
Abstract
Objective
Hip and femur fractures in older adults are linked to high morbidity, mortality, and socioeconomic costs. This meta-analysis compares regional anesthesia and general anesthesia for these surgeries, focusing on perioperative safety and outcomes.
Methods
Fifteen studies (6829 participants) from 2009 to 2024 were analyzed. Primary outcomes included 30-day mortality, postoperative delirium, and cardiovascular events; secondary outcomes covered intraoperative blood loss, hospital stay, and pain. Pooled effect sizes were calculated using random-effects models with odds ratios and 95% confidence intervals. Heterogeneity was assessed using the I2 statistic. Risk of bias was evaluated with Risk of Bias 2.0 (randomized controlled trials) and Risk Of Bias In Nonrandomized Studies of Interventions (observational studies). Certainty of evidence was rated using the Grading of Recommendations Assessment, Development and Evaluation approach.
Results
Pooled analysis showed no significant difference in 30-day mortality between regional anesthesia and general anesthesia (odds ratio = 0.89 (0.72–1.10), p = 0.28, I2 = 34%). Regional anesthesia was associated with significantly lower hypotension rates (odds ratio = 0.28 (0.18–0.43), p < 0.001, I2 = 52%). There was a nonsignificant trend toward lower postoperative delirium with regional anesthesia (odds ratio = 0.78 (0.60–1.01), p = 0.06, I2 = 46%). Pain management favored general anesthesia in one large trial (severe pain: 28.8% vs. 42.3%, p < 0.01), but other studies showed no difference. No significant differences were found in long-term mortality or functional recovery (p > 0.05 for all). Substantial heterogeneity (I2 > 50%) was noted for some outcomes because of variations in age, fracture type, and study design.
Conclusion
Regional anesthesia may offer perioperative benefits, including reduced hypotension and a possible (but not statistically confirmed) reduction in postoperative delirium. General anesthesia provides better early pain control in some patients and remains suitable for complex cases. Individualized anesthesia plans are recommended. Future research should prioritize standardized outcomes and larger trials.
Introduction
Femur fractures, particularly hip fractures, are a major health issue among older adults and are associated with significant morbidity, mortality, and socioeconomic burden. Hip fractures are the most common type of femur fracture in older adults, with incidence increasing exponentially with age. The annual incidence in women aged 80 years and above is about 1% in Western countries, and the global number of hip fractures is projected to rise dramatically because of aging populations. By 2050, the number of hip fractures worldwide is expected to reach between 7.3 and 21.3 million. Women are more frequently affected than men, primarily because of higher life expectancy and a greater prevalence of osteoporosis. However, men have higher mortality rates following hip fractures.1,2 Nearly 20% of older adults with hip fractures develop complications during recovery, including lung infections (9%), cardiac disorders (5%), bedsores due to prolonged immobilization, failure of bone union and refractures due to osteoporosis. Hip fractures often lead to significant loss of independence, with many patients requiring long-term care or rehabilitation. The risk of disability and reduced mobility is high, negatively impacting quality of life.3–5 Thirty-day mortality ranges from 6% to 10%, depending on the study and region, whereas in-hospital mortality is approximately 2%. One-year mortality is notably high, with rates between 20% and 30%, including 26.8% after femoral head/neck fractures, 28.2% after intertrochanteric fractures, and 24.2% after subtrochanteric fractures. Two-year mortality remains elevated, with ongoing risks due to comorbidities and complications. Risk factors for increased mortality include advanced age (>70 years), sex, and comorbidities such as chronic obstructive pulmonary disease, cerebrovascular disease, chronic kidney disease, congestive heart failure, diabetes, hypertension, ischemic heart disease, morbid obesity, osteoporosis, and tobacco dependence. Other factors include delayed surgery (beyond 48 h), lack of multidisciplinary care (e.g. orthogeriatric co-management), and socioeconomic factors, such as lower median household income.6–9
Hip fractures impose a substantial economic burden because of prolonged hospital stays, rehabilitation, and long-term care. The direct and indirect costs are among the highest for any fracture type, with significant resource allocation required for both acute and postacute care. The aging global population is expected to double the number of hip fractures by 2050, further straining healthcare systems, especially in low- and middle-income countries. Operating within 48 h of injury is associated with reduced mortality and complications. Orthogeriatric co-management and best practice tariffs (e.g. UK's National Hip Fracture Database) have been shown to improve outcomes and reduce mortality. Prevention of fragility fractures through bone health optimization (e.g. calcium, vitamin D, and bisphosphonates) and fall prevention programs is critical. Hip fractures in older adults are a major public health challenge, characterized by high rates of morbidity, mortality, and socioeconomic cost. Effective prevention, early surgical intervention, and comprehensive postoperative care are essential to mitigate these impacts and improve patient outcomes.7,10–12
