
Abstract
Objective
The traditional method of intraspinal anesthesia relies on surface anatomical landmarks for positioning, which is associated with a low accuracy rate. In addition, the procedure remains challenging, and the identification of anatomical structures is complex. This study aimed to develop an adaptive attention U-network to enhance the segmentation performance of spinal structures under ultrasound images.
Methods
Ultrasound videos of the spines were collected from 80 pregnant women, yielding a total of 1000 annotated images that were used to establish a novel database, spine ultrasound image dataset. Adaptive attention U-network uses the multidepth convolution kernel and adaptive local channel attention modules to effectively extract multiscale features. Subsequently, the global attention gate module and multiscale adaptive dynamic modulation were introduced to capture critical features and enhance image super-resolution performance. Comprehensive experiments were conducted on the spine ultrasound image dataset and public breast ultrasound images dataset, in which adaptive attention U-network was juxtaposed with other current medical image segmentation models using metrics including dice similarity coefficient.
Results
On the spine ultrasound image dataset, adaptive attention U-network achieved a mean dice similarity coefficient of 0.905. In external validation using the breast ultrasound images dataset, the network's segmentation of benign tumor structures reached a dice similarity coefficient of 0.857, demonstrating superior generalization capabilities. Adaptive attention U-network demonstrated consistent segmentation stability across all tested structures.
Conclusions
The proposed adaptive attention U-network significantly enhances the segmentation accuracy for spinal anatomical structures in ultrasound images, demonstrating superior precision compared with existing methods.
Keywords
Introduction
Background
Intraspinal anesthesia, including spinal block and epidural block, is a commonly used clinical anesthesia approach owing to its convenience and cost-effectiveness. 1 During spinal anesthesia procedures, anesthesiologists can quickly perform puncture and administer anesthetic agents at specific locations within the patient's spinal canal without the need for complex airway management and deep monitoring of multiple organ functions, as required in general anesthesia. This significantly reduces preoperative preparation time and enhances surgical efficiency. Additionally, the equipment and drugs required for intraspinal anesthesia are relatively simpler and less expensive than those required for general anesthesia, eliminating the need for expensive general anesthetic drugs and sophisticated anesthesia maintenance and monitoring equipment. This is particularly beneficial for controlling medical costs, particularly in primary healthcare units or resource-limited areas. 2
In traditional clinical anesthesia procedures, surface anatomical structures are typically used to guide the location of the puncture site. Studies have shown that the accuracy of locating adult lumbar intervertebral spaces using palpation is approximately 30%, whereas the accuracy can be significantly improved to 71% under ultrasound guidance. Furthermore, palpation-based localization may result in errors involving more than one segment have been reported in 27% of cases, whereas with ultrasound guidance, errors are limited to no more than one segment. 3 This discrepancy indicates that traditional palpation methods are associated with a high risk of misjudging lumbar intervertebral spaces, whereas ultrasound can considerably improve the accuracy of lumbar intervertebral space assessment. Traditional methods are inaccurate for localization and may require multiple puncture attempts, with even greater challenges encountered in special populations such as older patients, patients with obesity, and pregnant women. In addition, puncture procedures performed using traditional methods are blind and invasive. Control of puncture depth is highly dependent on operator experience and tactile sensation, which may result in injuries during needle puncture or catheter insertion, such as puncturing the ligamentum flavum, damaging venous blood vessels, or inserting the needle too deeply and potentially injuring the spinal nerves or spinal cord. In contrast, under ultrasound guidance, the puncture needle is visible throughout the whole process, allowing the operator to directly observe the position of the needle tip and thereby avoid critical structures. 4 Therefore, ultrasound technology enables accurate and rapid localization of lumbar segments, visualization of the puncture pathway, and enhanced safety. 5
However, there are still certain limitations associated with current ultrasound technology. Ultrasound operation is technically demanding, and structural identification remains challenging. The development of ultrasound-assisted localization technology aims to address these difficulties and improve accessibility. Therefore, the use of machine learning algorithms to identify structures in spinal short-axis images and improve the accuracy of ultrasound-based structural identification has considerable clinical significance. In recent years, multiple studies have focused on combining clinical ultrasound images with artificial intelligence algorithms to improve the accuracy and safety of clinical procedures.6–8 For inexperienced junior anesthetists, ultrasound-guided paramedian intraspinal anesthesia requires skilled ultrasound techniques and anatomical knowledge. Understanding and interpreting ultrasound images poses a significant challenge. Although this is an in-plane technique, real-time visualization of the needle shaft and tip is also difficult because the ultrasound scan site and needle entry site are separated by relatively long distances.9,10 On this basis, deep learning models can automatically recognize and segment structures such as the lumbar interspinal ligaments (ILs), articular processes, and anterior complex (AC) and posterior complex (PC) structures by training on large amounts of image data. This assists anesthesiologists in accurately locating the spinal canal and helps prevent complications, such as block failure or damage to related tissues and organs, that may result from limited experience or insufficient technical proficiency. 5
