
Abstract
Background
Long-term combination anti-tuberculosis regimens may lead to various types and severities of adverse drug reactions, potentially resulting in treatment discontinuation, interruption, or prolonged therapy.
Aim
Considering the lengthy duration of anti-tuberculosis combination regimens, it is crucial to monitor adverse drug reactions occurring during such treatment. This is the first hospital-based study conducted in western China to report adverse drug reactions and assess their prevalence and impact among children with tuberculosis receiving first-line anti-tuberculosis therapy.
Methods
A retrospective study was conducted on registered tuberculosis cases at the Children's Hospital of Chongqing Medical University from 2014 to 2023. Data on demographic characteristics, treatment regimens, and adverse drug reactions were collected and evaluated. Statistical methods were used to analyze factors associated with adverse drug reactions.
Results
Among 546 patients receiving anti-tuberculosis therapy, adverse drug reactions were reported in 476 (87.18%). Hyperuricemia was the most common adverse drug reaction (44.26%), followed by elevated liver enzymes without jaundice and elevated bile acids (10.38%) and leukopenia (8.31%). Most adverse drug reactions occurred within the first month of treatment (51.48%), whereas 33.44% persisted for >6 months. Pyrazinamide was the most frequently suspected causative drug (7.47%). Univariate analysis showed significantly higher adverse drug reaction rates among children aged 11–18 years, those with severe tuberculosis, those receiving the isoniazid + rifampicin + pyrazinamide + ethambutol + linezolid regimen, those on a recommended dose of rifampicin, and those receiving a high dose of pyrazinamide (p < 0.05). Logistic regression identified age (odds ratio = 1.640, 95% confidence interval: 1.127–2.388, p = 0.010) and the isoniazid + rifampicin + pyrazinamide + ethambutol + levofloxacin regimen (odds ratio = 0.210, 95% confidence interval: 0.048–0.932, p = 0.040) as factors that reduced the odds of adverse drug reactions.
Conclusions
A high occurrence rate of adverse drug reactions was observed in children undergoing anti-tuberculosis treatment. Timely recognition and management of adverse drug reactions is essential in this patient population.
Introduction
Tuberculosis (TB) is a chronic infectious diseases caused by mycobacterium tuberculosis (MTB) which can invade multiple organ systems in the human BODY; pulmonary TB is the most common type of TB. Currently, TB is one of the most harmful infectious diseases worldwide. 1 As stated in the global TB report, 2025, there were approximately 10.7 million TB patients worldwide in 2024, including 1.2 million children and young adolescents. Compared to 10.8 million in 2023, 10.7 million in 2022, 10.4 million in 2021, and 10.3 million in 2020, the patient count has shown a downward trend for the first time since 2020. It is estimated that there are currently 69.6 million cases of TB in China, making it the country with the fourth-highest TB burden in the world. However, the number of deaths in TB patients in China has decreased significantly. Compared with 2015, the estimated number of deaths in TB patients has decreased by 29% in 2024. Therefore, prevention and treatment of TB is crucial.
Long-term anti-TB combination regimens can cause various types and levels of adverse drug reactions (ADRs). Many studies have shown a high incidence of ADRs in patients undergoing anti-TB treatment, which could subsequently lead to treatment discontinuation or interruption and treatment time extension. Therefore, ADRs are an important factor contributing to the failure of anti-TB treatment. Our study analyzed the occurrence of ADRs in pediatric patients being administered anti-TB drugs at our hospital and identified the related influencing factors.
Materials and methods
Study design and population
This study was a descriptive study based on a retrospective review of patient medical records. The study analyzed the data of 546 patients diagnosed with TB who underwent treatment at Children's Hospital of Chongqing Medical University between January 2014 and December 2023. The study population included all newly diagnosed drug-susceptible TB patients who were scheduled to start anti-TB treatment.
Sample selection
Inclusion criteria were as follows: (a) confirmed diagnosis of TB and initiation of anti-TB treatment; (b) treatment using first-line anti-TB drugs, including but not limited to isoniazid (INH), rifampicin (RIF), pyrazinamide (PZA), and ethambutol (EMB); and (c) regular follow-up at our hospital throughout the treatment period until completion.
