
Abstract
Drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome is a severe T-cell–mediated adverse cutaneous reaction characterized by rash, fever, and visceral involvement following prolonged drug use. It is rarely induced by proton pump inhibitors, with no prior reports documenting pharmacist-identified pantoprazole-related DRESS syndrome and subsequent intervention. A female in her early 60s (Han Chinese ethnicity) was admitted to the intensive care unit of Xiangtan Central Hospital (Xiangtan, China) in mid-2024 for thoracoabdominal pain caused by a fall, and pantoprazole was initiated for stress ulcer prophylaxis on the hospital day 2. Twenty-six days after pantoprazole initiation, the patient developed diffuse macular erythema with desquamation, and her eosinophil percentage increased from 0.5% to 7.8% after 2 days of rash onset. The clinical pharmacist initially suspected meropenem hypersensitivity and recommended discontinuation of this agent; however, 5 days after the onset of rash, leucopenia was observed with the eosinophil percentage peaking at 18.4%, and subsequent discontinuation of pantoprazole resulted in defervescence within 48 h, gradual resolution of the rash, and normalization of blood counts within approximately 10 days of drug cessation. Despite the complex pathophysiology and diagnostic challenges associated with DRESS syndrome, the pharmacist’s identification of the suspected drug and targeted intervention achieved favorable outcomes, providing clinical reference for further research on DRESS syndrome.
Keywords
Introduction
Drug-induced hypersensitivity syndrome (DiHS), also referred to as drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome, is a severe adverse drug reaction (ADR). 1 The clinical manifestations of this condition include fever, extensive rash, concurrent damage to internal organs, lymph node enlargement, eosinophilia, and atypical lymphocyte proliferation. 2 This potentially life-threatening ADR affects patients of all ages, with an incidence ranging from 1/100,000 to 1/1000. In the absence of prompt diagnosis and active treatment, the mortality rate can reach 10%–20%. 3 The core principles of DRESS syndrome management involve immediate discontinuation of the suspected drug, adequate nutritional support, immunosuppressive therapy (particularly systemic corticosteroids and, in selected cases, other immunosuppressive agents), and individualized treatment regimens tailored to the patient's clinical condition. 4 Recent studies have shown that early stratification using the DiHS/DRESS severity score facilitates the identification of refractory cases. 5 Long-term follow-up is critical because late autoimmune complications may develop up to 3 years after the initial DRESS syndrome episode, whereas the initial drug reaction typically occurs 2–8 weeks after exposure. 6
Pantoprazole is a next-generation proton pump inhibitor (PPI), developed after omeprazole and lansoprazole, and belongs to the bis-anthraquinone benzimidazole class. 7 Differences in the substituents on its pyridine and benzimidazole rings distinguish its biochemical, pharmacokinetic, and pharmacological properties from those of omeprazole and lansoprazole, resulting in stronger selectivity and specificity.8,9 Pantoprazole inhibits gastric acid secretion by covalently binding to two sites of the hydrogen potassium adenosine triphosphatase (H+/K+-ATP) enzyme system in gastric parietal cells. In addition to suppressing gastric acid, it reduces gastric juice volume, inhibits pepsin secretion and activity, and impedes Helicobacter pylori proliferation. Clinically, pantoprazole is used to treat various gastrointestinal disorders, including gastric and duodenal ulcers, moderate-to-severe reflux esophagitis, and Zollinger–Ellison syndrome; it is also combined with other drugs for H. pylori eradication. 10 Common adverse reactions associated with pantoprazole use include dizziness, insomnia, drowsiness, nausea, diarrhea, constipation, rash, and myalgia, whereas the incidence of severe ADRs is relatively low. Long-term use of PPIs is also associated with multiple adverse effects, including osteoporosis, chronic kidney disease, increased risk of pneumonia, and elevated risk of Clostridioides difficile infection. 11
This report describes a case of possible pantoprazole-induced DRESS syndrome identified by a clinical pharmacist. Symptoms emerged 26 days after initiation of drug administration. Following the pharmacist's identification of pantoprazole as the suspected causative drug and subsequent discontinuation of the drug after consultation with clinicians, the patient's rash subsided and eosinophil (EOS) count decreased significantly. To the best of our knowledge, this is the first report of pharmacist-led identification of PPI-induced DRESS syndrome. Additionally, this study provides the first review of case reports on DiHS/DRESS syndrome induced by PPIs.
