
Abstract
Polyneuritis cranialis is characterized by the simultaneous or sequential inflammation of multiple cranial nerves, which may occur unilaterally or bilaterally. Although it is often related to infection, its exact etiology remains unclear. Due to its nonspecific clinical manifestations, diagnosis typically relies on the exclusion of other conditions. Herein, we report a case of postinfectious polyneuritis cranialis. The patient presented to our hospital with restricted mouth opening, dysphagia, coughing while drinking, dysarthria, and posterior neck pain following a finger injury. Laboratory tests showed markedly elevated inflammatory markers. Neurological examination revealed involvement of cranial nerves V, IX, X, and XII. Motor nerve conduction studies of the facial nerve suggested partial facial nerve damage. Brain magnetic resonance imaging demonstrated mild nonspecific white matter changes. After exclusion of alternative diagnoses, the patient was diagnosed with polyneuritis cranialis. The patient’s condition improved following corticosteroid pulse therapy and was subsequently discharged. This case highlights that the diagnosis of polyneuritis cranialis remains one of exclusion and is often clinically challenging. When encountering patients with rapidly progressive cranial nerve palsies, polyneuritis cranialis should be included in the differential diagnosis after more common structural or systemic etiologies have been excluded.
Keywords
Background
Polyneuritis cranialis (PNC) is characterized by paralysis of two or more cranial nerves (CNs), which may occur unilaterally or bilaterally, in the absence of spinal cord involvement. 1 Although the exact etiology remains unclear, PNC is generally considered a postinfectious hypersensitivity reaction. 2 Commonly identified triggers or associated factors include viral infections (such as varicella-zoster virus), underlying autoimmune diseases, and tumors.3,4 The precise prevalence and incidence of PNC are uncertain, as most available evidence is derived from case reports and small case series. An early domestic report describing three cases was published in the Journal of Stroke and Nervous Diseases in 1987. 5 To date, the largest case series remains that of Keane, who retrospectively analyzed 979 patients presenting with simultaneous or sequential involvement of at least two CNs. 6 Clinical manifestations of PNC vary according to the specific CNs affected. The most commonly involved CNs are III, VII, X, and XII, whereas involvement of CNs II and VIII is less frequent. 7 Diagnosis is often challenging and relies primarily on the identification of multiple cranial neuropathies after exclusion of other neurological disorders. Current management focuses on treating any identifiable underlying cause and providing symptomatic support. Both intravenous immunoglobulin (IVIG) and corticosteroids have been reported to be effective therapeutic options for PNC.8–13
This article presents a typical case of postinfectious PNC. Based on the clinical manifestations of multiple CN deficits and the exclusion of alternative diagnoses through appropriate investigations, PNC was confirmed. The patient showed marked symptomatic improvement following steroid pulse therapy and recovered without sequelae. This case underscores the value of early recognition and timely intervention in achieving favorable outcomes in PNC and provides additional support for the use of corticosteroid therapy in its management.
Case presentation
A woman in her late 50s presented to Guizhou Provincial People’s Hospital in November 2024 with a 5-day history of limited mouth opening and dysphagia. Ten days before admission, she sustained a laceration to her left little finger from a sharp stone, resulting in skin breakdown and bleeding; the wound was treated with local hemostasis. Five days before presentation, she developed restricted mouth opening and dysphagia. Her symptoms progressively worsened thereafter. She gradually developed dysarthria, coughing while drinking, and a persistent mild pulling sensation in the posterior neck. She sought medical assistance at a local hospital, where a barium swallow examination showed no significant abnormalities, and laryngoscopy revealed chronic pharyngitis. As the etiology remained unclear, she was transferred to our hospital on the same day for further evaluation and treatment. The patient had previously been in good health, with no history of hypertension, diabetes, coronary artery disease, or other chronic illnesses.