Exclusion criteria were as follows: (a) drug-resistant TB; (b) missing key clinical data, such as information regarding ADRs; and(c) non-drug-related reactions.
Data collection
Relevant data were extracted from medical records using a standardized data collection form. Extracted information included patient demographics (age, sex, weight, bacille Calmette–Guérin (BCG) vaccination history, and underlying diseases), TB diagnosis (pulmonary TB, extrapulmonary TB or systemic TB), treatment regimen and duration, invasive operations during treatment, drug usage (dosage and administration route), occurrence and duration of ADRs, main manifestations or affected organs/systems of adverse reactions, types of drugs suspected to cause adverse reactions, severity of adverse reactions, and use of glucocorticoids.
ADR definition
An ADR was defined as any adverse or unexpected reaction occurring during anti-TB drug administration. The types of ADRs considered included the following: (a) digestive; (b) hepatic; (c) skin; (d) renal; (e) ear; (f) eye; (g) hematological; (h) endocrine; (i) neurological; (j) physical; and (k) metabolism. ADRs were classified into three severity levels based on their impact on treatment: (a) mild (no need to discontinue treatment and/or an antidote was sufficient); (b) moderate (requiring a change in the treatment plan); (c) and severe (requiring temporary withdrawal or permanent discontinuation of anti-TB therapy).
Statistical analyses
Data cleaning was performed using Microsoft Excel, and statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) software (version 27.0). The results were presented as frequencies, means, and SDs. Appropriate statistical tests, such as analysis of variance and chi-square tests, were utilized. Univariate and multivariate logistic regression models were employed to test for the association between ADR onset and different factors. A p-value <0.05 was considered statistically significant.
Results
Clinical characteristics of patients
Among the 546 enrolled patients, 301 (55.13%) were men and 245 (44.87%) were women. Their mean age was 7.45 ± 4.09 years, with more one-fourth (27.47%) being adolescents (aged 11–18 years). Malnutrition (21 cases, 3.85%), genetic diseases (12 cases, 2.20%), and chronic inflammation (11 cases, 2.01%) were the most common comorbidities. In total, 277 patients (50.73%) were diagnosed with TB, 51 (9.34%) had extrapulmonary TB, and 218 (39.93%) had systemic TB. In patients with extrapulmonary TB, the most commonly affected locations were lymph nodes (23 cases, 4.21%), bone/joint (13 cases, 2.38%), and the meninges (11 cases, 2.01%). In terms of disease severity, severe TB accounted for the largest proportion of cases (286 cases, 52.38%).
Severe TB was defined according to the World Health Organization (WHO) guidelines and China's TB prevention and control guidelines as hematogenous pulmonary TB, tracheobronchial TB, tuberculous meningitis, or systemic TB.2,3 Non-severe TB was defined as other types of TB except severe TB.
Anti-TB regimen
In total, 546 patients were mainly treated with INH, RIF, PZA, EMB, streptomycin (SM), linezolid (LZD), levofloxacin (LX), moxifloxacin (MOX), amikacin (AMK), and rifapentine (RFT), with first-line anti-TB drugs being the main drugs. Most patients were administered INH + RIF + PZA + EMB during the intensive phase (410 cases, 75.09%), with a complete treatment duration of 16.40 (13.30, 20.30) months (minimum: 3.20 months and maximum: 48.00 months). The remaining patients were administered other regimens such as INH + RIF + PZA (39 cases, 7.14%) and INH + RIF + PZA + EMB + LX (33 cases, 6.04%), whereas one patient was administered the INH + RIF + PZA + EMB regimen for the entire duration of treatment (12.70 months). With respect to the doses of various anti-TB drugs administered to the 546 patients during treatment, most medications were used within the recommended dosage range (1581 cases, 69.56%), with only a few patients receiving high-dose therapy (100 cases, 4.40%).
According to the WHO guidelines, low dose is defined as using a dose below the lower limit of the recommended daily dose and not exceeding the maximum daily dose. 2 Recommended dose is defined as the dosage used within the recommended daily dose range and not exceeding the maximum daily dose or a dose below the lower limit of the recommended daily dose but reaching the maximum daily dose. High dose is defined as a regimen where doses exceed the upper limit of the recommended daily dose or the maximum daily dose.
