
Abstract
Spinal extradural meningeal cysts are rare spinal lesions, and the optimal surgical strategy remains debated, particularly regarding the relative importance of complete cyst wall excision and closure of the dural communication. We retrospectively reviewed 10 patients (5 male and 5 female; mean age, 38.5 years) who underwent surgical treatment for Nabors Type IA spinal extradural meningeal cysts at a single institution between 1987 and 2023. The median symptom duration was 5.5 months. All lesions showed cerebrospinal fluid–equivalent signal intensity on magnetic resonance imaging. Surgical approaches included total or subtotal laminectomy, hemilaminectomy, and osteoplastic laminotomy. The mean clinical follow-up period was 121.6 months. Nine patients underwent partial cyst wall resection or fenestration with primary dural defect closure; among the seven patients in this group with available postoperative radiological follow-up, no radiological recurrence was observed. The single patient in whom primary dural closure was not achieved showed a persistent residual or recurrent cystic lesion on follow-up imaging but remained clinically improved. No neurological complications were observed. These findings suggest that identifying and closing the dural communication may be an important component of durable spinal extradural meningeal cyst management, whereas complete cyst wall excision may not always be necessary. Because this was a small retrospective case series with incomplete imaging follow-up in some patients, these findings should be interpreted as supportive clinical observations rather than definitive evidence of causality.
Keywords
Introduction
Spinal extradural meningeal cysts (SEMCs) are rare lesions, accounting for approximately 1% of all spinal tumors. 1 Although these lesions are sometimes known as extradural arachnoid cysts, Nabors et al. classified extradural meningeal cysts without spinal nerve root fibers as Type IA spinal meningeal cysts.1,2 Multiple mechanisms have been proposed for their development and enlargement, including congenital factors, secretory activity of the cyst wall, osmotic gradients between the subarachnoid space and the cyst, pulsatile cerebrospinal fluid (CSF) dynamics, and a valve-like mechanism.3–5 Among these mechanisms, the check-valve or ball-valve concept is widely accepted because it explains progressive cyst expansion and subsequent neural compression. 6
Historically, surgical treatment often involved extensive exposure and attempted complete cyst excision. More recent pathophysiological and operative observations have shifted attention toward the dural communication between the subarachnoid space and the extradural cyst. If the communication persists, CSF inflow may continue despite partial removal of the cyst wall. In contrast, durable interruption of this communication may permit less extensive surgery in selected patients.
In this retrospective case series, we reviewed 10 surgically treated patients with Type IA SEMCs at our institution. We aimed to describe long-term clinical and radiological outcomes after a dural defect-oriented surgical strategy and to clarify the practical role and limitations of targeted dural repair in the management of these rare lesions.
This manuscript has not been posted as a preprint.
Materials and methods
Study design and patient selection
We retrospectively reviewed paper-based medical records from 1987 to 2012 and electronic medical records from the K-health clinical data warehouse from 2013 to 2023 to identify surgically treated patients diagnosed with spinal cystic lesions. Spinal meningeal and arachnoid cysts were screened, whereas syringomyelia, cystic tumors, synovial cysts, ganglion cysts, sacral cysts, and intradural cysts were excluded. Demographic characteristics, past medical history, clinical presentation, radiological findings, operative records, intraoperative images, pathological results, and follow-up data were reviewed.
A total of 28 surgically treated patients were initially identified. Patients with Nabors Type IB, II, or III cysts were excluded because sacral, perineural, and intradural cysts have distinct anatomical and pathophysiological features and require different treatment strategies. 1 The final cohort comprised 10 patients with Nabors Type IA SEMCs.
Ethics, reporting guideline, and patient deidentification
The study protocol was approved by the Institutional Review Board of Chonnam National University Hospital, Gwangju, Republic of Korea (IRB No. CNUH-2023-398; Approval Date: December 2023). The requirement for written informed consent for retrospective chart review was waived by the Institutional Review Board where applicable. All patients provided written informed consent for surgical treatment as part of routine institutional clinical practice. The reporting of the case illustrations conforms to the Case Report (CARE) guidelines (completed CARE checklist is uploaded as research data). 7 All patient details were deidentified; individual ages were reported as age ranges, and calendar dates were presented by month and year only.
Radiological evaluation and outcome definitions
All cystic lesions were isointense to CSF on both T1- and T2-weighted magnetic resonance imaging (MRI). MRI and computed tomography (CT) were used to evaluate lesion extent, bony remodeling, foraminal widening, and suspected dural communication. CT myelography was performed in one patient. In two patients, a focal signal void on T2-weighted MRI provided an additional clue to the location of the dural defect.
Clinical follow-up was defined as the final documented outpatient or inpatient assessment. Postoperative radiological follow-up was defined as the availability of postoperative MRI or CT sufficient to assess residual or recurrent cystic lesions. Because the study covered a long period, postoperative imaging was not uniformly available in all patients. Radiological recurrence was defined as the reappearance or enlargement of a cystic lesion after postoperative reduction or disappearance. A cystic cavity that persisted without interval enlargement was described as a persistent residual lesion rather than unequivocal recurrence.
Surgical treatment
Surgical intervention was indicated for symptomatic SEMCs associated with spinal cord or nerve root compression on MRI. The surgical approach, including total laminectomy, subtotal laminectomy, hemilaminectomy, or osteoplastic laminotomy, was selected according to the presumed location of the dural defect, the laterality of the lesion, the number of involved vertebral levels, and the surgical practice at the time of treatment.8,9 Earlier cases were generally managed with more extensive exposure, whereas more recent cases favored shorter-segment or reconstructive approaches when technically feasible.