The patient’s vital signs were normal on admission. She was alert and oriented. Physical examination revealed no abnormalities of the heart, lungs, or abdomen. Neurological examination showed bilaterally equal pupils (3 mm) with brisk pupillary light reflexes and intact corneal reflexes. Eye movements were normal in all directions, with no bilateral ptosis or diplopia, suggesting intact oculomotor nerve function. Forehead wrinkles and nasolabial folds were normal, and the corners of the mouth were not deviated, suggesting intact facial nerve function. Mouth opening was markedly limited (less than one fingerbreadth), with reduced contractile strength of the masseter and temporalis muscles on palpation. Facial sensation was intact and symmetrical bilaterally. Collectively, these findings suggested possible dysfunction of the motor division of CN V. Because of the restricted mouth opening, the jaw jerk reflex and pterygoid muscle strength could not be adequately assessed. In addition, the patient demonstrated restricted tongue protrusion, dysphagia, coughing while drinking, dysarthria, and a reduced gag reflex, indicating possible impairment of CNs IX, X, and XII. Oral examination revealed that the patient’s oromaxillofacial region was essentially symmetric, with no tenderness on palpation of the bilateral preauricular regions. Mouth opening was limited to less than one fingerbreadth, with a downward opening pattern. Bilateral condylar mobility, assessed by palpation through the external auditory meatus, was reduced. The patient described a pulling sensation in the posterior neck; however, active neck motion was full and unrestricted, without nuchal rigidity. Muscle strength and tone of the trapezius and sternocleidomastoid muscles were normal. Sensory examination for pain, temperature, and light touch was normal in all four limbs. Muscle strength and tone were normal, with no ataxia and a steady gait. All physiological reflexes were present, and no pathological reflexes were elicited. Overall, the examination findings were consistent with injury to multiple CNs.
To clarify the etiology of the multiple CN injuries, we conducted relevant examinations. Laboratory studies showed significant elevations in white blood cell (WBC) and neutrophil counts, accompanied by increased interleukin-6 (IL-6) and C-reactive protein (CRP) levels (Table 1). Blood biochemistry revealed mild abnormalities in cardiac enzymes and liver and kidney function (Table 2). Regarding imaging, noncontrast computed tomography of the jaw region showed no significant structural lesions (Figure 1). Concurrently, a stomatology consultation was obtained. Based on the combination of specialist physical examination and imaging findings, local causes, including odontogenic lesions, masticatory muscle disorders, and bone injury of the maxillofacial region were ruled out as causes of the patient’s limited mouth opening and dysphagia. Following recommendations from the neurology consultation, additional investigations were further performed. Lumbar puncture was undertaken to evaluate possible neuroinfection. Cerebrospinal fluid (CSF) analysis showed no significant abnormalities, and cultures demonstrated no bacterial or fungal growth (Table 3). The neostigmine test and repetitive nerve stimulation (RNS) were performed to exclude myasthenia gravis (MG), and both yielded negative results. Magnetic resonance imaging (MRI) demonstrated mild nonspecific white matter changes, with no evidence of skull base or cavernous sinus lesions, brain tumors, or cerebral infarction (Figure 2). Needle electromyography (EMG) of the masseter, frontalis, orbicularis oris, mentalis, and upper-limb muscles was normal. Nerve conduction studies of the facial nerve revealed reduced motor conduction velocity (MCV) in the left facial nerve (temporal, buccal, and marginal mandibular branches), with decreased compound muscle action potential (CMAP) amplitude in the left buccal branch. The right facial nerve buccal branch showed reduced MCV, decreased CMAP amplitude, and temporal dispersion. All other examined nerves demonstrated normal MCV, sensory conduction velocity, and F-wave parameters. After exclusion of other central nervous system lesions, the patient was ultimately diagnosed with PNC. The diagnosis was supported by characteristic clinical features, including involvement of multiple CNs (limited mouth opening, restricted tongue protrusion, dysphagia, coughing while drinking, and dysarthria) without limb weakness or ataxia. Physical examination findings were consistent with CN impairment and correlated with facial nerve motor conduction studies demonstrating bilateral partial facial nerve involvement. The patient received intravenous (IV) methylprednisolone pulse therapy (1000 mg for 3 days, followed by 500 mg IV and then 250 mg IV for 3 days). In addition, acetylglutamine, vitamin B12, and butylphthalide sodium chloride injection were administered to promote neural repair and improve neurological function.
Main inflammatory parameters.