Frequency of ADRs
Among the 546 patients, 476 (87.18%) developed at least one ADR, with a total of 915 ADR events recorded. Among the 476 patients with ADRs, 70 (12.82%) experienced no ADRs, 216 (39.56%) developed only one ADR, whereas 260 (47.62%) developed two or more ADRs during the treatment. Only two patients experienced 7 ADRs.
Common clinical manifestations of the ADRs to anti-TB drugs
All adverse effects that were observed during the anti-TB treatment are presented in Table 1. When we classified ADRs according to organ system involvement, cases of metabolic disorders were the most common (430 cases, 46.89%), followed by those of liver function injury (144 cases, 15.74%), blood system damage (121 cases, 13.22%), gastrointestinal symptoms (78 cases, 8.52%), and skin reactions (56 cases, 6.12%). The most frequently documented ADR was hyperuricemia, accounting for approximately 50% of all ADRs (405 cases, 44.26%), followed by elevated liver enzymes without jaundice and elevated bile acids (10.38%) and leukopenia (8.31%).
Frequency of adverse drug reactions to anti-TB drugs by type and severity.
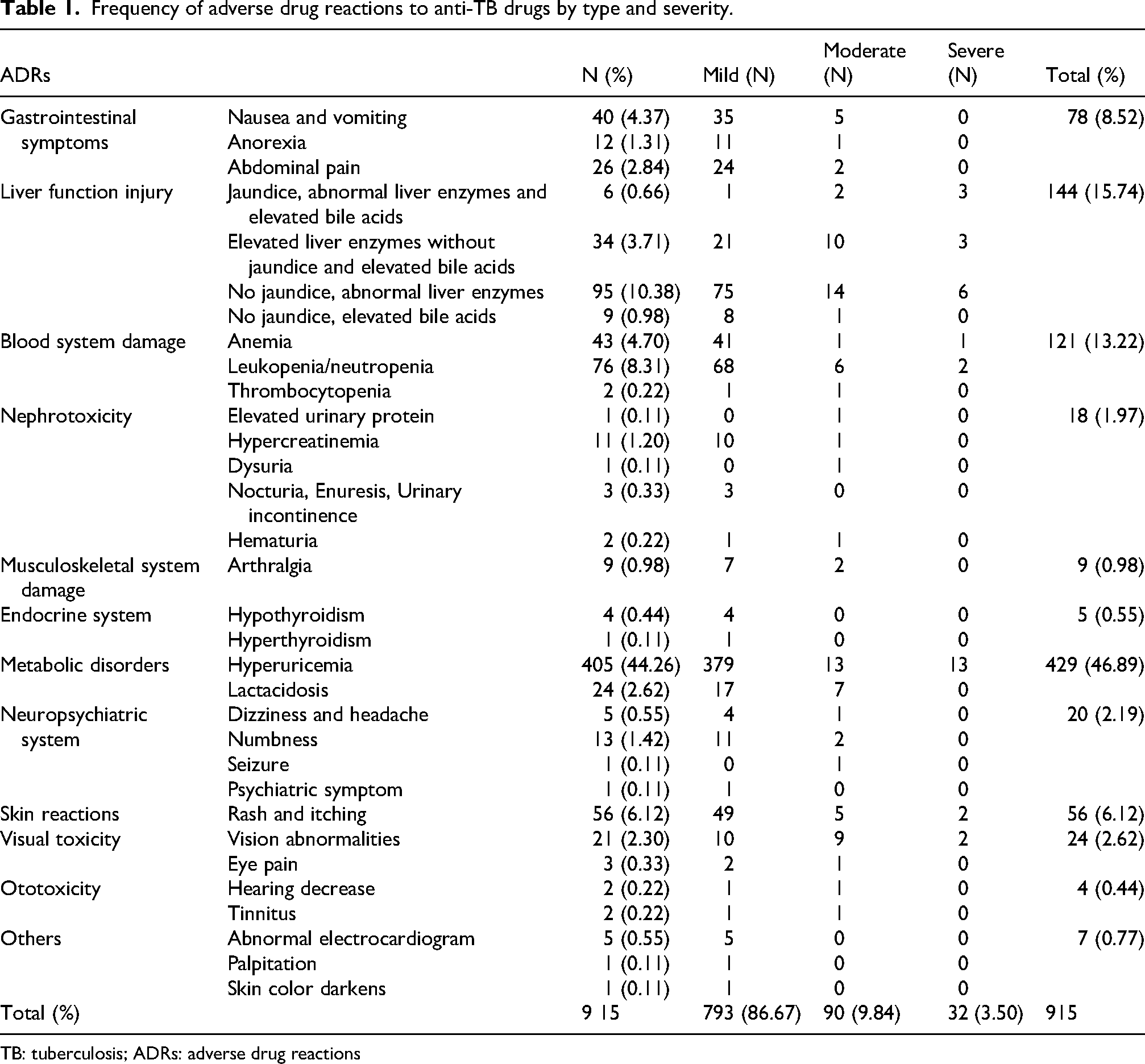
TB: tuberculosis; ADRs: adverse drug reactions
In terms of ADRs management, 90 patients (9.84%) required anti-TB regimen modification (moderate) and 32 (3.50%) required discontinuation (severe). Modification was most common among patients with abnormal liver enzymes accompanied with jaundice (14 cases, 15.56%), and discontinuation was most common in those with hyperuricemia (13 cases, 40.63%).
Occurrence time and duration of ADRs to anti-TB drugs
As presented in Table 2, 471 ADRs (51.48%) occurred within the first month of treatment, particularly within the first week (299 cases, 32.68%). These included liver function injury (46 cases, 31.94%), hyperuricemia (170 cases, 41.98%), and skin reactions (16 cases, 28.57%). In 306 cases (33.44%), ADRs manifested after 6 months of initiating anti-TB medications. Among them, liver function injury (39 cases, 27.08%), hematuria (12 case, 27.91%), leukopenia/neutropenia (22 cases, 28.95%), arthralgia (4 cases, 44.44%), hyperuricemia (200 cases, 49.38%), and