After laminectomy or laminotomy, the dorsal wall of the SEMC was typically identified as a thin, fragile, and transparent membrane containing CSF-like fluid. After opening or partially resecting the dorsal wall, the inner cyst membrane and the dural sac were inspected. Particular attention was paid to the dural sleeve around the nerve rootlets, where the communicating defect was most often encountered. When herniated rootlets were visible through the defect, they were gently reduced into the dural sac. The dural defect was then closed primarily, usually with 6–0 silk sutures, and cessation of CSF flow was confirmed intraoperatively. Complete excision of the entire cyst wall was not considered mandatory; instead, partial cyst wall resection or fenestration was performed to expose the dural communication and decompress the neural elements.
Histopathological examination, including immunohistochemical staining when available, confirmed the diagnosis of a meningeal or arachnoid cyst in all patients. Clinical follow-up was generally performed every 6 months during the first postoperative year and annually thereafter when possible. Radiological follow-up was performed according to clinical need and institutional practice during the relevant treatment period.
Results
The cohort consisted of 5 male and 5 female patients, with a mean age of 38.5 years (range, 16–76 years). The median duration of symptoms before surgery was 5.5 months (range, 0.3–48 months). Clinical presentations included lower back pain with lower-limb radiating pain in six patients and lower-limb motor weakness or gait disturbance in two patients. One patient had preoperative neurological deterioration. Six patients had a possible precipitating or associated history, including trauma, heavy load, acupuncture, or spinal blockade before symptom onset. The clinical characteristics of the 10 patients are summarized in Table 1.
Clinical characteristics of patients with spinal extradural meningeal cysts.
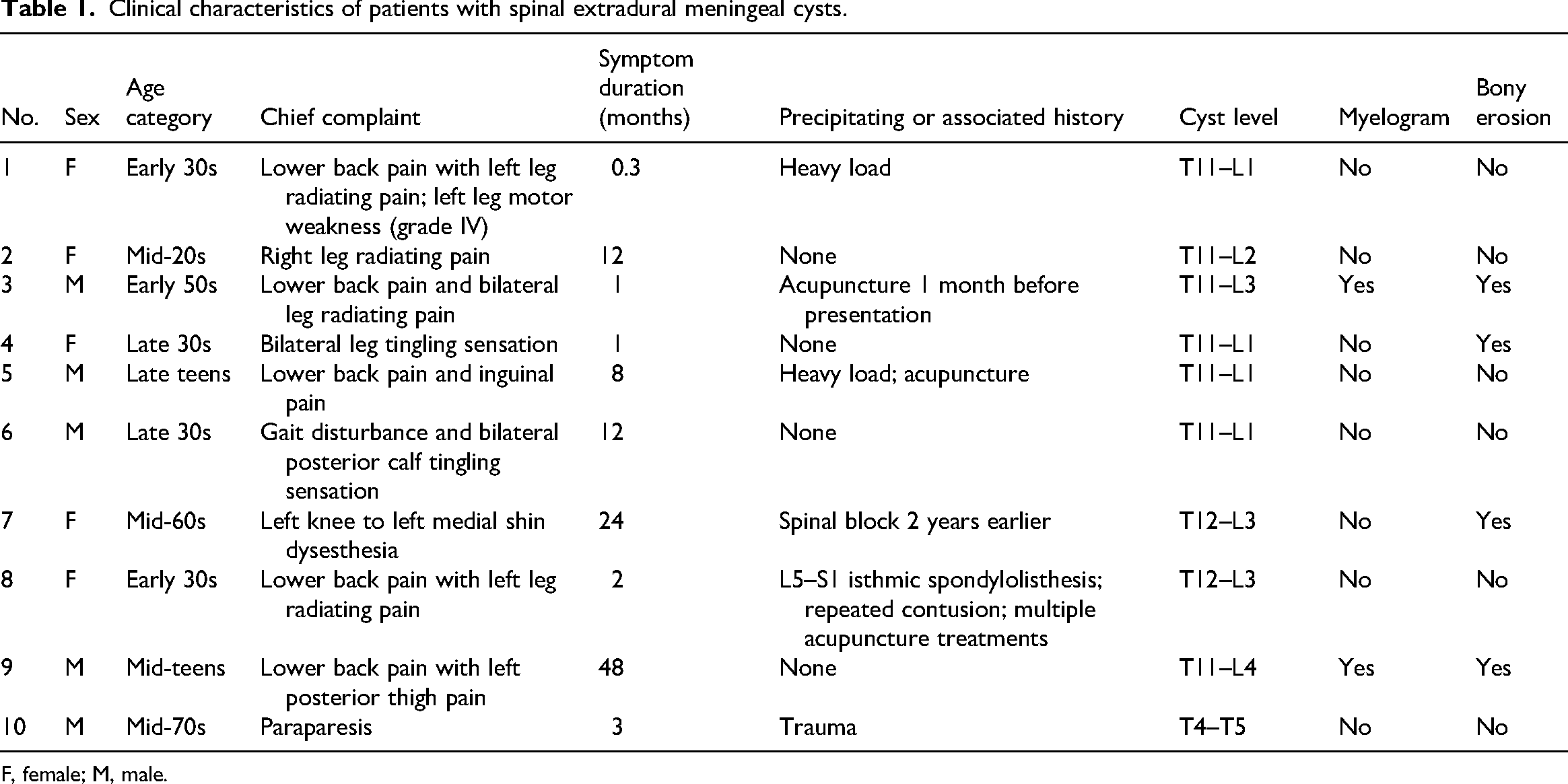
F, female; M, male.