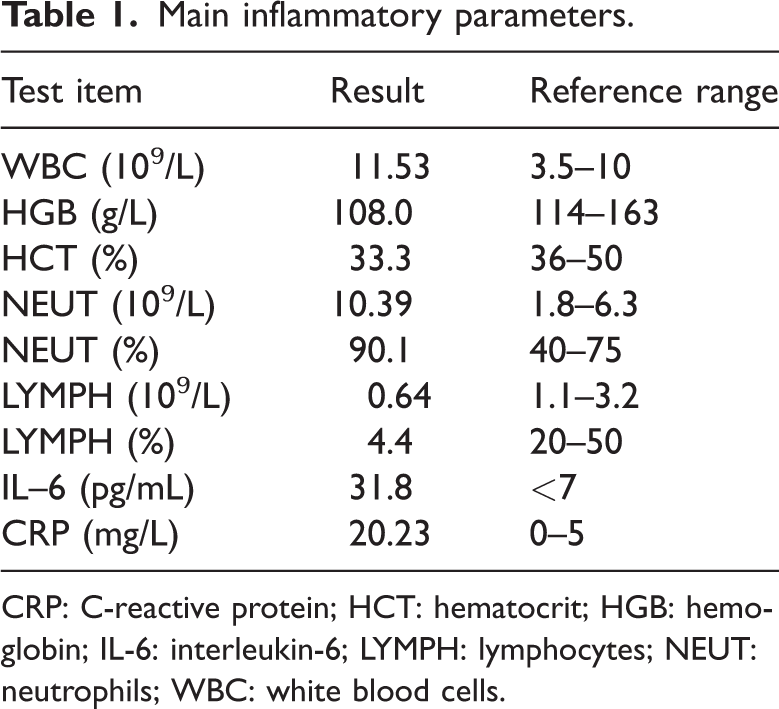
CRP: C-reactive protein; HCT: hematocrit; HGB: hemoglobin; IL-6: interleukin-6; LYMPH: lymphocytes; NEUT: neutrophils; WBC: white blood cells.
Abnormal liver, kidney function, and myocardial injury markers.
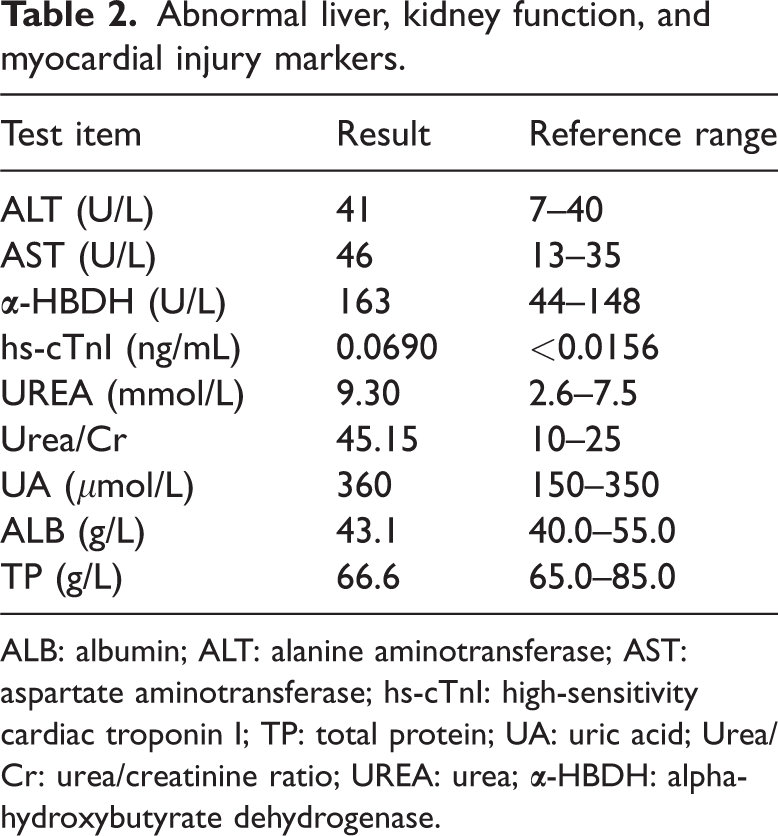
ALB: albumin; ALT: alanine aminotransferase; AST: aspartate aminotransferase; hs-cTnI: high-sensitivity cardiac troponin I; TP: total protein; UA: uric acid; Urea/Cr: urea/creatinine ratio; UREA: urea;
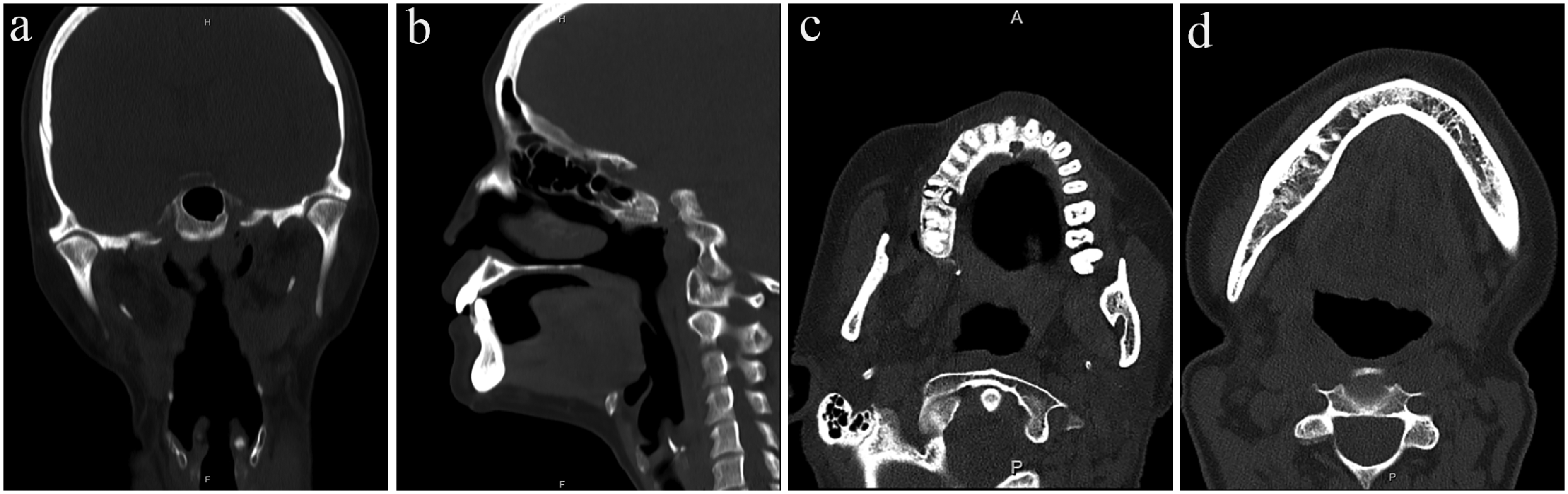
Imaging findings of the temporomandibular joints and jaw. (a) Coronal view of the craniofacial skeleton. (b) Sagittal view of the craniofacial skeleton. (c) Axial view of the maxilla. (d) Axial view of the mandible.
Cerebrospinal fluid analysis.

Glu: glucose; ICP: intracranial pressure; IgG: quantitative immunoglobulin G; NCC: nucleated cell count; PROT: protein.

Brain MRI of the present case. Axial T2-FLAIR of the brain shows white matter hyperintensities. MRI: magnetic resonance imaging.
Following the above treatments, the patient’s symptoms improved markedly. Trismus and dysphagia improved significantly, with mouth opening increasing from less than one fingerbreadth on admission to approximately three fingerbreadths by discharge (Figure 3). On the 23rd day of hospitalization, IV methylprednisolone was transitioned to oral prednisone acetate tablets (1 mg/kg/day), which were tapered by 5 mg every 2 weeks. After 24 days of treatment, the patient’s symptoms had nearly resolved, with normal mouth opening and tongue protrusion and no further dysphagia or coughing while drinking. The patient was discharged on a tapering regimen of prednisone acetate. At follow-up, when the dosage had been reduced to 30 mg daily, the patient’s condition remained stable, with normal oral intake and swallowing function and no recurrence of symptoms.