vision abnormalities (10 cases, 47.62%) persisted for >6 months. However, ADRs such as nausea and vomiting (24 cases, 60.00%), abdominal pain (13 cases, 50.00%), and skin reactions (42 cases, 75.00%) resolved within 1 month.
Adverse drug reactions to anti-TB drugs according to occurrence time and duration.
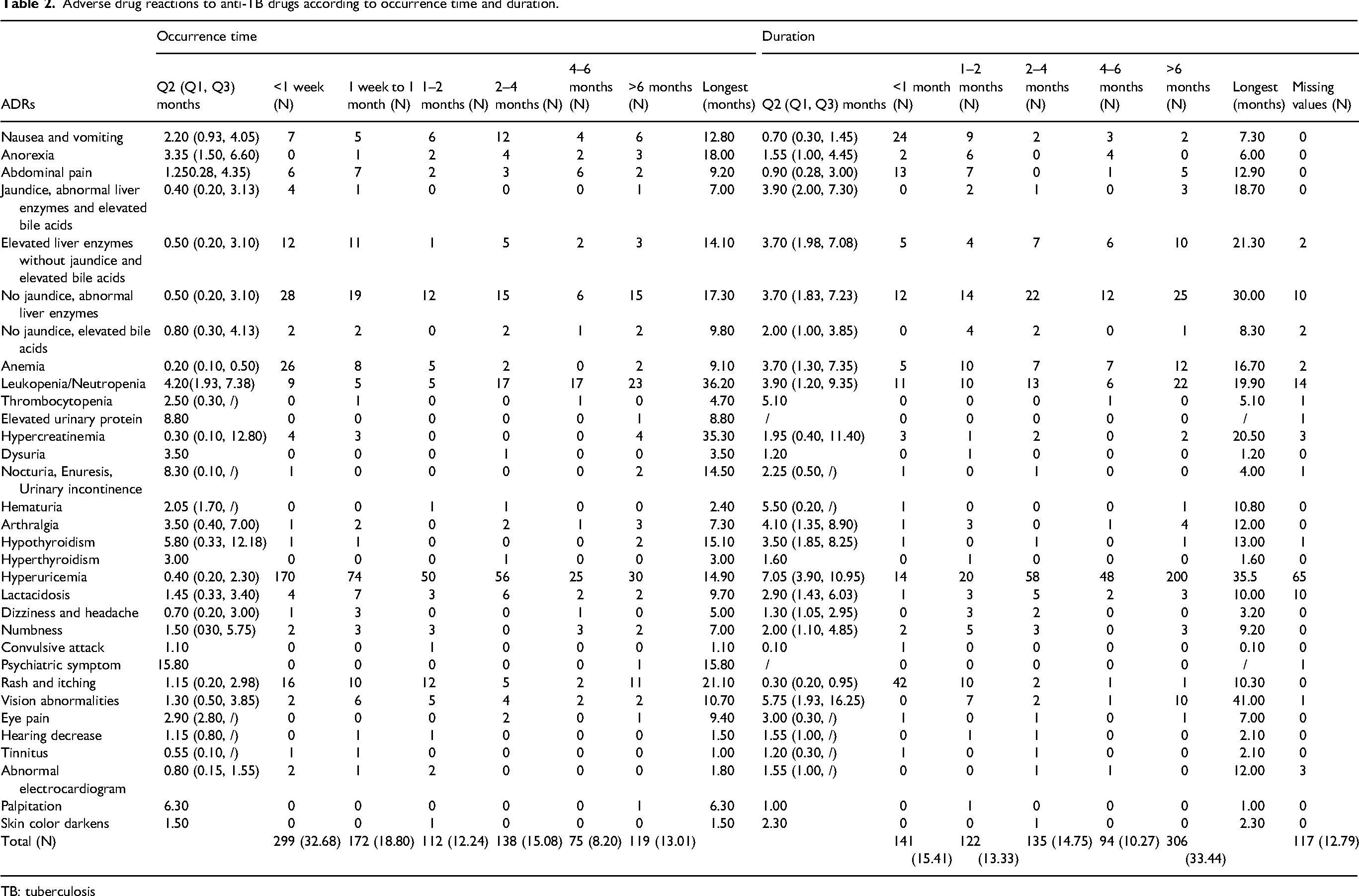
TB: tuberculosis
Suspected anti-TB drugs
The suspected causative drug was unknown in most patients who exhibited ADRs (738 cases, 83.48%). Among those identified via drug withdrawal trials, PZA was the most common (66 cases, 7.47%), followed by LZD (27 cases, 3.05%) and RIF (19 cases, 2.15%). For ARDs such as liver function injury, PZA (32 cases, 22.22%) was the most suspected drug, followed by RIF (8 cases, 5.56%). When the common symptoms were classified by the culprit drug, INH for leukopenia/neutropenia, RIF for liver function injury, leukopenia/neutropenia and skin reactions, PZA for liver function injury and hyperuricemia, EMB for vision abnormalities were common (Table 3).
Frequencies of ADRs to anti-tuberculosis drugs.
