
Abstract
Background
Effective pain management is critical following hemorrhoidectomy due to the dense nerve distribution in the anorectal region. Although compound methylene blue and liposomal bupivacaine are both used for postoperative analgesia, their comparative efficacy and safety profiles have not been systematically evaluated. This study aimed to compare the analgesic efficacy, opioid-sparing effects, and safety of liposomal bupivacaine with compound methylene blue in patients undergoing mixed hemorrhoidectomy.
Methods
This was a single-center, prospective observational cohort study involving 150 patients undergoing elective hemorrhoidectomy for stage III–IV mixed hemorrhoids. Patients were allocated into two groups: (a) the compound methylene blue group (n = 75) and (b) the liposomal bupivacaine group (n = 75). Postoperative pain was assessed using the numerical rating scale at rest over 72 h. Primary outcomes included cumulative pain scores, time to first rescue analgesia, and total rescue opioid consumption. Secondary outcomes included patient satisfaction, recovery metrics, and adverse events.
Results
The liposomal bupivacaine group demonstrated significantly lower cumulative pain scores over 72 h than the compound methylene blue group. Although the compound methylene blue group demonstrated marginally better pain control in the immediate postoperative period, liposomal bupivacaine provided superior and stable analgesia from 12 to 72 h. The proportion of patients who required rescue opioids was significantly lower in the liposomal bupivacaine group than in the compound methylene blue group. Patient satisfaction was significantly higher in the liposomal bupivacaine group. Furthermore, the incidence of adverse events was significantly lower in the liposomal bupivacaine group than in the compound methylene blue group.
Conclusions
Single-dose perianal infiltration of liposomal bupivacaine provides superior and more sustained postoperative analgesia than that of compound methylene blue in patients who have undergone mixed hemorrhoidectomy. Liposomal bupivacaine significantly reduces rescue opioid requirements, delays the need for supplemental analgesia, and improves patient satisfaction with a favorable safety profile.
Introduction
Hemorrhoids are a common and frequently occurring condition unique to humans, with grade III–IV mixed hemorrhoids often requiring surgical treatment. Due to the dense nerve distribution in the anal area and the direct stimulation of sensory nerve endings around the anus caused by surgical trauma, postoperative pain is a major challenge for these patients. 1 Approximately 75% of patients undergoing anal surgery reportedly experience moderate to severe pain. 2 This pain not only causes significant discomfort but can also trigger reflexive anal sphincter spasms, further intensifying the pain and potentially leading to complications such as urinary retention. Therefore, pain management after mixed hemorrhoid surgery is crucial, as uncontrolled pain may result in delayed recovery, increased risk of opioid dependence, and decreased patient satisfaction.3,4
The surgical management of hemorrhoids, particularly for grades III and IV, often involves open excisional hemorrhoidectomy (Milligan–Morgan procedure). Although highly effective in eradicating the pathology, this traditional approach is frequently associated with significant postoperative pain and discomfort, which remains a major limitation to patient satisfaction and rapid recovery. 5 The impact of this pain extends far beyond the surgical site; it profoundly disrupts patients’ quality of life by affecting basic functions such as sitting, ambulation, and sleep. This nociceptive burden can also trigger reflexive anal sphincter spasms, further complicating the healing process and potentially leading to urinary retention or delayed bowel function.
In the current era of enhanced recovery after surgery (ERAS), there has been a paradigm shift toward minimizing surgical trauma and prioritizing functional preservation. Consequently, the pursuit of superior analgesia is not solely about comfort, but represents a critical component of functional rehabilitation, enabling earlier mobilization and restoration of normal physiological activities. Furthermore, the landscape of hemorrhoidal treatment is evolving with the advent of minimally invasive techniques, such as laser hemorrhoidoplasty, which aim to reduce tissue damage and postoperative morbidity. However, for advanced hemorrhoidal disease requiring conventional excision, optimizing perioperative analgesia remains a cornerstone of clinical practice.
In recent years, local anesthetics such as bupivacaine, its liposomal formulation (liposomal bupivacaine (LB)), and methylene blue have garnered significant attention in postoperative pain management. These drugs provide long-lasting relief through different mechanisms; however, their efficacy, mechanisms, and suitability for patients undergoing hemorrhoidectomy have not been systematically compared. Herein, we elaborate on the analgesic mechanisms, advantages and disadvantages, and clinical evidence regarding the use of these three drugs in patients undergoing hemorrhoid surgery, providing a theoretical foundation for subsequent clinical research. First, bupivacaine is a classic long-acting local anesthetic that inhibits nerve conduction by blocking sodium channels, thereby reducing pain signal transmission. Its advantages include rapid onset and reliable effect, making it suitable for intraoperative and postoperative baseline analgesia.6,7 However, the main drawback of standard bupivacaine is its relatively short duration of action (typically 6–8 h), which often necessitates frequent supplementation with analgesics or opioids. 8 For example, studies on hemorrhoid surgery have shown that bupivacaine can significantly reduce postoperative visual analog scale (VAS) scores; however, its analgesic duration is limited, leading to increased opioid consumption.9,10 Systematic analyses have indicated that the analgesic effect of bupivacaine varies, depending on the administration method; for instance, although effective in transversus abdominis plane blocks, it still requires adjunct medications to maintain prolonged relief, highlighting its limitations as a standalone therapy.6,7,8
LB is an improved formulation of standard bupivacaine that uses liposomal encapsulation technology to extend drug release and achieve sustained analgesia. The specific mechanism involves the liposomal structure delaying the local diffusion of bupivacaine, thereby providing a long-lasting anesthetic effect. Its advantages include an extended duration of action (up to 72 h), significant reduction in postoperative opioid consumption, and potential benefits in high-risk surgeries such as hemorrhoidectomy.7,11 For example, a randomized controlled trial has shown that patients undergoing hemorrhoid surgery who received LB had significantly reduced opioid prescriptions and lower pain scores than those treated with standard bupivacaine. 11 Additionally, in wound infiltration or nerve blocks, LB use has demonstrated non-inferiority to bupivacaine combined with epinephrine. 7 However, its drawbacks include higher cost, complex formulation preparation, and, in some studies (such as meta-analyses), similar overall analgesic effects compared with standard bupivacaine, failing to demonstrate absolute superiority in all clinical scenarios. For instance, there was no significant difference in the pain score trajectories between the LB and control groups, suggesting that its effect is underestimated or influenced by confounding factors. 7 Therefore, as a novel formulation, LB requires further evaluation of its cost-effectiveness and long-term benefits in managing postoperative pain following mixed hemorrhoid surgery.