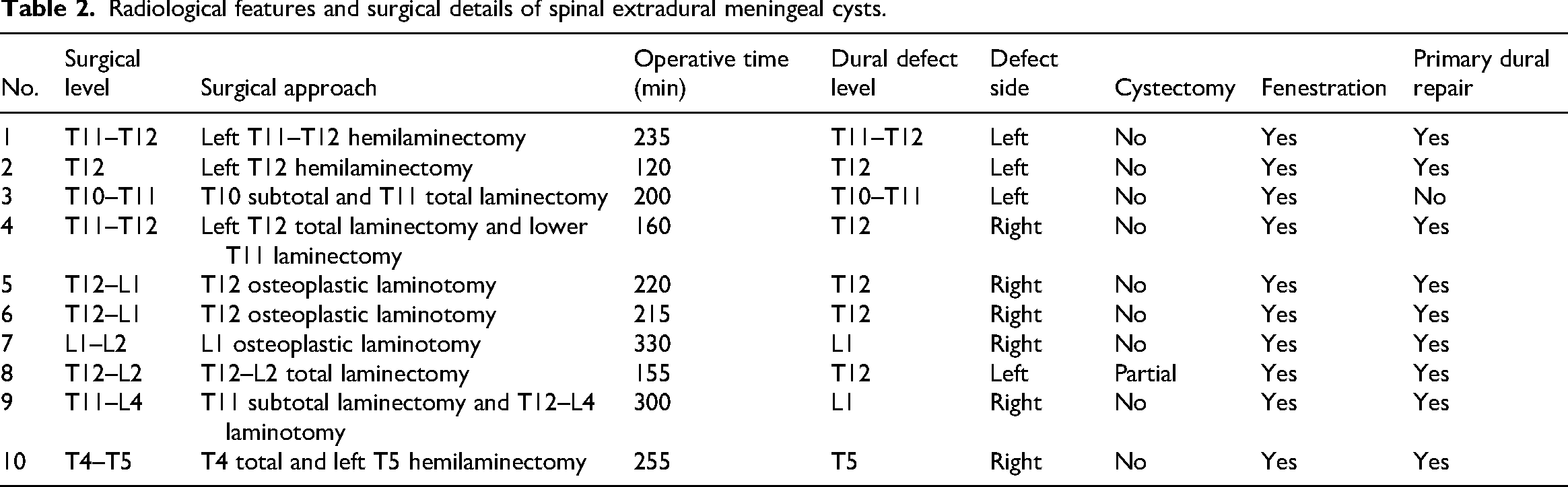
Eight of the 10 cysts were located at the thoracolumbar junction, 1 was located in the upper lumbar region, and 1 was located in the upper thoracic region. The most commonly involved levels were T12 and L1. The mean length of cyst involvement was 3.5 vertebral segments (range, 2–7 segments). The mean number of surgically exposed laminar levels was 1.6 (range, 1–3 levels), excluding the extent of laminotomy used for exposure in one long-segment case. Surgical approaches included total laminectomy in four patients, subtotal laminectomy in one patient, short-segment hemilaminectomy in two patients, and osteoplastic laminotomy in three patients (Tables 2 and 3).
Radiological features and surgical details of spinal extradural meningeal cysts.
Clinical and radiological outcomes of spinal extradural meningeal cysts.
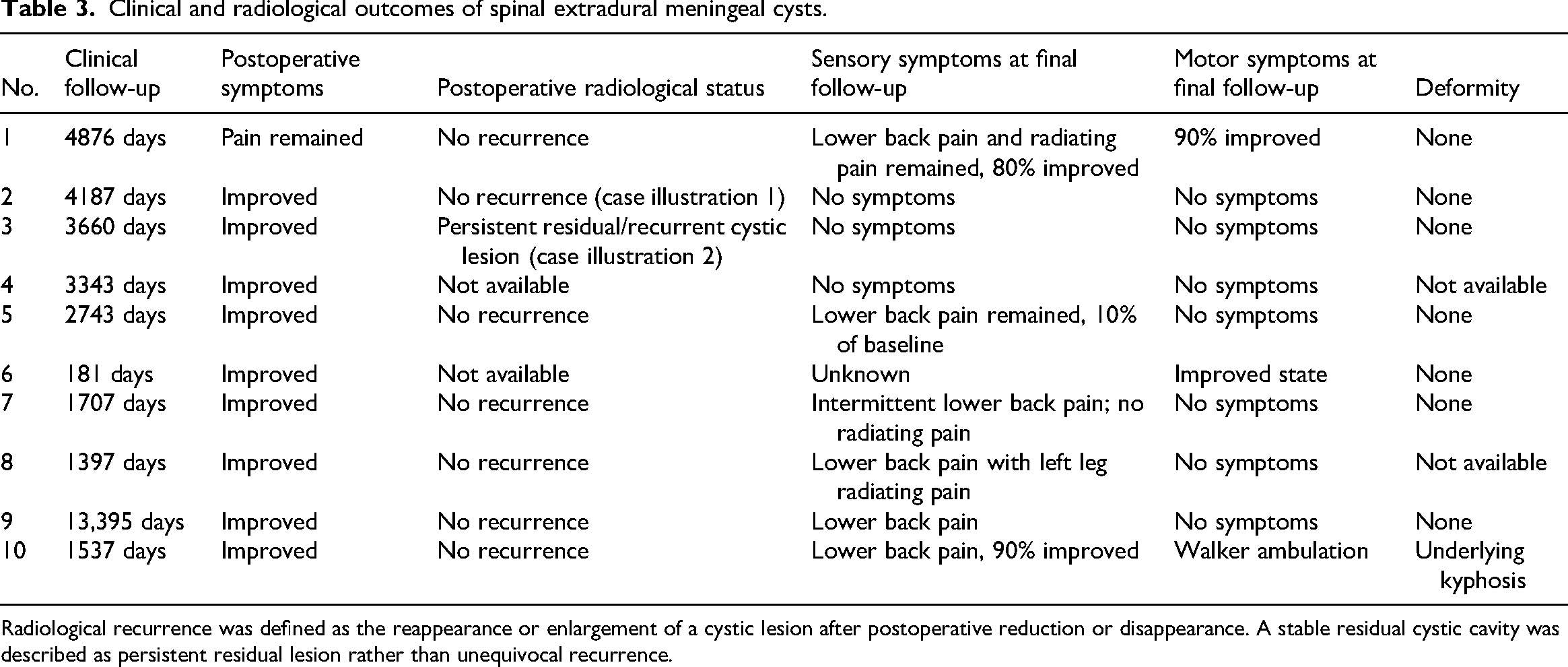
Radiological recurrence was defined as the reappearance or enlargement of a cystic lesion after postoperative reduction or disappearance. A stable residual cystic cavity was described as persistent residual lesion rather than unequivocal recurrence.