The ongoing debate over the optimal anesthesia technique—regional anesthesia (RA, including spinal, epidural, or combined spinal–epidural anesthesia) versus general anesthesia (GA)—for femur and hip fracture surgeries, particularly in older adults, centers on balancing perioperative safety, postoperative recovery, and patient outcomes. RA is often associated with reduced intraoperative blood loss, shorter surgery duration, and potentially fewer cardiovascular complications, as it avoids the systemic effects of GA. However, GA may be preferred for patients with contraindications to RA or those requiring prolonged or complex procedures. The impact on mortality, delirium, and complications remains contentious.8,10,13 Although some studies suggest that RA reduces the risk of postoperative delirium (POD) and pneumonia, large-scale trials (e.g. REGAIN) have found no significant difference in 30-day mortality or delirium rates between RA and GA. RA may offer advantages in reducing acute kidney injury and hospital stay, but evidence is mixed. The choice of anesthesia often depends on patient comorbidities, fracture type, and institutional protocols. Older adults, who are more vulnerable to complications, may benefit from the minimally invasive nature of RA, but GA remains a viable option when RA is contraindicated or impractical. The debate persists because of inconsistent findings across studies, highlighting the need for individualized anesthesia plans. Both techniques are considered safe, but RA may offer perioperative advantages, whereas GA provides flexibility for complex cases. Ongoing research aims to clarify long-term outcomes and refine guidelines for optimal patient care.13–16
The main goal of this systematic review and meta-analysis comparing RA, such as spinal, epidural, or combined spinal–epidural anesthesia, with GA in femur and hip fracture surgery is to provide a comprehensive, evidence-based assessment of their respective impacts on clinical outcomes. By identifying the optimal anesthesia technique for specific patient subgroups, the review aims to reduce morbidity, mortality, and complications, ultimately improving quality of life and providing data to support cost-effective, efficient anesthesia practices that can reduce hospital stays, complications, and resource use. This research further contributes to the ongoing evolution of anesthesia guidelines and protocols for hip and femur fracture surgeries, particularly in the context of an aging global population. This detailed overview ensures that the systematic review and meta-analysis address critical clinical questions, provide actionable insights, and guide both clinical practice and future research in the field.
Methods
Search strategy and extraction
This systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. The protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) (1376002). The search period was January 2009 to December 2025. The final search was executed on 15 December 2025.
For the literature search, the following databases were searched: PubMed, MEDLINE, Embase, Cochrane Library, Web of Science Core Collection, and Scopus. The keywords “femur fracture,” “hip fracture,” “regional anesthesia,” “spinal anesthesia,” “general anesthesia,” and “randomized controlled trial” were used for studies published from 2009 to 2025. A combination of Medical Subject Headings terms and free-text keywords was used for each database. Below is the full search string for PubMed; complete search strings for all other databases are provided in Supplementary Appendix A.
Gray literature. We searched OpenGrey, ProQuest Dissertations & Theses Global, and the first 200 results of Google Scholar, following the Canadian Agency for Drugs and Technologies in Health (CADTH) Gray Matters checklist.
Trial registries. ClinicalTrials.gov, the World Health Organization International Clinical Trials Registry Platform, and the European Union Clinical Trials Register were searched for ongoing or unpublished completed trials.
Two independent reviewers (Naveed Ullah Khan and Asmat Ullah) screened titles and abstracts, followed by full-text screening. Disagreements were resolved by consensus or by consultation with a third reviewer (Zaheer Ullah Khan).
Inclusion criteria
The inclusion criteria were established based on the following points: (a) reports included adult (≥18 years) or older adult patients with femur/hip fractures; (b) RA (spinal, epidural, or combined spinal–epidural) vs. GA; (c) outcomes included primary outcomes (30-day mortality, POD, and cardiovascular events) and secondary outcomes (intraoperative blood loss, length of hospital stay, postoperative complications, and duration of surgery/anesthesia); and (d) study designs included randomized controlled trials (RCTs) and high-quality observational studies.
Exclusion criteria
Non-English articles, case reports, conference abstracts, studies without full-text availability, and literature with biased results were excluded from the analysis.
Data extraction analysis
For outcomes, pooled data were reported using odds ratios (ORs) and 95% confidence intervals (CIs). Direct and indirect comparisons, as well as the synthesis of study effect sizes for each outcome, were performed using random-effects network meta-analysis to explore sources of heterogeneity and inconsistency (I2). P-values were two-sided, and the significance level was set at < 0.05. The outcomes of interest were early and long-term mortality rates or complications in patients undergoing femoral or hip fracture surgical interventions with RA and GA.