Methylene blue is a unique local anesthetic whose pain-relief mechanism is based on anti-inflammatory and neuroregulatory effects. It reduces nitric oxide (NO) production and inhibits nerve action potential transmission, thereby blocking pain conduction pathways. It effectively alleviates inflammatory responses and nerve hypersensitivity, which helps relieve postoperative pain. Its advantages include high safety and minimal adverse effects (such as no significant postoperative complications), making it widely used in mixed hemorrhoid surgery. 12 For example, studies on hemorrhoid surgery have shown that both 0.1% and 0.2% methylene blue significantly reduce VAS pain scores, particularly within the first 7 days after surgery, with the 0.1% concentration demonstrating higher safety (lower complication rates). 13 Additionally, the flexible dosing of methylene blue allows easy integration into local anesthesia protocols; for instance, intradermal injections can provide analgesic effects comparable with those of opioids with negligible adverse effects. 14
However, its drawbacks include uncertainty regarding the optimal concentration and the fact that its mechanism is more suitable for chronic or neuropathic pain rather than all acute pain scenarios. 13 Studies have also indicated that methylene blue's effectiveness after mixed hemorrhoid surgery is limited to postoperative days 1–7, after which its effect diminishes, necessitating combined use with other therapies for sustained relief.13,14 Clinically, innovative combinations have been developed, such as compound methylene blue injections containing both bupivacaine and methylene blue, which provide long-lasting analgesia through dual mechanisms. For example, in hip replacement surgery studies, a comparison of the use of amide local anesthetics alone versus in combination with methylene blue has shown that the combination offers better immediate and long-term benefits. 15
However, in the management of postoperative pain following mixed hemorrhoid surgery, existing studies lack a systematic comparison between LB and compound methylene blue. The research gaps are mainly reflected in several aspects: first, insufficient evaluation of advantages and disadvantages—methylene blue has a high safety profile but requires individualized concentration optimization, whereas LB reduces opioid dependence but is costly and shows variable efficacy.8,13 Second, heterogeneity in existing evidence—a meta-analysis on LB has shown inconsistent results (I2 = 48%), indicating that differences in study design or populations may affect conclusions; meanwhile, randomized trials on methylene blue are often limited by small sample sizes and lack multicenter validation. 8 Therefore, this study aimed to bridge these gaps by systematically comparing the relative effectiveness of compound methylene blue and LB in managing pain after mixed hemorrhoid surgery. The extended discussion evaluated how different administration protocols (such as concentration and timing) impact analgesic quality, integrating mechanistic advantages to achieve personalized treatment. Based on current studies, methylene blue's anti-inflammatory mechanism may be better suited for hemorrhoids with high postoperative inflammation, whereas the long-acting properties of LB can optimize resource allocation. Through prospective observational analysis, this study further quantified pain scores, opioid consumption, and safety endpoints to provide an evidence-based foundation for clinical guidelines.
Materials and methods
Research design
Study type. This study was designed as a prospective observational cohort study or a prospective observational analysis of prospectively maintained data. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 16 We reviewed data from a prospectively collected database of patients who underwent elective hemorrhoidectomy (Milligan–Morgan procedure) at our institution between December 2024 and March 2026. Although data extraction was performed retrospectively, patient enrollment, surgical procedures, and initial data recording followed a standardized prospective protocol.
Group allocation. Patients were allocated into two groups based on the anesthetic agent administered during surgery. To minimize selection bias, consecutive patients meeting the inclusion criteria were enrolled. The allocation was determined by the attending surgeon's preference based on drug availability and patient-specific factors (e.g. allergy history), not randomly. Despite the observational nature of the study, outcome assessors and data analysts were blinded to the group assignments during the statistical analysis phase.
Study duration. Assessments were performed immediately postoperatively, with a follow-up period of 14 days, which covered the peak pain phase and recovery period.
Sample size calculation. Based on previous similar studies, it was estimated that 75 patients per group were required to achieve statistical power for the primary outcome (VAS pain score) with α =0.05 and power =80%.
Inclusion criteria. The inclusion criteria were as follows:
Age 18–75 years and diagnosis of stage III or IV mixed hemorrhoids requiring elective hemorrhoidectomy; Standardized hemorrhoidectomy performed under spinal anesthesia as the surgical method; Absence of severe systemic diseases (such as liver or kidney dysfunction and cardiovascular diseases), American Society of Anesthesiologists (ASA) class I–II; No history of allergy to amide local anesthetics or methylene blue.
Exclusion criteria. The exclusion criteria were as follows:
Pregnant or breastfeeding women; History of chronic pain or long-term use of opioid medications; Severe liver or kidney dysfunction; Glucose-6-phosphate dehydrogenase (G6PD) deficiency or hypersensitivity to methylene blue/amide local anesthetics; Use of nonsteroidal anti-inflammatory drugs (NSAIDs) or corticosteroids within 72 h preoperatively.