Related work
Currently, the integration of artificial intelligence with medicine, particularly in the field of medical image processing, has achieved widespread applications, including image recognition and segmentation technologies as well as models capable of detecting and classifying lesions, such as tumors, various pathologies, and abnormal structures. Notably, deep learning has demonstrated results comparable to that of professional clinicians in identifying diabetic retinopathy and related eye diseases when evaluating retinal images of patients with diabetes from diverse ethnic groups. 11 Deep learning technology has significantly advanced the field of medical image segmentation. By automatically extracting complex features, these algorithms improve segmentation accuracy and efficiency, thereby contributing considerably to clinical diagnosis and treatment planning. 12 Convolutional Neural Networks (CNNs) are among the most commonly used architectures in deep learning and play a central role in medical image segmentation. These networks automatically extract spatial hierarchical features from images through multilayered convolutional operations, making them suitable for various medical imaging modalities. Kamnitsas et al. proposed a two-pathway, 11-layer deep three-dimensional CNN for precise brain lesion segmentation. 13 Slimi et al. proposed a framework capable of achieving effective noise suppression and precise anatomical segmentation, enabling clearer visualization of anatomical structures and their boundaries. 14 In the field of medical education, deep learning technology has also demonstrated significant application potential and value. 15 However, improvements in the performance of deep learning algorithms often come with increased complexity, which limits the clinical application of ultrasound-assisted image recognition technology.
Therefore, this study aimed to develop an innovative and efficient deep learning algorithm to assist clinicians in performing ultrasound-guided intraspinal anesthesia. The proposed algorithm is designed to automatically identify key spinal structures in short-axis ultrasound images, including ILs, APs, and AC and PC.
Dataset
Data sources
The spine ultrasound image dataset (SUID) was developed to focus on essential anatomical structures of spine under ultrasound scanning. Given the widespread use of intraspinal anesthesia in obstetric surgery and the high quality of maternal spinal ultrasound images, 80 pregnant women who underwent elective cesarean sections under ultrasound-guided intraspinal anesthesia at the First Hospital of Putian were retrospectively enrolled. Their video images of the spinal area were collected before the intraspinal anesthesia puncture procedure.
The study adhered to the principles of the Declaration of Helsinki Declaration 1975, as revised in 2024.16,17 This study was approved by the Ethics Committee of Putian First Hospital (Approval Number: 2024-167, Approval Date: 4 December 2024). All patient details have been deidentified.
Patients were placed in a lateral position, and ultrasound scanning began at the sacrum and proceeded longitudinally toward the head. A 2–5 MHz convex-array ultrasound probe (Shenzhen Huasheng Medical Technology Co., Ltd., model: Labat SP) was used. By counting the number of the interspaces, the operator moved the probe to the L3–L4 interspace and subsequently rotated it by 90°, adjusting the probe so that the midline of the screen aligned with the midline of the IL, the most conspicuous hyperechoic region. In this position, important anatomical structures involved in the puncture procedure could be visualized, namely ILs, APs, and the AC and PC. All scans were obtained in accordance with a standardized imaging protocol by the same experienced operator to minimize inter-device and inter-operator variability.
The basic characteristics of the enrolled patients are shown in Table 1.
Basic information of patients included in SUID.

BMI: body mass index; SUID: spine ultrasound image dataset.
Preparation and preprocessing of SUID
Each video was segmented into frames, from which 3–5 high-quality images with clear anatomical visualization were selected. “High-quality images” were defined as those demonstrating excellent visualization of anatomical structures, minimal artifacts, high contrast, and a high signal-to-noise ratio (SNR). To enhance model generalizability and mitigate the risk of overfitting, the training and evaluation datasets also deliberately included moderate-quality images exhibiting marginally reduced contrast and SNR.
These images were then manually annotated using Labelme by two anesthesiologists with extensive experience in performing intraspinal anesthesia, who established the anatomical structures to be labeled and the annotation criteria. To ensure the accuracy of the annotations, a cross-validation process was conducted between the two experts. Specifically, after each expert completed their initial annotations, the other expert reviewed them to identify any discrepancies. When disagreements occurred, the experts discussed the annotations until a consensus was reached. Subsequently, the annotations were verified by senior experts. If any dispute persisted, the corresponding data were excluded to ensure the reliability of the dataset. This process minimized variability and improved the overall quality of the annotations.
