
Abstract
Immunoglobulin A nephropathy is a common glomerular disease associated with mucosal immune dysregulation. We report the case of a young woman diagnosed with biopsy-proven immunoglobulin A nephropathy who achieved sustained clinical remission following sequential tonsillectomy and appendectomy performed for standard clinical indications. Tonsillectomy was associated with improvement in hematuria, whereas proteinuria persisted. Four years later, appendectomy for chronic appendicitis was followed by complete resolution of the proteinuria. The temporal association between these interventions and changes in disease activity is notable; however, causality cannot be established. This case highlights the potential relevance of extrarenal mucosal inflammatory conditions in selected patients with immunoglobulin A nephropathy and underscores the complexity of disease activity assessment. These observations should be considered hypothesis-generating and require further investigation.
Introduction
Immunoglobulin (Ig) A (IgA) nephropathy (IgAN) is the most prevalent form of primary glomerulonephritis worldwide and is characterized by mesangial deposition of IgA-containing immune complexes. Clinically, IgAN presents with persistent or recurrent hematuria, variable proteinuria, and a heterogeneous long-term prognosis, with approximately 20%–40% of patients progressing to end-stage kidney disease within two decades of diagnosis. 1
Increasing evidence indicates that the dysregulation of mucosal immunity plays a central role in IgAN pathogenesis. IgA is predominantly produced by mucosa-associated lymphoid tissue (MALT), and aberrant mucosal immune responses are believed to contribute to the overproduction of galactose-deficient IgA1 (Gd-IgA1), a key pathogenic factor in IgAN. In this context, tonsillectomy has been proposed as a therapeutic option in selected patients, particularly those with recurrent tonsillitis; however, clinical responses remain variable. 2
The appendix is another component of the gut-associated lymphoid tissue (GALT) and contains abundant immune cells involved in mucosal IgA production. However, the clinical relevance of appendiceal inflammation in IgAN has not been systematically investigated. Herein, we describe an unusual clinical course of IgAN in a patient who achieved sustained remission following sequential tonsillectomy and appendectomy.
Case report
A female in her early 20s was admitted to the 900th Hospital of PLA, Fuzhou, China, in April 2016 with intermittent gross hematuria lasting 1 month, which occurred following an upper respiratory tract infection. She had no history of autoimmune disease, skin rash, arthralgia, edema, or hypertension. Physical examination revealed bilateral tonsillar hypertrophy (grade II), with no peripheral edema. Her blood pressure was 103/65 mmHg.
Initial laboratory evaluation demonstrated hematuria (3+), proteinuria (2+), and erythrocyturia (erythrocyte count: 395 cells/μL). Her urine protein-to-creatinine ratio (UPCR) was 1329.3 mg/g, serum creatinine level was 77.1 μmol/L, and serum albumin level was 41.2 g/L. Complement levels, antinuclear antibodies, anti-streptolysin O titers, and C-reactive protein were within the normal ranges. Renal ultrasonography did not reveal any structural abnormalities. The initial laboratory results are summarized in Table 1.
Laboratory parameters at admission.

Alb: albumin; ALT: alanine transaminase; ASO: anti-streptolysin O; AST: aspartate transaminase; BUN: blood urea nitrogen; Cr: creatinine; CRP: C-reactive protein; eGFR: estimated glomerular filtration rate; FBS: fasting blood sugar; Hb: hemoglobin; HbA1c: glycosylated hemoglobin; LDH: lactate dehydrogenase; LDL-C: low-density lipoprotein cholesterol; Plt: platelet count; RBC: red blood cell; TC: total cholesterol; TP: total protein; WBC: white blood cell; Ig: immunoglobulin; C3: complement C3; C4: complement C4.
A renal biopsy was performed in April 2016. Light microscopy revealed 34 glomeruli, with mild mesangial hypercellularity, focal segmental sclerosis, and focal capsular adhesions. No crescents were observed. Tubulointerstitial changes were mild. Immunofluorescence microscopy demonstrated granular IgA deposition, predominantly in the mesangium, with extension along the segments of the capillary walls, accompanied with IgG and IgM deposition. The pathological diagnosis was IgAN, Oxford classification M0E0S1T0 (2009 criteria) (Figure 1). 3 Supportive therapy with losartan potassium (50 mg daily) was initiated. No immunosuppressive agents were used during the treatment course. During follow-up, her serum creatinine levels remained stable (51.5–67.2 μmol/L), whereas urinary protein excretion and hematuria levels (indicating proteinuria and hematuria) fluctuated. The UPCR ranged from 386.2 to 678.9 mg/g, and urinary erythrocyte counts ranged from 102 to 553 cells/μL.