Immediately after the surgery, all patients were administered perianal subcutaneous injections by the same team of surgeons in the operating room. The injection sites were the standard four perianal points (at the 3, 6, 9, and 12 o’clock positions), with a total volume of 20 mL. The injection depth was the subcutaneous layer (to avoid damage to deeper tissues).
For the compound methylene blue group, injection of a mixed solution of 0.1% methylene blue and 0.2% ropivacaine was administered. The preparation method was as follows: 10 mL of 0.1% methylene blue + 10 mL of 0.2% ropivacaine injection. Patients in the LB group were administered an injection of LB solution at a dose of 266 mg. Surgical standardization. All surgical procedures were performed by the same team of experienced surgeons (>10 years of experience in colorectal surgery). The specific technique used was the standard open excisional hemorrhoidectomy (Milligan–Morgan procedure). Briefly, elliptical incisions were made over the hemorrhoidal piles, the external component was dissected and excised, and the internal component was ligated at the base using absorbable sutures. No LigaSure or stapling devices were used to ensure homogeneity of surgical trauma.
Standard postoperative analgesia. Two hours postoperatively, each patients was administered an intravenous injection of 10 mL of 0.9% saline plus 30 mg of aminomethylbenzoic acid ketorolac.
Rescue analgesia. If a patient's postoperative pain score was >4 (VAS score > 4), rescue analgesia was administered via an intravenous injection of 100 mg tramadol.
Outcome measures. Primary outcome included postoperative pain intensity assessed using the VAS (0–10 points). VAS scores were recorded at 0, 6, 12, 24, 36, 48, and 72 h (day 3) postoperatively. Additionally, the total consumption of analgesics within the first 3 postoperative days was calculated and converted to morphine milligram equivalents (MMEs). Secondary outcomes included the following: (a) postoperative complications including acute urinary retention, secondary bleeding, perianal edema, and infection, among others; (b) time to first rescue analgesia and total tramadol consumption; (c) analgesia satisfaction, as assessed using a hospital-developed scale, where patients rated their experience at discharge as satisfied, neutral, or dissatisfied; (d) recovery indicators, including time to first ambulation, time to return of bowel function (first bowel movement), and length of hospital stay; and (e) safety indicators, including incidence of adverse reactions (such as rash and systemic toxicity).
Data collection and management
Baseline data. We recorded patient age, sex, BMI, severity of hemorrhoids, and surgery duration.
Postoperative monitoring. Postoperative monitoring included the use of standardized questionnaires and electronic logs to record pain scores, medication usage, and complications. Data will be confirmed through outpatient visits or phone follow-ups on days 7 and 14.
