
Abstract
Objective
This study investigated the efficacy of a combined technique involving percutaneous pedicle screw fixation and percutaneous kyphoplasty in treating osteoporotic vertebral compression fractures with endplate depression.
Methods
A prospective cohort of 120 patients with osteoporotic vertebral compression fractures with endplate depression was classified into Group A (n = 58, percutaneous pedicle screw fixation + percutaneous kyphoplasty) and Group B (n = 62, percutaneous kyphoplasty). Radiographic parameters, visual analog scale score, and Oswestry Disability Index were systematically compared between the two groups postoperatively.
Results
Group A demonstrated significantly better Cobb angle correction than Group B (p < 0.05). Both percentage of the anterior and central vertebral height of the injured vertebra were significantly higher in Group A across all time points (p < 0.05). Group A exhibited significantly less secondary loss of Cobb correction angle and percentage of secondary loss of vertebral height (p < 0.05). The Oswestry Disability Index was significantly lower in Group A from postoperative 3 months to 2 years (p < 0.05).
Conclusions
The application of percutaneous pedicle screw fixation + percutaneous kyphoplasty demonstrates significant advantages in treating osteoporotic vertebral compression fractures with endplate depression, including enhanced reduction efficacy, reduced postoperative secondary loss of correction, and decreased risk of implant failure. This approach represents a safe and effective therapeutic strategy.
Introduction
Osteoporotic vertebral compression fractures (OVCFs) represent the most common spinal fractures, predominantly affecting postmenopausal women and older adults.1–3 The thoracolumbar vertebrae, particularly T12 and L1, are most frequently involved. OVCFs with endplate depression are characterized by predominant collapse of the central vertebral body, which is more severe than that of the anterior vertebral body. This results in a depressed morphology that typically presents as a biconcave vertebral deformity, thus complicating central vertebral height restoration. Nonsurgical treatment increases the risks of pneumonia, deep vein thrombosis, and pressure ulcers, potentially leading to multiorgan dysfunction. Therefore, surgical intervention is recommended for these patients.
With the widespread adoption of minimally invasive concepts and technological advancements, percutaneous pedicle screw fixation (PPSF) and percutaneous vertebral augmentation techniques—such as percutaneous vertebroplasty (PVP) and percutaneous kyphoplasty (PKP)—have emerged as mainstream treatments for OVCFs.4,5 These techniques offer advantages over traditional open surgery, such as reduced trauma, minimal blood loss, faster recovery, and improved clinical outcomes.6–8 However, despite these advancements, standalone minimally invasive interventions still face multiple challenges. Studies have reported that PPSF is associated with inadequate early postoperative pain relief, screw loosening or breakage, “vacuum sign,” and secondary loss of vertebral height during follow-up. Similarly, PVP/PKP may lead to complications such as cement leakage, uneven cement dispersion, intravertebral cleft formation, insufficient vertebral reduction, and even secondary collapse of the injured vertebrae.
To address the limitations of standalone minimally invasive techniques, bone cement augmentation combined with PPSF has been proposed to increase vertebral ultimate load and maintain vertebral height, thereby reducing complication risks.9–11 Although the combined strategy of PPSF and balloon dilation-assisted reduction of the depressed endplate may offer superior reduction, its efficacy in restoring central vertebral height remains poorly documented. This study implemented a sequential treatment strategy consisting of minimally invasive percutaneous reduction and fixation, balloon dilation-assisted reduction of endplates, and polymethylmethacrylate (PMMA) cement augmentation. We prospectively enrolled 120 patients with single-level OVCF with endplate depression and systematically evaluated the clinical outcomes of PPSF combined with PKP, focusing on its advantages in restoring vertebral height, maintaining correction, and reducing complication rates.
Methods
Protocol and registration
This single-center, prospective randomized controlled trial was approved by the Ethics Committee of Nanjing Luhe People's Hospital, Nanjing, China (approval No. LHLL2020-020, dated 26 December 2020) and was registered with the Chinese Clinical Trial Registry (No. ChiCTR2500104911). The reporting of this study conforms to the Consolidated Standards of Reporting Trials (CONSORT) statements 12 and adheres to the Helsinki Declaration of 1975 as revised in 2024. Signed informed consent was obtained from all participants prior to enrollment. There was no patient or public involvement in the design, conduct, or reporting of this trial.
Participants
From January 2021 to December 2022, 152 patients with OVCFs treated at the Department of Orthopedics of Nanjing Luhe People’s Hospital were initially enrolled in this prospective study. Participants were assigned to Group A (PPSF with PKP) and Group B (conventional PKP). Inclusion criteria were as follows: (a) radiographically confirmed OVCFs with endplate depression involving T11 to L2 vertebrae; (b) AO Spine–German Society for Orthopedics and Trauma (DGOU) Osteoporotic Fracture (OF) score ≥6; 13 (c) All patients demonstrated central vertebral height loss >25% in the affected vertebral bodies, which was calculated using the formula: [100% − (injured vertebral height / average height of the adjacent vertebrae) × 100%]; (d) acute single-level OVCFs were confirmed using MRI with high signal intensity; (e) age ≥60 years with bone mineral density (BMD) T-score less than −2.5 SD. Exclusion criteria were as follows: (a) BMD T-score greater than −2.5 SD or less than −5.0 SD to minimize confounding from extreme osteoporosis; (b) nonosteoporotic fractures or pathological fractures secondary to malignancy or benign lesions; (c) old OVCFs; (d) active systemic or localized infections; (e) multilevel vertebral injuries; (f) patients requiring spinal canal decompression. The flow diagram of the study is presented in Figure 1.
