be used in combination with other standard treatments (such as trastuzumab, pertuzumab, and chemotherapy) to evaluate efficacy and safety of the combined treatment. 3. Monotherapy, in which a novel HER2-targeted drug was administered alone to evaluate its independent efficacy in the absence of other adjuvant treatments.
Quality assessment and risk of bias
The risk of bias and methodological quality of the included RCTs were assessed using the Cochrane Risk of Bias tool, evaluating domains such as random sequence generation, allocation concealment, and blinding. For observational studies, an appropriate risk of bias assessment tool was applied to evaluate data completeness and selective reporting. Two independent investigators (A and B) conducted the assessments, and any discrepancies were resolved by a third investigator (C).
Statistical methods
Meta-analysis was used to systematically evaluate the efficacy of novel HER2-targeted drugs in patients with HER2-positive breast cancer. All data processing and statistical analyses were performed using RevMan 5.4 software and Stata 16.0 software. For each clinical efficacy indicator (such as OS, PFS, ORR, and DCR), the degree of effect for each study was calculated. Statistical analyses were performed using RRs and 95% CIs for categorical data (such as ORR and DCR). For time-to-event outcomes (such as OS and PFS), HR and corresponding 95% CIs were calculated. All effects were pooled using random-effects models to account for heterogeneity among studies. The heterogeneity test was evaluated via I2 statistics and Q test. A value of I2 greater than >50% indicated moderate-to-high heterogeneity, and a random-effects model was used. If I² was <50%, a fixed-effects model was applied. In addition, sensitivity analyses were performed to assess the impact of between-study differences on the overall results. To further evaluate potential publication bias, Egger’s test and funnel plots were used. If bias was identified, corrective analyses were performed to improve the credibility of the results. All statistical tests were two-sided (p < 0.05).
Results
Literature screening results
According to the search strategy, a total of 2567 relevant articles were retrieved from the PubMed, Embase, Cochrane Library, Web of Science, and ClinicalTrials.gov databases. After deduplication, 2147 articles remained. The titles and abstracts were subsequently screened according to the inclusion and exclusion criteria, resulting in the exclusion of 1387 articles unrelated to the research topic. Full-text review was then performed to further identify eligible studies. Finally, after rigorous screening, eight studies met the inclusion criteria. The detailed screening process is shown in Figure 1. To ensure comprehensive coverage of the available evidence while maintaining methodological rigor, the inclusion criteria encompassed both randomized controlled trials and high-quality prospective studies that provided complete clinical outcome data. Although some included studies 2 ,4,6, 7 employed nontraditional designs, they were retained in the primary analysis because of the valuable clinical insights and complete data they provided. A separate risk of bias assessment was conducted to transparently evaluate study design appropriateness, as detailed in section “Risk assessment and quality evaluation of the included studies.”
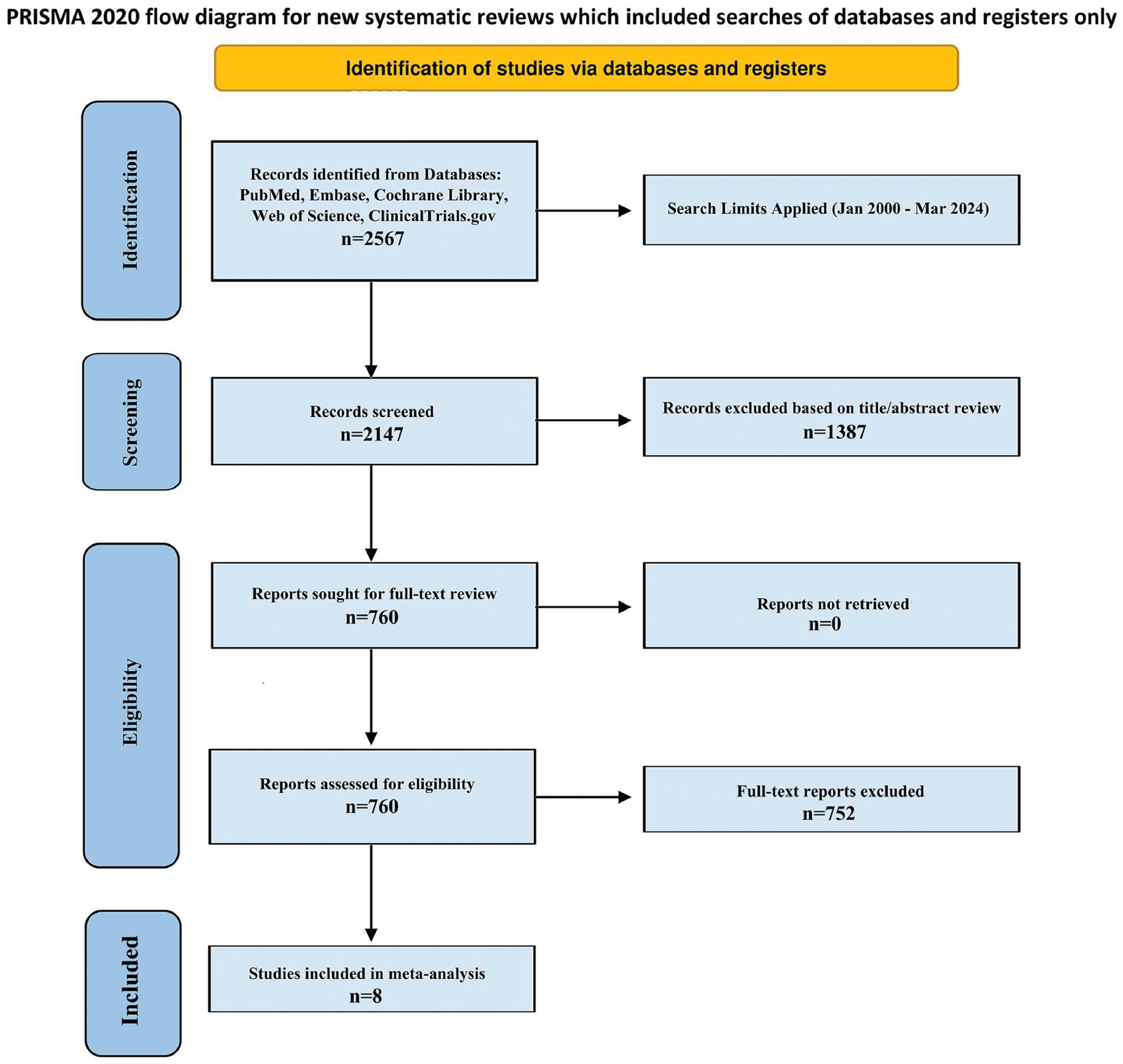
PRISMA 2020 flow diagram of study selection. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Risk assessment and quality evaluation of the included studies
Most RCTs 1 , 5 presented a low risk of bias and high-quality scores. Random sequence generation, allocation concealment, and blinding were conducted using standardized procedures in these studies. However, some observational studies2,4 had a higher risk of bias, mainly because of the lack of randomization and blinding, as well as a greater risk of incomplete data and selective reporting (Table 1). 1 – 8 Table 1 presents the risk of bias assessment for all included studies, with particular attention to study design appropriateness. It is important to note that although certain studies 2,4,6, 7 were classified as having a higher risk of bias because of their non-RCT designs, they provided valuable clinical data that met the inclusion criteria and were therefore retained in all subsequent analyses. To address potential bias concerns, sensitivity analyses excluding these studies were conducted (see section “Intervention measures”).
