
Abstract
Objective
To evaluate the efficacy of small-incision, point-by-point debridement combined with double-cannula negative-pressure irrigation and drainage in the treatment of granulomatous mastitis.
Methods
This single-center, retrospective matched cohort study included 118 patients with granulomatous mastitis who were treated at the Third People’s Hospital of Mianyang between January 2022 and December 2024. Patients with comparable clinical characteristics were matched in a 1:1 ratio and assigned to either the treatment or control group, with 59 patients in each group. Patients in the treatment group underwent small-incision, point-by-point debridement of necrotic tissue combined with double-cannula continuous negative-pressure irrigation and drainage, whereas those in the control group underwent conventional incision and drainage combined with negative-pressure drainage. Postoperative drainage volume, time to drain removal, frequency of dressing changes, wound healing time, primary healing rate, recurrence rate, and breast shape score were compared between the two groups.
Results
Compared with the control group, the treatment group had a significantly lower postoperative drainage volume, fewer dressing changes, shorter time to drain removal, and shorter wound healing time. The recurrence rate was significantly lower in the treatment group than in the control group (χ2 = 5.221, p < 0.05). The primary healing rate was significantly higher in the treatment group than in the control group (χ2 = 4.140, p < 0.05). In addition, breast shape scores were significantly higher in the treatment group. All between-group differences were statistically significant.
Conclusion
Small-incision, point-by-point debridement combined with double-cannula negative-pressure irrigation and drainage may promote wound recovery, reduce recurrence, and better preserve breast appearance in selected patients with granulomatous mastitis requiring surgical treatment. Further prospective studies are warranted to confirm these findings.
Keywords
Introduction
Granulomatous mastitis (GM), also known as granulomatous lobular mastitis (GLM), is a rare benign chronic inflammatory disease of the breast characterized by granulomatous changes in the lobules of the mammary gland. However, in recent years, the incidence of GM has shown an increasing trend. 1 The main clinical manifestations include breast masses, pain, erythema, and swelling. Some patients may develop abscesses and ulceration, which can further progress to fistulas or sinus tracts. The heterogeneous clinical manifestations and lack of specific clinical features make both diagnosis and treatment challenging. 2 GM is typically associated with a prolonged disease course, lasting for months or years, and is prone to recurrence, which may further aggravate the condition. Owing to its unclear etiology, no standardized diagnostic or therapeutic protocol has yet been established in clinical practice. 3 Current treatment strategies mainly include pharmacological therapy and surgical intervention. 4 Surgical treatment can effectively remove lesions and remains an important therapeutic approach for GM. However, clinical outcomes vary considerably among different surgical techniques. Therefore, exploring more optimized surgical strategies is crucial for promoting postoperative recovery and improving patients’ quality of life.
Patients and methods
Research population
Study design and participants
This single-center, retrospective cohort study was conducted at the Third People's Hospital of Mianyang, Sichuan, China. Clinical data were retrospectively collected from patients diagnosed with GM who were treated at our institution between January 2022 and December 2024. After performing screening according to predefined diagnostic, inclusion, and exclusion criteria, 118 eligible patients were included in the final analysis. Written informed consent was obtained from all patients.
Patients were assigned to the treatment or control group according to the surgical procedure performed. Baseline characteristics were compared between the two groups to assess their comparability. Patients in the treatment group underwent small-incision, point-by-point debridement of necrotic tissue combined with double-cannula continuous negative-pressure irrigation and drainage, whereas those in the control group underwent conventional incision and drainage combined with negative-pressure drainage. Clinical outcomes were collected from medical records and postoperative follow-up data.
Baseline clinical data were extracted from medical records, including age, body mass index (BMI), disease duration, lesion diameter, lesion location, number of involved quadrants, history of previous treatment, and clinical subtype. Disease severity was assessed according to clinical manifestations, including abscess formation, sinus/fistula or skin ulceration, and mass-type lesions. The number of involved quadrants was recorded to reflect the extent of breast involvement.
Patients were included if they fulfilled all of the following criteria: (a) GM confirmed on pathological biopsy; (b) presence of surgical indications, including abscess formation, skin ulceration, sinus/fistula formation, obvious necrotic tissue requiring debridement, persistent symptoms after conservative treatment, or recurrent disease requiring local intervention; and (c) availability of complete clinical records and follow-up data.
Patients were excluded if they fulfilled any of the following criteria: (a) presence of other breast diseases, such as malignant tumors or breast tuberculosis; (b) concurrent severe systemic diseases; (c) a clinical diagnosis of GM without pathological confirmation; and (4) substantial missing clinical data.