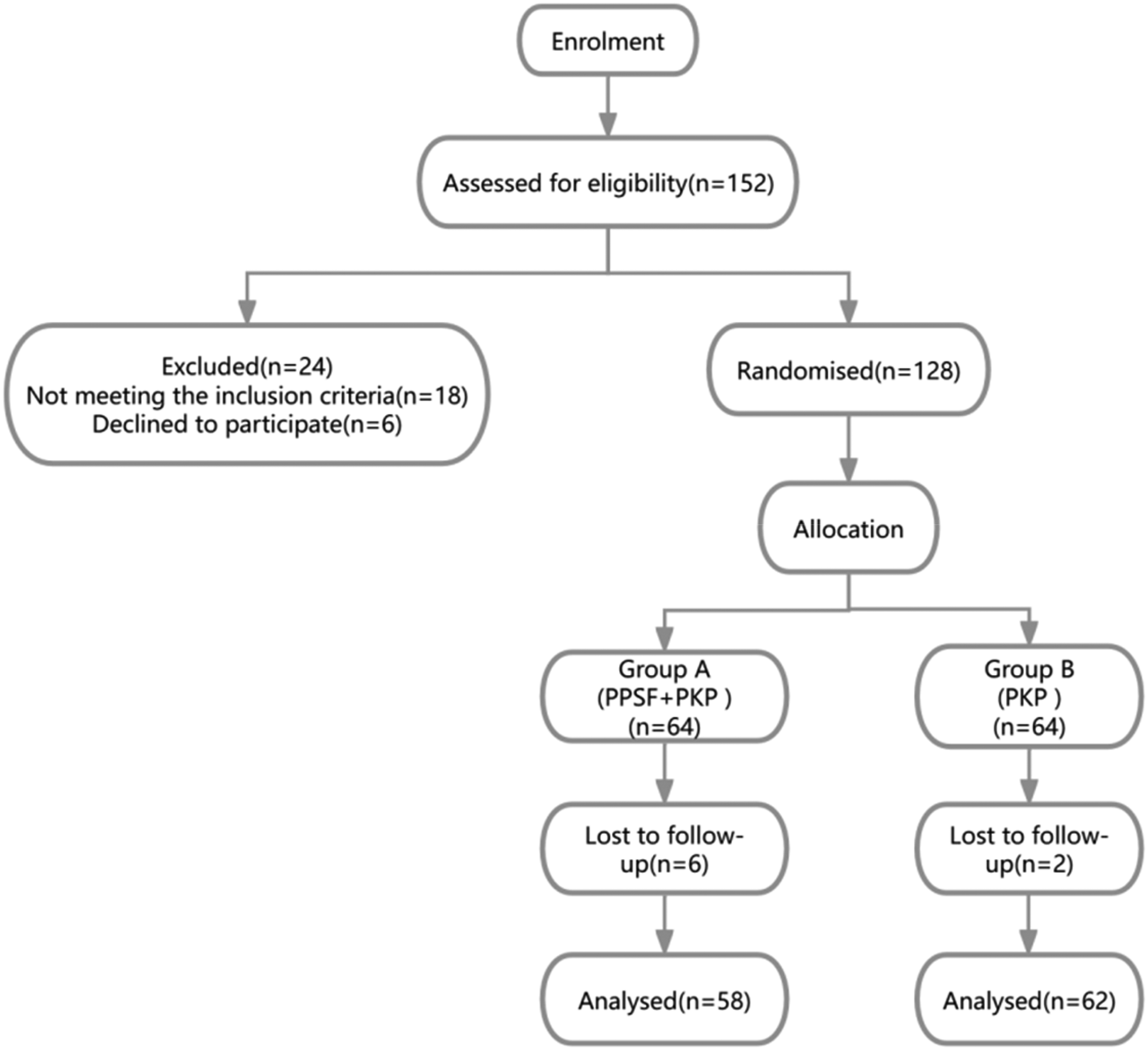
Flowchart of the selection process.
Study procedures
A computer-generated random sequence was used to allocate patients in a 1:1 ratio. The allocation sequence was created before patient enrollment using a web-based random number generator. The assignments were placed in sequentially numbered, opaque, sealed envelopes by an independent investigator uninvolved in patient assessment. Patients meeting the inclusion criteria were randomly assigned to either the intervention or control group. On the day of the surgery, after verifying eligibility and obtaining informed consent, the attending clinician opened the envelope to reveal the group assignment. The surgeon was then informed of the outcome, while the patient and outcome assessor were blinded to it.
The clinical trial was to be terminated if any serious adverse events occurred, such as nerve injury, vascular injury, allergic reaction, and unstable vital signs.
Surgical methods
After group allocation, surgery was performed in accordance with the designated procedure. All surgical procedures were performed by a consistent team of orthopedic surgeons.
Group A (PPSF + PKP)
First step. After general anesthesia was administered, the patient was placed prone on a radiolucent table with bolsters. Under C-arm fluoroscopy, the pedicle landmarks of the injured and adjacent vertebrae were identified. Following disinfection, four small incisions were made over the adjacent vertebrae. Trocar needles were advanced into the vertebral bodies via a pedicular trajectory, followed by guidewire insertion and working cannula placement. The pedicle tracts were dilated using a cannulated tapered drill. Four polyaxial pedicle screws (Stryker, USA) were inserted. Appropriate rods were placed bilaterally, and gradual distraction was applied to achieve fracture reduction before final tightening.
Second step. Under fluoroscopy, trocar needles were advanced into the injured vertebral pedicle with appropriate angulation. Lateral fluoroscopy confirmed needle tips below the depressed endplate. After guidewire insertion and working cannula placement, a cannulated tapered drill was used to create a tract to the sub-endplate region. A balloon was then inflated incrementally to 180 psi using a pressure-controlled system, and the target pressure was maintained for 60 s to create a cavity. Within 30 s of balloon deflation, prepared polymethyl methacrylate bone (PMMA) cement (Stryker, USA) was injected slowly during the transition from the stringy to the dough-like phase. Cement dispersion was monitored, and injection was stopped when cement approached the posterior vertebral margin, ensuring no leakage into the spinal canal. The working cannula was left in place for approximately 10 min to allow cement polymerization before removal (Figure 2).
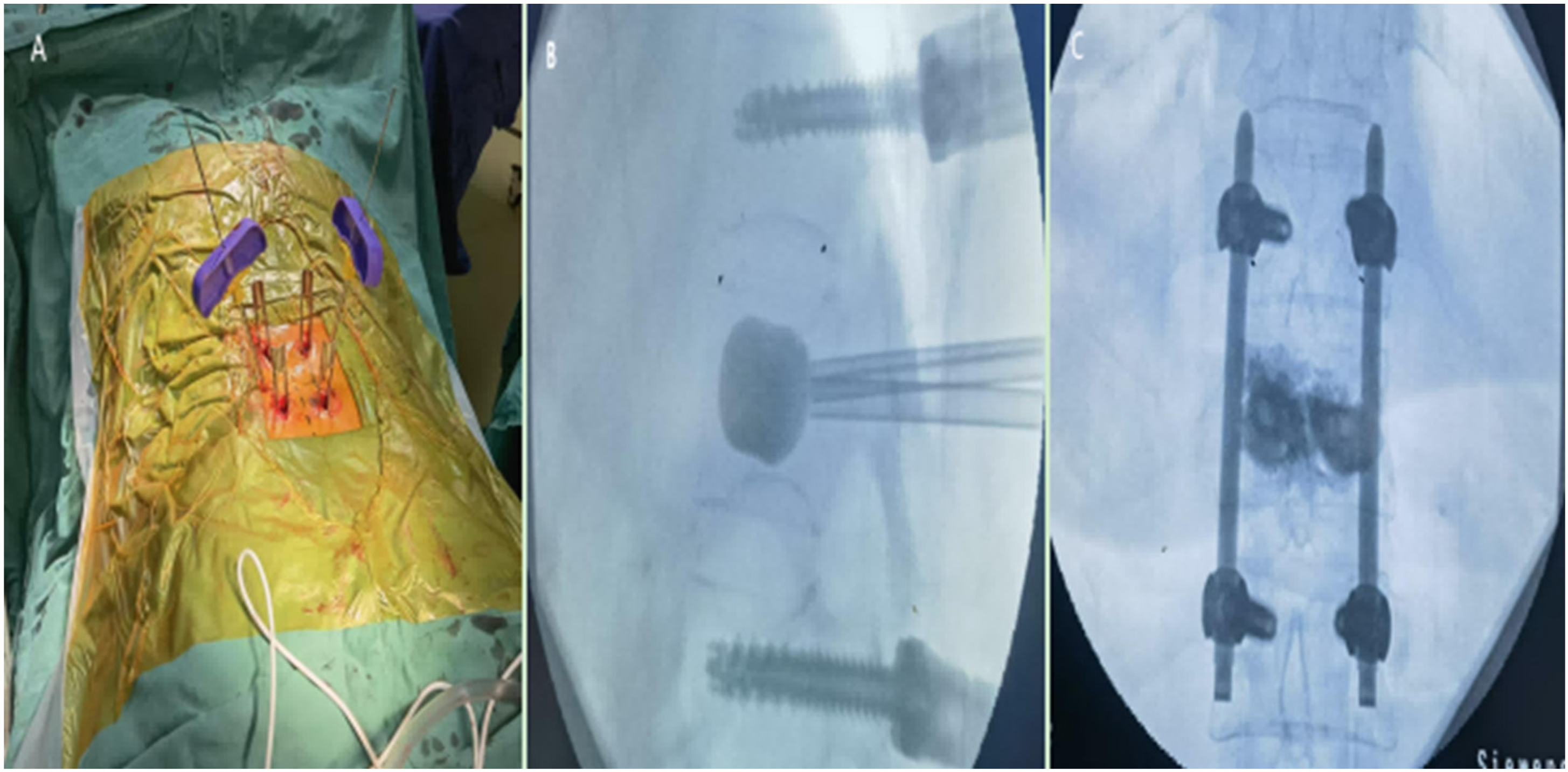
PPSF combined with balloon dilation-assisted reduction and PMMA augmentation for OVCFs. (a) Percutaneous pedicle screw placement and establishment of the balloon working cannula. (b) Balloon dilation-assisted reduction of the depressed endplate after PPSF. (c) Fluoroscopic image post-PPSF fixation and PMMA augmentation.