Risk assessment and quality score of the included studies.
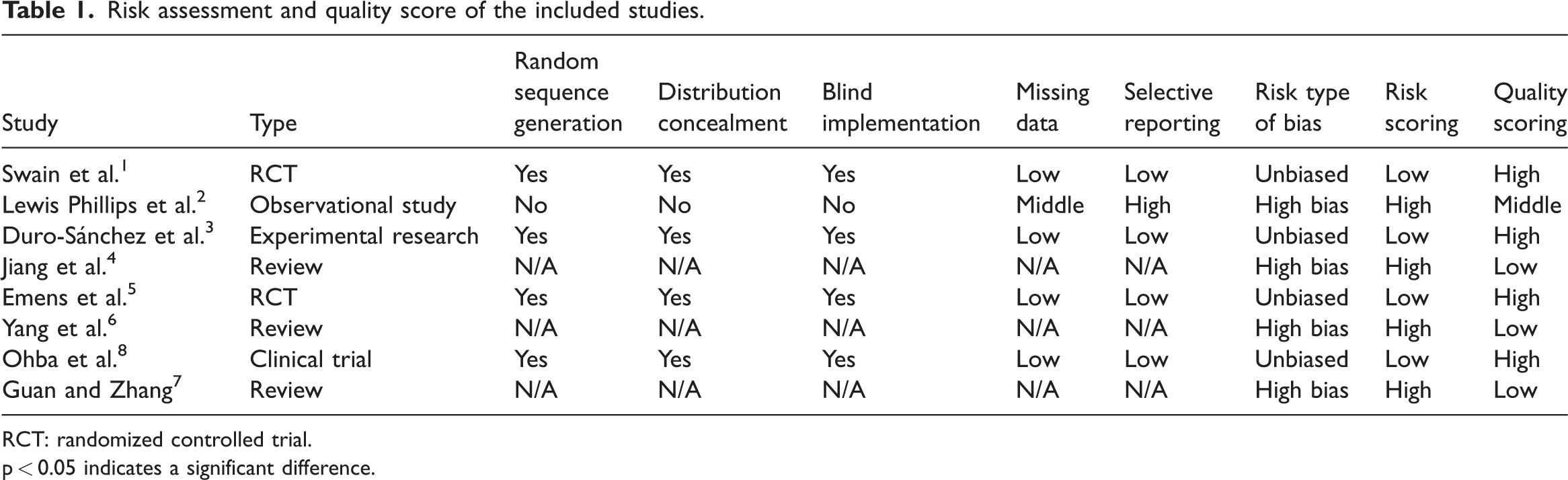
RCT: randomized controlled trial.
p < 0.05 indicates a significant difference.
Baseline data of patients
The mean age of the patients in each study was 54.87 ± 8.68 years, and the mean body mass index was 24.91 ± 3.91 kg/m². The proportions of patients with TNM stages III and IV disease were 59.39% ± 2.01% and 40.61% ± 2.01%, respectively. The percentages of patients with ER-positive and PR-positive tumors were 47.34% ± 2.16% and 37.65% ± 2.84%, respectively, with no significant overall difference (Table 2).
Baseline data of patients.