Data management. Data management included double entry into an electronic database to ensure accuracy.
Software tools. The Statistical Package for Social Sciences (SPSS) software (version 26.0) or R software was used, with a significance level of α of 0.05.
Discussion points and literature support
Rationality of dose selection. The choice of 0.1% methylene blue dosage is based on prior studies demonstrating its safety and equivalent analgesic efficacy, whereas the addition of ropivacaine draws on its synergistic mechanism in nerve blocks (prolonging analgesia duration). The 266-mg dose of LB corresponds to commonly used clinical dosages.
Potential challenges. Multiple previous studies have indicated that the effectiveness of LB may vary depending on the type of surgery, with its advantages possibly not being significant in hemorrhoidectomy. Meanwhile, the adverse reaction rate of compound methylene blue is low (only rash reported); however, local toxicity requires monitoring.
Innovation. This design is the first to directly compare the analgesic effect of compound methylene blue and LB in patients who have undergone hemorrhoidectomy, bridging a gap in the literature where no direct comparison exists. The study methodology is rigorously based on corpus content to ensure scientific validity and reproducibility. In practical implementation, drug dosages and follow-up time points can be adjusted to accommodate specific resources.
Results
In total, 75 patients undergoing hemorrhoidectomy were included. Patient characteristics stratified by the two treatment groups are shown in Table 1. The pain intensity score-time curves after hemorrhoidectomy for the compound methylene blue and LB groups are shown in Figure 1.
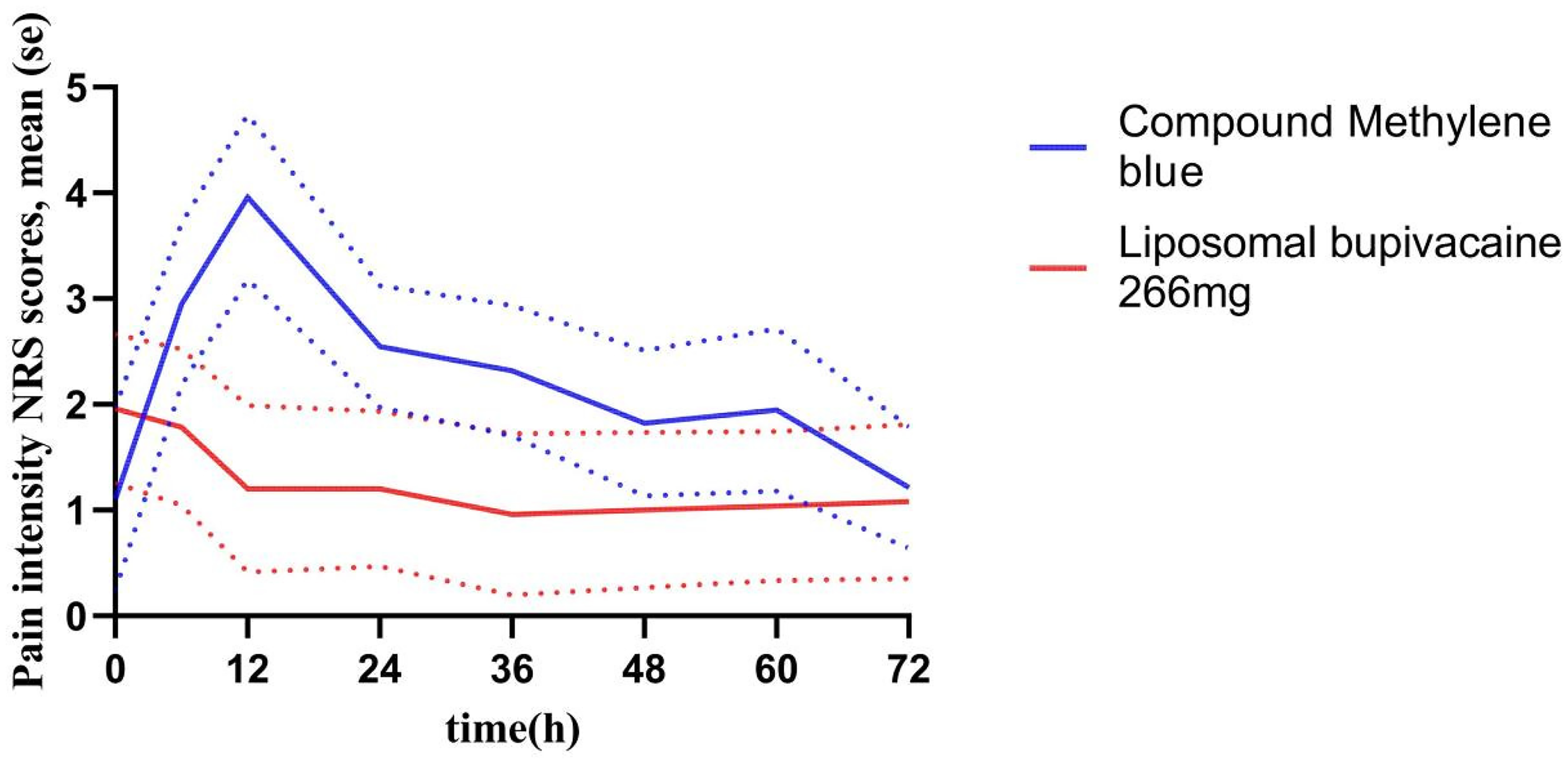
Numerical rating scale (NRS) pain intensity time curves for two treatment groups.
Mean ± standard error (SE) of pain intensity scores (NRS) at various time points after hemorrhoidectomy: compound methylene blue versus liposomal bupivacaine groups.
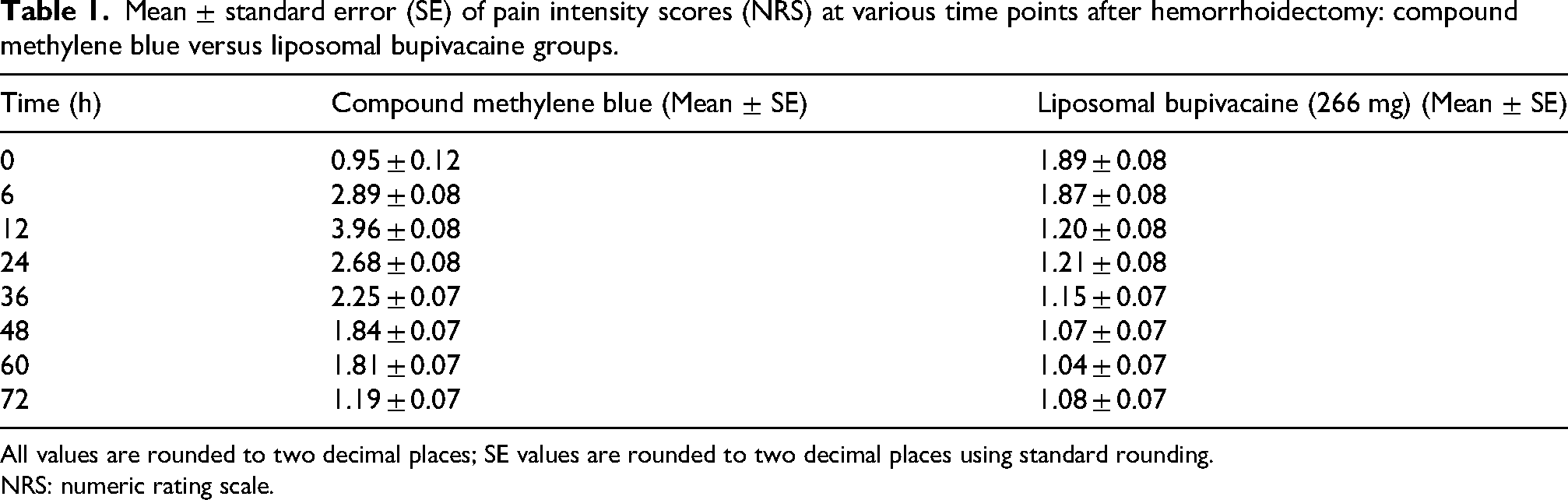
All values are rounded to two decimal places; SE values are rounded to two decimal places using standard rounding.
NRS: numeric rating scale.
As shown in Figure 1 and Table 1, the numeric rating scale (NRS) scores in the compound methylene blue group peaked at 12 h (approximately4) and then gradually declined. In contrast, the NRS scores in the LB group dropped rapidly from baseline (approximately 1.9) and stabilized at approximately 1.0–1.2 after 12 h, significantly lower than those in the compound methylene blue group (especially between 12 and 72 h). Table 1 indicates that compound methylene blue may offer better pain control in the early period (0–6 h) compared with LB; however, the difference between the two gradually diminishes over time. Overall, LB demonstrated a more sustained and stable analgesic effect.