Group B (PKP)
The position of the injured pedicle was located and marked under G-arm fluoroscopy. PKP was performed in the same manner as in Group A. Prepared PMMA bone cement (Stryker, USA) was injected under C-arm fluoroscopic guidance. The working cannula was removed after the cement had completely polymerized.
Postoperative treatment
On the first postoperative day, patients were instructed to maintain strict supine positioning to prevent bleeding from wounds and reduce incision-related complications. Early rehabilitation protocols commenced with supervised isometric exercises targeting the lumbar paraspinal musculature and progressive lower limb elevation maneuvers to enhance neuromuscular activation. Assisted ambulation with external braces was initiated on postoperative day 2 under physiotherapist guidance. A standardized anti-osteoporotic regimen comprising oral calcitriol and calcium carbonate D3, along with a single intravenous infusion of zoledronic acid, was administered to both cohorts within the first postoperative week. Following discharge, patients were enrolled in a structured transition program incorporating graded resumption of daily activities. Systematic outpatient follow-ups were conducted at 1, 3, 6, 12, and 24 months postoperatively, including clinical assessments and radiographic evaluations.
Data evaluation
A senior clinician, blinded to group allocation, recorded and collected the clinical and radiographic data for each patient at 1, 3, 12, and 24 months postoperatively. Demographic and clinical parameters analyzed included sex, age, comorbidities, recent use of anti-osteoporosis drugs, BMD T-scores, preoperative hospitalization, cement volume, operative duration, and blood loss. Clinical outcomes were assessed preoperatively and postoperatively using the visual analog scale (VAS)and Oswestry Disability Index (ODI).14,15 All complications were documented, such as surgical site infections, neurological symptoms, PMMA leakage, and implant-related issues. Lateral radiographs were used to measure the Cobb angle and anterior vertebral height percentage (AVH%)/central vertebral height percentage (CVH%), calculated as (anterior or central height/mean height of adjacent vertebrae × 100%]. Secondary loss of anterior vertebral height (SLAVH), secondary loss of central vertebral height (SLCVH), secondary loss of Cobb angle (SLCA) were calculated between 2 days and 2 years postoperatively to evaluate maintenance of correction.
Statistical analyses
