
Abstract
Hepatic portal venous gas is an uncommon radiologic finding that has been rarely reported in neurocritical care settings. This article presents two clinically instructive case reports of severe neurological disorders complicated by HPVG. Both patients presented with abdominal distension, absent bowel sounds, and septic shock following neurological surgery, and abdominal imaging confirmed the presence of hepatic portal venous gas. These cases provide valuable clinical references for the abdominal management of patients in neurocritical care.
Keywords
Case 1
Neurological findings
A female aged approximately 40 years was admitted to the Second Hospital of Lanzhou University in August 2024 because of a space-occupying lesion in the right cerebellopontine angle region (Figure 1). The patient had no significant past medical history, family history, or genetic disorders. She subsequently underwent craniotomy for tumor resection (Figure 2).

(a) Cranial computed tomography (CT) axial. A mass lesion is located in the right cerebellopontine angle (CPA), presenting as a mound-like morphology with a broad base attached to the dura mater and well-defined borders (red arrow). Significant mass effect is observed. The adjacent pons, right middle cerebellar peduncle (MCP), and fourth ventricle are compressed and deformed. (b) Volume-rendered 3D CT angiography of the brain. The right internal carotid artery (RICA; blue arrow), basilar artery (BA; red arrow), and right posterior cerebral artery (RPCA; yellow arrow) demonstrate compressive displacement. The remaining intracranial vessels are well opacified. Magnetic resonance imaging (MRI), axial, T2-weighted phase (T2WI). (c) A space-occupying lesion is seen in the right CPA, demonstrating slightly hyperintense T2 signal (red arrow). The left trigeminal nerve (orange arrow) and left Meckel cave (blue arrow) are clearly visualized. The course of the right trigeminal nerve and right Meckel cave is encased by the tumor and cannot be visualized. (d) The right CN VII (red arrows) and cranial nerve (CN) VIII (blue arrows) demonstrate a normal course. (e) Contrast-enhanced T1-weighted image (CE-T1WI). The anterior clinoid process (red arrow) shows intact bone structure without obvious destruction.
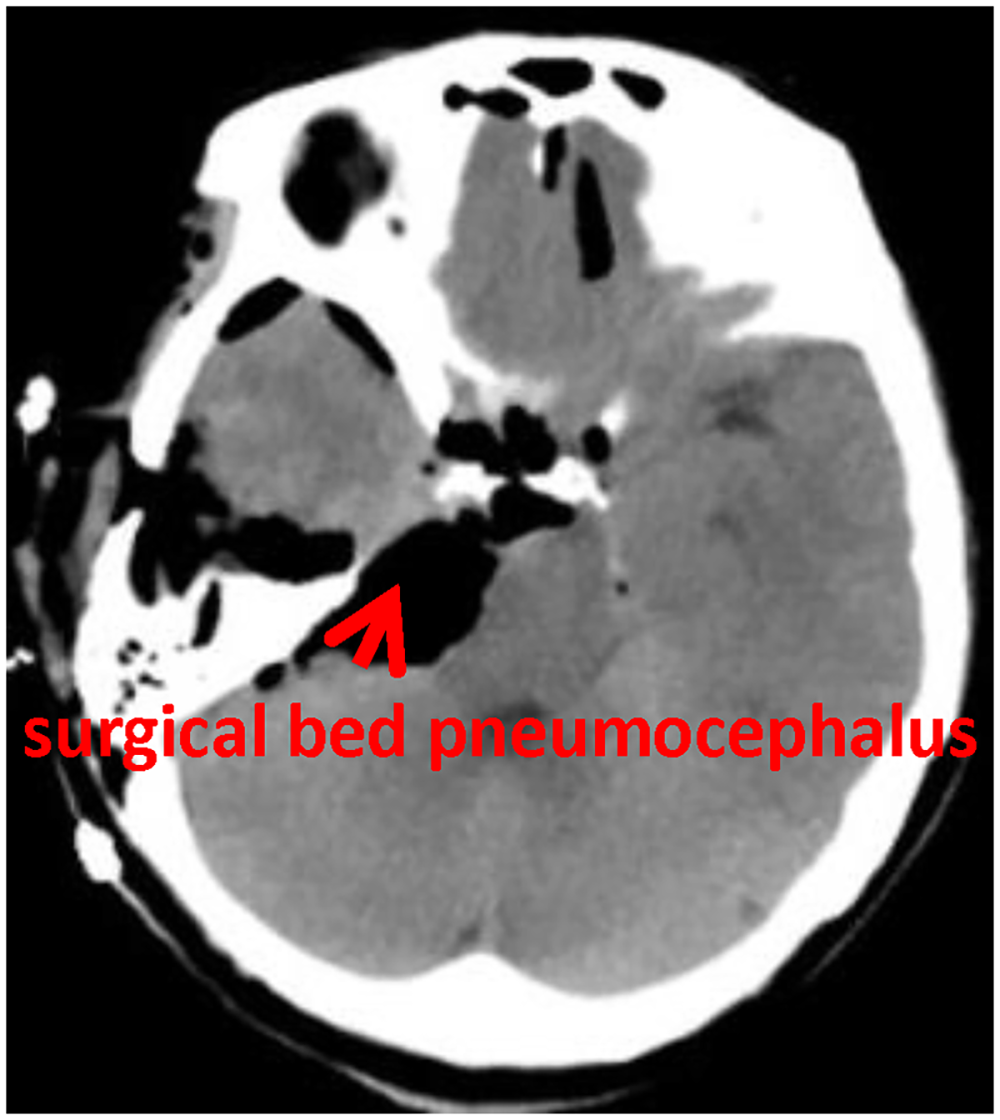