Figure 2 shows that the area under the curve (AUC) for NRS pain scores over the first 72 h postoperatively (NRS AUC0–72h) of the compound methylene blue group was significantly higher than that of the LB group. The LB group exhibited lower cumulative pain intensity scores (NRS AUC0–72h) within 72 h postoperatively p < 0.0001). This indicates that within 72 h postoperatively, the overall pain level was higher and the analgesic effect was poorer in the compound methylene blue group. Although compound methylene blue may exert a stronger analgesic effect in the early stage, its overall duration and intensity of pain relief are inferior to those of LB. There was a significant difference between the two groups at 0 h (1.89 vs. 0.95), suggesting different baseline pain levels. Attention should be paid to whether randomization was adequate or if there was imbalance between the two groups.
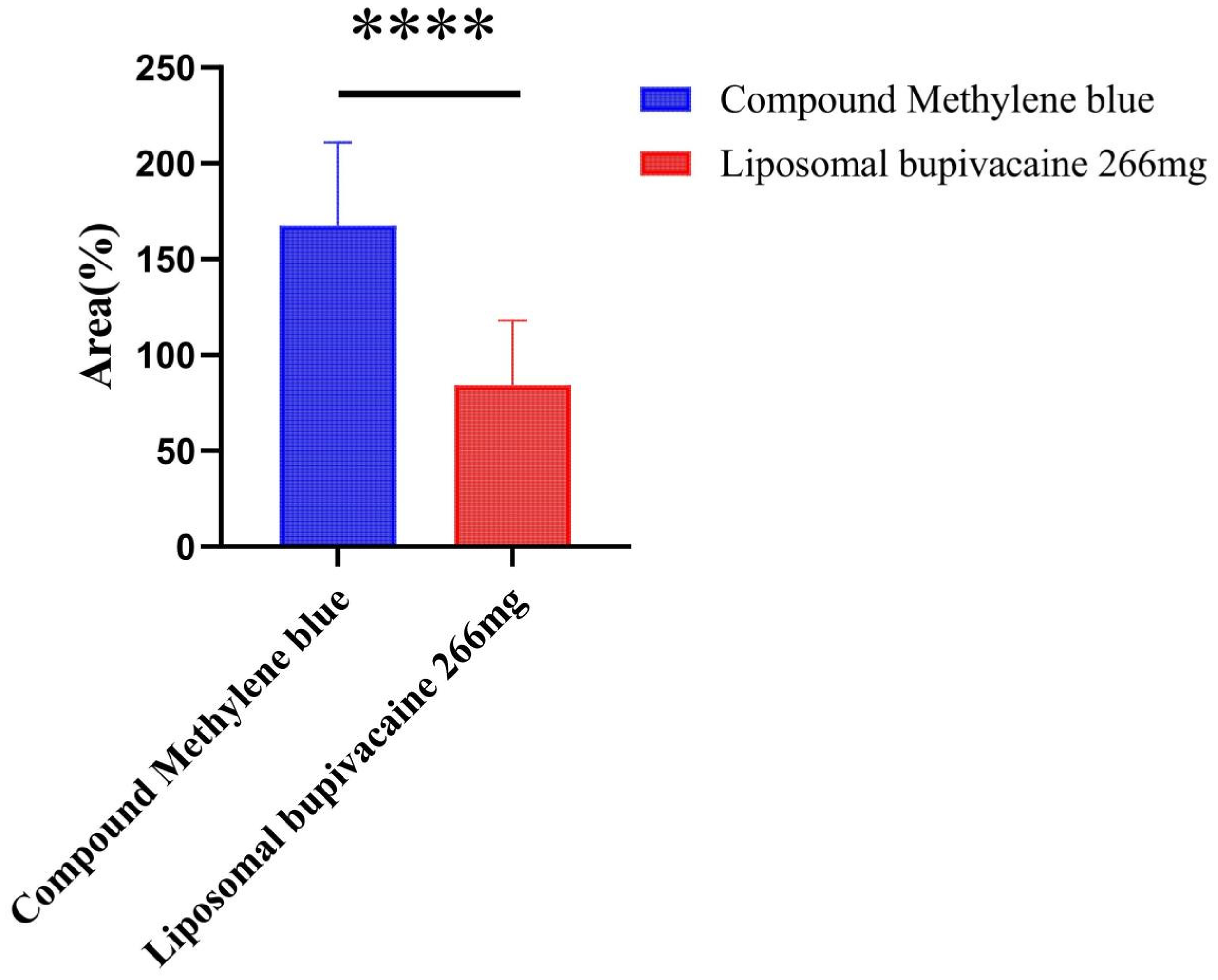
Significance analysis of NRS AUC0–72h between the two groups. The blue bars represent the compound methylene blue group, and the red bars represent the 266 mg liposomal bupivacaine group. AUC refers to the area under the curve of pain intensity (NRS) from 0 to 72 hours, reflecting the overall pain burden; ***indicates a highly significant statistical difference between the two groups (P < 0.001).
The time to first use of opioid rescue medication was significantly longer in the LB group than in the compound methylene blue group, indicating a longer duration of analgesia and a more stable effect. The Kaplan–Meier curve and hazard ratio (HR) results suggest that LB offers a significant advantage in terms of postoperative pain control (HR = 2.82; 95% confidence interval (CI): 1.73 to 4.59; p < 0.001; Figure 3).