A total of 1000 images were generated, and rotation and flipping techniques were applied for data enhancement. These images were used to train and validate the model. Specifically, 80% of the videos were allocated to create the training set for model training, whereas the remaining 20% were used to create the test set for model performance evaluation.
Model design
Structure of adaptive attention U-network (U-net) (AAU-Net)
U-Net is an encoder–decoder architecture based on CNNs that combines the high-level semantic information of the encoder with the low-level detail information of the decoder through skip connections, thereby achieving precise localization. 18 Therefore, this study designed an improved version of U-Net, the AAU-Net. The overall architecture is presented in Figure 1.

Overall structure of AAU-Net.
As shown in Figure 1, AAU-Net takes a single-channel 512 × 512 ultrasound image as input (Con1-5). After the first convolutional operation, the feature representation is expanded to a 32 × 512 × 512 feature map for subsequent multilevel feature extraction. Appropriate strides are applied within each convolutional layer to maintain the size of the feature map, whereas max pooling is used to halve the height and width and double the number of feature channels when transitioning to the next network layer. For example, the Con1 feature map, after max pooling, produces a Con2 feature map of size 64 × 256 × 256.
A single encoder–decoder structure consisting of a contracting path (encoder) and an expansive path (decoder) was adopted. The encoder comprises the multidepth convolution kernel (MDCK) module (detailed in section MDCK) and the adaptive local channel attention (ALCA) module (detailed in section ALCA ) and uses the Gaussian error linear unit (GELU) activation function.
To capture globally significant features, the global attention gate (GAG) module (detailed in section GAG ) was applied. The GAG module suppresses noise and captures critical global features. Connections between the encoder and decoder are established through skip connections incorporating the GAG module.
Finally, the decoder concatenates the received feature maps and applies convolutional and transposed convolutional operations to resize the feature maps and adjust the number of channels, ensuring that the output Exp feature map is the same size as the corresponding Con feature map. Within the decoder, the input low-resolution image is first transformed into the feature space using a 3 × 3 convolutional layer and then successively passed through multiscale adaptive dynamic modulation (MSADM) module, another 3 × 3 convolutional layer, and a GELU layer. The resulting output is added to the output of the first convolution layer to generate the final result. The MSADM module (detailed in section MSADM) was used to enhance the efficiency and efficacy of image super-resolution by learning multiscale feature representations and dynamically modulating spatial features.
Multidepth convolution kernel
The convolution operation enables comprehensive feature extraction and pattern recognition from input data, making it a fundamental component of deep learning. The size of the convolution kernel is crucial in determining the receptive field and feature extraction ability of each layer. Smaller kernels can effectively capture local details; however, their receptive fields are limited, making it difficult to perceive broader global information. In contrast, larger kernels are more effective at capturing global features but require additional parameters, substantially increasing the computational burden. This heightened complexity may also amplify the risk of overfitting, particularly when working with limited data, thereby complicating model training. Previous studies have indicated that stacking multiple 3 × 3 kernels can approximate the larger receptive fields of larger kernels, enhancing representational power and moderating computational and parameter requirements. 19
Therefore, we designed the front encoder, MDCK, which is composed of three convolutional branches. The proposed MDCK structure is shown in Figure 2.
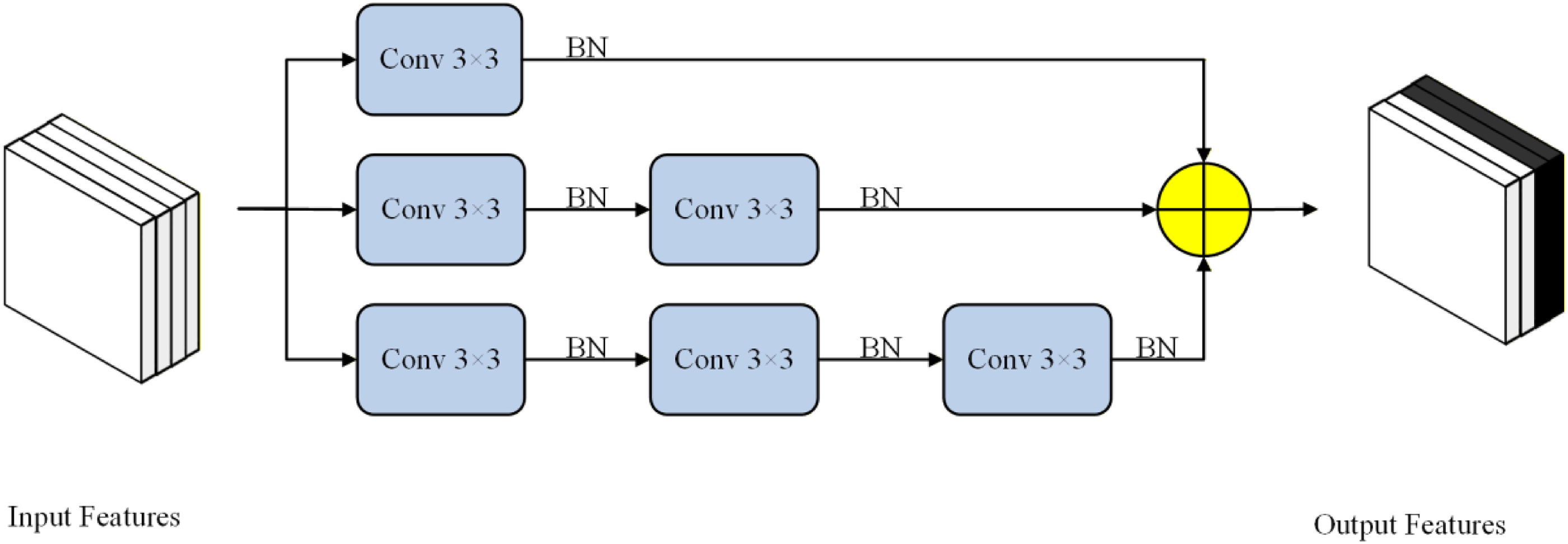
Structure of MDCK module (⊕: residual connection).