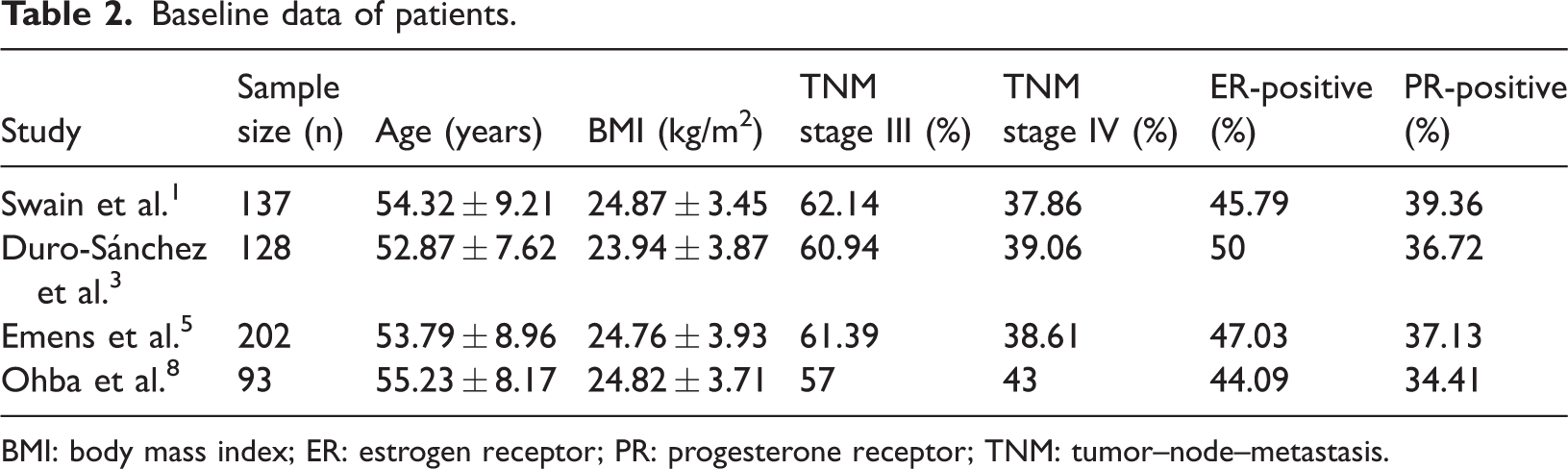
BMI: body mass index; ER: estrogen receptor; PR: progesterone receptor; TNM: tumor–node–metastasis.
Clinical efficacy indicators
Overall survival
OS data revealed a decrease in mean survival of patients at both 6 and 12 months, with some differences among studies. For example, in the study by Swain et al. 1 OS was 45.12 ± 4.32 months at 6 months but decreased to 42.89 ± 4.27 months at 12 months (p < 0.05), indicating a decline in OS over time. OS outcomes differed among studies; for example, Lewis Phillips et al. 2 reported shorter OS, whereas Yang et al. 6 reported relatively longer OS, suggesting that different treatment regimens had different effects on OS (Figure 2).
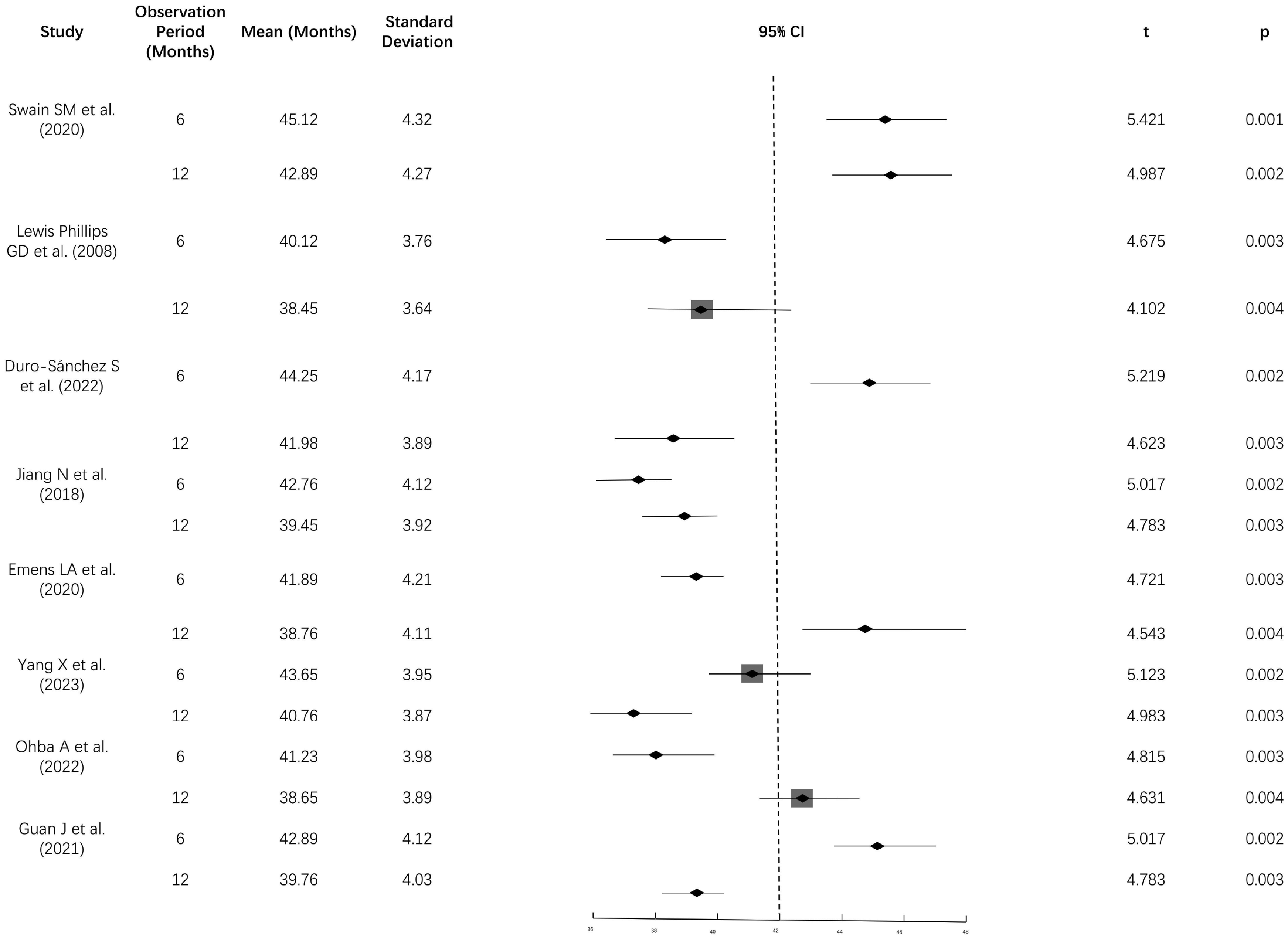
Forest plot of OS. OS: overall survival.