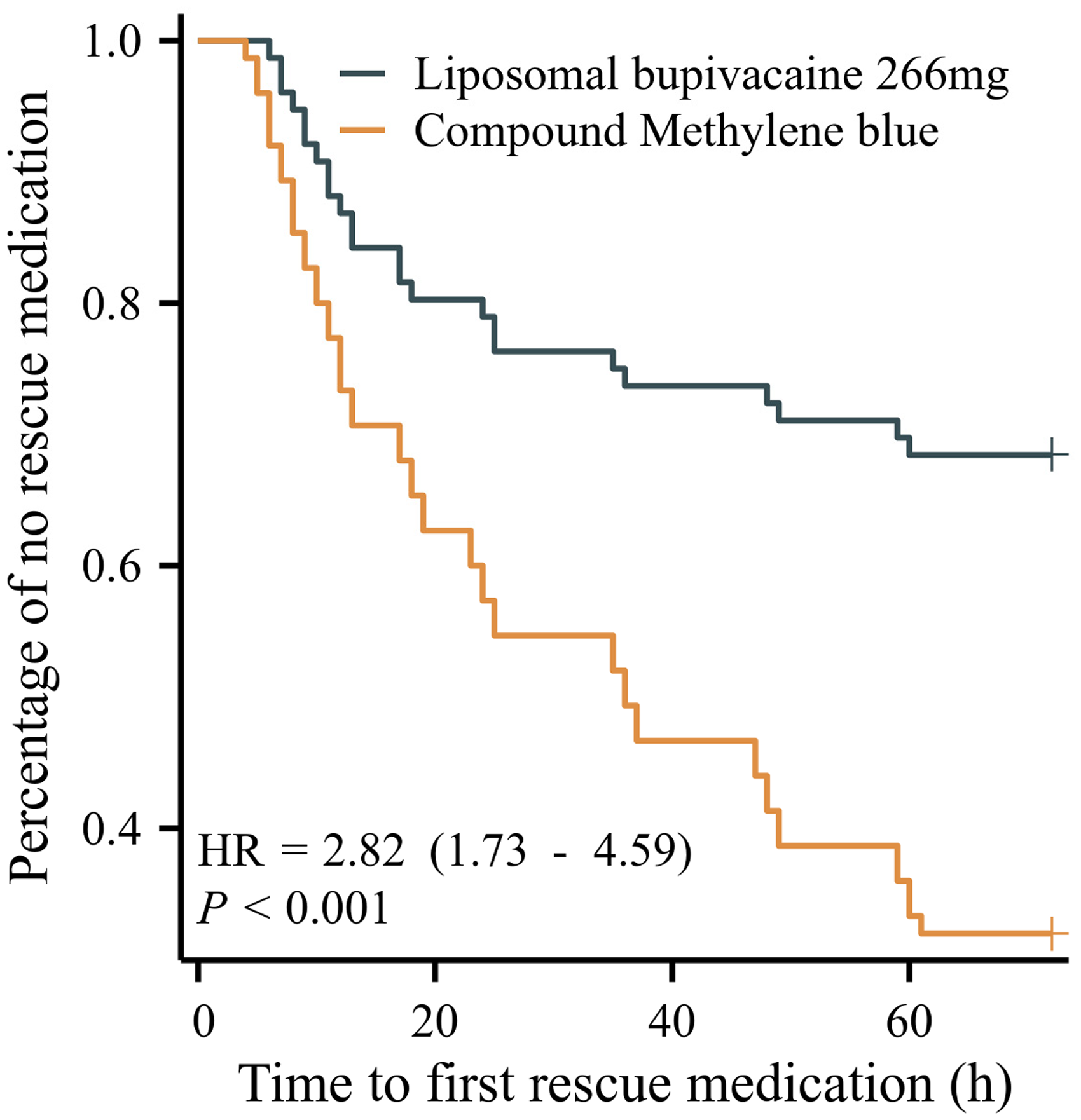
Kaplan–Meier survival curves showing the time distribution of the first use of opioid rescue medication within 72 h postoperatively for the two groups. The blue line represents the liposomal bupivacaine (266 mg) group, and the orange line represents the compound methylene blue group.
Table 2 indicate that the LB group had a significantly lower rate of rescue medication use within 72 h post-surgery compared with the compound methylene blue group (30.7% vs. 68.0%), demonstrating superior and longer-lasting analgesic effects (Table 2). Further odds ratio (OR) analysis showed that patients using compound methylene blue had a 4.5 times higher risk of requiring rescue analgesia (Table 3) than those in the LB group, with the difference being highly statistically significant (p < 0.001). These findings support the clinical advantage of LB in managing postoperative pain after mixed hemorrhoid surgery.
Postoperative rescue analgesia consumption over the first 72 h.

Odds ratios for postoperative rescue medication use (within 72 h).

Patient pain satisfaction was significantly higher in the LB group (Table 4) than in the compound methylene blue group (82.67% vs. 57.33%), indicating greater patient acceptance in clinical practice. A statistically significant difference in satisfaction between the two groups was demonstrated based on the chi-square test (p < 0.05). These findings further support the superior patient experience and clinical value of LB for postoperative analgesia.
Comparison of postoperative pain satisfaction between the two groups.

A significantly lower adverse reaction rate was observed in the LB group compared to the compound methylene blue group (2.7% vs. 13.3%), indicating a superior safety profile (Table 5). A statistically significant difference was observed in the chi-square test (p = 0.0206). These results suggest that LB provides effective analgesia with reduced systemic impact, thereby offering distinct advantages for clinical application.
Incidence of postoperative adverse reactions.

Discussion
The primary finding of this study was that resting and defecation pain scores within 72 h postoperatively were significantly lower in the LB group than in the compound methylene blue group. These results are highly consistent with the unique pharmacokinetic properties of LB. Bupivacaine is released in a controlled manner by the multivesicular liposome structure, providing long-acting local anesthetic blockade for over 72 h. Consequently, the peak period of postoperative acute inflammatory response and pain is effectively covered. 17 The superiority observed in this study may be attributed to this sustained-release mechanism. Postoperative pain peaks were significantly reduced, and dependence on opioids was diminished. For instance, a randomized controlled trial involving 120 hemorrhoidectomy patients has demonstrated that NRS pain scores within 48 h postoperatively were significantly lower in the LB group than in the standard local anesthetic group (mean difference: −1.8; 95% CI: −2.3 to −1.3; p < 0.001).18,19 Higher patient satisfaction was also reported. Superiority of LB over traditional bupivacaine in improving analgesic efficacy and reducing adverse effects, such as nausea and vomiting, has also been confirmed by Chitty et al. in a quality improvement evaluation of perioperative analgesic protocols for hemorrhoidectomy. 18 The critical role of liposome technology in extending the duration of local analgesia was thus highlighted. Consistent conclusions were drawn from a prospective, double-blind, randomized controlled trial (n = 180) conducted in 2025 across three tertiary hospitals in China. 20 Resting pain and dynamic pain (e.g. during walking or defecation) following mixed hemorrhoid surgery were more effectively alleviated by LB. The most significant analgesic advantage was observed on the first postoperative day, which is considered a critical period for recovery.