In the first branch, the input feature x is passed through a 3 × 3 convolution with a dilation rate of 1, followed by a batch normalization (BN) layer, before being directly output. 20 In the second and third branches, the input feature x passes through two and three such convolutional layers, respectively, before output generation. The outputs from the three branches are subsequently combined through residual connections before being passed to the next stage. By using sequences of small convolution kernels to emulate large ones and combining the outputs of convolutions applied at varying frequencies through residual links, these pathways collectively capture a diverse feature representation and highlight relationships among different anatomical structures. This approach improves the retention of both local detail and contextual context. Furthermore, the GELU activation function replaces the commonly used rectified linear unit (ReLU) activation function after each convolution in the MDCK module. Compared with ReLU, GELU provides a smoother nonlinear mapping, thereby enhancing model expressiveness and robustness, particularly for complex image segmentation tasks. 21
The expression for the MDCK structure is as follows:
In Equation (1), 
In this equation,
ALCA
Recently, channel attention mechanisms have demonstrated great potential for improving the performance of CNNs. Although these mechanisms increase computational complexity to some extent, they improve overall model efficiency. By focusing on important channels, the model can avoid allocating excessive computational resources to channels that contribute little to the task. The squeeze-and-excitation (SE) block was developed to adaptively recalibrate channel-wise feature responses by explicitly modeling interdependencies among channels. 22 However, because of the dimensionality reduction process, there is still room for performance improvement in this module.
To introduce appropriate cross-channel interactions, the ALCA module was introduced as the back-end encoder. This module addresses the contradiction between performance and complexity in CNN channel attention mechanisms and maintains good versatility and adaptability. The proposed ALCA structure is shown in Figure 3.
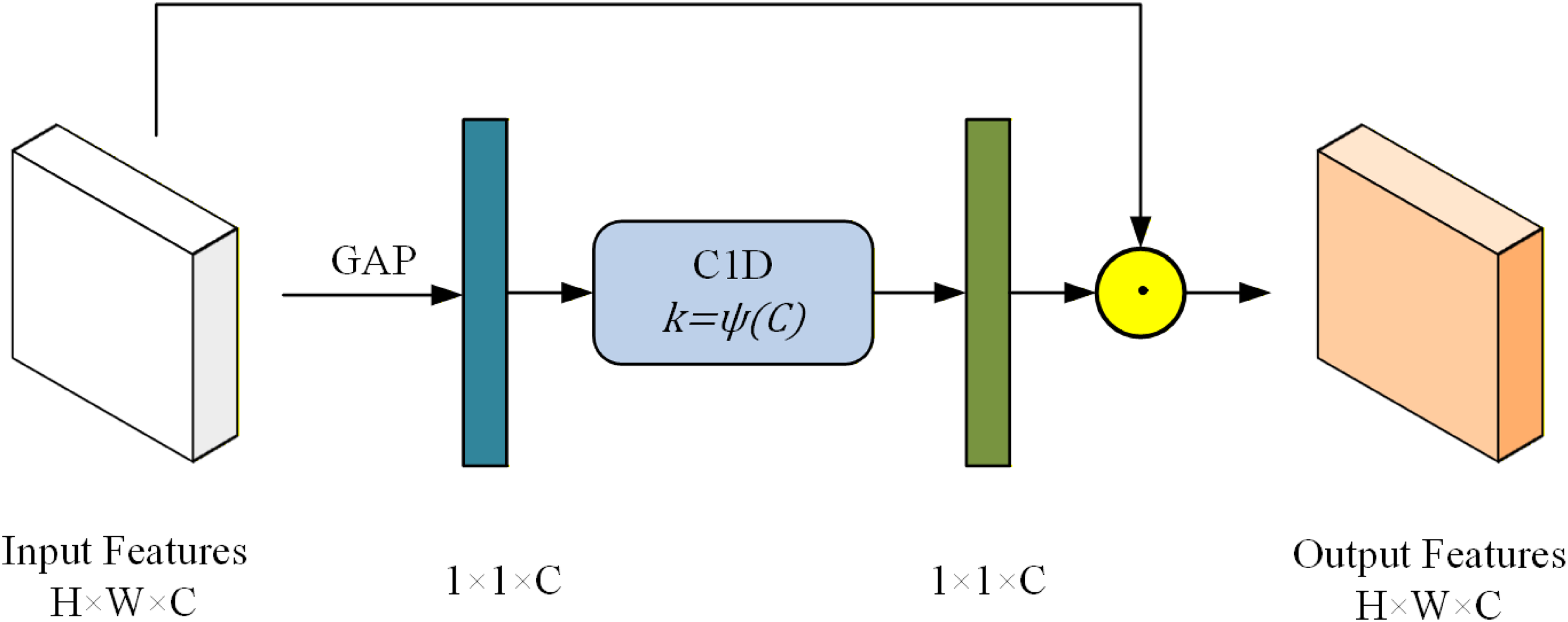
Structure of ALCA module (⊙: element-wise product).
The ALCA module obtains features through global average pooling (GAP) and then generates channel weights using fast 1D convolutions, where the kernel size (
The expression for the fast 1D convolution can be defined as follows:

In the ALCA module, high-dimensional channels have longer-range interactions, whereas low-dimensional channels undergo shorter-range interactions through nonlinear mapping. The module does not need to reduce the dimension of the input data, allowing the weight of each channel to directly correspond to its features, thereby improving the learning effect of the channel attention. Moreover, it introduces very few additional parameters and computational quantities, ensuring that the overall model remains lightweight.