Renal histopathology and immunofluorescence findings in IgA nephropathy. (a) Periodic acid-Schiff (PAS) staining (original magnification 400×) demonstrates mild mesangial hyperplasia with focal capsular adhesions in the glomerulus; (b) periodic acid-silver methenamine (PASM)–Masson trichrome staining (original magnification 200×) shows tubulointerstitial alterations, characterized by tubular atrophy, epithelial cell swelling, and focal interstitial fibrosis with scattered inflammatory cell infiltrates. Interstitial fibrosis and tubular atrophy (IFTA) involve <25% of the cortical area, consistent with T0 classification. (c) Immunofluorescence microscopy (original magnification 400×) reveals granular IgA deposition predominantly in the mesangium, with extension along segments of the glomerular capillary walls. (d) Immunofluorescence staining for C3 (original magnification 400×) shows weak and focal staining without significant mesangial or capillary wall deposition.
In May 2018, the patient underwent bilateral tonsillectomy for recurrent tonsillitis, based on standard clinical indications, not as treatment for IgAN. Histopathological examination demonstrated chronic tonsillitis with lymphoid follicular hyperplasia and crypt abscess formation (Figure 2(a)). Following tonsillectomy, her hematuria improved substantially; however, proteinuria persisted, with UPCRs ranging from 340.5 to 628.2 mg/g.

Histopathological characteristics of chronic tonsillitis and appendicitis. (a) Chronic tonsillitis. The submitted tonsillar tissue is covered by hyperplastic squamous epithelium with preserved cellular polarity. Subepithelial lymphoid tissue demonstrates follicular hyperplasia with enlarged germinal centers. Some crypts are dilated and contain secretions. Scattered areas of degenerated muscle tissue and focal well-differentiated glands are observed. (b) Acute exacerbation of chronic appendicitis. Diffuse thickening of the appendiceal wall is noted, accompanied with fibrous tissue proliferation, marked acute and chronic inflammatory cell infiltration, and focal lymphoid hyperplasia. The inflammatory infiltrate consists mainly of lymphocytes, plasma cells, and neutrophils, with scattered eosinophils present.
In September 2022, the patient underwent laparoscopic appendectomy for acute exacerbation of chronic appendicitis. Histopathology revealed chronic inflammatory changes with neutrophilic infiltration and mucosal fibrosis (Figure 2(b)). One month after the appendectomy, urinalysis normalized, with complete resolution of proteinuria and sustained absence of hematuria, which had already improved prior to the appendectomy. Losartan was discontinued. During the subsequent follow-up, complete clinical remission was maintained, with UPCR values of 45.7–64.1 mg/g, erythrocyturia (erythrocyte count: 3–8 cells/μL), and stable serum creatinine levels (52.4–61.3 μmol/L). Detailed follow-up data have been presented in Figure 3.
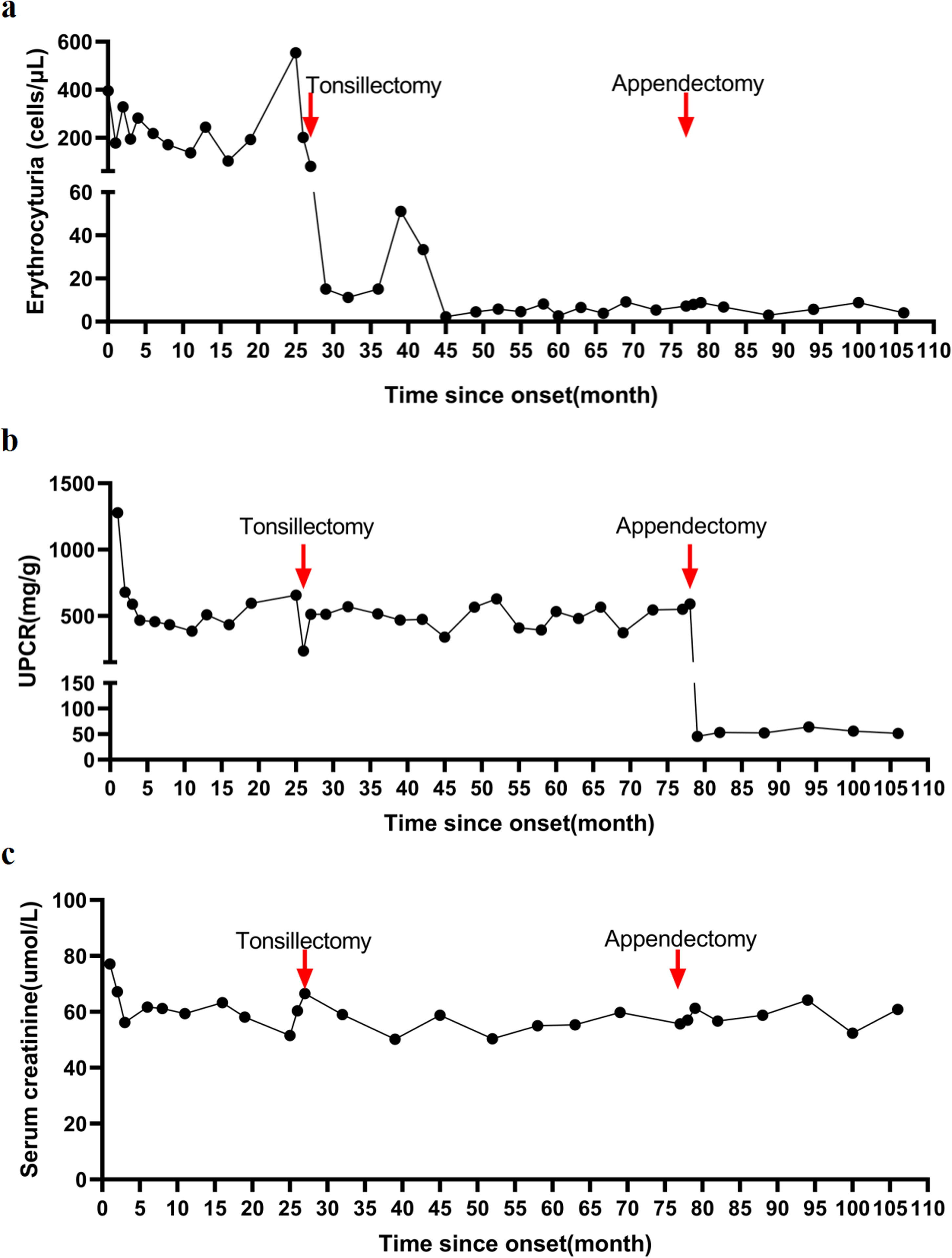
Long-term renal outcome following surgical interventions. (a) Tonsillectomy improved hematuria but not proteinuria; (b) appendectomy normalized proteinuria; (c) during the follow-up period, serum creatinine levels remained stable within the normal range.