Cranial computed tomography (CT), axial. The surgical region demonstrates clear anatomy with improved mass effect compared with the preoperative tumor. Compression and displacement of the pons and fourth ventricle have resolved, and the cerebellopontine angle cistern is re-visualized. Pneumocephalus is noted in the surgical bed (red arrow), with no obvious hemorrhage.
Abdominal manifestations and management
After the procedure, daily measures were implemented to maintain regular bowel movements. On postoperative day 7, the patient developed abdominal distension and weakened bowel sounds. However, no significant abnormalities were identified on abdominal computed tomography (CT) examination (Figure 3). Following enema administration with Kaiselu, 1000 mL of thin watery stool was passed, resulting in partial relief of the abdominal distension. On postoperative day 8, the abdominal distension worsened further. Despite treatment measures, including fasting, promotion of gastrointestinal peristalsis, traditional Chinese medicine enemas, and acupuncture, the abdominal distension persisted. Bowel sounds disappeared and were accompanied by diarrhea. The intra-abdominal pressure was 22 mmHg, and blood pressure decreased. Laboratory tests revealed a white blood cell (WBC) count of 24.77 × 109/L, neutrophil percentage of 89.00%, and procalcitonon (PCT) level of 0.583 ng/mL. Septic shock was suspected, and empirical anti-infective therapy with imipenem-cilastatin (1 g, q8h) combined with linezolid (0.6 g, q12h) was initiated. In addition, fluid replacement and vasoactive agents were administered to maintain blood pressure. Abdominal CT (Figure 4) demonstrated intestinal obstruction, pneumatosis intestinalis, and extensive gas within the hepatic portal venous system. Septic shock secondary to intestinal bacterial translocation into the bloodstream was considered the most likely diagnosis. The patient received the aforementioned anti-infective and supportive treatments for 5 days; however, her condition deteriorated rapidly, and blood pressure became increasingly difficult to maintain despite vasoactive support and fluid replacement. After being informed of the condition, the family elected to withdraw treatment, and the patient was subsequently discharged.