CT myelography was performed preoperatively in one patient but did not precisely localize the dural defect. The locations of dural defects were variable and did not consistently correspond to the most prominent topographical features of the cyst, including foraminal widening. Bony scalloping or erosion was observed in four patients, and the dural defect was located at the site of bony change in two of these patients. T2-weighted MRI showed focal signal voids in two patients, and these findings correctly suggested the intraoperative location of the dural defect.
The mean clinical follow-up period was 121.6 months (approximately 10.1 years). Clinical follow-up was available for all 10 patients, and all patients showed symptomatic improvement at the final follow-up. No postoperative neurological complications were observed. Postoperative radiological follow-up adequate for assessment of cyst recurrence or persistence was available in eight patients. Among the seven patients who underwent primary dural repair and had postoperative radiological follow-up, no radiological recurrence was observed. In the single patient in whom primary dural closure was not achieved, follow-up MRI showed a persistent residual or recurrent cystic lesion without symptomatic worsening.
Case illustrations
Case illustration 1
In July 2012, a woman in her mid-20s was admitted to this institution with progressive back pain and bilateral buttock pain accompanied by severe shooting pain radiating to the anterior aspect of the ankle. The pain had no clear postural variation or specific aggravating factors, but the clinical course fluctuated, with periods of worsening and improvement. There was no history of spinal injection or significant trauma preceding the pain. Preoperative neurological examination showed no significant lower-extremity motor weakness.
Lumbar spine CT demonstrated spinal canal widening and bony remodeling at the T11–L1 level (Figure 1(a)). Lumbar MRI revealed a dorsally located extradural cystic lesion displacing the thecal sac ventrally at T11–L1. The cyst was septated into two compartments, and the fluid showed signal intensity identical to CSF on both T1- and T2-weighted images (Figure 1(b)). A focal signal void on T2-weighted MRI was observed at the left T12–L1 intervertebral foramen (Figure 1(c), yellow arrow), suggesting a communicating dural defect.
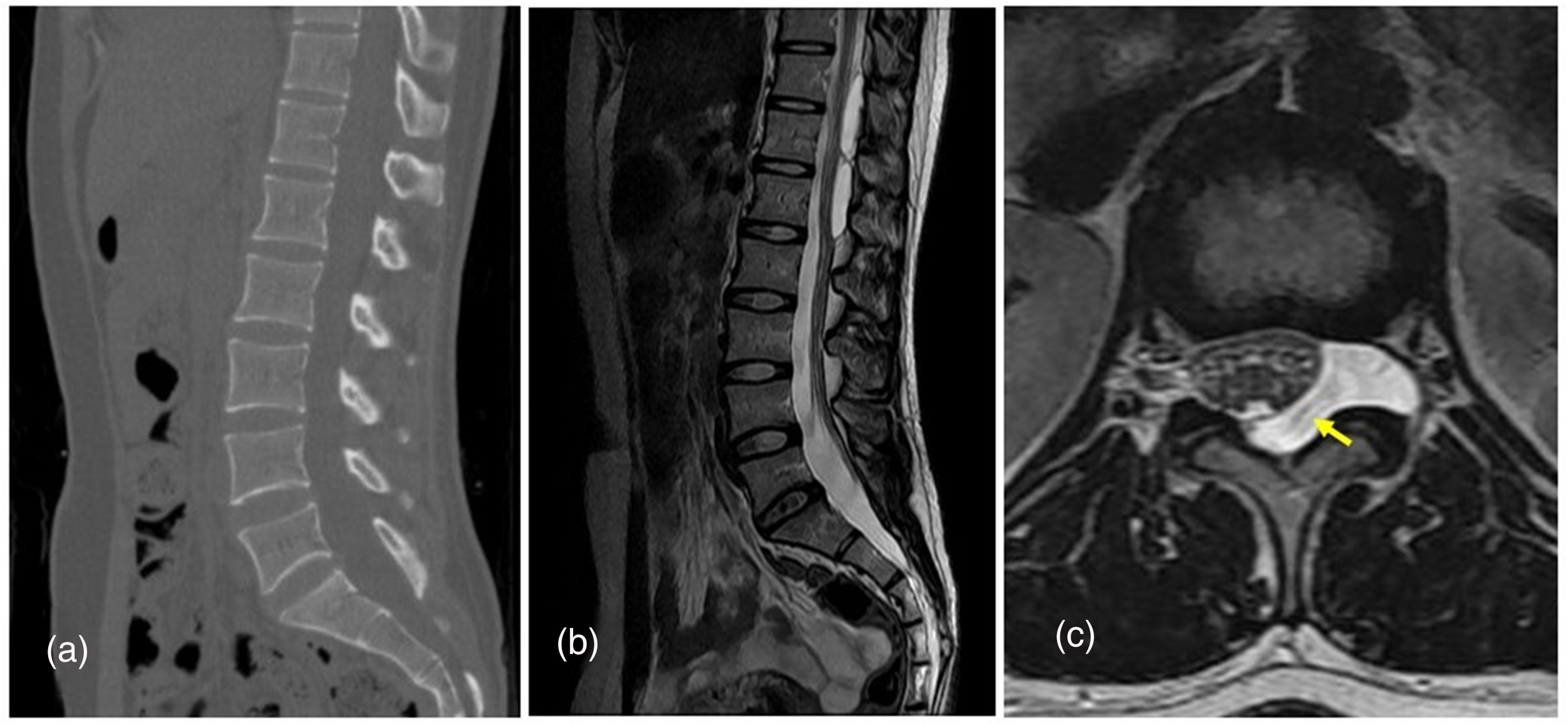
Preoperative imaging of the extradural meningeal cyst in case illustration 1. (a) Axial CT image demonstrating spinal canal widening and bony remodeling at T11–L1; (b) sagittal T2-weighted MRI showing a dorsally located extradural cystic lesion displacing the thecal sac ventrally at T11–L1. The cyst is septated into two compartments, and the fluid signal is identical to CSF. (c) Axial T2-weighted MRI identifying a focal signal void at the left T12–L1 intervertebral foramen (yellow arrow), suggesting a communicating dural defect.