Case report
The reporting of this case conforms to the Case Report (CARE) guidelines. 12 Written informed consent was obtained from the patient for treatment and case publication, and all patients details have been deidentified to protect anonymity.
A female in her early 60s (Han Chinese ethnicity) was admitted to the intensive care unit of Xiangtan Central Hospital (Xiangtan, China) in mid-2024 following a fall from a height, resulting in severe thoracoabdominal trauma. She had no significant previous medical, family, or drug allergy history. On the day the rash and fever developed, her body temperature was up to 38°C; diffuse macular erythema with superficial desquamation distributed over the trunk and extremities without pruritus was present; and there was no evidence of new-onset respiratory distress, abnormal pulmonary auscultation, abdominal pain, nausea, vomiting, diarrhea, chest pain, palpitations, edema, or new neurological deficits.
On the hospital day 2, the patient underwent embolization of bilateral internal iliac artery branches, and ventilator-associated pneumonia developed shortly; therefore, empirical piperacillin/tazobactam was administered. On the hospital day 11, her body temperature and procalcitonin level increased, and a blood culture indicated Gram-positive cocci. Accordingly, antimicrobial treatment was escalated to meropenem and vancomycin. On the following day, hypernatremia was noted, and intravenous pantoprazole (40 mg once daily) was initiated for stress ulcer prophylaxis, and continuous renal replacement therapy was started. On the hospital day 18, metagenomic next-generation sequencing identified Acinetobacter baumannii, Candida tropicalis, and herpes simplex virus type 1, and fluconazole was added to the regimen. On the hospital day 26, a central line sample grew carbapenem-resistant A. baumannii, and the antimicrobial regimen was adjusted to meropenem, colistin, and caspofungin.
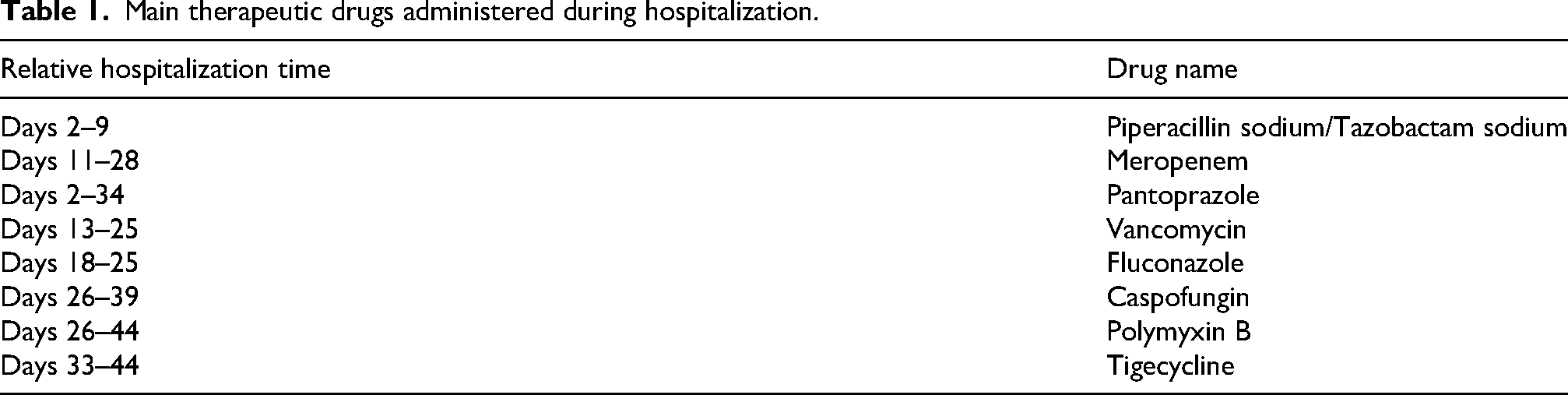
