
Abstract
Objective
To assess diabetes mellitus-related knowledge, attitudes, risk perception, and preventive understanding among non-diabetic adults in Iraq.
Methods
This cross-sectional study used convenience, voluntary sampling to recruit adults aged 18 years or older without a prior diagnosis of diabetes mellitus from different regions of Iraq between June and October 2025. Participants completed a culturally adapted questionnaire assessing sociodemographic characteristics, diabetes mellitus knowledge, attitudes, information sources, and beliefs regarding prevention. Descriptive statistics, Mann–Whitney U tests, quantile regression, and binary logistic regression were used.
Results
The study included 874 participants. Nearly half (48.4%) reported a family history of diabetes mellitus. Common symptoms, such as frequent urination (89.9%) and excessive thirst (84.2%), were widely known, whereas less obvious symptoms, such as unexpected weight loss, were less well recognized. Awareness of some complications, such as loss of consciousness (94.2%) and amputation (93.8%), was high, while awareness of others, such as kidney damage (69.5%) and eye disorders (78.3%), was moderate. Quantile regression analysis showed significantly lower knowledge scores among participants without a medical background (β = −4.214, p < 0.001). In addition, higher knowledge scores were significantly associated with more positive attitudes toward diabetes mellitus (odds ratio = 1.179, 95% confidence interval: 1.108–1.255, p < 0.001), whereas older age was associated with less favorable attitudes (odds ratio = 0.545, p < 0.001).
Conclusions
Adults without diabetes in Iraq demonstrated a good basic understanding of diabetes mellitus; however, important gaps remain in knowledge of symptoms, complications, and key risk factors. These findings highlight the need for practical, evidence-based public health education to support prevention efforts and reduce the future burden of diabetes mellitus.
Introduction
Diabetes mellitus (DM) is a chronic metabolic condition caused by insufficient insulin secretion, impaired response to insulin, or both, leading to elevated blood glucose levels. 1 Globally, diabetes represents a major public health issue. 2 By 2022, over 800 million adults had been diagnosed with DM, with its prevalence increasing from 7% in 1990 to about 14% in 2022. 3 This significant increase in DM rates is strongly driven by sedentary behavior, obesity, and unhealthy diets, especially in rapidly urbanizing developing countries. 4 By 2040, more than 70 million people across the Middle East and North Africa are expected to be living with diabetes. 5 As in many neighboring countries, diabetes prevalence in Iraq has risen sharply, affecting an estimated 17% of adults, nearly half of whom (8.1%) remain undiagnosed. 6
Non-diabetic individuals represent a critical target for diabetes prevention, as this group includes those at risk of developing the disease as well as individuals who may already have undiagnosed diabetes. Improving knowledge in non-diabetic populations can support earlier recognition of symptoms, reduce delays in diagnosis, and promote risk-reducing behaviors and lifestyle modification before the onset of complications. 7 Previous cross-sectional studies among adults without DM have assessed the role of knowledge in preventive behaviors. These studies consistently show that individuals with better knowledge are more likely to engage in preventive practices such as healthier diets and regular physical activity, emphasizing that effective diabetes prevention relies heavily on strengthening knowledge within non-diabetic populations.8,9 Awareness of the classical symptoms of DM, such as polyuria and polydipsia, is crucial for early detection, while recognizing possible complications including kidney failure and vision problems encourages individuals to adopt preventive measures and participate in regular screening. 10
Evaluating the knowledge, attitudes, and preventive practices of individuals without diabetes is essential for identifying gaps that could limit efforts to prevent the disease. This study was guided by a knowledge-attitude-practice framework, which is commonly used in public health research to examine awareness and beliefs as they may reflect in health-related behaviors. 11 Although several instruments have been developed and validated to assess public knowledge of diabetes symptoms, complications, and risk factors,12–18 many were designed for populations with different cultural, linguistic, healthcare, and socioeconomic contexts. Certain items within existing tools may not adequately reflect local beliefs, terminology, healthcare access patterns, and public perceptions relevant to Iraqi society. Therefore, a culturally adapted questionnaire was developed using previously published instruments as a foundation, with modification and contextual refinement to improve clarity, cultural relevance, and applicability to the Iraqi population. Given the increasing burden of diabetes and the persistence of public knowledge gaps, evaluating community awareness, attitudes, and preventive practices can help inform evidence-based health education interventions, support earlier recognition of diabetes, and reduce future disease burden. In doing so, this work provides relevant evidence for policymakers, healthcare educators, and clinicians seeking to design community-oriented prevention strategies for individuals without a prior diabetes diagnosis.