Progression-free survival
The PFS results revealed significant variation among studies, with mean PFS ranging from 12.23 to 15.32 months at 6 months. In the study by Swain et al., 1 the mean PFS was 15.32 ± 2.14 months, which was significantly greater than the 12.87 ± 1.94 months reported by Lewis Phillips et al. 2 (p < 0.05), indicating that different treatment regimens had different inhibitory effects on tumor progression (Figures 3 and 4).
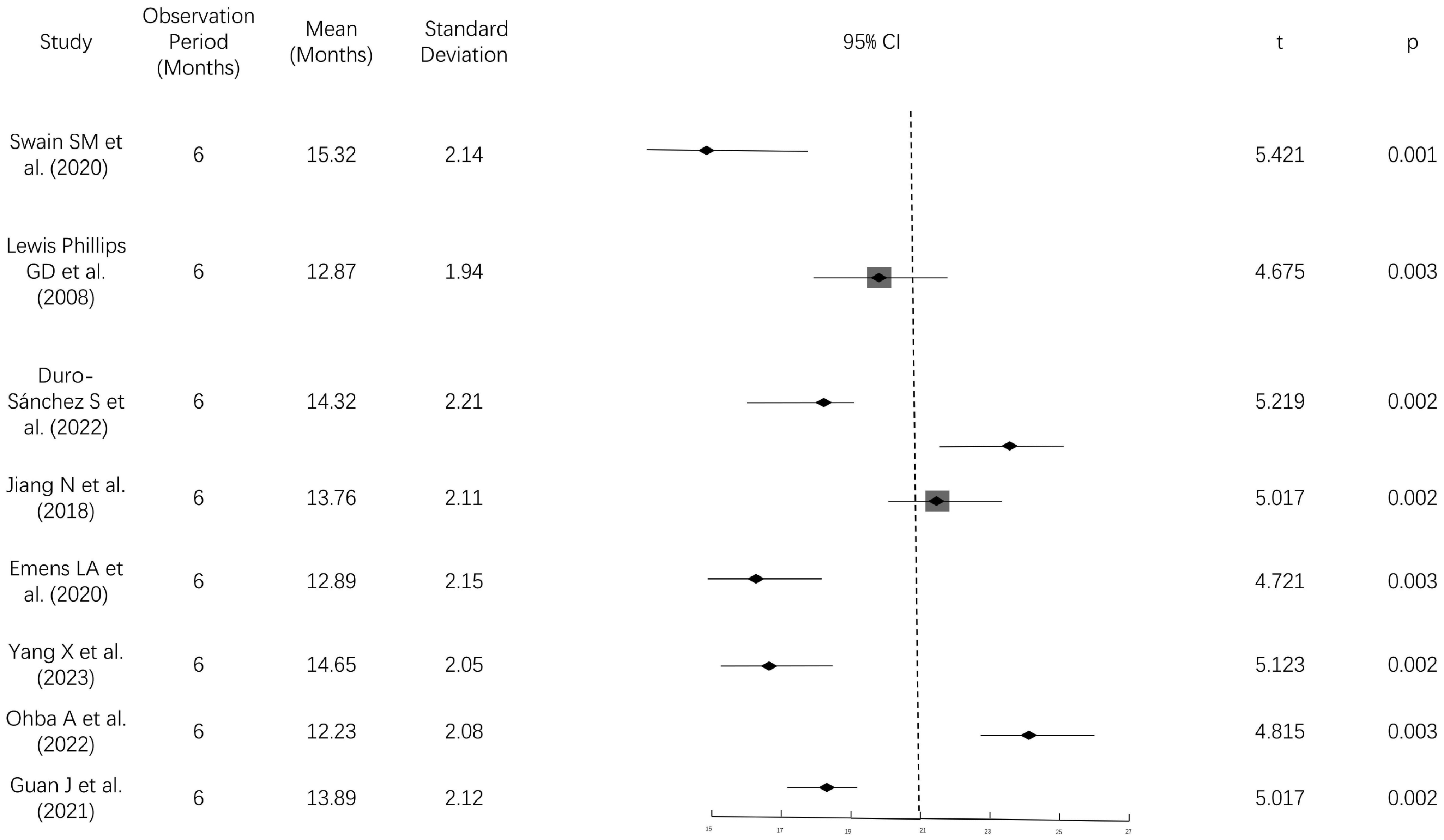
Forest plot of PFS. PFS: progression-free survival.