On the hospital day 27, diffuse macular erythema with superficial desquamation appeared on the patient's trunk and limbs (Figure 1). Figure 1(a) shows confluent dark red lesions with fine scaling on the back, and Figure 1(b) presents similar desquamating erythema on the lower legs. The rash worsened on the hospital day 29, and the EOS percentage (EOS%) increased from 0.5% to 7.8%. The clinical pharmacist suspected a hypersensitivity reaction related to meropenem and recommended discontinuation of meropenem, with subsequent adjustment to colistin and tigecycline according to previous microbiological results. On the hospital day 34, leucopenia was observed, and the EOS% further increased to a peak of 18.4%, prompting comprehensive re-evaluation of all recently administered medications. Pantoprazole was then suspected as the causative agent and was discontinued. Within 48 h of pantoprazole withdrawal, the patient's body temperature normalized. The skin eruption gradually subsided, and complete blood count parameters returned to normal levels by hospital day 44. The patient had no prior drug allergies, and the chronology of antimicrobial and supportive interventions has been summarized in Table 1. The clinical pharmacist played a pivotal role in the patient's medication management and follow-up during hospitalization. Figure 2 illustrates the key pharmacist interventions and subsequent outcomes, whereas Figure 3 presents critical data from pharmacist-monitored blood counts and creatinine levels. Figure 3(a) reflects dynamic changes in EOS%, white blood cell (WBC) count, and EOS count, and Figure 3(b) shows the variations observed in the creatinine level during the treatment course.

Cutaneous lesions observed on the patient’s back and leg during hospitalization. Large patches of dark red erythema and desquamation were noted on the (a) back and (b) lower legs. No patient identifiers are present in the figure.
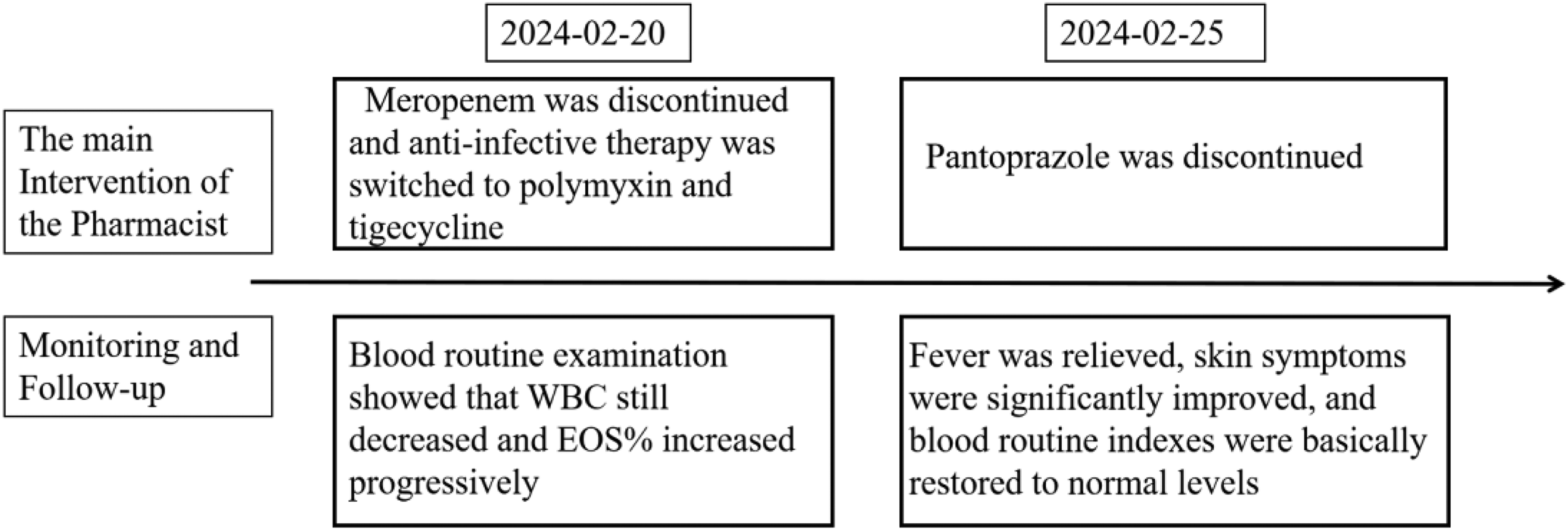
Pharmacist’s key interventions and follow-up results.