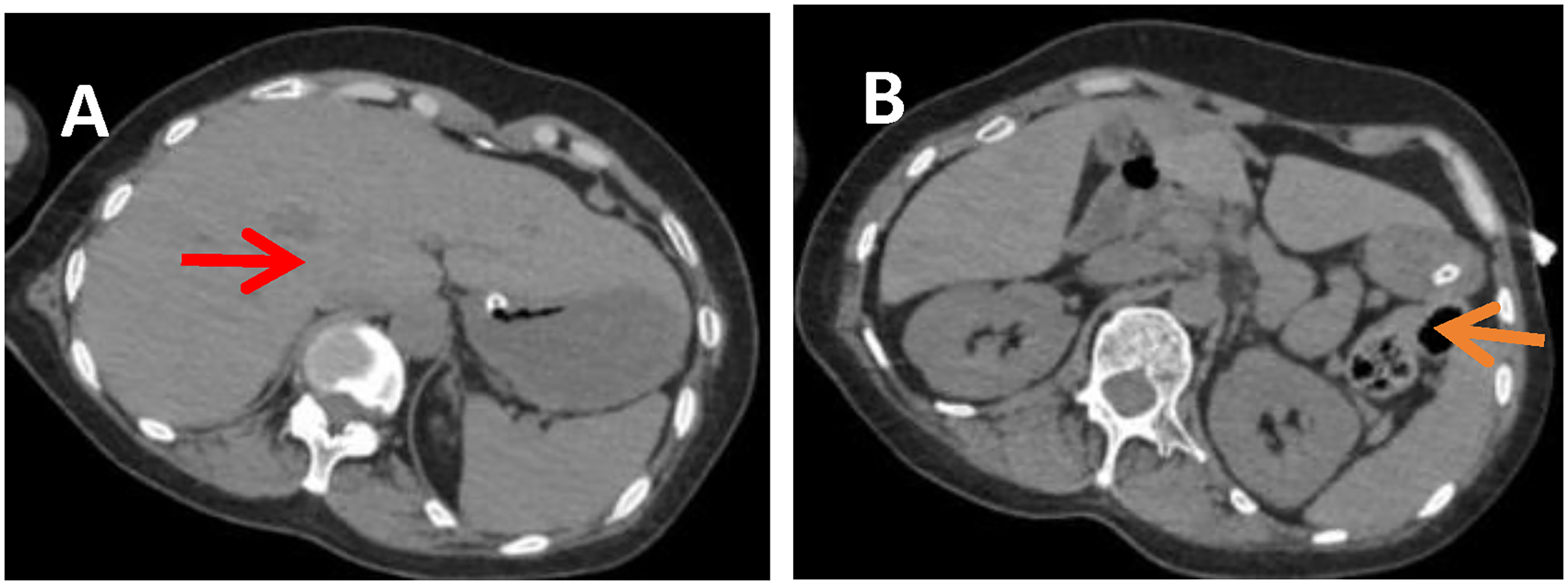
Abdomen computed tomography, axial. No specific signs of severe intestinal obstruction are identified. No portal venous gas is seen in the liver (red arrow, image A), and no dilatation of the bowel loops is noted (orange arrow, image B).

Abdomen computed tomography (CT), axial. (a) Upper abdominal axial CT (at the level of the porta hepatis): Extensive portal venous gas is present in the liver (red arrow). Gas is distributed along the portal venous system, demonstrating characteristic branching low
Case 2
Neurological findings
A female in her 50s was admitted to the Second Hospital of Lanzhou University in November 2024 because of diffuse subarachnoid hemorrhage secondary to a cerebral aneurysm (Figure 5). The patient had no remarkable past medical, family, or genetic history. Following admission, she underwent aneurysm clipping, hematoma evacuation, and decompressive craniectomy (Figure 6). Postoperatively, her intracranial condition remained relatively stable; however, she remained comatose with a Glasgow Coma Scale (GCS) score of E1V1M1.

Cranial computed tomography, axial (Case 2). (a) Intracerebral hemorrhage in the right frontal lobe with intraventricular rupture (red arrow), diffuse subarachnoid hemorrhage (orange arrow), and a right subdural hematoma beneath the cranial plate (blue arrow) are identified. The right lateral ventricle is compressed and narrowed, with leftward midline shift and evidence of cerebral herniation.