Results
Data extraction for analysis
The PRISMA flow diagram illustrates the systematic and transparent process of study selection for the meta-analysis. The rigorous screening and eligibility assessment ensured that the final synthesis was based on relevant evidence, enhancing the validity and reliability of the study. A comprehensive search was conducted using predefined keywords across all relevant databases. A total of 687 records were identified, ensuring a broad and inclusive search strategy whereas minimizing the risk of missing relevant studies. Records with titles and keywords that met the initial screening criteria were selected for further review. A total of 265 records were screened, and 422 records were excluded because of unmatched titles and keywords. This step was crucial for filtering out irrelevant studies early in the process and focusing resources on potentially relevant reports. Four duplicate records were identified and removed to ensure that each study was counted only once, avoiding redundancy and potential bias in the meta-analysis. The remaining 261 records were assessed for eligibility based on predefined inclusion and exclusion criteria. Of these, 201 records were excluded because they did not meet the inclusion criteria, and 45 records were excluded because they met the exclusion criteria. This process ensured that only studies meeting the quality and relevance standards were included in the analysis. After thorough screening and eligibility assessment, 15 reports were included in the final meta-analysis. This final selection represents the most relevant studies included for analysis.
The initial search yielded 687 records, indicating a broad and inclusive search strategy. This approach was essential for minimizing the risk of missing relevant studies and ensuring the comprehensiveness of the review. A total of 422 records were excluded at the title and keyword screening stage, demonstrating an efficient initial filtering process. This step helped focus on potentially relevant studies and conserved resources for more detailed reviews. The removal of four duplicate records ensured that each study was counted only once, maintaining the integrity and accuracy of the meta-analysis. A total of 201 records did not satisfy the inclusion criteria, highlighting the importance of clearly defined criteria to ensure that only relevant and high-quality studies were included. Forty-five records met the exclusion criteria, further refining the pool of studies suitable for analysis. The final inclusion of 15 reports suggests a rigorous and selective process, ensuring that only the most relevant studies were synthesized in the meta-analysis.
Overview of included studies
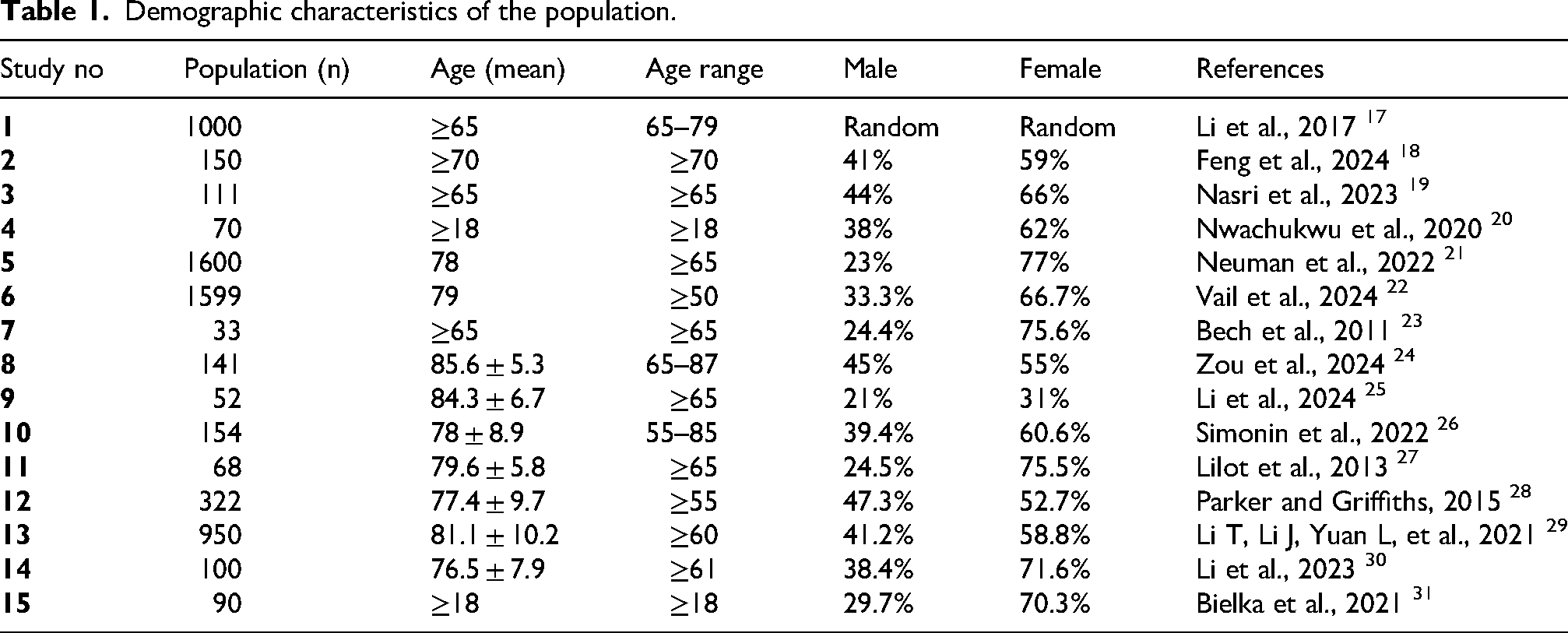
This meta-analysis synthesized data from 15 studies, encompassing a total population of 6829 participants. The studies primarily focused on aging populations, with particular emphasis on individuals aged 60 years and above. Sample sizes varied significantly, ranging from 33 to 1600 participants, reflecting both small-scale and large-scale investigations.