The patient underwent left-sided hemilaminectomy at T12. After removal of the ligamentum flavum, a cystic mass was identified in the epidural space. The cyst wall was thin and transparent under microscopic inspection (Figure 2(a)). After opening the dorsal cyst wall, a large amount of CSF-like fluid drained from the lesion. Dissection of the multilayered transparent membrane exposed a communicating dural defect at the dural sleeve near the left T12 rootlet (Figure 2(a)). Herniated rootlets were identified within the defect and were reduced without sacrifice or injury. The dural defect was closed primarily with sutures (Figure 2(b)). Pathological examination confirmed an arachnoid cyst with flattened epithelial lining. The patient had no postoperative neurological complication, and the symptoms improved after surgery. Follow-up MRI 6 years postoperatively showed no recurrence (Figure 2(c)).
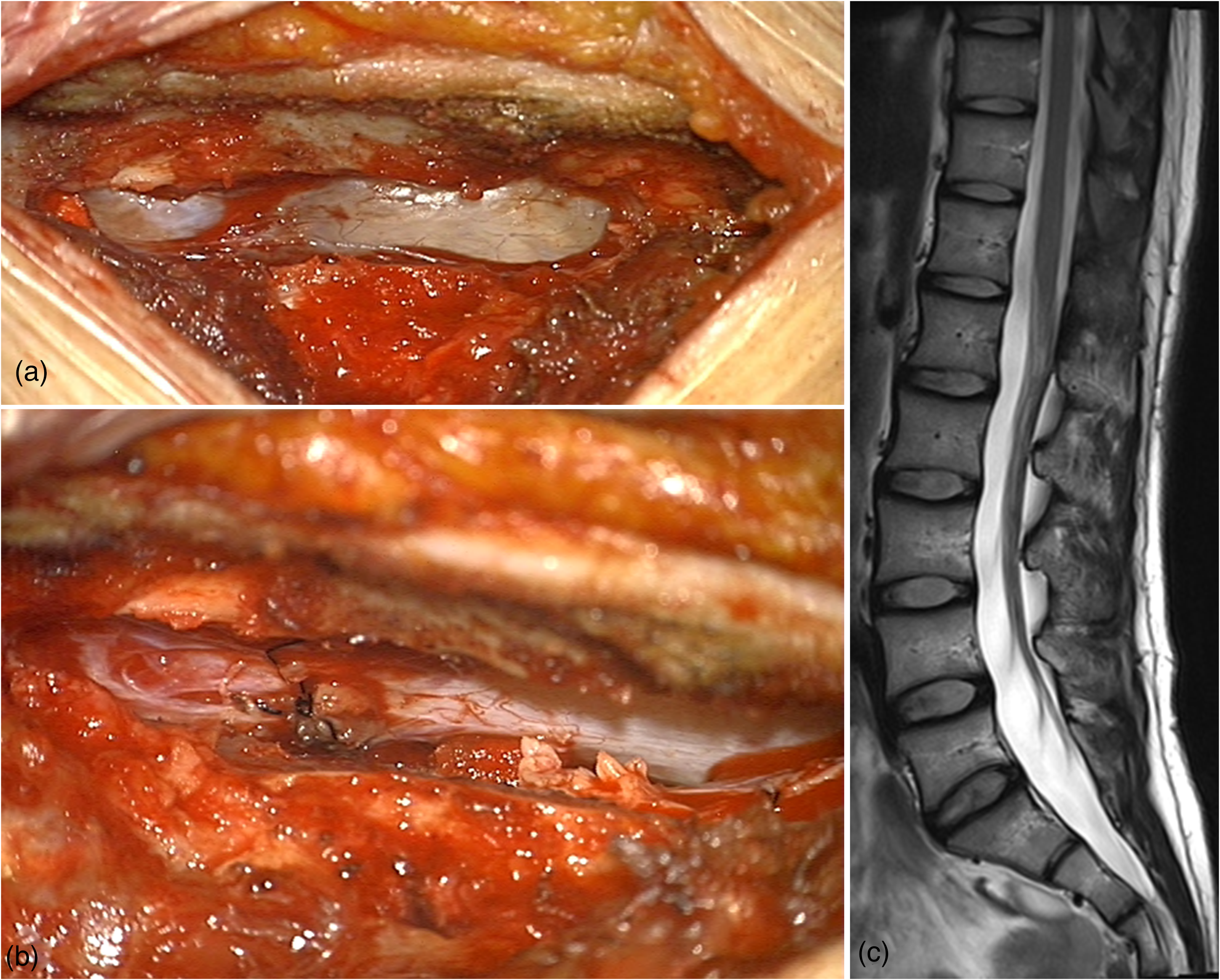
Intraoperative findings and postoperative outcome in case illustration 1. (a) Intraoperative photograph showing a thin, transparent dorsal cyst wall and multilayered cyst membrane. The communicating dural defect near the left T12 rootlet is exposed. (b) Photograph showing primary suture closure of the dural defect with preservation of the rootlets; (c) follow-up MRI 6 years postoperatively, showing no recurrence.
Case illustration 2
In December 2013, a man in his early 50s was admitted to this institution with a 1-month history of lower back pain and radiating pain in both legs. He had undergone acupuncture treatment after symptom onset. Despite conservative management, bilateral posterior leg pain persisted. Neurological examination showed no significant motor weakness, no increase in deep tendon reflexes, and no pathological reflexes.