A sample size of 118 was required for the analysis to achieve adequate statistical power. Demographic and clinical characteristics were compared between the two groups. The Shapiro–Wilk test confirmed normality of the relevant continuous variables. Normally distributed data were expressed as mean ± SD. Categorical variables were expressed as frequencies and percentages. Continuous variables were compared between the two groups using independent-samples t-tests and within the same group (preoperative vs. postoperative) using paired-samples t-tests. Categorical variables were analyzed using the chi-square test or Fisher's exact test. All analyses were performed using the Statistical Package for Social Sciences (SPSS) software (version 19.0, IBM Corp.), with a two-tailed p-value <0.05 considered statistically significant. Unpaired Student’s t-test was used for comparing two independent groups. For comparisons of preoperative and postoperative data within the same group of patients, we used paired Student's t-tests.
Results
General data
In total, 128 patients were initially assigned to the two study cohorts. After excluding 8 patients due to loss to follow-up, 120 patients with OVCF were ultimately included in the final analysis. Both groups exhibited comparable BMD and preoperative hospitalization duration. The PMMA volume was 5.86 ± 1.25 mL in Group A and 6.42 ± 1.12 mL in Group B. There was no significant difference in age, sex, BMD, fracture level, preoperative hospital duration, or PMMA volume between the two groups (Table 1). Comparative analysis of surgical parameters revealed statistically significant intergroup differences. The operative duration was substantially longer in Group A (68.79 ± 8.24 min vs. 31.94 ± 9.38 min); Group A also exhibited greater intraoperative blood loss (27.76 ± 6.96 mL vs. 14.84 ± 6.20 mL). Both comparisons demonstrated statistical significance (p < 0.001; Table 1).
Comparison of the basic characteristics of the participants of Groups A and B.
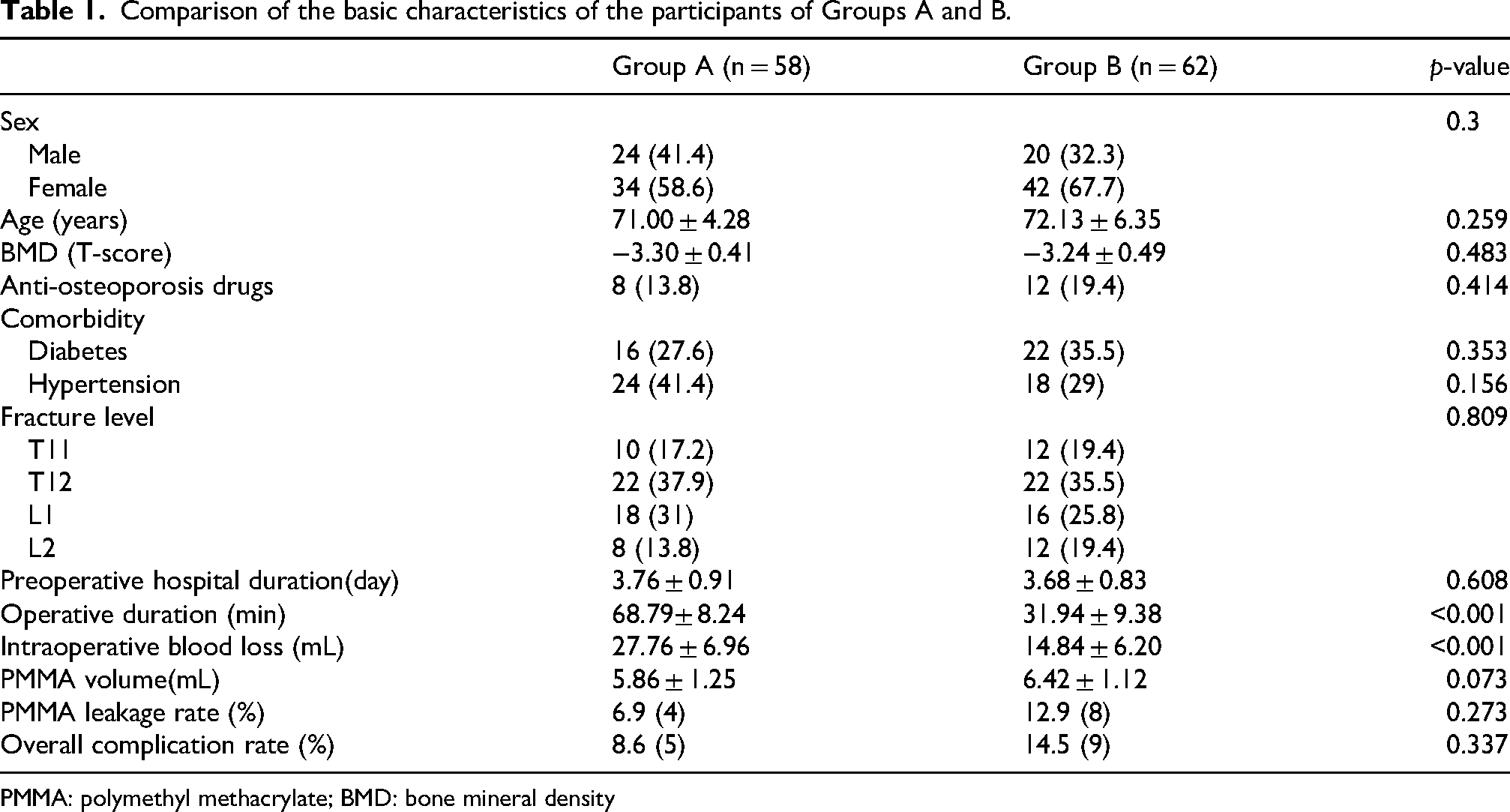
PMMA: polymethyl methacrylate; BMD: bone mineral density
Radiographic data
Both cohorts demonstrated significant improvements in the Cobb angle, AVH%, and CVH% at postoperative 2 days, 3 months, 1 year and 2 years compared with the preoperative baseline measurements (p < 0.05) (Table 2, Figures 3 and 4). Intergroup comparisons revealed superior radiographic parameters in Group A across all timepoints (Figures 5 and 6). Group A exhibited significantly lower secondary loss of Cobb correction angle (mean difference: 1.12°; 95% confidence interval (CI): 0.63°–1.49°), SLAVH% (mean difference: 2.66%; 95% CI: 1.97%–3.29%), and SLCVH% (mean difference: 1.15%; 95% CI: 0.42%–1.58%) than Group B during 2 years of follow-up (p < 0.05) (Table 2).
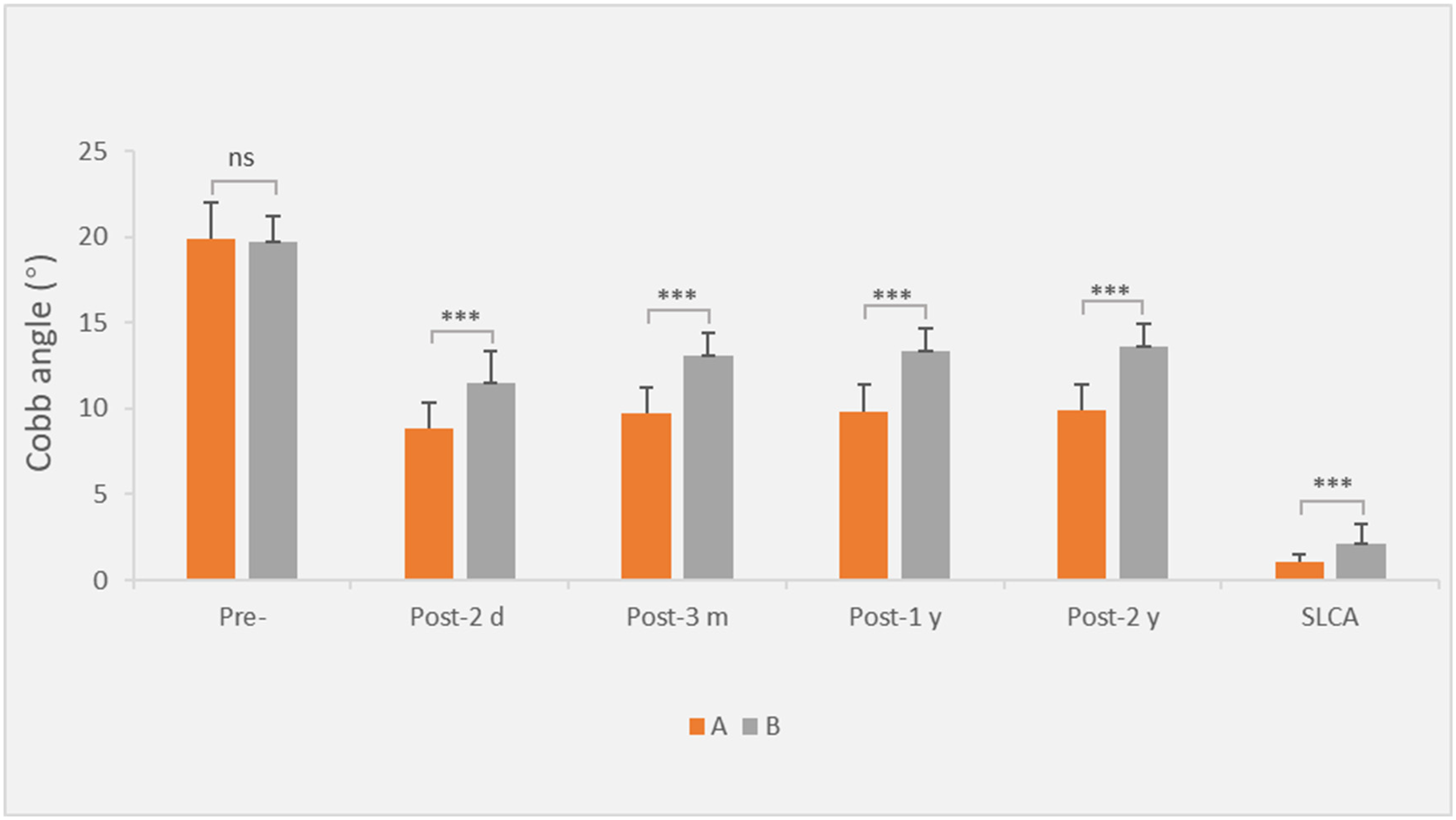
Bar chart showing the Cobb angle (°) of the two groups at preoperative and postoperative time points.