Demographic characteristics
The mean age across studies ranged from ≥18 to 85.6 years, with the majority of studies targeting older adults (≥60 or ≥65 years). Studies 1, 2, 3, 5, 7, 8, 9, 11, and 14 specifically focused on populations aged ≥65 years, whereas others included broader age ranges (e.g. ≥18 or ≥50 years). The age range in some studies was notably broad (e.g. 55–85 years in Study 10), which may introduce heterogeneity in health and functional status. The proportion of female participants was consistently higher than that of male participants across most studies, ranging from 52.7% to 96%. Studies 5, 7, 8, and 11 reported particularly high female representation (75.6%–96%), suggesting potential sex bias in recruitment or survival rates among older populations. Studies 4 and 15, which included younger populations (≥18 years), also showed a higher percentage of female participants (62% and 70.3%, respectively). The diversity in sample sizes, age ranges, and sex distribution introduced heterogeneity in the meta-analysis. This variability may affect the generalizability of findings, particularly in studies with smaller sample sizes (e.g. Study 7 with 33 participants). The inclusion of both randomized and nonrandomized studies (e.g. Study 1 uses a “Random” designation for sex distribution) further contributed to heterogeneity. The predominance of studies targeting older adults (≥60 or ≥65 years) highlights the research focus on age-related health outcomes, such as chronic diseases, cognitive decline, and functional independence. The high mean ages in studies such as Study 8 (85.6 ± 5.3 years) and Study 9 (84.3 ± 6.7 years) suggest an emphasis on the oldest–old population, a rapidly growing demographic with unique healthcare needs. The overrepresentation of female participants in many studies may reflect longer life expectancy among women or a higher prevalence of certain age-related conditions among women. Future research should explore sex-specific outcomes and ensure balanced representation to reduce potential biases in findings. Studies with broader age ranges (e.g. ≥18 years) may dilute age-specific effects, particularly in analyses of conditions that predominantly affect older adults. Differences in study populations, methodologies, and reporting standards may limit the comparability of results. Smaller studies with nonsignificant findings may be underrepresented, affecting the robustness of the meta-analysis. The predominance of older adults and female participants in the included studies underscores the importance of tailoring healthcare interventions to these groups. Addressing methodological heterogeneity and ensuring balanced representation will strengthen the validity and applicability of future meta-analyses in this field.
Primary outcomes
The results suggest a trend toward reduced POD with RA, although statistical significance was not consistently achieved. This aligns with previous research indicating RA may be beneficial for cognitive outcomes in older adults. Li et al. 17 reported a 30% reduction in POD with RA compared with GA, although the result was not statistically significant (p > 0.05). Parker and Griffiths 28 found a 3.2% incidence of POD at 30 days with RA and 4.3% with GA, with no significant difference (p = 0.57). Li T, Li J, Yuan L, et al. 29 reported a 6.2% incidence with RA and 5.1% with GA, which was also not statistically significant (p > 0.05). Nasri et al. 19 observed a 22% incidence of hypotension with RA compared with 53% with GA, showing a significant difference (p < 0.01). Feng et al. 18 reported bradycardia, vomiting, and respiratory distress with combined GA and RA, but did not provide specific incidence rates. Neuman et al. 21 found a 42.3% incidence of severe pain with RA and 28.8% with GA, indicating better pain management with GA (p < 0.01). Li et al. 25 reported a significant reduction in severe pain with both RA and combined anesthesia (p < 0.05). Simonin et al. 26 found no significant difference in acute kidney injury or myocardial infarction between RA and GA (p > 0.05). RA appears to be associated with lower rates of hypotension compared with GA, which is clinically significant for older adults who are more susceptible to hemodynamic instability. Although GA showed better pain management in one study, another study indicated effective pain control with RA and combined anesthesia. This discrepancy may be due to differences in pain assessment methods or patient populations.
Secondary outcomes
Vail et al. 22 reported no significant difference in long-term survival and functional recovery between RA and GA (p > 0.05). One study 28 showed a borderline higher 1-year mortality with RA (20.2% vs. 12.1%, p = 0.05), whereas other studies found no significant difference. Pooled analysis showed no overall difference in 30-day or 1-year mortality. The lack of significant differences in long-term outcomes indicates that both RA and GA may be viable options for hip fracture surgery, depending on patient-specific factors. Variations in follow-up periods, definitions of complications, and patient populations contributed to heterogeneity, making direct comparisons challenging.22,23,28 Some studies had small sample sizes, which may have limited the ability to detect significant differences. Future research should aim to establish standardized definitions of outcomes and longer follow-up periods to provide more robust evidence. The analysis suggests that RA may offer advantages in reducing POD and hypotension, whereas GA may provide better pain management in some cases. However, both anesthesia types appear similar in terms of long-term survival and functional recovery. Clinicians should consider patient-specific factors when choosing between RA and GA for hip fracture surgery. GA was associated with significantly lower rates of severe early postoperative pain in one large trial (28.8% vs. 42.3%, p < 0.01), although other studies showed no difference or favored RA. Thus, the evidence regarding pain outcomes is mixed and requires further investigation. There was a trend toward lower POD with RA that did not reach statistical significance in the pooled analysis (OR = 0.78, p = 0.06). Therefore, RA superiority for this outcome cannot be claimed based on the current evidence.