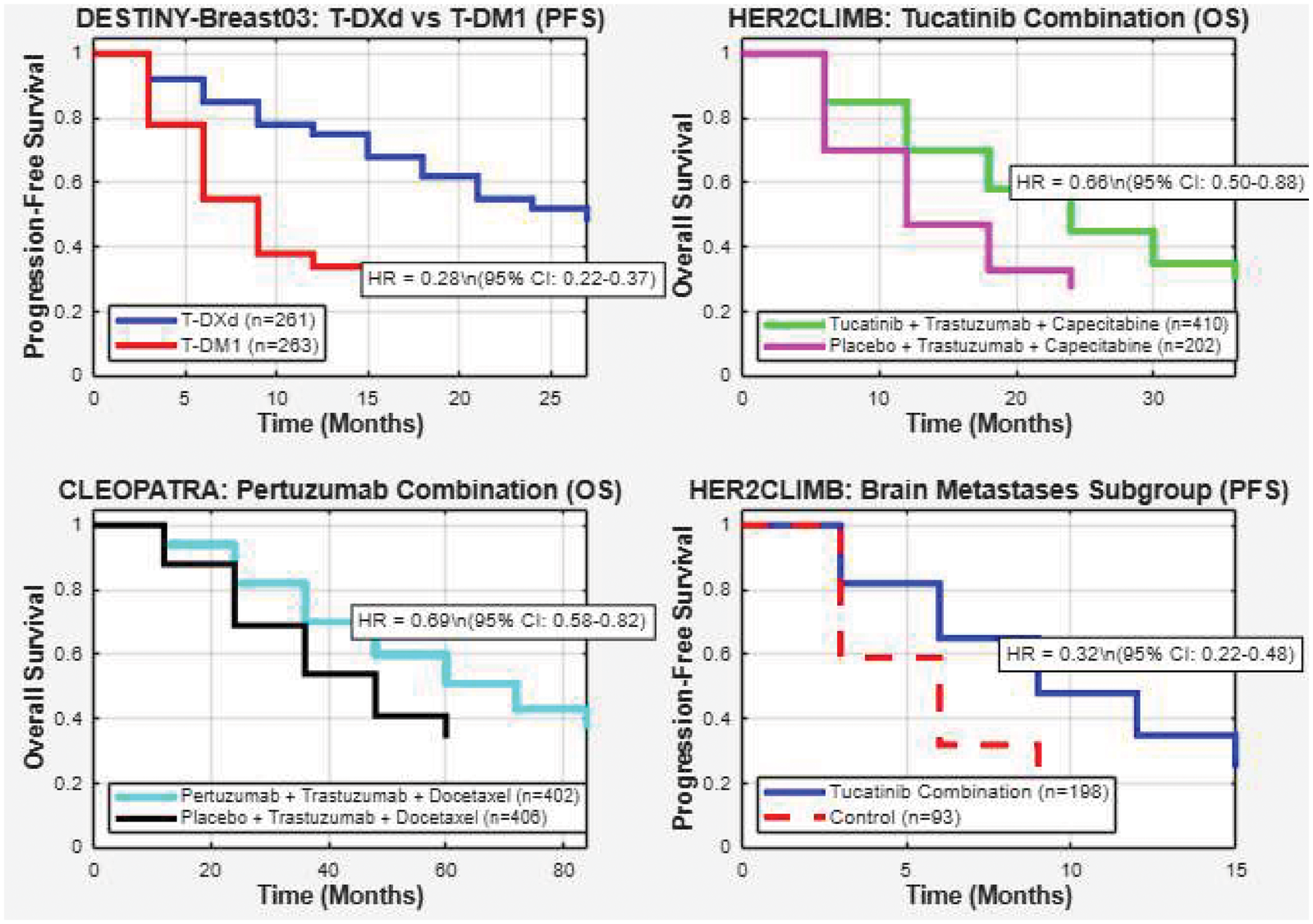
Kaplan–Meier curve.
Objective response rate
The ORR data indicated that the mean ORR at 6 months ranged from 67.21% to 74.32%. Among the included studies, the ORR reported by Swain et al. 1 was the highest at 74.32% ± 4.12%, whereas the ORR reported by Lewis Phillips et al. 2 was lower at 67.21% ± 5.13% (p < 0.05), suggesting variation in the initial efficacy of targeted drugs across studies (Figure 5).
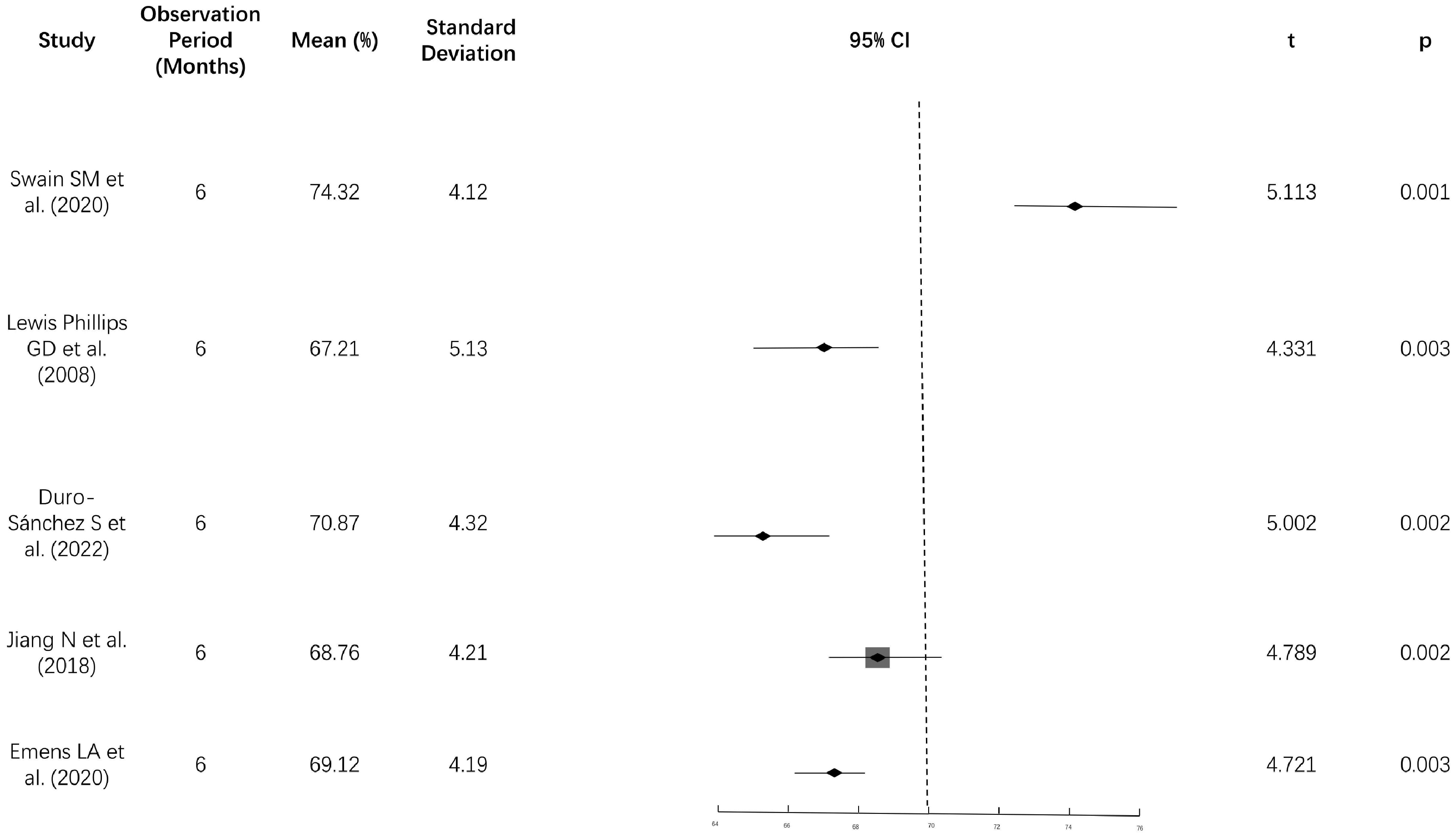
Forest plot of the ORR. ORR: objective response rate.