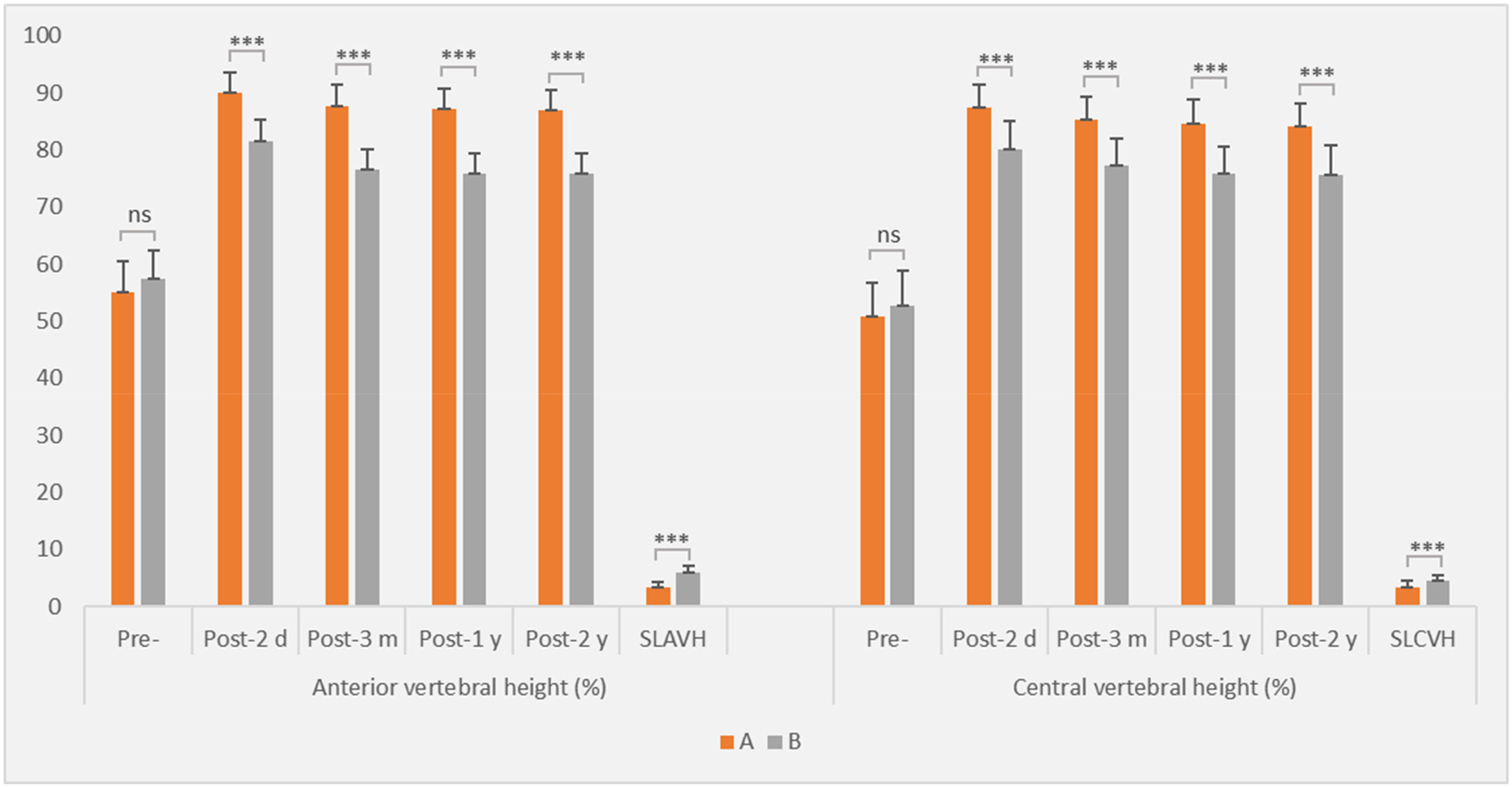
Bar chart showing injured vertebral body height (%) in the two groups at preoperative and postoperative time points.
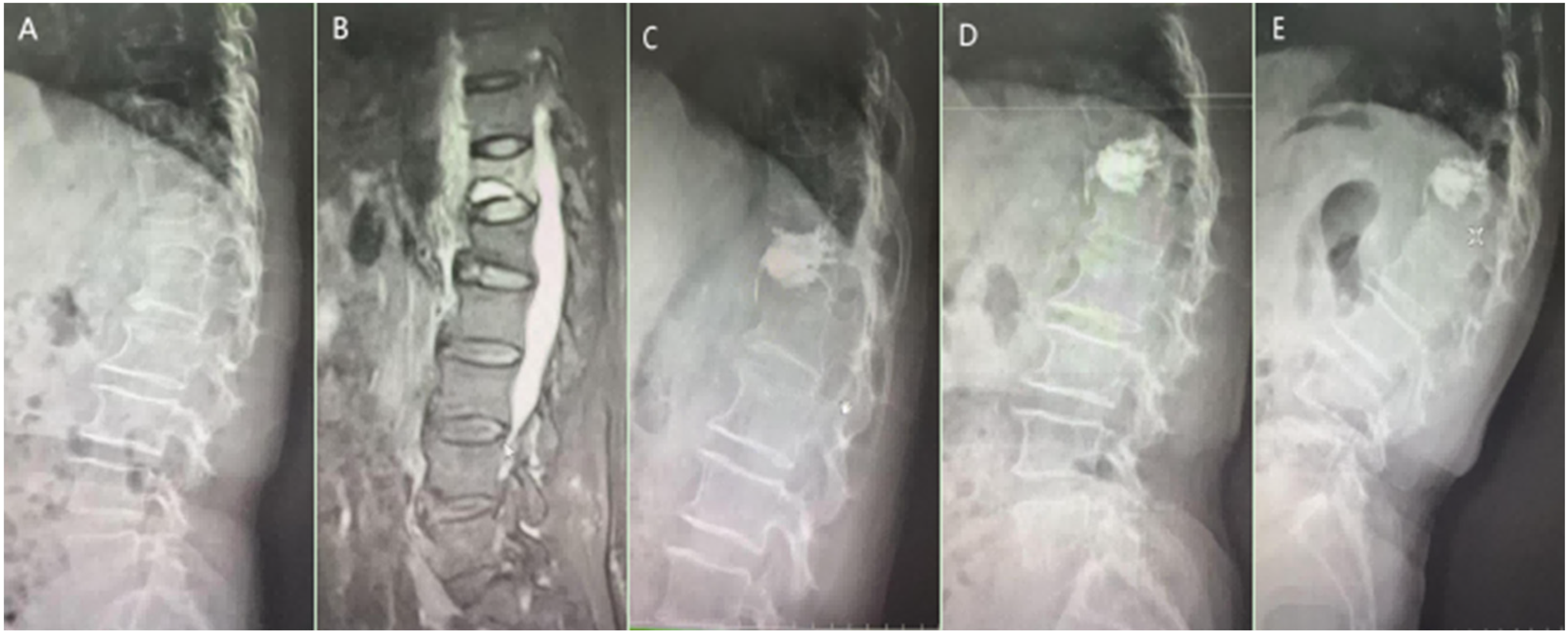
An 83-year-old female patient with an osteoporotic T12 vertebral compression fracture was treated with PKP. (a) Preoperative lateral radiograph demonstrates T12 vertebral fracture with significant compression.(b) MRI reveals an acute T12 vertebral compression fracture. (c) Postoperative 2-day lateral radiograph confirms unsatisfactory vertebral height restoration. (d) Postoperative 3-month lateral radiograph shows secondary loss of correction compared with baseline. (e) Postoperative 2-year lateral radiograph reveals progressive secondary loss in the injured vertebra.