Methods
Study design and population
This cross-sectional study recruited participants from different regions of Iraq between June and October 2025 using a convenience, voluntary sampling approach. Participants were enrolled after voluntarily responding to the online questionnaire or in-person outreach. Eligible participants were adults aged 18 years or older, without a prior diagnosis of DM, who were willing to take part in the study. Electronic informed consent was obtained from all participants before participation. Ethical approval was granted by the Institutional Review Board (IRB) and the Deanship of Research at Al-Rasheed University College, Baghdad, Iraq (reference number RUCPD10012601; approved on 15 May 2025). The study was conducted in accordance with the Declaration of Helsinki of 1975, as revised in 2024.
No identification information was obtained in the online questionnaire. The reporting of this cross-sectional study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 19 All mandatory questionnaire items required for analysis had to be completed before submission; therefore, submitted questionnaires contained no missing values. Participants could withdraw at any time before submission by leaving the questionnaire incomplete.
Tool development and validation
The questionnaire was developed following an extensive review of previously published studies.12–18,20 It comprised four main sections. The first section collected participants’ sociodemographic characteristics, along with personal and family medical history. The second section assessed diabetes knowledge across multiple domains, including general knowledge, symptoms, risk factors, and complications. The third section evaluated participants’ attitudes toward DM. The final section examined exposure to diabetes-related information and beliefs regarding preventive measures. The full questionnaire is included as supplementary material.
Content validity was assessed by an expert panel consisting of one endocrinologist, two pharmacists, and one clinical pharmacist. The translation process was conducted by two independent bilingual healthcare professionals experienced in medical terminology and academic research. Initially, the questionnaire was translated into two separate Arabic versions. The research team then reviewed both versions and resolved discrepancies to produce a single consensus version. This version was subsequently back-translated into English by an independent bilingual clinical pharmacist fluent in both Arabic and English and compared with the original questionnaire. All versions, including the original English and final Arabic versions, were reviewed to identify and resolve any remaining inconsistencies. The translation process followed Brislin's principles for cross-cultural research. 21
A pilot study involving 30 non-diabetic adults was conducted to assess the clarity, comprehensibility, and internal consistency of the study instrument. Participants completed the questionnaire after providing informed consent and were asked to comment on item clarity, wording, and perceived difficulty. Data from the pilot study were not included in the final analysis. Measurement bias was reduced through expert validation, translation/back-translation, and pilot testing.
Sample size calculation
A convenience, voluntary sampling strategy was used in this study. The required sample size was estimated assuming a 95% confidence level and a 4% margin of error, yielding a minimum of 601 participants. A total of 874 individuals were ultimately enrolled, indicating that the target sample size was exceeded.
Statistical analysis
To perform statistical analyses, Statistical Package for the Social Sciences version 26 was used. Participant characteristics and study variables were summarized using descriptive statistics. The Kolmogorov–Smirnov test indicated that the data were not normally distributed; therefore, nonparametric statistical methods were applied. Continuous variables were presented as medians with interquartile ranges (IQRs), while categorical variables were expressed as frequencies and percentages.
The knowledge score was calculated by assigning 1 point for each correct response and 0 points for each incorrect response. Bivariate analyses were first conducted to compare knowledge and attitude scores between participants working or studying in the medical field and those without a medical background and between participants with and without a family history of DM. Because the score distributions were non-normally distributed, subgroup comparisons were performed using the Mann–Whitney U test, with results reported as medians and IQRs. Quantile regression was then employed to assess the relationship between predictor variables and the median knowledge score, as this approach provides robust estimation of median outcomes and is less sensitive to outliers than ordinary linear regression. The quantile regression model included age group, gender, marital status, educational level, working or studying in the medical field, income level, previous receipt of diabetes-prevention information, place of residence, presence of chronic disease, family history of DM, and information source. Binary logistic regression was also performed to identify factors associated with participants’ attitudes toward DM, with positive attitude as the dependent outcome. Positive attitude was defined as an attitude score above the sample median. The binary logistic regression model included knowledge score, age group, gender, marital status, educational level, working or studying in the medical field, place of residence, income level, presence of chronic disease, family history of DM, information source, and previous receipt of diabetes-prevention information. All variables were entered into the regression models simultaneously. Multicollinearity was assessed using the variance inflation factor (VIF), and no collinearity was observed, as all VIF values were below 3. Statistical significance was set at p < 0.05.