This study was reviewed and approved by the Ethics Committee of the Third People's Hospital of Mianyang, Sichuan, China. All patient data were deidentified before the analyses. This study was conducted in accordance with the Declaration of Helsinki of 1975, as revised in 2024, and was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Sample size
This was a single-center retrospective cohort study based on available clinical records; therefore, no formal a priori sample size calculation was performed. The sample size was determined based on the number of eligible patients treated at our institution during the study period. All patients who met the inclusion and exclusion criteria between January 2022 and December 2024 were screened, and 118 patients were finally included in the analysis.
Clinical context of our institution
The Third People's Hospital of Mianyang is a regional referral center for inflammatory breast diseases, including GM. In our clinical practice, many patients are referred after a prolonged disease course, unsuccessful conservative treatment, abscess formation, skin ulceration, sinus/fistula formation, or disease recurrence. Therefore, surgical intervention is mainly considered for selected patients with complicated or refractory GM, rather than for all patients with this condition.
Surgical indications and severity assessment
Surgical treatment was considered for patients with GM who presented with abscess formation, skin ulceration, sinus or fistula formation, obvious necrotic tissue requiring debridement, persistent symptoms after conservative treatment, or recurrent disease requiring local intervention. At our institution, GM was not routinely graded using a universally accepted standardized severity scale. Therefore, disease severity was evaluated according to clinical manifestations and baseline lesion characteristics, including clinical subtype; lesion size; number of involved quadrants; presence of abscess, sinus/fistula, or skin ulceration; and history of previous medical or surgical treatment.
Research methods
Treatment procedures
Treatment group
Patients in the treatment group underwent small-incision, point-by-point debridement of the necrotic tissue combined with double-cannula continuous negative-pressure irrigation and drainage. Patients were placed in the supine position, with the affected upper limb abducted and fixed at 90°. After intravenous anesthesia, routine disinfection and draping were performed. A curved incision of approximately 4 cm was made along the margin of the areola. The necrotic tissue was removed in a point-by-point manner, and inflammatory lesions were incised and drained while preserving the surrounding normal breast structure as much as possible. After debridement, a double-cannula irrigation and drainage device was inserted and connected to a negative-pressure suction system. Postoperatively, continuous irrigation with 500–1000 mL of normal saline per day was performed according to the characteristics of the drainage fluid. The drainage tube was removed when the irrigation fluid became clear, and no purulent secretion or residual necrotic tissue was observed.
Control group
Patients in the control group underwent conventional incision and drainage combined with negative-pressure drainage. Patient positioning was the same as that in the treatment group. After intravenous anesthesia, a radial incision of approximately 5 cm was made at the lesion site. Pus was adequately drained, and inflammatory lesions and necrotic tissue were removed. The abscess cavity was then repeatedly irrigated using hydrogen peroxide solution and normal saline. After thorough cleaning, a negative-pressure drainage tube was inserted, the incision was sutured, and the operative cavity was closed. A local compression dressing was applied postoperatively to enable hemostasis. Postoperative dressing changes were performed regularly. The drainage tube was removed when the drainage volume remained below 15–20 mL/day.
Postoperative management and follow-up
No routine postoperative antibiotics were administered to either group. Postoperative wound management consisted mainly of drainage, irrigation, local dressing changes, and regular wound assessment. The dressing was changed every 1–2 days during hospitalization or more frequently in cases of obvious exudation, contamination, or loose dressings. At each dressing change, the wound condition, amount and characteristics of drainage, local redness and swelling, and signs of infection were evaluated.
The discharge criteria included stable vital signs, absence of active bleeding or uncontrolled local inflammation, effective drainage or satisfactory wound condition, adequate pain control, and the ability to continue wound care and follow-up on an outpatient basis. After discharge, patients returned to the outpatient clinic regularly for wound assessment and dressing changes until the wound was clean and free of secretion.
Patients were followed up at approximately 1 week, 2 weeks, 1 month, 3 months, 6 months, and 12 months postoperatively. Wound healing, drainage status, dressing requirements, recurrence, and breast appearance were evaluated during follow-up. Recurrence was defined as the reappearance of breast inflammatory lesions, abscess, sinus/fistula, or mass at the original or adjacent site after wound healing during the follow-up period.