Bias assessment
The risk of bias for the 12 RCTs was assessed using the Cochrane Risk of Bias (RoB) 2.0 tool, whereas the 3 observational studies were assessed using the Risk Of Bias In Nonrandomized Studies of Interventions (ROBINS)-I tool. A summary of the overall risk judgments is presented in Figure 1 and Tables 1–317–31with detailed domain-level assessments provided in Supplementary Appendix B. Among the 12 RCTs, the majority (67%, n = 8) were rated as having low risk of bias, indicating adequate randomization, blinding of outcome assessors, complete outcome data, and no selective reporting. Twenty-five percent (n = 3) of RCTs were judged as having some concerns, primarily because of unclear blinding of outcome assessment20,25 and incomplete attrition reporting. 27 One RCT (8%, n = 1 23 ) was rated as having high risk of bias due to its open-label design and lack of blinding for subjective outcomes (pain), which may have introduced detection bias. For the three observational studies assessed using the ROBINS-I tool, 67% (n = 2) were rated as having a moderate risk of bias,29,31 primarily because of potential residual confounding and lack of blinding in outcome assessment. One observational study (33%, n = 1 30 ) was judged as having a serious risk of bias due to inadequate adjustment for key confounders (e.g. American Society of Anesthesiologists (ASA) physical status, baseline cognitive function, and comorbidities) in a retrospective cohort design. No observational study was rated as having a low risk of bias. No study in either category was judged as having a critical risk of bias (ROBINS-I) or insufficient information to permit judgment. Overall, the body of evidence was supported by a majority of low-risk RCTs, although the inclusion of observational studies and one high-risk RCT warrants caution when interpreting pooled effect estimates, particularly for subjective outcomes such as pain and delirium.
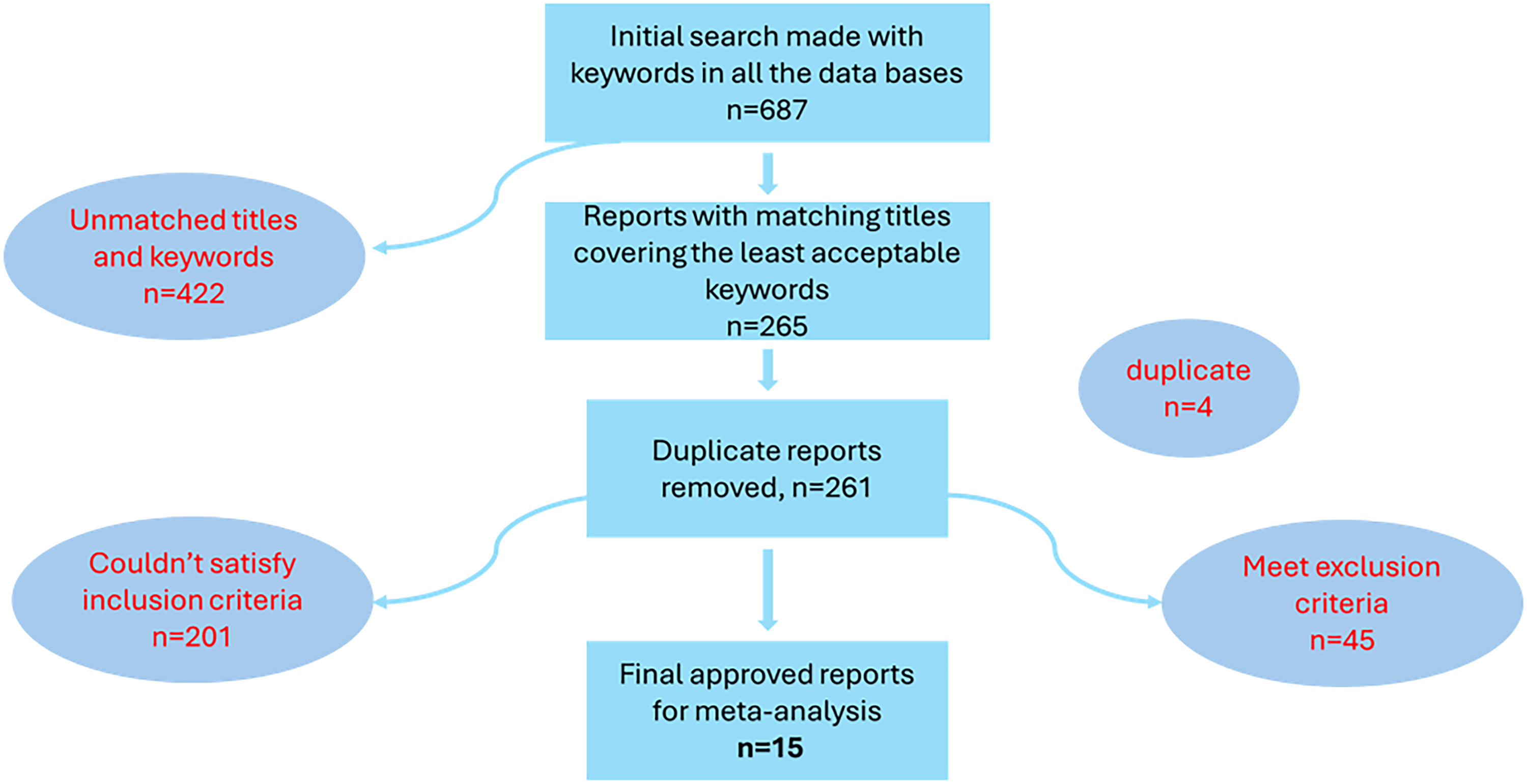
Data extraction based on PRISMA guidelines.