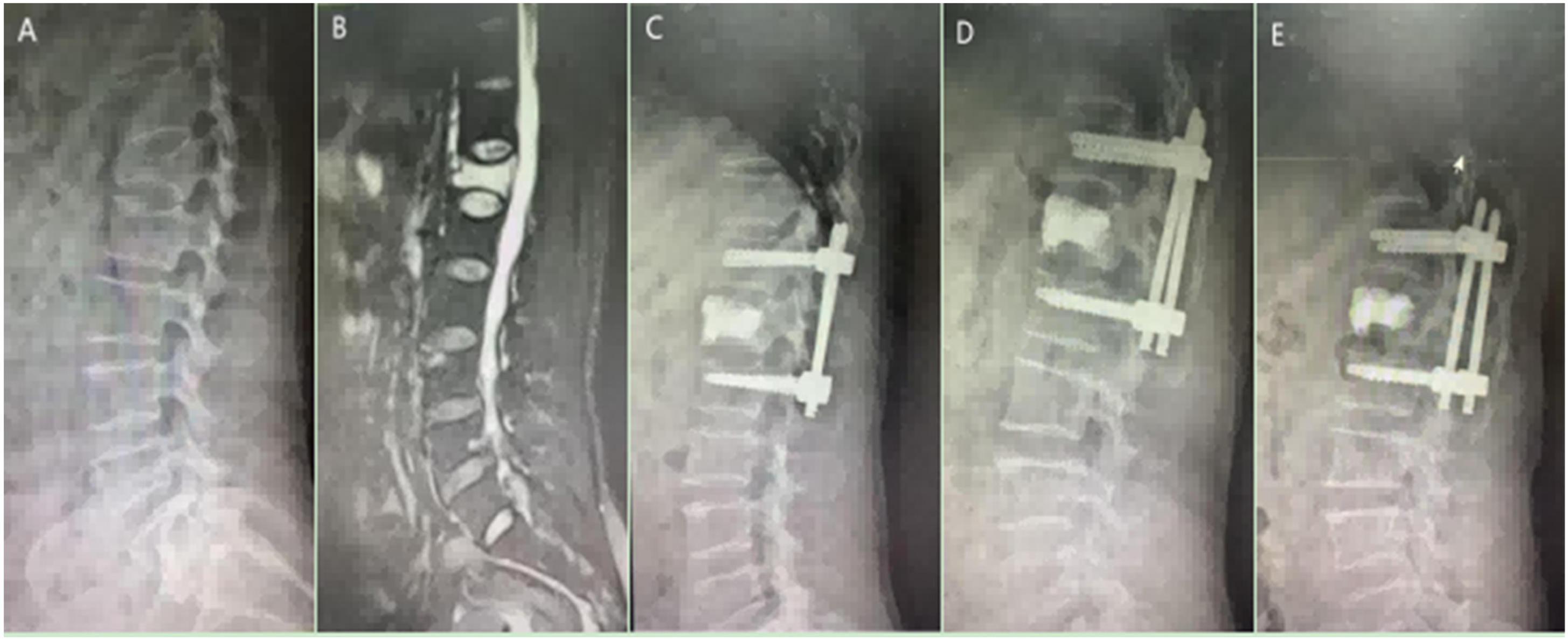
A 78-year-old female patient with an osteoporotic L1 vertebral compression fracture with endplate depression was treated with PPSF combined with PKP. (a) Preoperative lateral radiograph demonstrates L1 vertebral fracture with significant compression and endplate depression. (b) MRI reveals an acute L1 vertebral compression fracture. (c) Postoperative 2-day lateral radiograph confirms satisfactory vertebral height restoration and kyphosis correction. (d) Postoperative 3-month lateral radiograph shows maintained ideal vertebral height. (e) Postoperative 2-year lateral radiograph reveals no significant secondary loss of restored vertebral height.
Comparison of the Cobb angle (°) and injured vertebral body height (%) between the two groups.

SLCA: secondary loss of Cobb angle; SLAVH: secondary anterior vertebral height loss; SLCVH: secondary central vertebral height loss; pre-: preoperative; post-2 d: postoperative 2 days; post-3 m: postoperative 3 months; post 1-y: postoperative 1 year.
significant differences compared with preoperative data, p < 0.05.
Clinical data
Postoperative clinical assessments revealed favorable pain control outcomes in both groups. No patient reported severe pain (VAS score ≥ 7) or significant sleep disturbance secondary to pain. Comparative analysis demonstrated substantial improvements from baseline in both VAS score and ODI values at all postoperative intervals (p < 0.05). However, intergroup comparisons revealed no statistically significant differences in the VAS scores (p > 0.05). In contrast, functional assessment showed that the ODI values were significantly lower in Group A from postoperative 3 months to 2 years (Table 3, Figure 7).
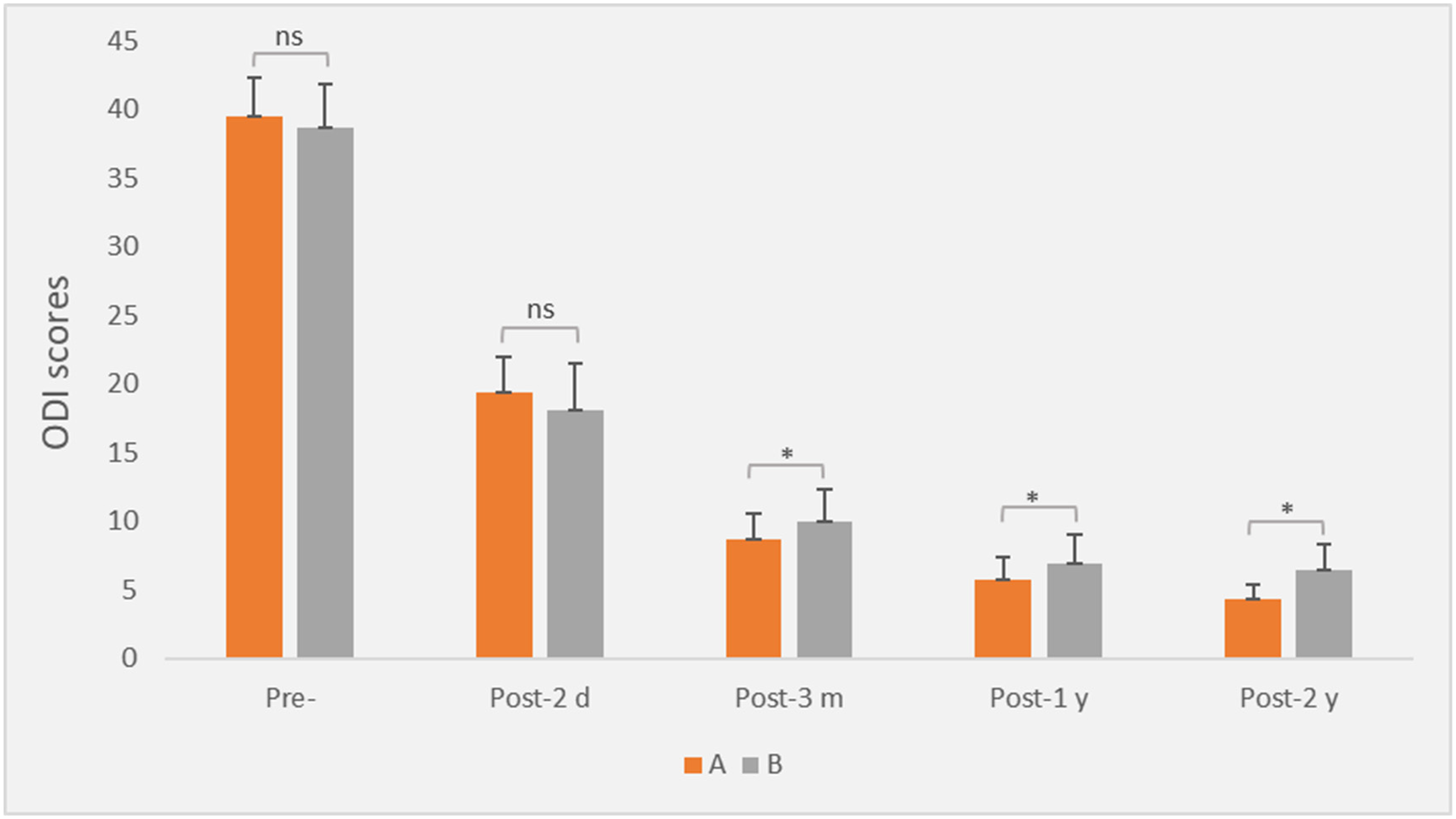
Bar chart showing the ODI values of the two groups at preoperative and postoperative time points.