In contrast, inferior performance was observed in the compound methylene blue group (containing methylene blue and ropivacaine) in this study. Although anti-inflammatory and analgesic effects have been confirmed for methylene blue via inhibition of NO synthase activity, reduction of NO production, and interference with nerve action potential conduction, clinical efficacy remains limited by short duration of action and local tissue irritation. 14 A study involving 180 hemorrhoidectomy patients has revealed that although 0.1% or 0.2% methylene blue slightly reduced total analgesic consumption over 14 days, the magnitude of reduction was far less than that achieved using LB. 13 Furthermore, statistical significance in reducing opioid usage was not demonstrated in multiple studies. This discrepancy is likely attributed to the sustained release of LB for over 72 h, whereas the narrow therapeutic window of methylene blue renders it more suitable as an adjunct rather than a primary analgesic agent. 14 Notably, a compound formulation (methylene blue plus ropivacaine) was used in the current study. However, high-quality evidence regarding the analgesic efficacy of such compounds in anorectal surgery is currently lacking. Existing data have focused primarily on individual components, suggesting that compound formulations do not necessarily synergistically enhance long-acting analgesic effects.13,14
Further support for the conclusions of this study is provided by multiple investigations across diverse surgical models, which consistently demonstrate that LB significantly reduces postoperative pain intensity and opioid consumption. For instance, in applications involving abdominal wall nerve blocks or incision infiltration, median pain scores and MME consumption on postoperative days 1–3 were significantly lower in the LB group than in the standard bupivacaine group.11,21 A randomized controlled trial (n = 90) focusing on posterior lumbar fusion has revealed that intraoperative incision infiltration with LB reduced total opioid consumption by approximately 57% within 72 h postoperatively. 22 Additionally, hospital stays were shortened. These findings are highly consistent with the “opioid-sparing effect” observed in the LB group in the current study. Moreover, a significant reduction in the requirement for rescue analgesics was observed in the LB group, which corroborates the improvement in pain scores. This opioid-sparing effect holds substantial clinical significance. Within the context of the widely implemented ERAS protocol, minimizing opioid usage is recognized as a core principle. This approach effectively prevents adverse reactions such as nausea, vomiting, constipation, drowsiness, and respiratory depression. 6 Opioid dependence is reduced by LB. Consequently, patient comfort is enhanced, and early ambulation, restoration of bowel function, and shortened hospital stays may be facilitated. Thus, the overall recovery process is accelerated.
A key finding of this study is that superior analgesia was achieved using LB without compromising safety. Lower incidences of common complications, such as postoperative arrhythmia and nausea or vomiting, were observed in the LB group compared with those in the compound methylene blue group, indicating a favorable safety profile. Furthermore, we implemented strict safety monitoring protocols to address the specific risks associated with the use of methylene blue. Notably, no cases of methemoglobinemia, hemolysis, or anaphylactic shock were observed in the compound methylene blue group. This is likely attributed to our strict exclusion of patients with G6PD deficiency (a known risk factor for hemolysis) and our adherence to the recommended dosage (0.1%), which is below the threshold typically associated with serotonin toxicity. These findings suggest that when administered according to guidelines in a selected patient population, compound methylene blue remains a safe option; however, clinicians must remain vigilant regarding these potential idiosyncratic reactions. For instance, in a large retrospective cohort study involving over 500 patients undergoing anorectal surgery, the incidence of urinary retention in the LB group was only 1.8%. No significant difference was found compared with groups receiving standard local anesthetics or normal saline controls. 23 Similarly, a favorable safety profile has been confirmed for methylene blue in hemorrhoidectomy patients. 24 In a randomized controlled trial (n = 180), no statistical difference in overall complication rates was detected between the groups receiving 0.1% or 0.2% methylene blue and the control group that was not administered methylene blue. 13 Reported adverse effects, such as transient local pruritus and mild staining, were characterized as mild, self-limiting, and reversible. These results collectively indicate that both interventions were well tolerated. More importantly, it is emphasized in this study that the analgesic advantage of LB was not achieved by increasing complication risks. Instead, secondary risks associated with severe pain were indirectly reduced through optimized pain control.
This safety conclusion is highly consistent with previous studies in other surgical fields. For example, a prospective study (n = 120) on abdominoplasty patients has revealed no difference in the incidence of adverse events (AEs) or serious adverse events (SAEs) between the LB incision infiltration and control groups. 25 No elevated drug-specific risks, such as neurotoxicity and arrhythmia, were observed. Furthermore, a systematic review and meta-analysis comprising 12 randomized controlled trials and 2158 patients explicitly stated that LB did not increase the risk of AEs, including urinary retention, nausea, vomiting, dizziness, or delayed wound healing, across various surgical types. 26 Thus, LB can be safely integrated into multimodal analgesic protocols following mixed hemorrhoid surgery. No new safety hazards were introduced. Instead, functional complications may be indirectly reduced through effective pain control. This favorable safety profile provides a robust evidence-based foundation for its widespread application within ERAS pathways.