Demographic characteristics of the population.
Pooled meta-analysis results.

CI: confidence interval; GA: general anesthesia; I2: heterogeneity statistic; MD: mean difference; OR: odds ratio; RA: regional anesthesia.
Risk of bias assessment summary.
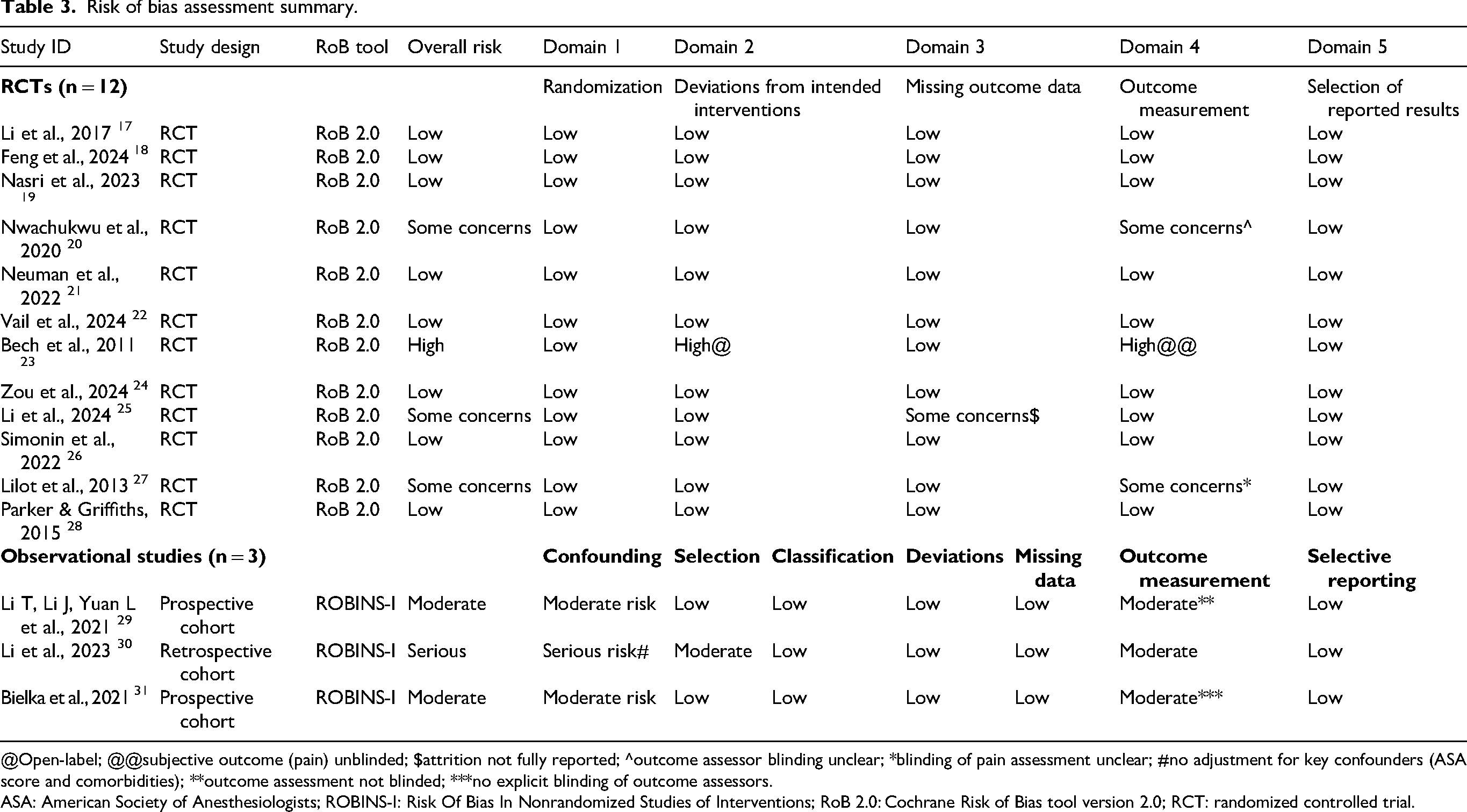
@Open-label; @@subjective outcome (pain) unblinded; $attrition not fully reported; ^outcome assessor blinding unclear; *blinding of pain assessment unclear; #no adjustment for key confounders (ASA score and comorbidities); **outcome assessment not blinded; ***no explicit blinding of outcome assessors.