GAG
The GAG for medical image segmentation was introduced to extract important information from the ALCA module without significantly increasing computational cost.
24
First, a 1 × 1 convolution is applied to combine the upsampled features 

Structure of GAG module (⊗: multiplication).

In Equations (5) and (6),
MSADM
In AAU-Net, the decoder gradually restores the high-level features extracted by the encoder to the same resolution as the input image, thereby enabling pixel-level image segmentation.
In the MSADM module, image super-resolution is efficiently achieved through four steps: input features, multiscale feature generation, feature aggregation, and feature modulation. 25 First, the normalized input features are divided into four groups of components, which are then processed separately. A 3 × 3 depth-wise convolution is applied to the first group, whereas the remaining groups are sampled individually using pooling operations. The proposed MSADM structure is shown in Figure 5.

Structure of MSADM module (⊙: element-wise product).
Given the input feature X, this procedure can be formulated as follows:


The formulation can be expressed as follows:

Experiments
Experiment setup
We developed the model using the PyTorch framework, with computations performed on an Nvidia GTX-A6000 Ada graphics processing unit (GPU). Training was conducted end-to-end on SUID and breast ultrasound image (BUSI), 26 with each central processing unit (CPU) handling a batch size of eight images. The Adam optimizer was employed with a momentum setting of 0.9 and a weight decay of 1e−4. A dynamic learning rate schedule was used, starting at 1e−4 and decaying to a minimum of 1e−2 using a cosine annealing decay without any restarts. Training was limited to 100 epochs to reduce the risk of overfitting given the limited dataset size. All modules were initialized from scratch without pretraining or prior initialization. To ensure fairness, all comparative models were trained under identical experimental settings, including the same dataset split, data augmentation strategies, optimizer settings, learning rate schedule, batch size, and training epochs.
A total of 80% of the dataset was randomly selected for training the neural network model, and once training was completed, the remaining 20% was used for testing. The dice similarity coefficient (DSC) was used as the evaluation metric to assess model performance in ultrasound image segmentation. Four target anatomical structures were assessed: ILs, APs, the AC, and the PC.
The DSC is computed as follows:
Segmentation results on SUID
AAU-Net was trained for 100 training iterations on SUID and compared with advanced models using the DSC metric for each segmented structure. Table 2 presents the DSC values for the four target structures and the final mean DSC (mDSC) of the different networks.27–30
Segmentation results on SUID from different networks.