Comparison of VAS and ODI scores between the two groups.
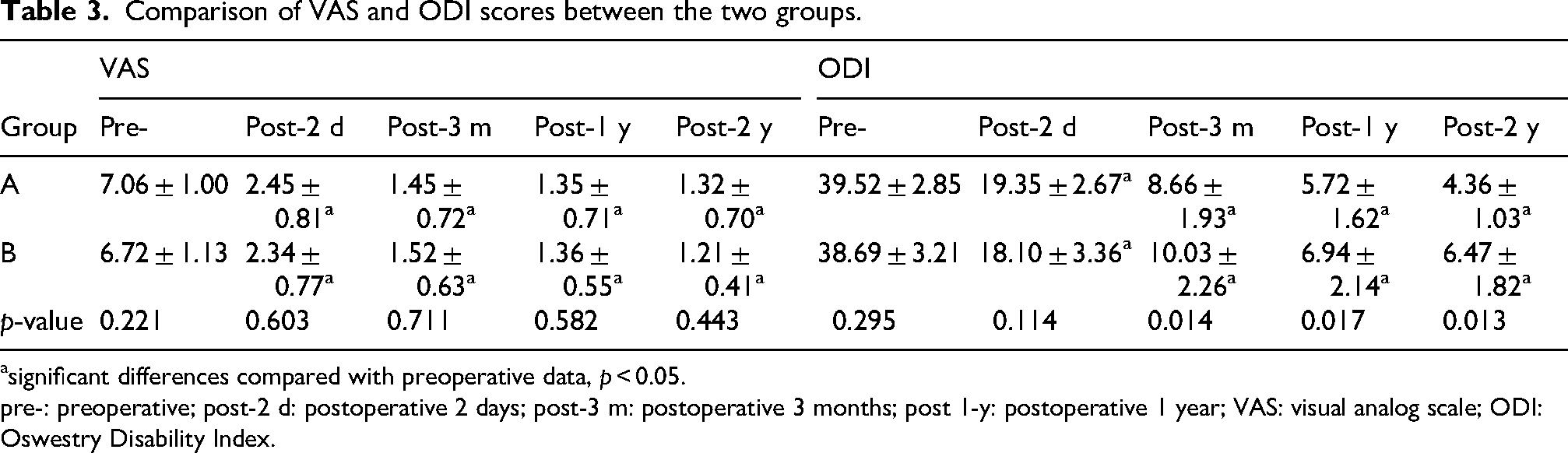
significant differences compared with preoperative data, p < 0.05.
pre-: preoperative; post-2 d: postoperative 2 days; post-3 m: postoperative 3 months; post 1-y: postoperative 1 year; VAS: visual analog scale; ODI: Oswestry Disability Index.
Complication data
All surgical interventions were successfully completed without surgical site infections, nerve injuries, or cardiovascular events. During the 24-month follow-up period, no refractures or adjacent fracture events were documented in either group. Perfect implant integrity was maintained in Group A with zero cases of implant failure. The overall complication rates were 8.6% (5/58) for Group A and 14.5% (9/62) for Group B, with a risk difference of −5.9% (95% CI: −17.3% to 5.5%, p > 0.05) (Table 1). Specifically, the PMMA leakage rates were 6.9% (4/58) in Group A and 12.9% (8/62) in Group B, with a difference of −6.0% (95% CI: −16.6% to 4.6%), indicating no statistically significant intergroup difference (p > 0.05) (Table 1). Notably, all leakage cases remained clinically asymptomatic and required no additional intervention.
Among patients with comorbid hypertension and/or diabetes in both groups, one case of postoperative delirium occurred in Group A and one case of recurrent postoperative cerebral infarction occurred in Group B. The difference in these complication rates was not statistically significant (p > 0.05), suggesting that Group A was not associated with an increased perioperative morbidity risk, despite its longer operative duration and greater blood loss. Both patients recovered after effective treatment.
The quantitative superiority demonstrated in our results suggests that PPSF combined with PKP provides enhanced fracture reduction quality, significantly reduced secondary loss of correction, and improved functional outcome over time compared with single PKP techniques.
Discussion
Although vertebral augmentation achieves immediate vertebral stabilization and pain relief through bone cement polymerization, its efficacy remains confined to local stiffness restoration without addressing global spinal alignment and anatomical reconstruction. For OVCFs with endplate depression, the use of only vertebral augmentation techniques is associated with multiple biomechanical deficiencies.
First, standalone vertebral augmentation may result in insufficient deformity correction. Studies have demonstrated that PVP for OVCFs achieves only modest Cobb angle reduction from 18.1° preoperatively to 15.1° postoperatively, with the percentage improvement in anterior vertebral height of 49.8% to 63.4%. 16 Huang et al. reported anterior vertebral height restoration from 49% to 80% after PKP. 17 Our comparative analysis revealed a significantly smaller Cobb correction angle in the PKP monotherapy group (8.83° ± 1.49°) than in the multimodal intervention group (11.47° ± 1.86°), highlighting the insufficiency of isolated vertebral augmentation in restoring sagittal balance. Second, intravertebral clefts compromise mechanical support. Xiong et al. confirmed, based on their analyses of 48 cases of postoperative secondary fractures, that disruption of endplate integrity increases collapse risk by 3.2-fold. 18 Cyclic loading in flexion and extension on fractured osteoporotic vertebra can generate an intravertebral cleft, leading to abnormally elevated stress in the cortical bone adjacent to the endplate in fractured vertebra. 19 Third, the cement typically exhibits a cloud-like dispersion pattern within the vertebral body. Progressive osteoporotic bone trabecular degeneration and expansion of the intravertebral cleft reduce cement–bone interfacial bonding strength, generating micromovement that elevates re-collapse risk. Fourth, depressed endplates significantly increase cement injection resistance and hinder sub-endplate diffusion. This maldistribution induces uneven stress distribution, amplifying postoperative collapse susceptibility.
Standalone PPSF in osteoporotic patients is limited by poor screw anchorage and stress concentration at screw–bone interfaces, exacerbated by diminished bone mass and mechanical strength. These factors increase the risk of implant-related complications such as insufficient intraoperative deformity correction, screw loosening, and secondary fracture. These adverse events primarily stem from multifactorial stress concentration and failure of biomechanical compensation mechanism. First, endplate depression fractures, especially the biconcave type, often render traditional posterior vertebral body distraction ineffective in restoring middle column height. As the anterior and middle columns bear approximately 80% of axial loads, this structural deficiency elevates the risk of screw fatigue fractures and consequently predisposes the vertebra to progressive secondary height loss. Second, the “suspension effect” in short-segment fixation creates significant stress concentration and torsional moments, particularly in the lower lumbar spine where peak stress can reach 2–3 times the physiological levels.20,21 This construct–load mismatch fails to provide sufficient stability for high-load fractures. In contrast, utilizing the middle pedicle screws as the forward driving point can generate a robust string force for effective reduction and kyphosis correction. 22 Furthermore, implant stability is influenced by BMD and load-bearing cross-sectional area. Diminished BMD significantly impairs screw pullout strength. 23 Finally, the use of polyaxial screws introduces micromotion and provides inferior biomechanical properties compared with monoaxial designs, including reduced compression yield load (302.5 ± 42.3 N), elastic stiffness (30.8 ± 4.1 N/mm), and yield strength (9.3 ± 1.5) MPa, diminishing both intraoperative reduction efficiency and postoperative maintenance of correction. 24 Additionally, residual intravertebral clefts often persist after fracture reduction, further compromising stability.