Lumbar MRI showed a large cystic lesion on the dorsal aspect of the thecal sac, compressing the spinal cord ventrally from T10 to L4 (Figure 3(a) and (b)). Associated myelopathic cord signal change was observed (Figure 3(a)). The lesion had a lobulated cystic appearance, with high signal intensity on T2-weighted images and low signal intensity on T1-weighted images. Lumbar CT confirmed a posterior epidural cystic mass at T10–L4 with indentation of the spinal cord. CT myelography demonstrated filling of the cystic lesion with radiopaque contrast medium without extravasation into the subdural, subarachnoid, or epidural spaces, suggesting a contained communicating lesion (Figure 3(c) and (d)).
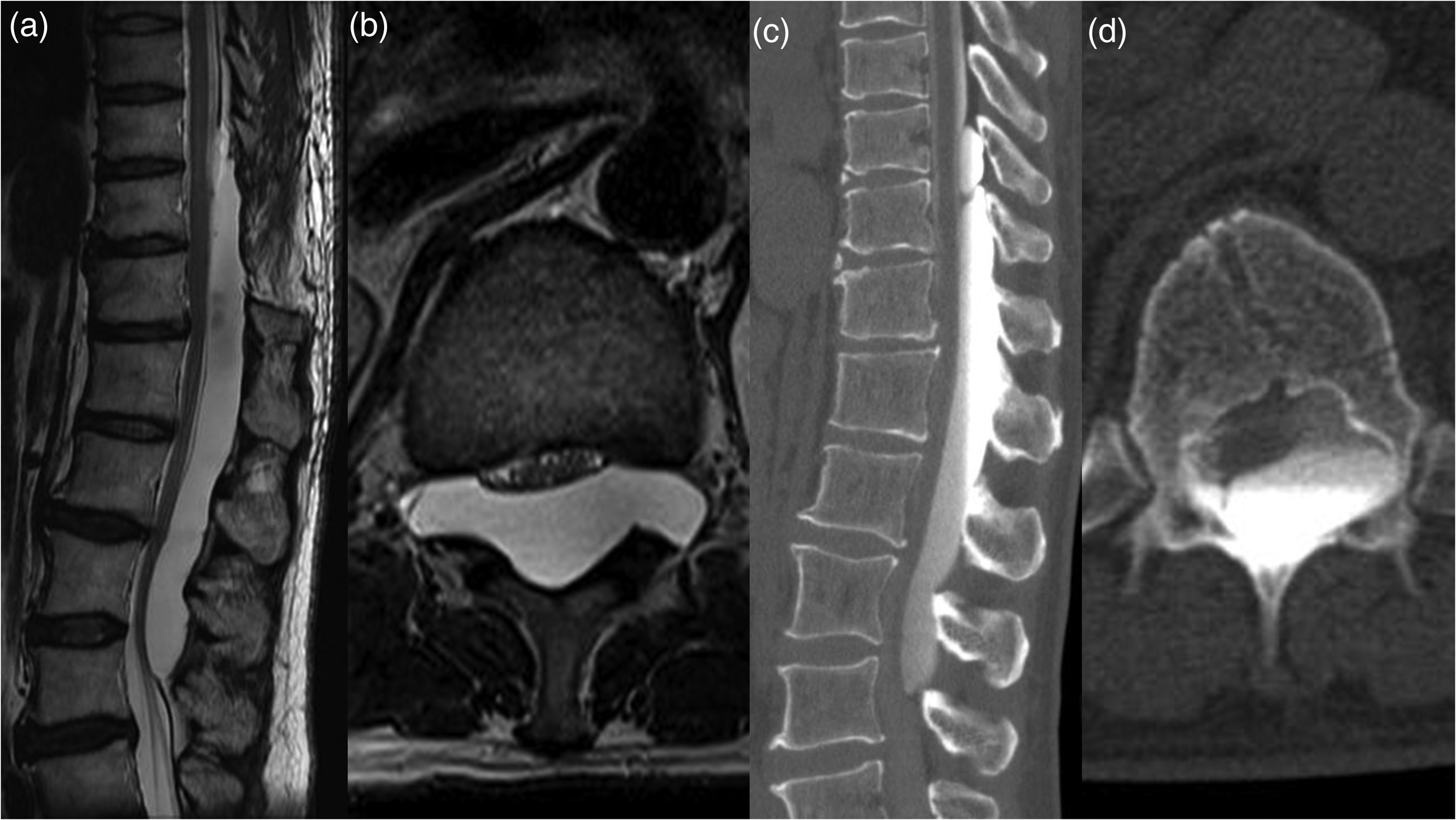
Preoperative imaging of the meningeal cyst in case illustration 2. (a) Sagittal T2-weighted MRI showing a lobulated, high-signal-intensity cystic lesion compressing the spinal cord ventrally from T10–L4, with associated myelopathic cord signal change; (b) axial T2-weighted MRI showing the posterior cystic lesion compressing the spinal cord; (c) CT myelography showing filling of the cystic lesion with contrast medium; (d) sagittal CT myelography confirming a contained lesion without contrast extravasation into surrounding spaces.
The patient underwent subtotal laminectomy at T10 and total laminectomy at T11. After removal of the laminae, the outer membrane of the cyst was exposed and partially resected. Dissection was performed between the thinned dura mater and the inner cyst membrane (Figure 4(a)). At the T10–T11 level, a suspected communicating tract was identified on the left side. Dissection of this tract resulted in CSF leakage, which was managed with coagulation and sealing rather than primary suture repair (Figure 4(b)). No further CSF leakage was observed, and the procedure was completed.