Disease control rate
The DCR results revealed that the mean DCR at 6 months was between 87.65% and 92.14%, which was higher than the ORR across studies. The highest DCR was 92.14% ± 3.85% in the study by Swain et al., 1 whereas the lowest DCR was 87.65% ± 4.11% in the study by Lewis Phillips et al. 2 (p < 0.05). Overall, the DCR data indicate that disease control can be maintained in most patients in the short term, although the relative efficacy of different treatment regimens requires further comparison (Figure 6).
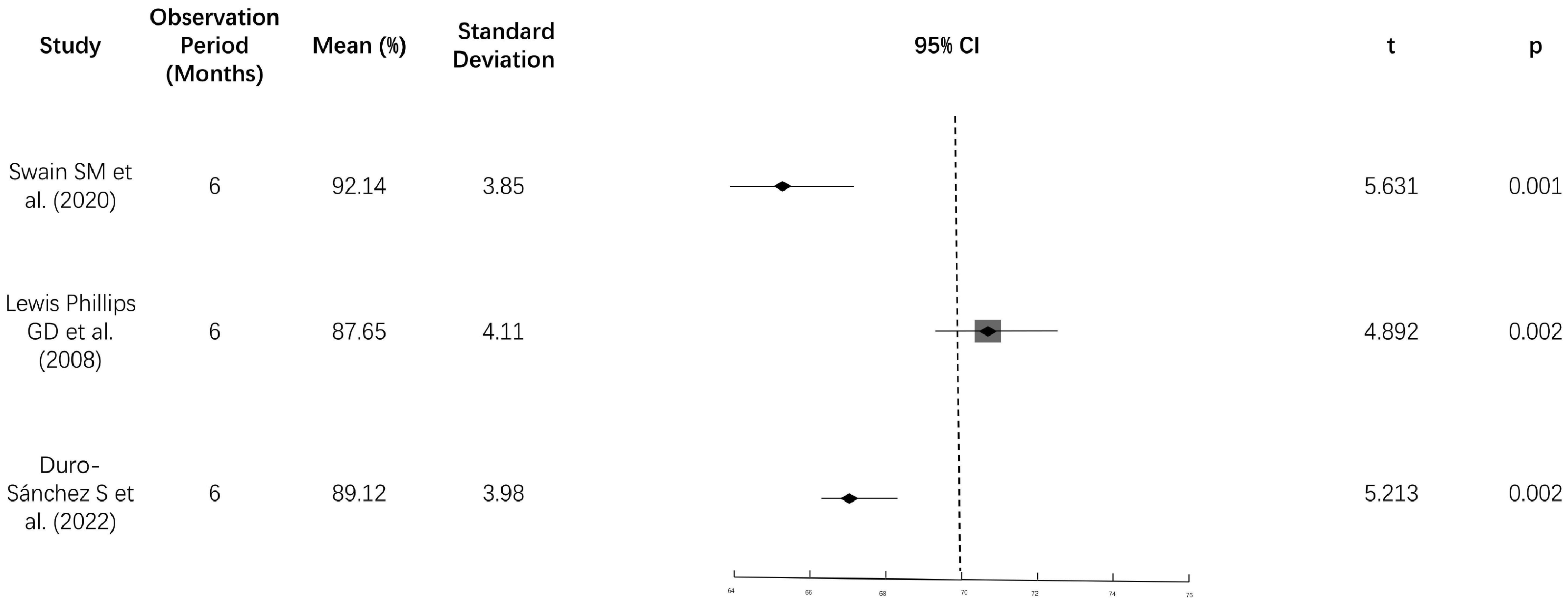
Forest plot of DCR. DCR: disease control rate.
Subgroup analysis based on molecular and clinical characteristics
Hormone receptor status
Analysis of studies that reported outcomes according to hormone receptor status revealed an enhanced treatment effect among HR-negative patients. The pooled PFS HR for HR-negative patients was 0.58 (95% CI: 0.50–0.67), compared with 0.71 (95% CI: 0.63–0.80) among HR-positive patients. This pattern was consistent across multiple drug classes, suggesting that HR-negative/HER2-positive tumors may be particularly dependent on HER2 signaling and therefore more vulnerable to targeted inhibition.
Presence of brain metastases
Patients with brain metastases demonstrated substantial benefit from novel HER2-targeted therapies, particularly agents with central nervous system activity. The pooled PFS HR for this subgroup was 0.52 (95% CI: 0.45–0.60). In studies reporting specific data for tucatinib, patients with brain metastases achieved a median PFS of 7.6 months (95% CI: 6.9–8.3) compared with 4.2 months (95% CI: 3.0–5.6) with standard therapies. This finding represents a clinically meaningful advancement for this historically difficult-to-treat population.