Clinical parameters
The following clinical parameters were evaluated:
Postoperative drainage volume. Daily postoperative drainage volume was monitored and recorded until the removal of the drainage tube. Drain removal time. In the control group, the drainage tube was removed when the drainage volume remained below 15–20 mL/day. In the treatment group, the tube was removed when the irrigation fluid became clear, and no purulent secretion or residual necrotic tissue was observed. Frequency of dressing changes. Postoperative dressing changes were performed until the dressing remained clean and free of secretions. Wound healing time. Wound healing was defined as complete epidermal coverage without redness, swelling, oozing, or pain. Primary healing rate. Primary healing was defined as wound healing with neat margins, absence of infection, and tight closure after suturing. Recurrence rate. Patients were followed up for 12 months postoperatively. Recurrence was defined as the reappearance of breast inflammatory lesions, abscess, sinus/fistula, or mass at the original or adjacent site after wound healing during the follow-up period. Breast shape score. Breast shape was assessed using the Harris Breast Shape Scale, which evaluates symmetry, contour, nipple position, and skin texture on a scale of 1–10. Higher scores indicate better breast appearance.
Statistical analyses
Statistical analysis was performed using Statistical Package for Social Sciences (SPSS) software for Windows (version 26.0, SPSS Inc., Chicago, IL, USA). Continuous variables with a normal distribution were expressed as mean ± SD and compared using the independent-samples Student's t-test. Non-normally distributed continuous variables were expressed as median (P25, P75) values and compared using the Mann–Whitney U test. Categorical variables were expressed as n (%) and compared using Pearson's χ2 test or Fisher's exact test, as appropriate. A two-sided p-value <0.05 was considered statistically significant.
Results
Baseline characteristics
Baseline characteristics and disease severity indicators are summarized in Table 1. The two groups were comparable in terms of age, BMI, disease duration, lesion size, lesion location, number of involved quadrants, history of previous treatment, and clinical subtype, including abscess type, mass type, and sinus/ulceration type. Abscess-type disease was present in 39 patients (66.1%) in the treatment group and 41 (69.5%) in the control group, indicating that a substantial proportion of patients requiring surgical treatment had complicated local lesions. No statistically significant differences were observed in the baseline characteristics between the two groups.
Baseline characteristics and disease severity indicators of the two groups.
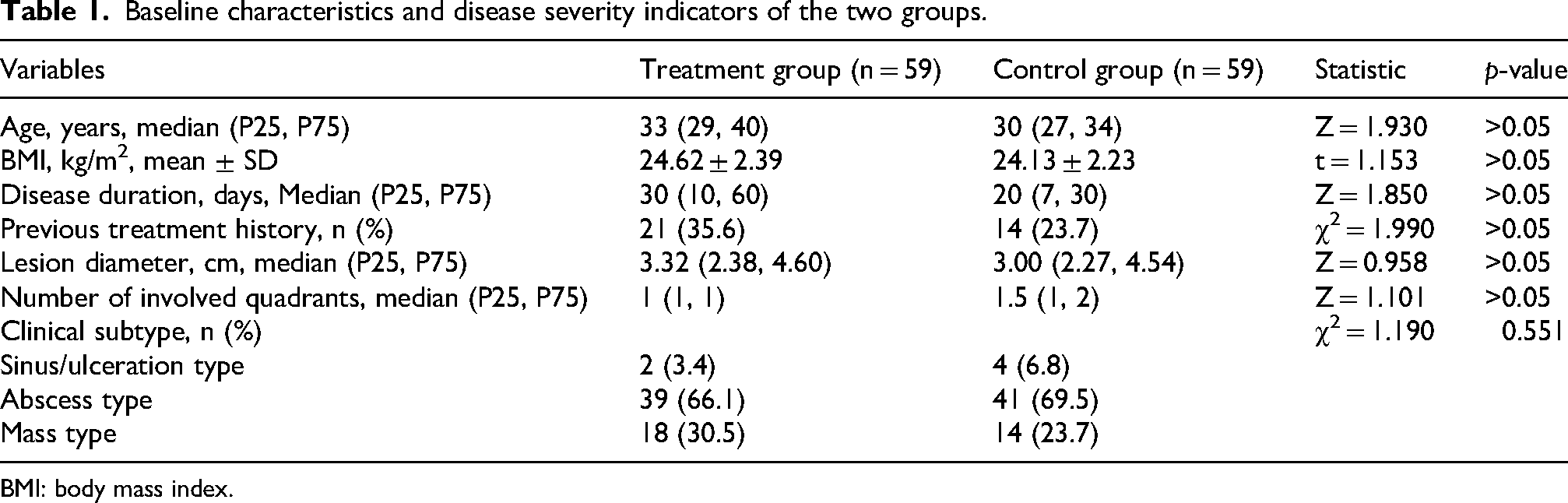
BMI: body mass index.