(a) On admission, the patient had limited mouth opening, measuring less than one finger’s breadth. (b) After treatment, the mouth opens normally to approximately three finger’s breadth.
The reporting of this study conforms to the Case Report (CARE) guidelines. 14 We obtained the patient’s signed consent for publication. We have de-identified all of the patient’s details such that the identity of the patient may not be ascertained in any way. In addition, we obtained consent from the patient for treatment.
Discussion
PNC is a rare neurological disorder characterized by unilateral or bilateral involvement of multiple CNs. 15 Its clinical manifestations vary depending on the specific CNs affected. Previous reviews have shown that PNC has several characteristic features. First, it typically presents acutely, often following a preceding infection, with initial nonspecific symptoms such as headache, dizziness, diplopia, hoarseness, and dysphagia. 13 Second, apart from the involvement of multiple CNs, there is no evidence of other neurological lesions; specifically, it is not accompanied by any limb symptoms or signs. 13 Another important characteristic is the absence of albuminocytological dissociation in the CSF. 13 The clinical presentation in our case closely aligned with these characteristic features. The patient had a history of trauma before the onset of neurological symptoms. Blood test results suggested infection and mild organ dysfunction. She presented with limited mouth opening, dysphagia, coughing while drinking, and dysarthria, suggesting involvement of CNs V, IX, X, and XII. Motor nerve conduction studies of the facial nerve further supported facial nerve involvement. Meanwhile, no limb symptoms or signs were observed throughout the entire disease course, and CSF analysis showed no albuminocytologic dissociation. Therefore, the patient met the clinical diagnostic criteria for PNC.