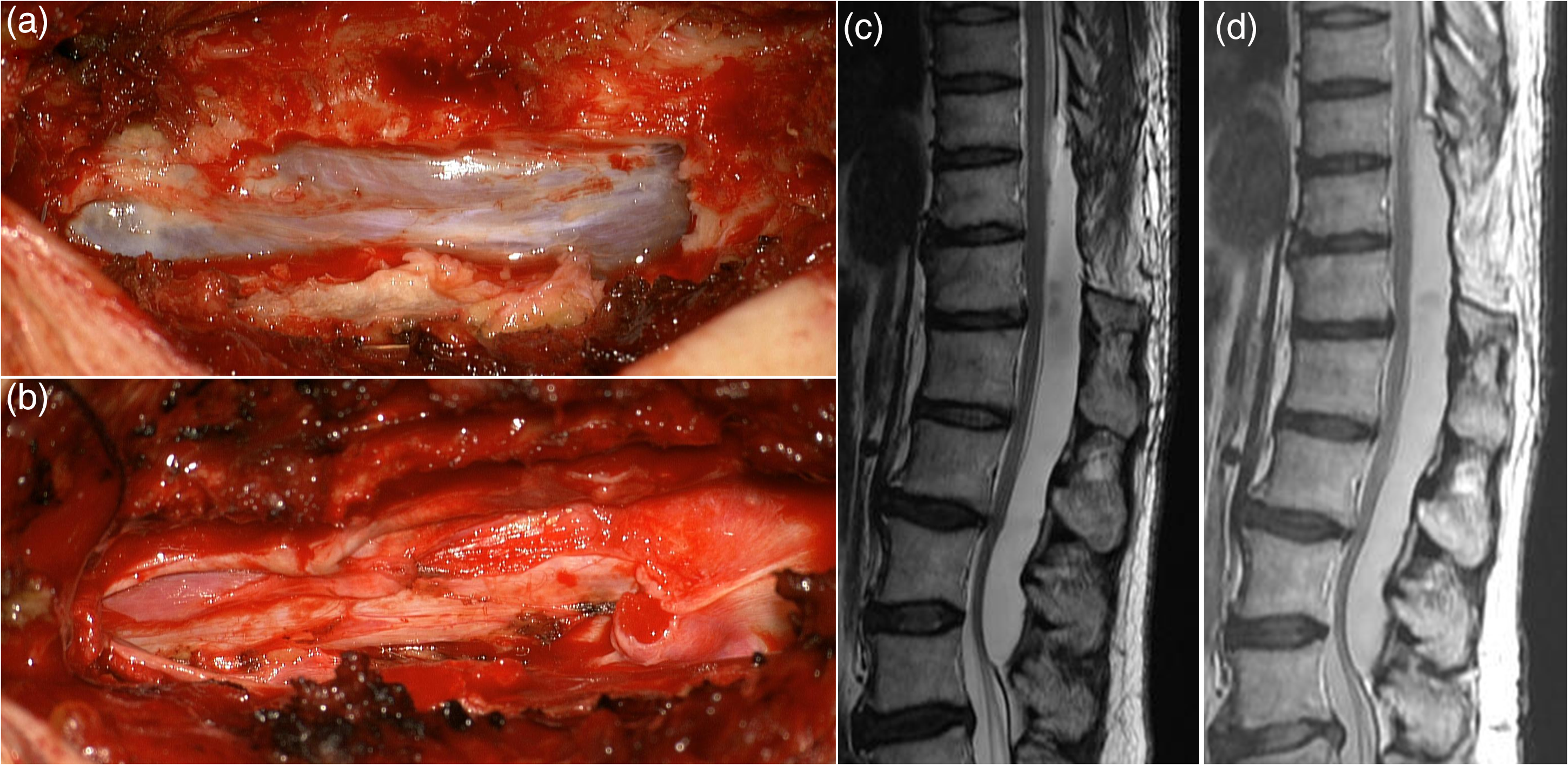
Intraoperative findings and postoperative outcomes in case illustration 2. (a) Intraoperative photograph showing dissection between the thinned dura mater and the inner cyst membrane; (b) photograph illustrating management of a suspected communicating tract at T10–T11, with coagulation and sealing performed to control CSF leakage; (c) sagittal T2-weighted MRI 6 months postoperatively showing a persistent residual or recurrent cystic lesion; (d) sagittal T2-weighted MRI 5 years postoperatively showing no interval enlargement and preserved spinal alignment.
Postoperative pathological analysis confirmed an arachnoid cyst. The patient's back and radiating pain improved without neurological deterioration. Follow-up MRI at 6 months and 5 years showed a persistent residual or recurrent cystic lesion without interval enlargement, and the patient remained asymptomatic (Figure 4(c) and (d)). This case was therefore interpreted as radiological persistence or recurrence without clinical recurrence.
Discussion
Spinal meningeal cysts are rare and may resemble arachnoid cysts radiologically and intraoperatively. However, the term meningeal cyst is often preferred because arachnoid cells are not always identified on pathological examination. 10 Nabors et al. classified spinal meningeal cysts according to anatomical location and the presence or absence of neural tissue, providing a practical framework for distinguishing Type IA extradural cysts from perineural and intradural cysts. 1
The pathogenesis of SEMCs remains incompletely understood. Dural defects may be congenital or idiopathic or may develop after trauma, inflammation, or other mechanical factors.4,5 These defects are commonly reported near the junction between the thecal sac and the nerve root sleeve.2,5 In the present series, six patients had a possible precipitating or associated event before symptom onset, supporting but not proving the possibility that mechanical or iatrogenic factors may contribute to dural weakening in some patients.
Several mechanisms have been proposed for cyst enlargement, including active CSF transport, osmotic gradients, pulsatile CSF dynamics, and a valve-like mechanism.2–4 Histological observations that cyst lining cells are not secretory have shifted attention toward passive CSF transport. 4 Rohrer et al. described a ball-valve mechanism in which CSF enters the extradural cyst but cannot freely exit, resulting in progressive enlargement. 6 In our cases, intraoperative findings often demonstrated CSF egress through the dural defect and rootlet herniation at the communication site, which is consistent with this pathophysiological model.