Results of pharmacist-monitored (a) blood routine tests and (b) creatinine levels.
Main therapeutic drugs administered during hospitalization.
Comprehensive assessment showed no evidence of pulmonary, renal, gastrointestinal, or cardiac involvement during the clinical course of suspected DRESS syndrome. Renal dysfunction had been present before the appearance of the rash and did not deteriorate acutely during the reaction period. The patient's rash subsided after the discontinuation of pantoprazole, and no systemic corticosteroids or other immunosuppressants were required for the treatment of DRESS syndrome. Subsequently, she was transferred to the general ward of her local hospital and was advised to undergo regular follow-up after discharge. During this period, there was no recurrence of DRESS syndrome or any autoimmune complications.
Discussion
DRESS syndrome is a severe cutaneous ADR with variable latency period from drug initiation to symptom onset. Latency is not universal, and in antibiotic-associated cases, particularly those related to penicillin, the onset of DRESS syndrome may be shorter, as supported by the findings by Castagna et al. 13 The typical interval ranges from 2 to 8 weeks after initial drug exposure. 14 The cutaneous manifestations of this condition are diverse and include urticaria, eczema, lichenoid changes, exfoliative dermatitis, erythema, target lesions, purpura, vesicles, pustules, or their combinations. 15 Common triggering agents include antiepileptic drugs, antibiotics, allopurinol, and nonsteroidal anti-inflammatory drugs, whereas PPIs are rare causes, accounting for only 0.2%–0.3% of all reported cases.16,17
The diagnosis of DRESS syndrome primarily relies on the European registry of severe cutaneous adverse reactions (European RegiSCAR) scoring system, a validated and widely used tool with a score range of −4 to 9. Diagnostic certainty is categorized as follows: (a) score <2 (no DRESS syndrome); (b) score: 2–3 (possible DRESS syndrome); (c) score: 4–5 (highly probable DRESS syndrome); and (d) score >5 (definite DRESS syndrome). 18 DRESS syndrome is often associated with polypharmacy; the most common triggers include anticonvulsants (37.3%), antibiotics (24.8%), and allopurinol (8.2%). 1 Due to the outdated nature and small sample sizes in previous studies, we reviewed recently published studies and identified 21 reported cases of PPI-associated DRESS. Most patients were female (mean age: 62.0 ± 11.3 years), with esomeprazole being the most commonly implicated PPI (11/21, 52.4%), followed by pantoprazole (4/21, 19.1%) and omeprazole/lansoprazole (3/21, 14.3%).19–26 However, as this was a literature review, the generalizability of the sample is limited.