Significantly higher patient satisfaction was observed in the LB group. This outcome represents the cumulative effect of the aforementioned advantages, including superior pain control, reduced opioid requirements, fewer adverse reactions, and an enhanced overall recovery experience. Patient satisfaction is defined as a multidimensional subjective indicator. It is profoundly influenced by multiple factors, such as postoperative pain intensity, burden of analgesic-related AEs, sleep quality, and speed of functional recovery. 27 In the current study, an overall satisfaction rate of 82.7% was achieved in the LB group. This rate was significantly superior to that in the compound methylene blue group (57.3%, p = 0.044). This difference is not only statistically significant but also holds clear clinical value.
The phenomenon of “pain rebound,” which often occurs after the dissipation of traditional local anesthetics, was effectively prevented owing to the continuous, stable, and long-acting local analgesia provided by LB. Consequently, patient experience was significantly enhanced. For instance, in a randomized controlled trial involving 93 patients undergoing arthroscopic rotator cuff repair, significantly lower NRS pain scores within 48 h postoperatively were reported in the LB incision infiltration group compared with those in the control group. Simultaneously, analgesic satisfaction scores and sleep quality were significantly improved in this group. 19 Similarly, in the field of plastic surgery, multiple studies have confirmed that the analgesic efficacy and safety of LB in breast reconstruction and abdominoplasty are comparable, if not superior, to those using standard multimodal analgesic protocols. The extended analgesic window is considered to reduce nocturnal pain interference, thereby directly improving patient satisfaction. 8
Although minimally invasive techniques such as laser hemorrhoidoplasty have shown promise in reducing postoperative discomfort by preserving anatomical structures, 5 effective pain management remains a cornerstone in traditional hemorrhoidectomy, which is still widely performed for advanced (III–IV) hemorrhoids. Our study focuses on optimizing analgesia within the conventional surgical framework.
In the context of anorectal surgery, a significant reduction in early postoperative opioid requirements was observed in the LB group. These objective metrics were found to be extremely consistent with high satisfaction levels. This finding is supported by several recent studies. More importantly, patient satisfaction has been incorporated as a core quality metric within the ERAS pathways. 28 It is emphasized that patient-centered analgesic goals should extend beyond pain scores alone to encompass sleep, emotional status, functional recovery, and subjective satisfaction. LB aligns precisely with this modern analgesic philosophy.
Beyond the immediate postoperative period, it is vital to view the pelvic floor not as an isolated anatomical compartment but as part of a complex, integrated system involving the abdomen, spine, posture, and breathing mechanics. 29 Postoperative pain can disrupt the muscular synergies within this system, leading to compensatory patterns and delayed functional recovery.
Effective analgesia plays a pivotal role in restoring this harmony. By reducing reflexive anal sphincter spasms and pain-induced guarding, LB infiltration may facilitate the restoration of normal pelvic floor coordination. Furthermore, identifying patients with pre-existing pelvic floor dyssynergia and utilizing targeted analgesia could be a future direction for personalized rehabilitation. 30 In this study, the improved recovery metrics (such as earlier ambulation) observed in the LB group suggest a positive impact on this integrated functional recovery, although specific pelvic floor functional scores were not measured.
Taken together, the transition from “effective pain relief” to “high-quality experience” was achieved using LB via the integration of long-acting analgesia, an opioid-sparing effect, and a favorable safety profile. The significantly higher patient satisfaction not only validates the technical advantages but also underscores the profound significance of investing in advanced analgesic strategies for enhancing healthcare quality and patient value.
Limitations and future directions
Certain limitations of this study must be acknowledged. First, as a single-center retrospective cohort study, our findings may be subject to selection bias despite our efforts to control for confounders, and their generalizability requires validation through larger-scale, multicenter studies. Second, blinding of the surgeons was not feasible due to the distinct physical appearances of the two agents, which may have introduced performance bias; however, this potential influence was mitigated via the implementation of double-blinding for both patients and outcome assessors. Third, although adequately powered for the primary outcome, the sample size (n = 150) remains relatively modest, warranting future multicenter trials with larger cohorts. Fourth, the follow-up period was limited to 14 days, precluding the assessment of long-term outcomes such as scar formation and late complications. Fifth, we did not employ standardized functional assessment tools (e.g. the Cleveland Clinic Incontinence Score or Pelvic Floor Impact Questionnaire) to evaluate the comprehensive impact on quality of life; future research should integrate these patient-reported outcome measures to provide a more holistic view of recovery. Finally, a formal pharmacoeconomic evaluation was not performed. Although the unit cost of LB exceeds that of methylene blue, this expense must be weighed against its potential comprehensive benefits, including reduced opioid consumption, shortened recovery times, and improved patient satisfaction. Future cost-effectiveness analyses are essential to obtain critical evidence guiding institutional drug selection decisions.
Conclusion
This study confirms that a single intraoperative perianal infiltration of LB represents a superior analgesic strategy than that using methylene blue for postoperative pain management following mixed hemorrhoid surgery. More significant and sustained analgesia was achieved with LB use. In addition, postoperative requirement for rescue opioids was significantly reduced, and higher patient satisfaction was achieved. Meanwhile, no increased risk of complications was observed. Based on these findings, LB should be regarded as a valuable component within multimodal analgesic protocols for anorectal surgery. A robust tool is thus provided for facilitating accelerated patient recovery and enhancing the surgical experience.
Footnotes
Ethics approval and consent to participate
The study protocol was reviewed and approved by the Institutional Review Board (IRB): (Approval Number: NYKY-2026–175–01, Date: (5 March 2026)). This study adhered to the tenets of the Declaration of Helsinki. The need for informed consent was waived by the committee due to the retrospective nature of the study, which posed no more than minimal risk to the participants and because obtaining informed consent was impracticable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data sharing statement
Data will be shared by the corresponding author on reasonable requests made over email.