Results
A total of 874 participants were included in the study. As shown in Table 1, most participants were women (62.4%) and within the age group of 18–29 years (51.7%). The majority of participants held a college or university degree (72.9%), were not married (56.2%), and were working or studying in the medical field (58.4%). The vast majority resided in urban areas (91.2%). The median body mass index (BMI) was 24.66 (IQR: 22.45–27.74). In terms of health status, 82.3% of participants reported no chronic diseases, and nearly half (48.4%) reported having a family history of DM.
Participants’ sociodemographic characteristics.

*Values are presented as count (%) unless otherwise indicated. BMI is presented as median (IQR).
BMI: body mass index; IQD: Iraqi Dinar; IQR: interquartile range.
Table 2 summarizes participants’ knowledge of diabetes, covering general concepts, symptoms, complications, and risk factors. The median knowledge score was 21 (IQR: 18–24) out of a maximum score of 29. Internal consistency was evaluated using Cronbach's alpha (α), demonstrating good reliability (α = 0.8). Overall, awareness of DM as a chronic disease was remarkably high, with over 90% of participants correctly identifying its key characteristics. Similarly, most respondents accurately recognized the diagnostic basis of DM and the need for insulin therapy in some patients. These findings reflect a strong basic understanding of the condition. However, important gaps were observed regarding hereditary and familial risk. Only 52.9% of participants correctly identified DM as a hereditary disease, and only 40.0% recognized family history as a risk factor, indicating limited awareness of genetic and familial susceptibility to DM. However, there was noticeable variation in knowledge about DM symptoms and complications. Although common symptoms such as frequent urination (89.9%) and excessive thirst (84.2%) were widely identified, less pronounced symptoms, such as unexpected weight loss, generalized weakness, or blurred vision, were significantly less recognized, with about half of the participants answering incorrectly. A similar pattern was observed for awareness of complications. Although
Diabetes knowledge assessment.
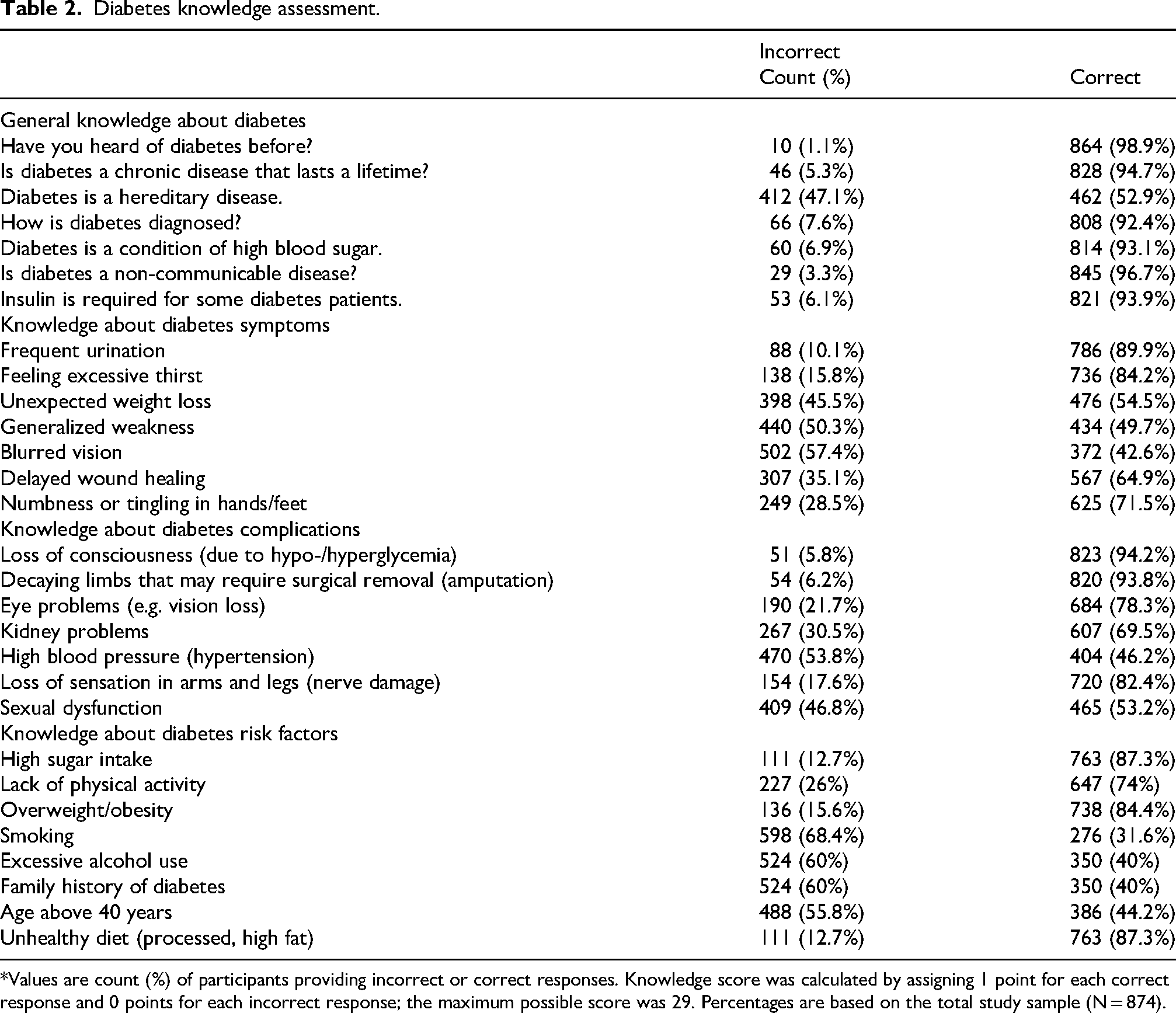
*Values are count (%) of participants providing incorrect or correct responses. Knowledge score was calculated by assigning 1 point for each correct response and 0 points for each incorrect response; the maximum possible score was 29. Percentages are based on the total study sample (N = 874).