Notably, DRESS syndrome exhibits variable and nonspecific clinical manifestations. Clinical attention must extend beyond rash morphology to include comprehensive assessment and meticulous differentiation of multiorgan system damage. DRESS syndrome involves T-cell activation, viral reactivation, and sustained systemic immune dysregulation. Major clinical features include fever, extensive skin rash, eosinophilia, and involvement of visceral organs, including the lung, kidneys, heart, and gastrointestinal tract. Visceral organ involvement represents the most important prognostic determinant and directly influences the intensity of clinical management and patient outcomes. 16
In patients with DRESS syndrome, the liver represents the second most frequently involved solid organ following the skin. 27 Elevations in liver enzyme levels may precede the onset of rash, typically presenting as mild abnormalities. 28 The predominant pattern of liver injury is cholestatic, followed by mixed cholestatic-hepatocellular injury. 29 In rare instances, acute liver failure may progress to a severity necessitating liver transplantation. 16 Lung involvement is also relatively common in DRESS syndrome, manifesting in approximately 32% of all cases. 30 The most common pulmonary manifestations include diffuse interstitial infiltration, interstitial pneumonia, pleural effusion, dyspnea, hypoxemia, and cough. Severe cases may progress to acute respiratory distress syndrome (ARDS), respiratory failure, and even death. Less common pulmonary manifestations include pulmonary hemorrhage, bronchiolitis, and pulmonary fibrosis. 31 The typical renal manifestation of DRESS syndrome is acute interstitial nephritis (AIN), which is the most classic renal phenotype. The clinical features include elevated serum creatinine level, decreased glomerular filtration rate, sterile pyuria, hematuria, mild to moderate proteinuria, and renal tubular dysfunction. In severe cases, the patient may develop acute kidney injury (AKI) requiring renal replacement therapy. 32 A systematic review and evaluation has indicated that although most patients exhibited concurrent liver damage, one out of every five patients presented with isolated renal involvement. 33 Gastrointestinal involvement in DRESS syndrome takes various forms and is relatively rare. 34 Less common gastrointestinal manifestations include nausea, vomiting, watery diarrhea, abdominal pain, colitis, intestinal mucosal edema, pancreatitis, ascites, esophagitis, gastritis, enteritis, and late autoimmune sequelae caused by pancreatic injury, such as fulminant type 1 diabetes, autoimmune type 1 diabetes, and type 2 diabetes. 35 Cardiac involvement is less common but life-threatening and includes myocarditis, arrhythmia, pericarditis, cardiac dysfunction, and elevated cardiac enzymes, which can lead to hemodynamic instability and poor prognosis. 36
This case represents possible DRESS syndrome associated with pantoprazole exposure. The clinical pharmacist performed sequential medication evaluation and targeted drug discontinuation, which led to rapid and complete patient recovery. For severe or refractory cases of DRESS syndrome, systemic corticosteroids or other immunosuppressive agents remain the mainstay of treatment. Thus, we emphasize that multidisciplinary consultations require detailed documentation of symptoms and close monitoring of signs to extract actionable information. Furthermore, given the complex immunological mechanisms underlying DRESS syndrome, structural or metabolic similarities between drugs may trigger cross-allergic reactions. High-quality studies are needed to optimize risk stratification, assessment, and evidence-based treatment strategies for DRESS syndrome.
This study has certain limitations. Due to the limited medical resources available at primary healthcare facilities, auxiliary tests for risk stratification and identification of drug-related causative factors, such as pharmacogenomic testing (human leukocyte antigen (HLA) genotyping and cytochrome P450 (CYP) genotyping) and in vivo tests (patch tests and delayed intradermal tests), were not feasible. Future studies should prioritize enhancing pharmaceutical management and minimizing oversight to improve patient safety.
Conclusion
This case demonstrates the important role of clinical pharmacists in identifying possible DRESS syndrome related to pantoprazole use in a critically ill patients being administered multiple medications. Early identification and prompt discontinuation of the suspected drug enabled complete clinical recovery without additional immunosuppressive treatment. This case provides valuable clinical evidence for the monitoring, identification, and management of PPI-related severe cutaneous adverse reactions.
Footnotes
Acknowledgment
All authors acknowledge the patient's consent to publish this manuscript.
Ethics statement and informed consent
This case report was approved by the Medical Ethics Committee of the Third People's Hospital of Chengdu, Chengdu, China (ID: 2025-0029; 18 Nov 2025). The reporting of this study conforms to the Case Report (CARE) guidelines. This study obtained written informed consent from the patient. This retrospective case report used anonymized data.
Author contributions
Lei HB and Liu X conceptualized the case report. Chen GH and Zheng YH drafted the manuscript. All authors revised the manuscript, contributed to its refinement, and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Xiangtan Medical Scientific Research Project (Grant No. 2024-xtyx-21). The authors received no additional financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Original contributions to the study are included in the manuscript. For further inquiries, please contact the corresponding author.