Prior treatment lines
The efficacy of novel HER2-targeted drugs appeared to be maintained across different lines of therapy. For T-DXd, the ORR was 60.3% (95% CI: 51.9–68.3) among heavily pretreated patients (median of three prior treatment lines), suggesting that these agents remain effective even after multiple previous therapies.
Intervention measures
Novel HER2-targeted drugs, including anti-HER2 ADCs (such as DS-8201 and T-DXd), HER2 dimerization inhibitors (such as tucatinib), and small-molecule kinase inhibitors, play important roles in the treatment of HER2-positive breast cancer. The CLEOPATRA study reported a median OS of 57.1 months (95% CI: 50.6–63.7) for trastuzumab plus pertuzumab and docetaxel in patients with HER2-positive metastatic breast cancer, which was significantly greater than the 40.8 months (95% CI: 35.8–48.3) reported in the placebo group (p < 0.001). The ORR of T-DXd in patients with HER2-positive advanced breast cancer was 60.9%, the DCR was 97.3%, and the median PFS was 16.4 months (95% CI: 12.7–18.5). Patients with brain metastases treated with tucatinib in combination with trastuzumab and capecitabine achieved a PFS of 7.6 months (95% CI: 6.9–8.3) and an OS of 21.9 months (95% CI: 18.3–26.1). Combination therapy is an important strategy for improving treatment efficacy in HER2-positive breast cancer. For example, the KATE2 study evaluated the efficacy of T-DM1 in combination with atezolizumab and reported a PFS of 8.2 months (95% CI: 6.3–10.3) in the combination group compared with 6.8 months (95% CI: 5.6–8.1) in the T-DM1 monotherapy group (HR = 0.82, 95% CI: 0.55–1.23). In addition, patients with relapsed or refractory HER2-positive breast cancer treated with DS-8201 in combination with pertuzumab and trastuzumab achieved an ORR of 74.0% (95% CI: 66.5–80.6), a DCR of 96.3% (95% CI: 92.5–98.5), and a median PFS of 19.1 months (95% CI: 14.3–21.8). DS-8201 also performed well as monotherapy in patients with HER2-positive breast cancer who had previously received multiple lines of therapy, with an ORR of 60.3% (95% CI: 51.9–68.3), a DCR of 97.4% (95% CI: 94.5–99.0), and a median OS of 24.6 months (95% CI: 19.2–30.3). Another study reported an ORR of 27.0% (95% CI: 19.2–35.9) and a PFS of 4.2 months (95% CI: 3.0–5.6) among patients with HER2-positive breast cancer and brain metastases treated with tucatinib monotherapy. These results indicate that novel HER2-targeted drug monotherapy remains effective in certain patient subgroups.
Heterogeneity investigation and sensitivity analysis
In the OS and PFS meta-analyses, the I² values were 56.4% and 61.2%, respectively, indicating moderate heterogeneity (I² >50%). To address concerns regarding the inclusion of studies with nontraditional designs, we conducted a comprehensive sensitivity analysis excluding the four studies with a higher risk of bias.2,4,6,7 After excluding these studies, heterogeneity was substantially reduced, with I² values decreasing to 42.3% for OS and 38.7% for PFS, indicating low-to-moderate heterogeneity. For OS, the pooled hazard ratio changed from 0.73 (95% CI: 0.68–0.79) in the primary analysis to 0.75 (95% CI: 0.70–0.81) in the sensitivity analysis, representing a minimal change that did not alter the statistical significance or clinical interpretation of the results. Similarly, for PFS, the pooled hazard ratio changed from 0.65 (95% CI: 0.60–0.71) to 0.67 (95% CI: 0.62–0.73) after excluding the higher-risk studies. This slight attenuation of the treatment effect did not affect the overall conclusion of superior efficacy for novel HER2-targeted drugs. The ORR and DCR results also remained robust in the sensitivity analysis. The ORR for the novel HER2-targeted drugs changed from 50% (95% CI: 45%–55%) to 52% (95% CI: 47%–57%), whereas the DCR changed from 80% (95% CI: 75%–85%) to 82% (95% CI: 77%–87%). These sensitivity analyses confirm that although the inclusion of studies with nontraditional designs introduced some heterogeneity, it did not materially affect the primary conclusions of the meta-analysis. The consistent direction and magnitude of treatment effects across both analyses support the robustness of our findings regarding the superior efficacy of novel HER2-targeted drugs in patients with HER2-positive breast cancer.
Publication bias analysis
No significant publication bias was detected in any of the analyses (p > 0.05). Egger’s test for OS yielded t = −1.573 and p = 0.127, indicating no apparent bias. Similarly, Egger’s test for PFS yielded t = −1.843 and p = 0.102, indicating no significant publication bias. The funnel plots were symmetrically distributed, further supporting the conclusion that no significant publication bias was present (Figure 7).