The reporting of this case conforms to the Case Report (CARE) guidelines. 4
Discussion
IgAN is increasingly being recognized as a disease associated with dysregulated mucosal immune responses. According to the widely accepted multi-hit hypothesis, mucosal immune activation plays a central role in disease initiation and progression. 5 Tonsillar involvement has been extensively studied, and tonsillectomy has been associated with improvement in urinary abnormalities in selected patients; however, its long-term efficacy remains uncertain.6–8
The potential benefit of tonsillectomy in IgAN has been most consistently reported in East Asian populations, particularly in Japanese cohorts, whereas evidence in other ethnic groups remains limited and inconclusive. Therefore, the generalizability of this approach across different populations is uncertain.
In the present case, tonsillectomy was followed by a marked reduction in hematuria; however, proteinuria persisted, suggesting partial modulation of disease activity. Notably, complete clinical remission occurred only after appendectomy performed 4 years later for chronic appendicitis. The temporal relationship between appendectomy and disease remission is notable; however, causality cannot be inferred. Hematuria improved prior to appendectomy and remained stable thereafter, whereas proteinuria demonstrated a more marked reduction following the appendectomy. This discrepancy underscores the complexity of disease activity assessment in IgAN, wherein different clinical parameters may not change synchronously. Importantly, the temporal association observed in this case does not establish a causal relationship.
The appendix is a component of the GALT and contains abundant immune cells involved in mucosal immunity. MALTs, including the tonsils and appendix, are considered to participate in systemic immune responses.9,10 However, the extent to which these tissues influence the clinical course of IgAN remains unclear.
Certain important limitations must be acknowledged. Importantly, remission in the present case was primarily assessed based on clinical parameters, particularly the degree of proteinuria, without sequential histopathological evaluation or serial measurements of Gd-IgA1 and other immunological biomarkers. Therefore, the biological impact of appendectomy on disease activity remains speculative. This report describes a single patient, and spontaneous remission, long-term supportive therapy and relatively mild histopathological features may have contributed to the favorable outcome. Another limitation of this report is the lack of measurement of disease-specific biomarkers, such as Gd-IgA1, which may have provided additional insights into the underlying immunological changes. In addition, serial measurements of immunological markers were unavailable. Accordingly, this observation should be regarded as hypothesis-generating rather than confirmatory.
Conclusion
We report an unusual clinical course of IgAN in a patient who achieved sustained remission following sequential tonsillectomy and appendectomy. Although a causal relationship cannot be established, this case suggests an association between mucosal inflammation conditions and disease activity in selected patients. Further mechanistic and clinical studies are needed to clarify the role of extrarenal mucosal immune tissues in IgAN.
Footnotes
Acknowledgments
The authors used Deepseek to improve the clarity of the manuscript. The authors take full responsibility for the content.
Ethics declarations
Ethical approval was not required for this case report in accordance with institutional policies. Written informed consent to treatment was obtained from the patient as part of routine clinical care. Written informed consent for publication was obtained from the patient. All patient details have been deidentified to protect privacy.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by CY, MQ, YZ, and JC. The first draft of the manuscript was written by JC, and all authors provided their views on previous versions of the manuscript. All authors have read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the 900th Hospital of Joint Logistic Support Force Annual Hospital Research Plan (2020Z09, 2021MS14) and The Joint Logistics Medical High-Quality Specialty of the Joint Logistics Support Force (LQYZ-SZ).
The Joint Logistics Medical High-Quality Specialty of the Joint Logistics Support Force, 900th Hospital of Joint Logistic Support Force Annual Hospital Research Plan, (grant numbers: LQYZ-SZ, 2020Z09, and 2021MS14).
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.