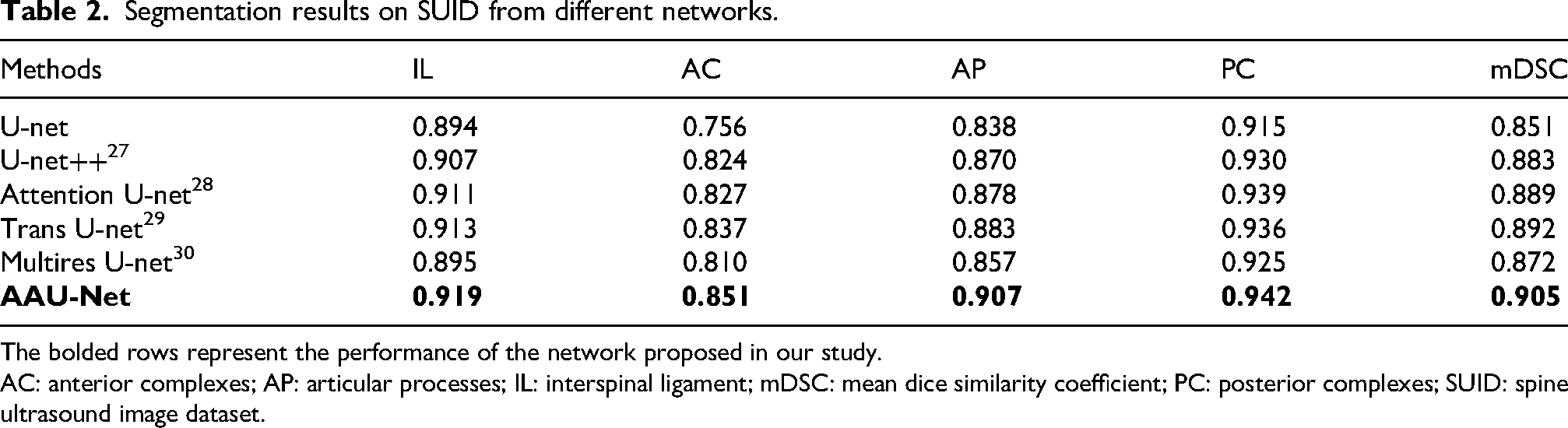
The bolded rows represent the performance of the network proposed in our study.
AC: anterior complexes; AP: articular processes; IL: interspinal ligament; mDSC: mean dice similarity coefficient; PC: posterior complexes; SUID: spine ultrasound image dataset.
The findings indicate that AAU-Net achieved the best performance across all four target anatomical structures. As shown in Figure 6, AAU-Net not only achieved higher segmentation accuracy but also generated smoother segmentation boundaries.

Comparative visualization of segmentation results from different networks (A: interspinal ligament, B: articular processes, C: posterior complex, D: anterior complex). In the images, text at the bottom right indicates the mean dice similarity coefficient value of corresponding network.
After excluding patients with body mass index (BMI) >30 kg/m2 in SUID (13 in 80), we observed no significant difference in segmentation performance (in mDSC).
Segmentation results on public datasets
To evaluate the generalization capability of AAU-Net, the model was trained on the public BUSI dataset, 26 and its segmentation performance was compared with that of advanced models using the DSC metric. The BUSI dataset, a widely used resource in breast cancer research, contains 780 ultrasound images categorized as normal, benign, or malignant, all with annotated masks, enabling the evaluation of tumor detection and segmentation methods.
For external validation, the benign tumor category, comprising 487 images, was selected. After 100 iterations, the performance results of the segmentation of benign tumor structure on the BUSI dataset reached the DSC of 0.857, indicating that AAU-Net exhibited robust performance and high stability.
Ablation study for the proposal
An ablation study was conducted to evaluate the effectiveness of AAU-Net. The original U-Net served as the baseline model, and experiments were performed by adding or removing individual modules. Evaluation metrics included DSC values for the IL, AP, PC, and AC. All experimental settings were kept consistent with the training methodology described above to isolate the contribution of each module. The results are presented in Table 3.
Results of the ablation study.