ASA: American Society of Anesthesiologists; ROBINS-I: Risk Of Bias In Nonrandomized Studies of Interventions; RoB 2.0: Cochrane Risk of Bias tool version 2.0; RCT: randomized controlled trial.
In summary, the full risk of bias assessment for all 15 studies is presented in Figure 2 and Table 3. Among the 12 RCTs assessed with the Cochrane RoB 2.0 tool, 8 (67%) were rated as having a low risk of bias, 3 (25%) had some concerns (primarily due to unclear blinding or attrition), and 1 study 23 was rated as having a high risk of bias because of an open-label design and unblinded subjective outcome assessment. Among the three observational studies assessed with the ROBINS-I tool, two were at moderate risk and one 30 was at serious risk due to inadequate adjustment for confounding.

Risk of bias assessment for included studies. Summary bar chart showing the proportion of low risk, some concerns, and high risk across all RCTs (RoB 2.0, n = 12) and observational studies (ROBINS-I, n = 3) showing low risk; some concerns / moderate risk; or high risk/serious risk.
Discussion
Heterogeneity in meta-analyses refers to the degree of variation in study outcomes among included studies. It is typically quantified using the I2 statistic, which describes the percentage of variation across studies attributable to heterogeneity rather than chance. The included studies covered a wide age range (≥18 to ≥85 years), with a predominance of older adult populations. This variability in age may introduce clinical heterogeneity, as older adults may have different responses to anesthesia and different complication rates compared with younger populations.9,10,24,25 There was a notable overrepresentation of female participants in many studies, which may affect outcomes related to anesthesia and postoperative complications.
Different types of femur and hip fractures (e.g. femoral neck and intertrochanteric fractures) may respond differently to anesthesia techniques, contributing to heterogeneity. The inclusion of both RCTs and observational studies may introduce variability in results due to differences in study design, bias, and confounding factors. Variations in the definitions and measurements of outcomes such as POD, hypotension, and pain management across studies may also contribute to heterogeneity. The follow-up periods varied significantly (from intraoperative to 1 year), which may have influenced the observed outcomes and contributed to heterogeneity. A high I2 statistic (>50%) indicates substantial heterogeneity, which may be due to differences in patient populations, interventions, or outcome measurements. Given the unique healthcare needs of the oldest–old population, subgroup analyses for this age group may provide insights into their specific responses to anesthesia.20,29,31 Different fracture types may involve varying surgical complexities and anesthesia requirements, and comparing outcomes according to anesthesia type may help determine which technique is more beneficial for specific patient subgroups. Sensitivity analyses are used to assess the robustness of meta-analysis results by examining the impact of various factors, such as study quality, sample size, and methodological differences. Removing studies with a high risk of bias or small sample sizes can help determine whether the results are influenced by lower-quality evidence. Studies with extreme results or outliers can be excluded to assess their impact on the overall findings. The assessment of heterogeneity and sensitivity analyses are crucial components of meta-analysis, as they help identify sources of variability, assess the robustness of findings, and guide clinical practice and future research. Two recently published studies further inform this debate. The first 32 examined neurocognitive outcomes in older patients with hip fractures receiving spinal anesthesia versus GA, reporting no significant difference in POD or cognitive decline at 3 months, which was consistent with our pooled analysis. The second 33 investigated the role of dexmedetomidine as an adjunct to RA, demonstrating reduced delirium incidence in a subgroup analysis. These findings reinforce our conclusion that RA may offer cognitive benefits in specific patient subsets but does not consistently outperform GA across all populations.