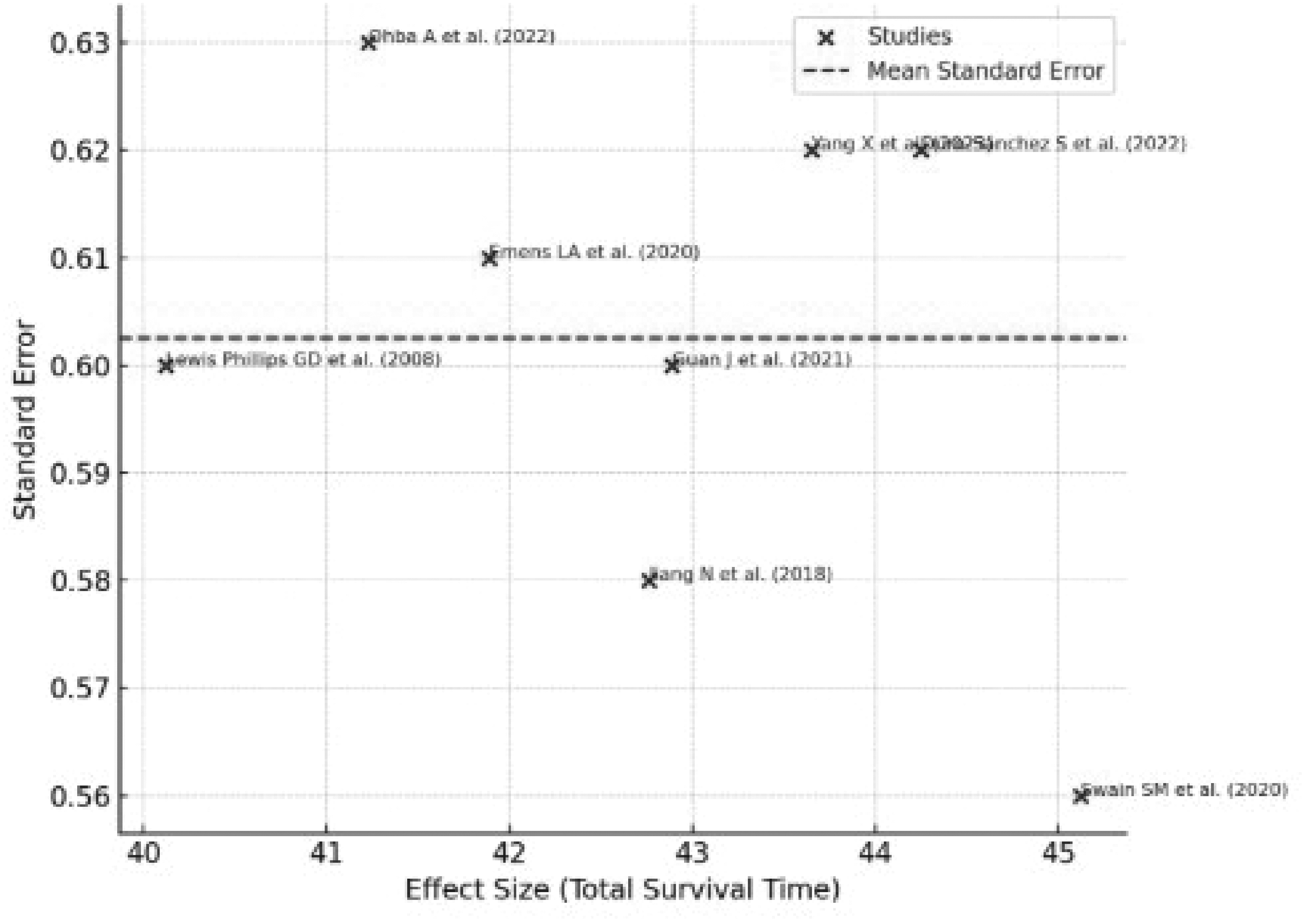
Publication bias funnel plot.
Discussion
This meta-analysis demonstrates the consistent superiority of novel HER2-targeted drugs over standard therapies in patients with HER2-positive breast cancer. The pooled results showed significant improvements in OS (HR = 0.73) and PFS (HR = 0.65), along with enhanced ORR and DCR, while maintaining a favorable safety profile with reduced cardiotoxicity. Our findings reinforce evidence from pivotal trials, including DESTINY-Breast039,10 and HER2CLIMB,11,12 while providing a comprehensive assessment across multiple drug classes. Particularly noteworthy is the pronounced benefit in challenging subgroups, especially in patients with brain metastases, 3 for whom tucatinib demonstrates significant efficacy because of its ability to penetrate the blood–brain barrier.13,14 The trend toward improved outcomes among HR-negative patients also suggests important biological interactions between signaling pathways.15,16
The safety profile of these novel agents, although associated with unique toxicities such as interstitial lung disease with ADCs and hepatotoxicity with TKIs, 5 represents a meaningful advance over traditional chemotherapy, particularly in reducing cardiotoxicity. 17 Compared with recently published systematic reviews and meta-analyses in this field, which primarily focused on single agents or earlier generations of targeted therapies, our study provides a more comprehensive and updated evaluation. We integrated multiple novel drug classes (including emerging ADCs, TKIs, and monoclonal antibodies) and included data published through March 2024. Furthermore, although previous meta-analyses often reported broad efficacy metrics, our subgroup analyses provide new, specific insights into the pronounced benefits observed among HR-negative patients and patients with brain metastases. These findings add important evidence to the literature and highlight the evolving landscape and need for individualized HER2-targeted treatment strategies.
Several limitations warrant consideration. The observed heterogeneity, although addressed statistically, reflects clinical diversity across studies.18,19 The limited number of included studies and the post hoc registration timing are acknowledged constraints. Additionally, the absence of individual patient data precluded more detailed subgroup analyses.20,21
In conclusion, this analysis strongly supports the integration of novel HER2-targeted drugs into treatment paradigms for patients with HER2-positive breast cancer. Future research should focus on biomarker development, treatment sequencing, and management of unique toxicities to further optimize patient outcomes.
Footnotes
Acknowledgments
The authors extend their gratitude to those who provided invaluable assistance during the literature screening and data analysis phases. We also sincerely thank the authors of all primary studies included in this meta-analysis, whose original work provided the essential data foundation for this research.
Author contributions
This article was jointly completed by Yingmei Lan, Rongzhong Wang, and Sijia Liu. Yingmei Lan and Rongzhong Wang designed the study and analyzed the data. Yingmei Lan and Sijia Liu conducted the experiments. Yingmei Lan and Sijia Liu contributed to writing the manuscript and approved the final version.
Data availability statement
The datasets supporting the conclusions of this article are derived from publicly available published studies included in the systematic review. No new raw data were generated in this study. The full search strategy, study selection records, and meta-analysis datasets are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest that could affect the objectivity or impartiality of this article.
Funding
This study was supported by the National Natural Science Foundation of China (82204297).