Cranial computed tomography, axial. The right lateral ventricle remains narrowed, and the midline shift is improved compared with the previous examination. A partial bony defect of the right temporoparietal bone is present (red arrow). A patchy high-density shadow is noted in the right frontotemporal lobe (orange arrow), with metallic clip artifacts at the right middle cerebral artery (green arrow) and basilar artery (blue arrow).
Abdominal manifestations and management
On postoperative day 3, the patient developed abdominal distension and weakened bowel sounds (1/min). An abdominal CT scan revealed intestinal gas accumulation and dilatation (Figure 7). Metoclopramide (10 mg, q8 h, ivgtt) was continued to improve gastrointestinal motility. A Kaiselu enema and daily acupuncture at traditional Chinese medicine acupoints were performed to maintain a daily bowel movement volume of approximately 400–700 mL, and the abdominal distension was partially relieved. However, on postoperative day 6, the abdominal distension recurred and worsened. No bowel sounds were heard; the intra-abdominal pressure was 17 mmHg, blood pressure decreased to 85/57 mmHg, and body temperature increased to 38.9°C. Laboratory tests revealed a WBC count of 19.13 × 109/L, neutrophil percentage of 91.10%, PCT of 5.590 ng/mL, lactate of 7.3 mmol/L, K+ of 4.0 mmol/L, and albumin of 34.2 g/L. Septic shock was highly suspected. Vasoactive drugs were infused via a pump to correct shock, and anti-infective treatment with vancomycin (1 g, q8h) combined with imipenem-cilastatin (1 g, q8h) was initiated. Abdominal color Doppler ultrasonography showed heterogeneous echogenicity of the liver parenchyma, with small amount of gas-like hyperechoic signals. The intestinal tract was dilated, with gas and fluid accumulation, particularly in the colon. The colonic wall demonstrated a “key-board sign” (Figure 8), intestinal peristalsis was weakened, and the intestinal contents exhibited reciprocating flow. Severe gas accumulation was observed in the upper abdomen, and the superior mesenteric artery and vein could not be visualized. Abdominal CT demonstrated gas-density shadows within the portal vein branches and superior mesenteric vein. The small intestine and colon were dilated, with multiple gas-density shadows in the intestinal wall. Treatment measures, including fasting, parenteral nutritional support, gastrointestinal decompression, placement of an intestinal obstruction catheter, traditional Chinese medicine enema, acupuncture at traditional Chinese medicine acupoints, and hot fennel compresses, were implemented to promote gastrointestinal peristalsis. Concurrently, after consultation with the general surgery department, intestinal obstruction and possible intestinal necrosis were considered, and surgical treatment was recommended. The family members refused surgery and chose to continue conservative treatment. After 4 days of treatment, vasoactive drugs were gradually tapered. Repeat laboratory testing showed a WBC count of 10.42 × 109/L, neutrophil percentage of 93.90%, and PCT level of 1.710 ng/mL. Physical examination revealed improvement in abdominal distension and the return of bowel sounds (2/min). Repeat abdominal CT demonstrated absorption of pneumatosis intestinalis and portal/superior mesenteric venous gas compared with the previous scan. Owing to severe craniocerebral injury, the patient's level of consciousness did not improve (Figure 9). Subsequently, the family elected to withdraw treatment, and the patient was discharged.

Abdomen computed tomography, axial. (a) No obvious portal venous gas is identified. (b) Multiple intestinal loops are distributed throughout the abdominal cavity, with scattered gas-density opacities in the bowel lumen (red arrow). No marked or diffuse bowel dilatation is observed, and there is no “giant sacculated” obstructive dilatation pattern. Bowel wall edema (no low-density halo), bowel wall thickening (no high-density halo), and intramural gas (pneumatosis intestinalis) are absent.

Abdomen computed tomography, axial. (a) Upper abdomen. Gas-density opacities are present within the portal vein branches (red arrow). (b) Lower abdomen. Diffuse bowel dilatation and gas accumulation throughout the entire abdominal bowel loops are observed, demonstrating continuous tubular low-density opacities. The intestinal lumen diameter is significantly enlarged (red arrow), and air-fluid levels are present (blue arrow).