severe outcomes such as loss of consciousness and amputation were widely recognized (94.2% and 93.8%, respectively), awareness of other serious complications, including kidney damage (69.5%) and eye disorders (78.3%), was more moderate. Participants showed low recognition of hypertension and sexual dysfunction as complications of DM, pointing to critical knowledge gaps.
Knowledge of diabetes risk factors was generally high for modifiable lifestyle factors such as lack of physical activity (74%) and obesity (84.4%). However, recognition of smoking and alcohol consumption as risk factors was lower, at 31.6% and 40%, respectively.
In the bivariate analysis, participants working or studying in the medical field had significantly higher knowledge scores than those without a medical background (median 23 (IQR: 21–25) vs. 18,15–21 p < 0.001). They also showed more favorable attitude-score distributions (44–4 vs. 4,3–4 p < 0.001). In contrast, knowledge scores did not differ according to family history of DM (2118–24 among participants with a family history vs. 2217–24 among those without, p = 0.973). Participants with a family history of DM showed a small but statistically significant favorable shift in attitude-score distribution, despite identical median and IQR values (44–4 vs. 4,4–4 p = 0.027).
Table 3 displays the quantile regression model that investigates the factors influencing DM knowledge scores among the participants. The findings revealed that being single was linked to a significantly lower knowledge score (p = 0.021). Importantly, individuals without a medical background had significantly lower knowledge, with those not studying or working in the medical field showing a substantial negative association (β = −4.214, p < 0.001). Similarly, participants who had not previously received information regarding DM prevention showed significantly lower knowledge levels (β = −1.929, p < 0.001). Additionally, relying on non-scientific sources was linked to poorer knowledge (β = −1.571, p = 0.001), indicating that inaccurate information sources might contribute to these knowledge gaps. Conversely, neither urban residence nor other sociodemographic factors such as age, gender, or income demonstrated significant associations with knowledge scores.
Quantile regression of diabetes knowledge score.

*Quantile regression estimated the median knowledge score (q = 0.5).
β: regression coefficient; Std. Error: standard error; Sig.: p-value; CI: confidence interval. Categories marked 0c served as reference categories.