Clinical efficacy
Representative deidentified clinical photographs are shown in Figure 1. The images demonstrate typical complicated GM manifestations before treatment, including breast erythema, swelling, abscess formation, skin ulceration, sinus/fistula formation, necrotic tissue, and lesion-area marking. Representative postoperative images further illustrate wound healing, breast contour recovery, and the application of double-cannula negative-pressure irrigation and drainage in the treatment group.

Representative deidentified clinical photographs showing disease severity, surgical intervention, and postoperative appearance in patients with granulomatous mastitis (GM). (a) Representative preoperative images showing complicated GM manifestations, including breast erythema, swelling, abscess formation, skin ulceration, sinus/fistula formation, necrotic tissue, and lesion-area marking. (b) Representative preoperative images of patients in the treatment and control groups. The left image shows a patient from the treatment group before the surgery, and the right image shows a patient from the control group before the surgery. (c) Representative postoperative appearances of patients from the treatment and control groups. The left image shows postoperative wound healing and breast contour after small-incision, point-by-point debridement combined with double-cannula negative-pressure irrigation and drainage, whereas the right image shows the postoperative appearance of a patient who underwent conventional incision and drainage combined with negative-pressure drainage. (d) Early postoperative image of a patient from the treatment group following small-incision, point-by-point debridement combined with double-cannula negative-pressure irrigation and drainage.
As shown in Table 2, the treatment group had a significantly higher primary wound healing rate and a lower recurrence rate than the control group (both p < 0.05).
Comparison of the primary healing rate and recurrence rate between the two groups (n (%)).

Postoperative drainage volume, time to drain removal, frequency of dressing changes, and wound healing time
Postoperative drainage volume and frequency of dressing changes were significantly lower in the treatment group than in the control group (p < 0.05). Additionally, both time to drain removal and wound healing time were significantly shorter in the treatment group than in the control group (p < 0.05). The relevant results are presented in Table 3.
Comparison of postoperative drainage volume, frequency of dressing changes, time to drain removal, and wound healing time between the two groups (median (P25, P75)).

Breast shape score
Breast shape scores were significantly higher in the treatment group than in the control group (p < 0.01), as detailed in Table 4.
Comparison of breast shape scores between the two groups (median (P25, P75)).
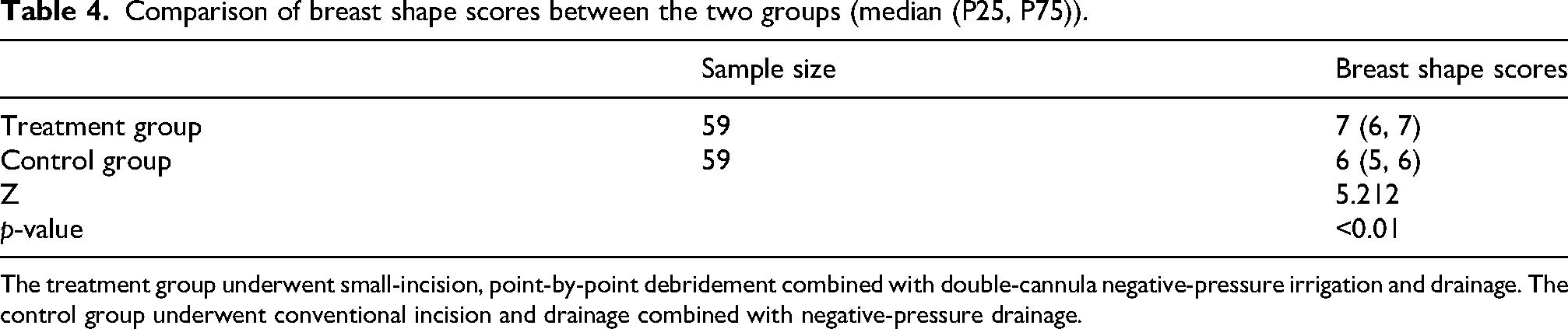
The treatment group underwent small-incision, point-by-point debridement combined with double-cannula negative-pressure irrigation and drainage. The control group underwent conventional incision and drainage combined with negative-pressure drainage.