Abdomen computed tomography (CT), axial. (a) Upper abdomen. The gas-density opacities within the portal vein have resolved. (b) Lower abdomen. Bowel dilatation has decreased compared with the previous examination, with scattered air-fluid levels remaining (red arrow).
Discussion
The etiology of intestinal ischemia following brain injury is not attributable to a single factor but rather to intestinal microcirculatory failure caused by multiple neurological, endocrine, inflammatory, and hemodynamic factors, with inflammation and bacterial translocation serving as amplifiers. We hypothesize the mechanisms as follows.
Gut-brain axis (GBA)
1
dysfunction. GBA refers to a complex bidirectional communication system between the brain and the gut. It comprises the gastrointestinal tract,
2
central nervous system (CNS), autonomic nervous system (ANS), and enteric nervous system (ENS), all of which interact and influence one another.3,4 Following brain injury, the hypothalamic–pituitary–adrenal axis becomes dysregulated, leading to a massive release of catecholamines (epinephrine and norepinephrine). This causes intense systemic vasoconstriction, with the splanchnic vessels (mesenteric arteries) being particularly sensitive to catecholamines. The resulting marked constriction or even spasm of the mesenteric arteries leads to a sharp reduction in intestinal blood flow, which may contribute to nonocclusive mesenteric ischemia (NOMI), a frequent and important potential cause of intestinal ischemia following severe brain injury. Simultaneously, traumatic brain injury triggers a massive release of tissue factors,
5
activating the extrinsic coagulation pathway and also damaging endothelial cells, resulting in a systemic hypercoagulable state known as “trauma-induced hypercoagulation.” Consequently, microthrombi form within the mesenteric arterioles or small arteries, which can directly occlude the vessels and cause arterial occlusive mesenteric ischemia.6,7 Mechanical ventilation-induced intra-abdominal hypertension. Mechanical ventilation increases intra-abdominal pressure, impairing intestinal perfusion and function.
8
Arterial occlusive mesenteric ischemia (AOMI). AOMI is also one of the causes of hepatic portal venous gas (HPVG). The most common etiology is cardiogenic emboli (atrial fibrillation, atrial flutter, and left atrial thrombus detachment), followed by detached atherosclerotic plaques from the thoracic/abdominal aorta and fragments from aortic dissection. Other contributing factors include underlying conditions such as systemic atherosclerosis, hypertension, hyperlipidemia, and diabetes mellitus, which result in severe pre-existing mesenteric arterial atherosclerosis, luminal stenosis, rough intima, and reduced blood flow. In the setting of brain injury, aggressive dehydration therapy to reduce intracranial pressure causes hemodynamic fluctuations, further slowing splanchnic blood flow. Additionally, prolonged immobilization and a hypercoagulable state may lead to in situ thrombosis, resulting in complete luminal occlusion. For definitive diagnosis, abdominal computed tomography angiography (CTA) is required.
The intestine is extremely sensitive to ischemia. When blood supply is reduced for more than 15–20 min, intestinal mucosal epithelial cells begin to undergo necrosis and sloughing, resulting in a loss of mucosal barrier function. Anaerobic bacteria within the necrotic intestinal wall (such as Escherichia coli and Clostridium perfringens) proliferate extensively and produce gases including hydrogen, carbon dioxide, and methane through fermentation. When intestinal wall ischemia progresses to transmural necrosis, gas in the submucosa or subserosa can penetrate the thin venous wall (where venous pressure is much lower than arterial pressure) and enter the mesenteric veins. The gas subsequently travels through the mesenteric veins into the main portal vein, manifesting as HPVG on imaging.