Preoperative localization of the dural defect remains challenging. Plain radiographs and CT may reveal indirect signs such as bony erosion, spinal canal enlargement, foraminal widening, or vertebral scalloping. 2 MRI is the principal diagnostic modality because SEMCs typically show signal intensity equivalent to CSF and demonstrate their relationship to the thecal sac and neural elements. Nevertheless, the most widened foramen or most prominent bony change does not always correspond to the actual dural defect, as also observed in our series. Delayed CT myelography, cine-MRI, and epidural cystography have been proposed to improve localization of small dural communications near nerve root sleeves.2,11,12 In the present series, CT myelography was performed in one patient but did not precisely identify the dural defect, whereas a T2 signal void correctly suggested the defect location in two patients.
The main value of this series is the long-term clinical observation supporting a defect-oriented surgical concept. In large multilevel SEMCs, radical cyst wall excision may require extensive exposure and may increase the risk of postoperative deformity or instability. If the dural communication can be identified, partial cyst wall resection or fenestration combined with primary dural repair may achieve neural decompression and interruption of the CSF inflow pathway and limit surgical morbidity. Our finding that no radiological recurrence was detected among patients with both primary dural repair and available postoperative imaging supports this concept, although it does not establish causality because of the small sample size and the absence of a balanced comparison group.
This study also illustrates the practical limitation of the strategy. In some patients, the dural defect cannot be confidently localized preoperatively or may not be amenable to primary suture closure intraoperatively. In such situations, excessively limited exposure may risk missing the communication site, whereas complete historical cyst excision may be unnecessarily invasive. Osteoplastic laminotomy may provide a useful compromise by allowing adequate exposure to inspect the likely defect region and preserve posterior elements and potentially reducing the risk of post-laminectomy deformity. Jian et al. reported that the lateral aspect around T12–L1 is a common site of fistulas in SEMCs, and this region was also frequently involved in our series. 13
The practical take-home message is therefore not that dural closure is the sole determinant of recurrence prevention but that surgeons should actively search for and close the dural communication whenever feasible. Complete removal of the entire cyst wall is not always required if the communication can be reliably interrupted and adequate neural decompression is achieved.
This study has several limitations. First, it was a retrospective single-center case series with only 10 patients. Second, the inclusion period was long, during which imaging protocols, operative techniques, and follow-up practices evolved substantially. Third, only one patient did not undergo primary dural repair; consequently, the study cannot establish a causal relationship between dural closure and prevention of recurrence. Fourth, postoperative radiological follow-up was incomplete in some patients. Fifth, surgical approaches were heterogeneous, reflecting changes in clinical practice over time. Finally, patient-reported outcome measures were not collected using standardized instruments. These limitations require cautious interpretation of the observed association between dural repair and favorable long-term radiological outcomes.
Conclusion
In this small retrospective case series of SEMCs, targeted identification and closure of the dural communication was associated with favorable long-term clinical outcomes and low radiological recurrence among patients with available postoperative imaging. These findings support a less extensive, dural defect-oriented surgical strategy when the communication site can be identified. Larger multicenter studies are needed to clarify the relative contributions of dural repair, cyst wall resection, and surgical exposure to long-term recurrence prevention.
Supplemental Material
sj-txt-1-imr-10.1177_03000605261460303 - Supplemental material for Spinal extradural meningeal cysts: Long-term outcomes of a dural defect-oriented surgical strategy
Supplemental material, sj-txt-1-imr-10.1177_03000605261460303 for Spinal extradural meningeal cysts: Long-term outcomes of a dural defect-oriented surgical strategy by Jong-Hwan Hong, Jong-Hoon Jung, Ji-Ho Jung, Moon-Soo Han and Jung-Kil Lee in Journal of International Medical Research
Supplemental Material
sj-docx-2-imr-10.1177_03000605261460303 - Supplemental material for Spinal extradural meningeal cysts: Long-term outcomes of a dural defect-oriented surgical strategy
Supplemental material, sj-docx-2-imr-10.1177_03000605261460303 for Spinal extradural meningeal cysts: Long-term outcomes of a dural defect-oriented surgical strategy by Jong-Hwan Hong, Jong-Hoon Jung, Ji-Ho Jung, Moon-Soo Han and Jung-Kil Lee in Journal of International Medical Research
Footnotes
Acknowledgments
This work was supported by the Gwangju AI Healthcare Ecosystem Establishment Project funded by the Ministry of Science and ICT (MSIT, Korea) Balanced National Development Account (Project Name: Gwangju AI Healthcare Ecosystem Establishment Project/Project Number: H0401-26-1001). This work was also supported by a grant (BRCI26085) of Chonnam National University Hospital Biomedical Research Institute.
The authors used AI tools only to improve the English language and readability of the manuscript. No AI tools were used for the study design, data analysis, interpretation, or generation of scientific content.
Ethical approval and informed consent
This study was approved by the Institutional Review Board of Chonnam National University Hospital (IRB No. CNUH-2023-398; approval date: December 2023). Written informed consent for surgical treatment was obtained from all patients as part of routine care. Individual informed consent for study participation was not obtained because the study used only deidentified retrospective data and the investigators did not have access to direct patient identifiers.
Author contributions
J-HH contributed to study conception and design, data acquisition, analysis and interpretation, and manuscript drafting. J-HJ, J-HJ, and M-SH contributed to data acquisition, interpretation of clinical and radiological findings, and critical revision of the manuscript. J-KL supervised the study, contributed to interpretation of the findings, and critically revised the manuscript for important intellectual content. All authors approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and analyzed during the current study are not publicly available because they contain potentially identifiable clinical information, but deidentified data may be made available from the corresponding author on reasonable request and subject to institutional approval.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.