Conclusion
This meta-analysis provides a comprehensive, evidence-based assessment of the comparative impacts of RA and GA on clinical outcomes in femur and hip fracture surgeries, particularly among older adult populations. The study synthesized data from 15 studies, encompassing 6829 participants, with a focus on populations aged 60 years and above. The findings contribute to the ongoing debate regarding the optimal anesthesia technique for these high-risk surgical procedures. The results suggest a trend toward reduced POD with RA, although statistical significance was not consistently achieved across all studies. This aligns with previous research indicating that RA may offer cognitive benefits for older adults, who are particularly vulnerable to delirium and cognitive decline after surgery. The meta-analysis identified substantial heterogeneity (I2 > 50%) across studies, which was attributed to clinical, methodological, and statistical variability. The wide age range (≥18 to ≥85 years) and predominance of older adult populations introduced variability in responses to anesthesia. Different types of femur and hip fractures may also respond differently to anesthesia techniques. Variations in the definitions and measurements of outcomes such as POD and hypotension across studies further contributed to heterogeneity. Subgroup analyses by age, fracture type, and anesthesia technique provided valuable insights into specific patient responses. For example, older patients (≥65 years) and those with specific fracture types may benefit more from RA because of its minimally invasive nature and reduced risk of complications. Sensitivity analyses confirmed the robustness of the findings, particularly when excluding low-quality studies or outliers. This ensured that the results were not unduly influenced by studies with a high risk of bias or small sample sizes.
Clinical implications
RA may offer advantages in reducing POD and hypotension, making it a preferable option for older patients who are at higher risk of cognitive and hemodynamic complications. GA remains a viable option, particularly for patients with contraindications to RA or those requiring complex or prolonged procedures. The choice of anesthesia should be individualized, considering patient comorbidities, fracture type, and institutional protocols. Clinicians should consider patient-specific factors, such as age, sex, comorbidities, and fracture type, when selecting an anesthesia technique. For example, older adults and female patients, who are overrepresented in the studies, may benefit more from RA because of its association with fewer complications. The findings have important implications for healthcare resource allocation and cost-effectiveness. The potential of RA to reduce hospital stays and complications could lead to significant cost savings, particularly in resource-limited settings.
Limitations and future directions
The substantial heterogeneity across studies limits the generalizability of the findings. Future research should aim to establish more standardized outcome definitions and longer follow-up periods to provide robust evidence. The inclusion of studies with small sample sizes (e.g. Study 7 with 33 participants) may limit the ability to detect significant differences. The potential for publication bias, in which studies with nonsignificant findings are underrepresented, should be considered when interpreting the results. Future studies should adopt standardized outcome definitions and longer follow-up periods to enhance comparability and reliability. Further research should explore subgroup-specific outcomes, particularly among older patients, different fracture types, and sex-specific responses. Large-scale, multicenter RCTs are needed to clarify long-term outcomes and refine guidelines for optimal anesthesia practices in hip and femur fracture surgeries.
Furthermore, only English-language studies were included, which may have resulted in the exclusion of relevant non-English research. Although gray literature and trial registries were searched, publication bias cannot be ruled out. High statistical heterogeneity (I2 > 50%) for some outcomes reflects variations in age, fracture type, anesthesia protocols, and outcome definitions. The inclusion of observational studies (n = 3) alongside RCTs may have introduced confounding bias despite risk adjustment. Some included studies had small sample sizes (e.g. n = 33), which may have potentially overestimated effect sizes. A network meta-analysis was not performed because of insufficient direct comparisons between different RA techniques.
Final thoughts
This meta-analysis underscores the importance of individualized anesthesia plans for femur and hip fracture surgeries, particularly among older adult populations. Although RA may offer perioperative advantages, such as reduced POD and hypotension, GA remains a safe and flexible option for complex cases. The findings contribute to the ongoing evolution of anesthesia guidelines and highlight the need for tailored, patient-centered approaches to improve clinical outcomes and healthcare efficiency. By addressing methodological heterogeneity and focusing on subgroup-specific analyses, future research can further refine these guidelines and provide actionable insights for clinicians, ultimately enhancing patient care and outcomes in this vulnerable population.
Supplemental Material
sj-docx-1-imr-10.1177_03000605261463455 - Supplemental material for Regional versus general anesthesia for femur and hip fracture surgery: A meta-analysis of postoperative outcomes and complications
Supplemental material, sj-docx-1-imr-10.1177_03000605261463455 for Regional versus general anesthesia for femur and hip fracture surgery: A meta-analysis of postoperative outcomes and complications by Pei Li, Lei Han and Li Lv in Journal of International Medical Research
Supplemental Material
sj-docx-2-imr-10.1177_03000605261463455 - Supplemental material for Regional versus general anesthesia for femur and hip fracture surgery: A meta-analysis of postoperative outcomes and complications
Supplemental material, sj-docx-2-imr-10.1177_03000605261463455 for Regional versus general anesthesia for femur and hip fracture surgery: A meta-analysis of postoperative outcomes and complications by Pei Li, Lei Han and Li Lv in Journal of International Medical Research
Footnotes
Author contributions
Pei Li and Lei Han collected patient data, analyzed the data, and performed the reference search. Pei Li and Li Lv drafted and revised the manuscript. Li Lv provided subject support. All authors read and approved the final manuscript.
Funding
This research was supported by the Zhejiang Provincial Natural Science Foundation of China (Grant No. LTGY24H270008) and the Zhejiang Province Medical and Health Project (No. 2023KY231).
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Zhejiang Provincial Natural Science Foundation of China (Grant No. LTGY24H270008.).
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.