Notably, some reports have considered PNC to be a rare subtype of Guillain–Barré syndrome (GBS), accounting for approximately 3%–5% of all GBS cases.16–18 This is because some patients with GBS may initially present with PNC without ataxia, impaired consciousness, or significant limb weakness. 19 Nevertheless, these patients typically retain other core diagnostic features of GBS and its variants, including hyporeflexia, albuminocytologic dissociation in the CSF, neurophysiologic findings, and seropositivity for antiganglioside GQ1b and antiganglioside GT1a immunoglobulin G antibodies (anti-GQ1b or anti-GT1a IgG antibodies). 20 Consequently, despite presenting with features of PNC, these patients actually represent a phenotypic variant within the GBS spectrum. However, the clinical etiologies of PNC are diverse, and not all cases can be attributed to GBS. More common causes include infections (e.g. varicella-zoster virus or measles), immune abnormalities, poisoning, tumors, and other conditions. After the clinical manifestations and disease characteristics have been clarified, imaging studies play an important role in further supporting the diagnosis, particularly by excluding alternative disorders. Because of the small diameter and complex course of the CNs, conventional imaging techniques are often unable to adequately detect subtle lesions. 17 Therefore, imaging studies do not provide findings that are specific for the diagnosis of PNC. 21 Their primary utility lies in excluding structural causes such as tumors, meningiomas, and granulomatous diseases. The literature generally reports that most patients with PNC exhibit either normal brain MRI findings or only mild nonspecific white matter changes.8,10,11,16 In the present case, brain MRI demonstrated T2-FLAIR hyperintensity (Fazekas grade 1), consistent with mild nonspecific white matter changes and in agreement with previously reported findings. This nonspecific imaging finding further highlights that the diagnosis of PNC relies primarily on clinical manifestations and the exclusion of other pathologies.
Due to the nonspecific clinical presentation of PNC, diagnosis relies largely on exclusion. In this case, the differential diagnosis included MG, GBS, Miller Fisher syndrome (MFS), skull base pathology (e.g. nasopharyngeal carcinoma), brainstem encephalitis, and tetanus. The patient did not exhibit the typical diurnal fluctuation (morning improvement and evening worsening). Both the neostigmine test and RNS test were negative,13,22 effectively ruling out MG. GBS was excluded based on the absence of limb weakness, preserved reflexes, and normal CSF protein levels. MFS is typically characterized by the triad of ophthalmoplegia, ataxia, and areflexia, often accompanied by additional cranial nerve involvement, such as facial or bulbar palsy. 23 Although our patient presented with bulbar palsy, the absence of ophthalmoplegia and ataxia, together with preserved tendon reflexes, argued against MFS. Skull base metastasis from nasopharyngeal carcinoma was also excluded, as MRI did not reveal cortical bone defects or marrow replacement by low-signal tissue. 24 Brainstem encephalitis was likewise considered highly unlikely. This condition typically affects young adults and presents with CN palsies, ataxia, and pyramidal signs; 25 cranial MRI and CSF analysis usually aid in differentiation. In this case, neither the clinical presentation nor the investigation results were consistent with these features. In addition, it was important to differentiate the patient’s condition from tetanus. Typical tetanus is often associated with a history of trauma. Patients may present with prodromal symptoms such as fatigue, dizziness, headache, restlessness, sweating, and difficulty chewing. The hallmark clinical feature is generalized tonic spasm of the skeletal muscles, which typically begins in the masseter muscles and progressively spreads to other regions. 26 Specific manifestations may include dysphagia, trismus, risus sardonicus, neck stiffness, abdominal rigidity, as well as opisthotonos and respiratory distress caused by paroxysmal muscle spasms. 27 In this case, (a) the patient had a history of trauma but did not present with prodromal symptoms suggestive of tetanus infection; (b) although she experienced difficulty opening her mouth and swallowing, palpation revealed reduced contraction strength of the bilateral masseter and temporalis muscles rather than sustained tonic spasm, and her facial expression appeared natural; (c) she reported a pulling sensation in the posterior neck, but neck movement was unrestricted, with normal muscle strength and tone and no signs of neck stiffness; and (d) no opisthotonos or dyspnea was observed, and the abdomen remained soft. Therefore, tetanus was excluded. While progressively excluding other diseases and establishing a preliminary diagnosis of PNC, attention should also be paid to potential predisposing factors. Since the outbreak of the coronavirus disease 2019 (COVID-19) pandemic, multiple case reports and systematic reviews have confirmed that severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection can induce PNC as a peripheral nervous system complication of COVID-19.28,29 This condition may manifest as isolated cranial nerve involvement or occur in combination with GBS and MFS.28,30 Therefore, in the current era of persistent COVID-19 transmission, the possibility of SARS-CoV-2 infection should be considered in patients with PNC. In summary, the diagnosis of PNC in this case was established through the systematic exclusion of other potential conditions.