Discussion
GM is a chronic inflammatory condition that primarily affects women of childbearing age; however, it also occurs rarely in men.5,6 Its onset is associated with multiple clinical factors, including obesity or overweight status, reproductive and lactation history, immune dysregulation, and local inflammatory responses. 7 Although the condition can manifest bilaterally, unilateral involvement is significantly more prevalent. 8 Patients typically present with painful breast erythema and palpable lumps. With disease progression, some patients may develop abscesses, skin ulceration, and sinus or fistula. The nonspecific nature of these clinical manifestations, combined with a high propensity for recurrence often complicates both diagnosis and treatment. 9 Although the exact pathogenesis of GM remains unclear, several studies have suggested the involvement of autoimmune mechanisms, local trauma, hormonal imbalances, microbial infection, and altered host immune responses. 10 Currently, there is no consensus on a standardized treatment for GM. However, available management strategies can be broadly categorized into conservative, pharmacological, minimally invasive, and surgical approaches. Pharmacological therapies primarily involve glucocorticoids, antibiotics, immunosuppressants, and traditional Chinese medicine. Observation or conservative management may be appropriate for selected patients with mild disease, while systemic corticosteroids and immunosuppressive agents are typically reserved for those with severe inflammatory or recurrent conditions. Additionally, intralesional steroid injection has emerged as a minimally invasive option, offering effective local disease control while minimizing systemic steroid exposure. 11 Antibiotics may be considered for patients with suspected bacterial infections or positive cultures, though they are not universally required for all GM cases. 12 Importantly, in the present study, no routine postoperative antibiotics were administered in either group; however, satisfactory wound recovery and low recurrence were still observed, particularly in the treatment group. This finding differs from the empirical antibiotic strategy that is still commonly adopted in some clinical settings and in certain consensus-based treatment recommendations, suggesting that routine broad-spectrum antibiotic use is not necessary for selected GM patients without clear evidence of bacterial infection. Avoiding the unnecessary use of antibiotics may help reduce the risks of antimicrobial resistance, gut microbiota disturbance, and drug-related adverse events while also aligning with the principles of minimally invasive, safe, and efficient treatment. More broadly, these observations support the view that GM is often not a simple bacterial infectious disease but a chronic inflammatory condition with immune-mediated and non-bacterial inflammatory components. Surgical interventions generally encompass abscess incision and drainage, simple lesion excision, extended excision of necrotic tissue, and, in severe cases, total mastectomy.13,14 Therefore, surgery should not be regarded as a universal first-line treatment for all GM patients. Instead, it is more suitable for those with complicated or refractory disease, such as patients presenting with abscesses, skin ulceration, sinus/fistula formation, obvious necrotic tissue, or recurrent lesions or those with an inadequate response to conservative treatment. Although surgery is a highly effective treatment, it often compromises the postoperative aesthetic appearance of the breast. Consequently, when surgical intervention is warranted, it is crucial to select an approach that minimizes breast tissue damage and preserves aesthetic quality while effectively reducing the risk of recurrence.
Several patients were referred to our institution after a prolonged disease course, previous unsuccessful conservative treatment, abscess formation, or the development of complicated local lesions. This local clinical context may partly explain why surgical treatment was more commonly considered in the present cohort. We acknowledge that treatment patterns for GM vary across institutions, and in some centers, conservative therapy or intralesional steroid injection may be preferred for patients with early-stage disease and mild clinical severity. Therefore, the findings of this study should be interpreted in the context of selected patients with GM requiring surgical intervention rather than be generalized to all patients with GM.