Table 4 presents the binary logistic regression model examining the predictors of attitudes toward DM. The analysis showed that higher knowledge scores were significantly associated with more positive attitudes toward DM (odds ratio (OR) = 1.179, p < 0.001). Age was also a significant predictor, with older individuals being less likely to have positive attitudes toward DM (OR = 0.545, p < 0.001). Additionally, participants who were working or studying in the medical field were significantly more likely to have favorable attitudes toward DM (OR = 3.761, p < 0.001). Lower educational attainment was associated with a reduced likelihood of positive attitudes toward DM (OR = 0.348, p = 0.026), with participants holding a college or university degree or a high school education showing less favorable attitudes compared with those with postgraduate education. Conversely, gender, place of residence, income level, presence of chronic diseases, family history of DM, and prior exposure to information were not statistically significant.
Binary logistic regression of attitudes toward diabetes.

*Binary logistic regression was used with positive attitude toward diabetes as the dependent outcome.
β: regression coefficient; SE: standard error; Sig.: p-value; Exp(B): odds ratio; CI: confidence interval.
Values above 1 indicate higher odds of a positive attitude, while values below 1 indicate lower odds.
Discussion
The global burden of DM has increased steadily over recent decades, particularly in low- and middle-income countries, where delayed diagnosis and limited preventive efforts remain major challenges. 22 In Iraq, the prevalence of DM continues to rise, with a substantial proportion of cases remaining undiagnosed, underscoring the importance of prevention and early recognition at the community level.23,24 In this context, non-diabetic individuals represent a key target group for diabetes prevention strategies, as their level of knowledge and attitudes can influence risk perception, health-seeking behavior, and adoption of preventive practices. Therefore, the present study aimed to comprehensively assess diabetes-related knowledge and attitudes among non-diabetic Iraqi adults using a culturally adapted and population-specific questionnaire. By identifying knowledge gaps and attitudinal patterns, this study seeks to inform targeted public health interventions designed to enhance early recognition, promote preventive behaviors, and ultimately reduce the future burden of DM in Iraq.
Most participants demonstrated a strong understanding of basic DM concepts, including its chronic and non-communicable nature, associated hyperglycemia, diagnostic basis, and the role of insulin in the management of some patients. This level of general knowledge among non-diabetic adults is comparable to, and in some aspects exceeds, levels observed in studies conducted in Saudi Arabia, 25 South Africa, 26 and Ethiopia. 27 The relatively high awareness of these fundamental concepts may reflect an increasing public visibility of DM as a major health condition, as well as greater exposure to DM-related information through healthcare services, media, and community discourse, even among individuals without a formal diagnosis.
Clear gaps were observed in knowledge of DM symptoms and related complications. Although most participants were familiar with classical symptoms such as polyuria and polydipsia, awareness of less typical manifestations, including blurred vision, generalized weakness, weight loss, and delayed wound healing, was considerably lower. A similar pattern was evident for complications, with severe outcomes such as loss of consciousness and amputation widely recognized, whereas conditions such as hypertension, sexual dysfunction, kidney damage, and eye disorders were less consistently identified as DM-related complications. This selective pattern of knowledge is important, as limited awareness of early and less dramatic symptoms may delay help-seeking and diagnosis, while poor recognition of common complications may reduce perceived risk and urgency. A similar pattern has been reported previously among non-diabetic populations in diverse settings.28,29
With respect to modifiable risk factors, participants demonstrated strong awareness of several risks, including unhealthy, sugar-rich diets, physical inactivity, and obesity. This aligns with previous studies, which have reported a greater emphasis on diet, body weight, and physical activity as key determinants of DM risk.30,31 In contrast, the contribution of smoking and alcohol consumption to DM risk was largely overlooked. The particularly low recognition of alcohol consumption as a DM risk factor may partially reflect sociocultural and religious factors within Iraqi society, where alcohol use is less openly discussed in public health discourse compared with dietary habits and obesity. Similarly, smoking may be insufficiently emphasized in diabetes-related health education despite its established metabolic and cardiovascular effects. Awareness of non-modifiable risk factors, including age over 40 years and family history of DM, was also limited. Interestingly, although 48.4% of participants reported having a family history of DM, only 40.0% recognized family history as a DM risk factor. This finding suggests that personal exposure to diabetes within the family may not necessarily translate into accurate understanding of inherited or familial susceptibility. This pattern is consistent with findings from studies conducted in Poland and Ethiopia, where participants similarly underestimated the role of smoking, alcohol use, age, and genetic predisposition in DM risk.32,33 Taken together, these findings indicate a need for targeted public health messaging that addresses less well-recognized risk factors, with the aim of supporting prevention efforts and facilitating earlier detection. These findings may also reflect differences in health literacy and unequal exposure to evidence-based public health information, particularly regarding less visible symptoms and long-term complications of DM. 34