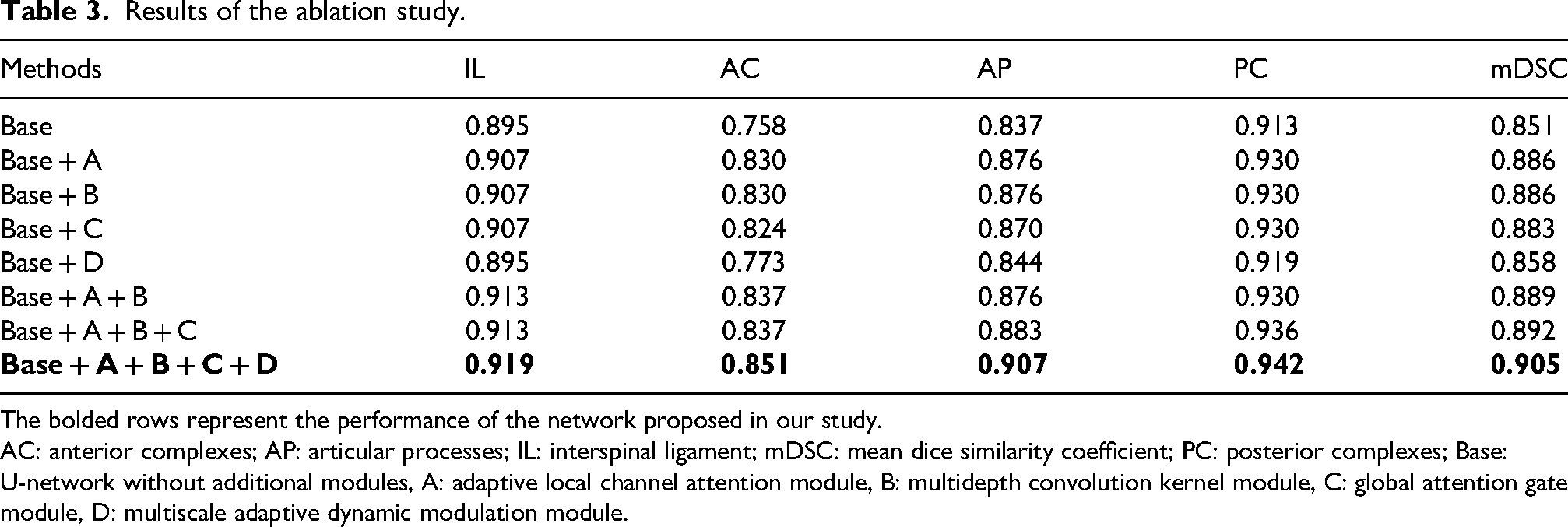
The bolded rows represent the performance of the network proposed in our study.
AC: anterior complexes; AP: articular processes; IL: interspinal ligament; mDSC: mean dice similarity coefficient; PC: posterior complexes; Base: U-network without additional modules, A: adaptive local channel attention module, B: multidepth convolution kernel module, C: global attention gate module, D: multiscale adaptive dynamic modulation module.
Overall, the baseline U-Net demonstrated relatively good recognition performance for all four structures, with DSC values exceeding 0.75 and an mDSC of 0.851. The first improvement in the ablation study involved incorporation of the ALCA module into the encoder of the standard U-Net framework without altering the internal modules. Initially, the MDCK module was integrated into the main encoder of the model utilizing the dual-encoder framework to evaluate changes in performance metrics. As shown in Table 3, the MDCK module produced improvements in structural recognition comparable to those achieved by the ALCA module. These findings suggest that the convolutional kernel enhancements contribute to more accurate preservation of image features. The GAG and MSADM modules were then incorporated into the skip connections and decoder, respectively. Both modifications resulted in improved segmentation performance compared with the original U-Net model during ablation testing, achieving mDSC values of 0.883 and 0.858, respectively.
Next, two or more modules were integrated simultaneously into the baseline model to assess their compatibility and determine whether their combined use could further improve segmentation performance. The results demonstrated that combining modules yielded better recognition performance than introducing each module individually. These findings indicate good compatibility among the proposed components. By enhancing the convolutional kernel structure, channel attention mechanism, skip connections, and image super-resolution, we successfully enhanced the segmentation performance of spinal images. Similar to the results of single tests, our complete model also achieved the greatest improvement over the baseline model in terms of PC structure.
Discussion
AAU-Net is a network based on U-Net, with comprehensive improvements made to its encoder, convolutional kernel, and decoder. Based on our validation results, this network performs well in the identification and segmentation of spinal structures in ultrasound images. Reviewing the results of the ablation tests, we observed that the improvement in identifying the deepest and most complex structure, the AC, is the most significant, whereas the improvement for the largest and easiest-to-distinguish structure, the IL, is relatively smaller. The relatively low segmentation performance of the AC is primarily affected by ultrasound acoustic shadowing and depth-related signal attenuation. The AC is located at a considerable distance from the probe and is obscured by superficial bone tissue,, resulting in substantially reduced contrast and indistinct boundaries in ultrasound images. 31 The proposed network improves segmentation performance under these challenging conditions through multiple architectural enhancements. In addition, after excluding patients with obesity, the segmentation performance of AAU-Net showed no significant improvement, demonstrating its good generalizability. However, because only 13 of 80 patients were excluded, further external validation is required to confirm robustness.