In the management of PNC, both corticosteroids and IVIG have been reported to be effective treatments, with most patients achieving favorable outcomes without residual deficits.8–13 Among these therapies, IVIG is applicable to patients with GBS presenting as PNC or its variants, special populations (such as pregnant women, children, and patients with diabetes), and settings in which medical resources permit. Corticosteroids are particularly suitable for patients with acute inflammatory presentations who are otherwise healthy, offering rapid anti-inflammatory effects at a relatively low cost. In this case, the patient had a history of trauma and markedly elevated inflammatory markers but was previously healthy and had no significant comorbidities. Given the confirmed diagnosis of PNC and her financial constraints, pulse corticosteroid therapy was selected as the primary treatment, supplemented with neurotrophic agents for supportive care. The patient ultimately achieved complete clinical recovery.
This report has several limitations, as certain key laboratory investigations could not be performed, and there was a lack of multidisciplinary collaborative diagnosis and treatment. First, owing to financial constraints, we were unable to perform antiganglioside antibody testing, particularly anti-GT1a antibody testing, could not be performed. Because anti-GT1a antibodies are closely associated with bulbar dysfunction, the absence of these data limited serological differentiation of GBS variants such as MFS and other autoimmune neuropathies. Second, screening for treatable pathogens, including varicella-zoster virus and other potentially relevant infections, was insufficient, which may have resulted in important infectious causes being overlooked. Furthermore, we lacked systematic evaluation of autoimmune markers and serum protein electrophoresis-related tests was not performed, limiting investigation of potential etiologies such as systemic autoimmune diseases, plasma cell disorders, and immunoglobulin proliferative abnormalities. In addition, multidisciplinary perspectives and research approaches were not integrated throughout the diagnostic and therapeutic process, limiting comprehensive multidimensional analysis of the disease. The absence of the aforementioned examinations and multidisciplinary research approaches restricted a more thorough etiological analysis and differential diagnosis. Therefore, the diagnosis was based largely on clinical features and the available investigations. This case suggests that, in future clinical practice, patients with complex CN involvement should undergo as comprehensive an evaluation as possible. In addition, multidisciplinary collaboration and interdisciplinary consultation should be strengthened to facilitate more accurate diagnosis.
Conclusion
In conclusion, our evaluation revealed that the diagnosis of PNC remains one of exclusion and is often clinically challenging. When encountering patients with rapidly progressive cranial nerve palsies, PNC should be included in the differential diagnosis after more common structural or systemic etiologies have been excluded. Establishing an early definitive diagnosis and promptly initiating high-dose corticosteroid pulse therapy are critical, as these measures may significantly improve neurological recovery and reduce the risk of permanent nerve injury.
Footnotes
Acknowledgments
We would like to thank the patient and her family for agreeing to the publication of this case report.
Author contributions
ZHM and WJ were responsible for drafting the manuscript, editing the manuscript, and approving the final version. PKJ, XXY, and HJJ contributed to data analysis and figure preparation. All authors read and approved the final manuscript.
Consent for publication
The authors obtained written informed consent from the patient for the publication of the data and images presented in this case report.
Data availability
All data supporting the findings of this study are included within the manuscript.
Declaration of conflicting interest
The authors declare that there are no competing interests.
Ethics approval and consent to participate
This report was approved by the Research Ethics Committee of The Second Affiliated Hospital of Guizhou University of Traditional Chinese Medicine (No. LW20251221; December 21, 2025). Consent was obtained from the patient and her family.
Funding
This work was supported by the Guizhou Provincial Science and Technology Projects (No. QKHJC-ZK[2022]-260); the Guizhou Provincial High-level Innovative Talent Projects (No. gzwjrs2023-005); and the Science and Technology Fund of the Guizhou Provincial Health Commission (No. gzwkj2021-320).