The delayed-onset secondary vertebral collapse following standalone PPSF in OVCF patients is primarily attributed to chronic bone metabolic imbalance and progressive structural deterioration. Mechanistically, stress-shielding effects within the instrumented segments reduce biomechanical stimulation, initiating a self-sustaining cycle of negative bone remodeling that exacerbates osteoporotic progression. Particularly, the intravertebral vacuum cleft (IVVC) is clinically significant due to its association with vertebral re-collapse. These pathological vacuum clefts not only occupy critical osteogenic space but also catastrophically diminish load-bearing capacity. This biomechanical compromise predisposes to vertebral re-collapse in the anterior and central regions. 25 A retrospective study has demonstrated significantly greater vertebral height loss in patients with implant removal at 1 year postoperatively compared with that in non-implanted controls. 26 Clinical evidence has demonstrated substantial prevalence of IVVC, with Xu et al. reporting a 34.7% incidence at the 6-month follow-up, which persisted at 22.4% at the final assessment. 27 Osterhouse et al. reported a case of delayed vertebral collapse with IVVC. 28
These findings advocate for a stratified therapeutic paradigm integrating biomechanical restoration and global sagittal alignment correction in OVCFs management. Recent studies have substantiated that the combined application of PPSF with PVP effectively reconstructs anterior and middle columns of the vertebral body, enhances load-bearing capacity, and reduces the risk of progressive correction loss postoperatively, demonstrating both safety and efficacy.29,30 In a long-term follow-up study by El Saman et al., this protocol achieved remarkable outcomes in vertebral fractures in older adults, with SLCA markedly minimized to 1.1°. 31 However, most of these studies were retrospective in nature, and the value of balloon dilation-assisted reduction of depressed endplates in PPSF for OVCFs has not been systematically reported. Therefore, this study prospectively analyzed the efficacy, including improved vertebral height restoration (anterior 90.06% ± 3.50%, central 87.43% ± 3.96%), significant Cobb correction angle (8.83° ± 1.49°), less secondary losses of correction (Cobb angle 1.04° ± 0.45°, anterior height 3.20% ± 0.97%, central height 3.30% ± 1.10%), and lower ODI values. In addition, no instances of implant loosening, refracture, or adjacent fracture were observed in the study cohort.
PPSF combined with balloon dilation-assisted endplate reduction and PMMA-augmented vertebra significantly improves the therapeutic outcomes in OVCFs with endplate depression by enhancing mechanical stability, restoring three-dimensional vertebral height and sagittal balance, and reducing complication rates. PMMA cementation restores anterior and middle column continuity, reestablishing anterior load-bearing capacity, while the posterior pedicle screw-rod system provides dynamic stabilization, redistributing spinal stress loads.
Through synergistic “inside-out” balloon dilation-assisted reduction and cantilever mechanisms, the strategy enables effective restoration of middle column height and kyphosis correction, with sustained anatomical alignment and minimal long-term correction loss. In addition, this strategy can also reduce complication rates. Prophylactic PMMA injection reduces the risk of vertebral collapse in high-load or type-A3 fractures by reinforcing the cancellous bone and preventing the development of an intravertebral vacuum cleft (“vacuum sign”). Balanced force transmission decreases the stress of screw, significantly lowering implant failure rates.
Although the PMMA leakage rates in the two groups were not statistically significant in this study (p = 0.273), the near twofold higher leakage rate in the PKP group (12.9% vs. 6.9% in the PPSF + PKP group) warrants clinical discussion. This may be because the PKP group has higher intravertebral pressure and requires greater cement injection pressure, which may account for its higher leakage rate. In contrast, in the PPSF + PKP group, pedicle screw reduction of the vertebral body reduced intravertebral pressure. Furthermore, the lack of statistical significance regarding PMMA leakage rates, which may be attributable to the small sample size, does not negate a potentially clinically meaningful difference.
During the procedure, a potential technical interaction between PPSF and the subsequent PKP may occur, which could affect balloon positioning or cement distribution. Based on our clinical experience, appropriately reducing the abduction angle of the PPS trocar needle under fluoroscopic guidance, slightly shifting the PKP entry point laterally, and moderately increasing its abduction angle can often prevent interference. Although performing reduction after cement augmentation is not an absolute contraindication, it must be performed with extreme caution. Under real-time fluoroscopic monitoring, minimal force should be applied to achieve millimeter-level adjustments. The objective of such distraction is primarily to make a slight adjustment and maintain tension rather than aggressively pursue perfect restoration of vertebral height. In cases of severe interference, open surgery under direct visualization may be considered to adjust the trocar trajectory.
Limitations
This study has certain methodological constraints requiring systematic refinement in subsequent research. First, the relatively small sample size resulted in suboptimal statistical power, which may have compromised the reliability of certain outcome assessments and the evaluation of rare complications (e.g. PMMA fragmentation incidence). Second, the relatively short-term follow-up period was insufficient for assessing long-term biomechanical consequences such as adjacent segment degeneration, and the functional impact of multi-segment fixation. Third, the technical complexity of this procedure required longer operative times and greater resource utilization, resulting in higher ancillary costs. This underscores the necessity of a formal cost-effectiveness analysis to better inform clinical decision-making. Fourth, although the overall loss to follow-up rate (8/128, 6.25%) was relatively low and baseline characteristics remained comparable between the two groups, the higher loss to follow-up rate (8/64, 9.38%) in Group A could have introduced attrition bias, and this imbalance may be related to differences in mobility, pain levels, or patient compliance. Finally, the single-center design may have introduced selection bias and limited the generalizability of the findings. Validation through large-scale, prospective, multicenter studies involving diverse ethnic populations is warranted.
Conclusion
The comprehensive approach of balloon dilation-assisted endplate reduction, cement augmentation, and PPSF led to improvements in vertebral stability, reduction, and functional status for severe OVCFs with endplate depression and kyphosis, with the added benefit of less correction loss. This minimally invasive approach can facilitate recovery and help achieve favorable clinical outcomes.
Footnotes
Ethical approval
This study was approved by Nanjing Luhe People’s Hospital Ethical Committee (No. LHLL2020–020). Written informed consent was obtained from all participants prior to enrollment, and the study adhered to the Consolidated Standards of Reporting Trials (CONSORT) guidelines and Helsinki Declaration (as revised in 2024).
Author contributions
DZ: formal analysis, writing–original draft, and writing–review & editing; XKY: writing–original draft; MX: data curation and software; XZ: data curation and visualization; XFY: software and writing–review & editing; and CKM: project administration and writing–review & editing. All authors have read and approved the final manuscript.
Funding
The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the Nanjing Medical Science and Technical Development Foundation (Grant Number YKK23237).
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are available from the corresponding author on request.