In clinical intraspinal anesthesia procedures, anesthetists must accurately determine the angle of needle insertion to avoid bony structures. The network structure developed in this study can accurately delineate the various anatomical structures visible in transverse ultrasound images of the intervertebral space, thereby assisting anesthetists in performing this procedure more effectively. The external validation results further demonstrate that our network can achieve robust performance not only in spinal structure segmentation but also in related segmentation tasks, thereby reducing the risk of overfitting.
However, several limitations remain. First, the spinal anatomy of pregnant women differs from that of the general population in several important respects, including increased lumbar lordosis curvature; ligament laxity; and a dilated, congested epidural venous plexus.32–34 These physiological changes may enhance the visibility of spinal structures yet simultaneously limit the applicability of algorithmic models developed using this dataset. Second, during image acquisition, the operator counted upward from the sacrum under ultrasound guidance to identify the L3–L4 interspace. The presence of lumbosacral transitional vertebrae may affect the accuracy of this localization process. Studies have reported a prevalence of lumbosacral transitional vertebrae of approximately 11%–29% in females, suggesting that up to one-third of images may contain deviations in intervertebral level identification.35,36 Although radiological assessment remains the gold standard for determining spinal levels, ultrasound localization was used in this study because it is the safest and most commonly used method for evaluating pregnant women. Third, only pregnant women were included because their spinal ultrasound images are generally clear and readily obtainable, and image acquisition does not impose additional burden on this population. 37 Furthermore, all scans were performed by the same operator to minimize inter-operator variability. Although these measures improve the internal validity of the study, they may limit its external validity. Another important limitation concerns computational efficiency in real-time applications. Preliminary laboratory experiments demonstrated that AAU-Net achieved approximately 16–28 frames per second (FPS) for 512 × 512 ultrasound images under NVIDIA RTX A6000 GPU acceleration, indicating its potential for near-real-time clinical assistance. However, the model has not yet been deployed on embedded ultrasound hardware or portable clinical devices. Consequently, actual deployment performance may vary depending on hardware resources and optimization strategies. Future work will focus on lightweight optimization, model quantization, and hardware-specific acceleration to improve real-world deployment efficiency. In addition, further clinical studies involving anesthetists with varying levels of experience are needed to evaluate the applicability of the network across different surgical procedures and to further improve model robustness and adaptability.
Looking ahead, there is increasing demand for the integration of machine learning algorithms into clinical ultrasound systems. Embedding such algorithms directly into ultrasound devices would enable clinicians to more conveniently utilize research advances in routine practice. However, this requirement imposes constraints on model complexity and necessitates a balance between model accuracy and computational size. In the present study, the encoder improvements substantially enhanced overall model performance without causing a substantial increase in model size. These characteristics may facilitate the future clinical implementation of machine learning algorithms in clinical settings.
Conclusion
This paper presents AAU-Net, a network designed for the segmentation and recognition of spinal structures during ultrasound-guided intraspinal anesthesia. The improved encoder, channel attention mechanism, skip connections, and decoder collaboratively enhance feature extraction and segmentation accuracy. The network demonstrates excellent performance in spinal ultrasound image segmentation, outperforming comparative models in the identification of target structures. External validation further confirms the model's strong generalization capability.
Footnotes
Ethical approval
This study has been approved by the Ethics Committee of Putian First Hospital (Approval No. 2024-167, Approval Date: 4 December 2024). The study is a retrospective research project involving clinical data from 80 patients, in accordance with international ethical guidelines and national legal requirements.
This research is a retrospective study and has been granted an exemption from the informed consent requirements by the ethics committee.
Author contributions
Jin S managed the coordination of the project and was responsible for data collection and writing the manuscript. Duan J and Chen Z were responsible for the primary design of the model and conducting experiments. Chen F contributed with data verification. Zhou M and Fang W assisted with data collection guidance and partial data acquisition. Lin L, Wu Q, and Zou Z provided overall guidance and guidance throughout the entire research process. Lin L and Zou Z provided funding and equipment provision. All authors have reviewed and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was supported by Shanghai Municipal Health Commission Special Research Project on Smart Healthcare (2025ZHYL044) and Putian Joint Health Project 2025 (2025NJYL026).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current study are not publicly available due to patient consent agreements and ethical restrictions. Requests for access to the data should be directed to the corresponding author.
Utilization of generative AI
During the preparation of the paper, DeepSeek (DeepSeek-R1-0528, utilized on 2025.6.1, via a cloud API) was used to improve language clarity and readability. The use of generative AI in the research strictly adhered to the guidance of the TITAN Guidelines. Afterward, the authors reviewed and thoroughly edited the content as needed and take full responsibility for the publication's content. The authors declare no conflicts of interest or financial relationships with any AI vendors.