The quantile regression analysis identified a medical background, whether professional or academic, as one of the strongest predictors of higher DM knowledge. This finding is consistent with evidence from a Chinese study showing substantially lower knowledge levels among non-medical compared with medical students. 35 Beyond formal training, prior exposure to information about DM prevention and reliance on scientific sources were also associated with higher knowledge scores. Similar associations have been reported in previous research, where individuals with diabetes-related education or training demonstrated greater understanding of the condition, 27 and where access to reliable information sources was linked to improved knowledge. 29 This finding is particularly important given the growing reliance on informal and social media-based information sources, which may contribute to misinformation and inconsistent understanding of DM risk factors and prevention strategies. Together, these findings suggest that structured education and the credibility of information sources play a central role in shaping DM-related knowledge, while reliance on non-scientific sources may contribute to misinformation and persistent knowledge gaps in the general population.
Marital status emerged as a significant correlate of DM knowledge, with unmarried participants demonstrating lower knowledge scores. One possible explanation is that marriage and partnership may increase exposure to health-related information through shared decision-making, caregiving roles, and greater engagement with health services, whereas single individuals may have fewer opportunities for informal health information exchange. 36 In contrast, and consistent with findings from non-diabetic populations in Saudi Arabia, 28 DM knowledge in the present study was not significantly associated with age, gender, or income level. This pattern suggests that social context and access to information may be more influential determinants of DM knowledge than demographic characteristics alone.
The binary logistic regression analysis showed that higher DM knowledge was significantly associated with more positive attitudes toward the condition. Practically, the observed OR indicates that each 1-point increase in knowledge score was associated with approximately 17.9% higher odds of having a positive attitude toward DM. Similarly, participants with a medical background were nearly four times more likely to demonstrate favorable attitudes toward DM compared with non-medical participants. This relationship suggests that understanding DM may shape perceptions of personal relevance and controllability, which are important precursors to engagement in preventive behaviors. Participants with a medical background were significantly more likely to exhibit favorable attitudes, whereas those with a high school education or less had lower odds of positive attitudes. Similar associations between DM knowledge, educational attainment, and attitudes have been reported in previous studies, reinforcing the link between understanding of the disease and more constructive perspectives toward prevention and management.29,33,37
Older age emerged as a significant predictor of less favorable attitudes toward DM. Older adults may also have reduced engagement with digital and social media-based health education platforms, which currently represent major channels for dissemination of preventive health information. This finding is consistent with evidence suggesting that older adults may face greater barriers to engaging with preventive health behaviors, including fatigue, reduced motivation, functional limitations, and the presence of competing health priorities. 25 Such barriers may shape attitudes by lowering perceived feasibility or relevance of prevention efforts. In contrast, attitudes toward DM were not significantly associated with gender, income level, place of residence, comorbidities, family history of DM, or prior exposure to information. Taken together, these findings suggest that attitudes may be shaped less by sociodemographic or medical characteristics and more by how DM-related information is understood, interpreted, and integrated, reinforcing the central role of knowledge quality in supporting positive preventive orientations.
The present findings have several practical public health implications. Educational interventions should place greater emphasis on under-recognized DM risk factors, including smoking, alcohol consumption, family history, and older age, as well as less visible symptoms and complications such as blurred vision, kidney disease, and hypertension. Public health campaigns may particularly benefit from targeting individuals without medical backgrounds and older adults, who demonstrated lower levels of knowledge or less favorable attitudes toward DM. In addition, the observed association between non-scientific information sources and poorer knowledge highlights the importance of promoting credible, evidence-based health communication through healthcare professionals, academic institutions, and reliable digital platforms to counter misinformation and improve DM awareness.