Neurocritical patients with impaired consciousness who require endotracheal intubation and continuous sedation-analgesia for neuroprotection are often unable to verbalize discomfort or cooperate with abdominal examinations 9 (e.g. assessment of tenderness/rebound tenderness). The diagnostic challenge in these two cases was that severe neurological deficits masked abdominal symptoms, making it challenging to identify abdominal complications at an early stage. HPVG is now recognized not as a specific disease entity but as a rare condition in patients with acute abdomen and high mortality. Clinically, abdominal abnormalities may initially present as abdominal distension, diarrhea, or constipation. 10 In clinical practice, attention should be paid to abdominal girth measurements and bowel-sound documentation. When abdominal abnormalities occur, 11 such as persistent diarrhea or refractory abdominal distension (>48 h), imaging studies including ultrasonography and CT are critical for detecting complications and guiding timely intervention. 12 In Case 2, repeated ultrasonography and CT examinations following abnormal abdominal findings confirmed the presence of intestinal ischemia. For acute mesenteric ischemia (AMI), whether arterial occlusive or nonocclusive, selective mesenteric angiography remains the “gold standard” for diagnosis because it directly visualizes the morphology of the affected vessels. Unfortunately, contrast-enhanced CT (including CTA and delayed-phase imaging) was not performed because of hemodynamic instability and the patient’s critical condition at the time of imaging. The patient’s vital signs deteriorated rapidly, and the clinical team considered the risks associated with transport and intravenous contrast administration for multiphasic CT to be unacceptably high. Consequently, only noncontrast CT images were obtained.
The management of HPVG generally follows two approaches: conservative treatment or surgical intervention. 13 Reliable guidelines for individual patients have not yet been established. The choice depends primarily on the patient's overall condition, laboratory findings, and, most importantly, imaging findings. HPVG itself is not an indication for emergency surgery. If the patient is clinically stable and there is no clear imaging evidence of intestinal ischemia or necrosis, surgery should generally be avoided. Antibiotics and gastrointestinal decompression are routine conservative therapies. Previous studies have reported that some patients with HPVG do not have intestinal necrosis and can be successfully treated with medication. 14 If CT demonstrates signs of intestinal perforation and/or severe ischemia/necrosis, including free intraperitoneal air, absent contrast enhancement of the intestinal wall, intestinal pneumatosis, or mesenteric arterial embolism, emergency surgery should be considered.
Limitations of the study
Early ischemic changes are best evaluated with contrast-enhanced multiphasic CT, and the absence of such imaging limited our ability to assess the degree of bowel wall enhancement and estimate the timing of ischemia. If the patient's condition had permitted, CTA would have been the preferred diagnostic modality. Furthermore, the patient did not undergo surgical treatment; therefore, histopathological findings were unavailable, preventing definitive differentiation of arterial occlusive intestinal ischemia. We acknowledge that, in Case 1, extensive tumor resection was performed in a region rich in small and fragile vessels; therefore, postoperative hemorrhage cannot be completely excluded as being related to surgical technical factors. However, this case should not be interpreted as reflecting suboptimal surgical management. A more conservative resection might have reduced the risk of bleeding but would likely have compromised oncological outcomes. The neurosurgical team conducted a multidisciplinary preoperative discussion and proceeded with resection after careful assessment of the risks and benefits.
Conclusion
HPVG has been recognized as a serious condition associated with high mortality, with reported mortality rates ranging from 29% to 56%. In clinical practice, attention should be paid to abdominal management. If any abdominal abnormalities are identified, emergency ultrasonography and CT should be performed promptly. Early intervention to improve gastrointestinal dysfunction may prevent progression to HPVG. 15
Footnotes
Acknowledgments
AI tools were used for the language improvement of this manuscript, and all authors bear sole responsibility for the scientific content of the work. The manuscript has been critically revised and edited for English language by a professional medical English editor with expertise in clinical case reports.
Ethical statement and informed consent
The Ethics Committee of The Second Hospital of Lanzhou University approved the study. The patient provided written informed consent for publication of this case and the accompanying images. The ethical approval number was 2025A-415. The reporting of this study conforms to CARE guidelines.
Informed consent statement
Written informed consent for medical treatment was obtained from the patients’ legal representatives prior to all clinical interventions; separate written informed consent for the publication of this case report and accompanying imaging materials was also obtained from them. All patient details have been deidentified.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Zhipeng Shen. The first draft of the manuscript was written by Shanshan Li, and Yingjie Zhang reviewed the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data availability is not applicable for this case report. All relevant data are included in the article.