This study presents a surgical approach that combines small-incision, point-by-point debridement with double-cannula negative-pressure irrigation and drainage, allowing precise removal of necrotic tissue through a relatively smaller incision. Compared with traditional surgical techniques, which often require larger incisions or wider exposure, this approach may minimize damage to surrounding healthy tissues, better preserve normal breast structures, and reduce the adverse impact on breast appearance. 15 The effective drainage and irrigation function of the double-cannula system facilitates timely removal of necrotic tissues and inflammatory mediators, thereby creating a more favorable local environment for tissue repair. This process may contribute to reduced recurrence and improved wound recovery. 16
The results of this study demonstrated that the primary healing rate was significantly higher in the treatment group than in the control group, while the recurrence rate was notably lower (p < 0.05). These findings suggest that small-incision, point-by-point debridement combined with double-cannula negative-pressure irrigation and drainage offers advantages in selected surgically treated patients by reducing residual necrotic tissue, improving drainage efficiency, and promoting local wound repair. The rationale for this approach is that GM frequently presents with multiple lesions and may involve more than one quadrant. 17 Compared with conventional incision and drainage, small-incision, point-by-point debridement combined with double-cannula negative-pressure irrigation may allow more precise localization and removal of necrotic tissues while minimizing residual lesions. In addition, double-cannula drainage facilitates the timely removal of inflammatory exudate and pus, thereby reducing exudate accumulation, limiting persistent local inflammation, and promoting wound healing. Notably, these favorable outcomes were achieved in the absence of routine postoperative antibiotic use, indicating that effective local debridement, continuous irrigation, and adequate drainage may be sufficient to control postoperative inflammation in selected GM patients. This finding further suggests that the postoperative management of GM should not rely solely on empirical anti-infective therapy but should also focus on the removal of necrotic tissue, elimination of inflammatory exudate, and restoration of the local wound healing environment. However, these findings should be interpreted with caution because this was a retrospective observational study, and treatment selection may have been influenced by disease severity, surgeon preference, and institutional practice patterns.
This study demonstrated that the breast shape score was significantly higher in the treatment group than in the control group, indicating that this surgical approach may be more effective in preserving breast appearance. This advantage may be attributed to point-by-point debridement combined with precise drainage, which allows selective removal of necrotic tissue while minimizing damage to surrounding normal breast tissue, thereby preserving the original anatomical structure and tissue volume. Additionally, double-cannula negative-pressure irrigation helps maintain local wound cleanliness, reduce tissue adhesion and induration, and promote wound healing. These factors may contribute to better preservation of breast softness and symmetry while reducing the risk of postoperative localized induration or asymmetry, resulting in higher breast shape scores. Nevertheless, cosmetic outcomes were evaluated using clinical breast shape scores rather than patient-reported outcome measures or blinded independent assessment. Future studies should incorporate standardized cosmetic evaluation tools and patient satisfaction scales to provide a more comprehensive assessment of postoperative breast appearance.
This study has certain limitations. First, this was a single-center study with a relatively limited sample size; therefore, information and selection biases could not be completely avoided. Second, no formal a priori sample size calculation was performed because this was a retrospective study based on available clinical records. Third, the follow-up duration was relatively short. Recurrence of GM may occur 1–2 years or longer after the surgery; therefore, short-term follow-up may not fully capture the long-term efficacy and recurrence patterns of different surgical procedures. Fourth, no stratified analysis was performed according to different clinical subtypes of GM, which may have masked potential differences in the efficacy of this procedure among specific patient subgroups. Fifth, procedure-related adverse events and long-term cosmetic outcomes were not systematically evaluated. Further prospective multicenter studies with larger sample sizes, longer follow-up, standardized severity grading, and stratified analyses according to clinical subtype are needed to validate these findings.
In conclusion, small-incision point-by-point debridement combined with double-cannula negative-pressure irrigation and drainage may improve wound recovery, reduce recurrence, and preserve breast appearance in selected patients with complicated or refractory GM requiring surgical intervention. However, because of the retrospective design and single-center setting, these findings should be interpreted with caution and validated in future prospective multicenter studies.
Footnotes
Acknowledgments
The authors would like to thank to all study participants for their cooperation.
Ethics approval and consent to participate
This retrospective study was approved by the Ethics Committee of the Third Hospital of Mianyang and adhered to the ethical principles outlined in the Declaration of Helsinki (as revised in 2024). Written informed consent forms were obtained from all patients.
Author contributions
Lanying Li and Haiming Jia contributed to the conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, and resource provision for the study. Haiming Jia supervised the study. Lanying Li drafted the original manuscript, and both Lanying Li and Haiming Jia contributed to manuscript review and editing. All authors read and approved the final manuscript.
Funding
The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Project of Mianyang Municipal Health Commission; Project Title: Application of Metagenomic Sequencing Technology in Etiological Diagnosis of Granulomatous Mastitis and Research on Integrated Traditional Chinese and Western Medicine Treatment Strategies (grant number 202234).
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data sharing statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Artificial intelligence (AI)–assisted language editing statement
During the preparation of this manuscript, AI-assisted language editing tools were used only to improve grammar, clarity, readability, and scientific expression. No AI tools were used for study design, patient selection, data collection, data analysis, statistical analysis, image generation, interpretation of results, or the formulation of scientific conclusions. All AI-assisted edits were carefully reviewed, verified, and approved by the authors. The authors take full responsibility for the accuracy, integrity, and originality of the manuscript.