Strengths, limitations, and future work
This study has several notable strengths, including the large sample size of 874 participants and the use of a questionnaire specifically developed for the Iraqi population. The instrument was constructed using a rigorous framework that incorporated expert content validation and a systematic translation and back-translation process, which is widely regarded as best practice for ensuring the accuracy and cultural appropriateness of research tools. 38
Several limitations should also be acknowledged. The cross-sectional design limits the ability to establish causal relationships between DM knowledge, attitudes, and preventive behaviors. In addition, the use of online recruitment and self-reported data may have introduced selection, recall, and social desirability biases. The predominance of urban, highly educated, and medically affiliated participants may further limit the generalizability of the findings to the broader Iraqi population, particularly underserved or rural communities. Furthermore, online recruitment may have contributed to a digital divide by underrepresenting individuals with limited internet access or lower digital literacy. Convenience sampling and voluntary participation may also have preferentially attracted individuals with greater health awareness or interest in health-related topics, potentially resulting in overestimation of DM-related knowledge and attitudes.
Future research should build on these findings by employing longitudinal designs to better examine causal relationships between DM-related knowledge, attitudes, and the adoption of preventive practices among non-diabetic individuals in Iraq. Incorporating objective health indicators, such as glycosylated hemoglobin, could strengthen the validity of self-reported data. Moreover, interventional studies are warranted to assess the effectiveness of evidence-based educational programs, particularly those targeting older adults and individuals with lower educational attainment, in addressing identified knowledge gaps and supporting DM prevention efforts.
Conclusion
Non-diabetic adults included in this study demonstrated awareness of several fundamental concepts related to DM; however, important gaps remained regarding symptoms, complications, and several key risk factors. Knowledge was higher among those with a medical background and among participants who relied on scientific sources of information. More positive attitudes toward DM were linked to better knowledge, younger age, and higher educational attainment. Taken together, these findings point to a clear need for practical, evidence-based public health education that focuses on early symptoms, complications, and under-recognized risk factors. Strengthening DM knowledge in non-diabetic populations may support prevention efforts and help reduce the future burden of the disease. However, given the predominance of urban, educated, and medically affiliated participants in the study sample, the findings may not fully represent the broader Iraqi population, particularly underserved or rural communities.
Supplemental Material
sj-docx-1-imr-10.1177_03000605261463409 - Supplemental material for Diabetes knowledge and attitudes among non-diabetic adults in Iraq: A cross-sectional study of awareness, risk perception, and preventive understanding
Supplemental material, sj-docx-1-imr-10.1177_03000605261463409 for Diabetes knowledge and attitudes among non-diabetic adults in Iraq: A cross-sectional study of awareness, risk perception, and preventive understanding by Walid A. Al-Qerem, Alaa H. Alsajri, Anan S. Jarab, Judith Eberhardt, Sura B. Subhi, Fatima S. Dahaam, Sarah A. Jasim, Tabarak W. Mohamed, Dina K. Al-Hashaki, Noor M. Alkhawwam and Lama F. Sawaftah in Journal of International Medical Research
Supplemental Material
sj-docx-2-imr-10.1177_03000605261463409 - Supplemental material for Diabetes knowledge and attitudes among non-diabetic adults in Iraq: A cross-sectional study of awareness, risk perception, and preventive understanding
Supplemental material, sj-docx-2-imr-10.1177_03000605261463409 for Diabetes knowledge and attitudes among non-diabetic adults in Iraq: A cross-sectional study of awareness, risk perception, and preventive understanding by Walid A. Al-Qerem, Alaa H. Alsajri, Anan S. Jarab, Judith Eberhardt, Sura B. Subhi, Fatima S. Dahaam, Sarah A. Jasim, Tabarak W. Mohamed, Dina K. Al-Hashaki, Noor M. Alkhawwam and Lama F. Sawaftah in Journal of International Medical Research
Footnotes
Ethical considerations
Ethical approval was granted by the IRB and the Deanship of Research at Al-Rasheed University College (reference number RUCPD10012601). The study was conducted in accordance with the Declaration of Helsinki.
Consent to participate
Electronic informed consent was obtained from all participants prior to participation.
Consent for publication
Electronic informed consent was obtained from all participants prior to participation.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request and subject to institutional approval.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.