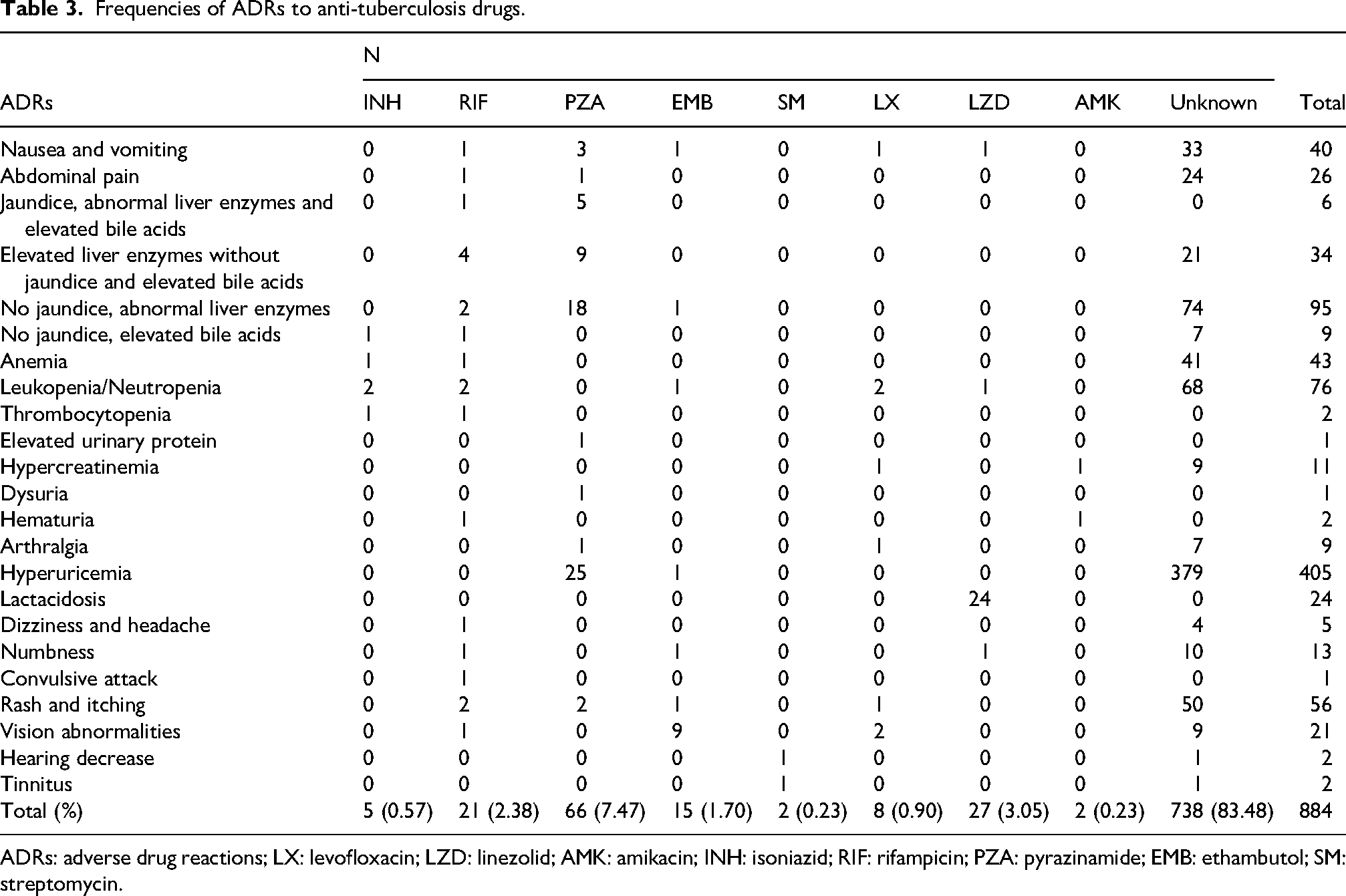
ADRs: adverse drug reactions; LX: levofloxacin; LZD: linezolid; AMK: amikacin; INH: isoniazid; RIF: rifampicin; PZA: pyrazinamide; EMB: ethambutol; SM: streptomycin.
Univariate analysis of factors related to ADRs
Univariate analysis revealed significant differences between the non-ADR and ADR groups in terms of age, TB severity, treatment regimen, RIF dose, and PZA dose (p ≤ 0.05). The frequency of ADRs was significantly higher among children aged 11–18 years than among those aged ≤3 years (90.00% vs. 81.58%, p = 0.050), among those with severe TB than among those with non-severe TB (90.21% vs. 83.85%, p = 0.026), among those who were administered the INH + RIF + PZA + EMB + LZD regimen than among those administered the INH + RIF + PZA regimen (95.24% vs. 69.23%, p = 0.012), among those administered the recommended dose of RIF than among those administered a high dose of RIF (88.58% vs. 66.67%, p = 0.027), and among those administered a high dose of PZA than among those administered a low dose of PZA (100.00% vs. 84.48%, p = 0.046) (Table 4).
Univariate analysis of factors related to ADRs.
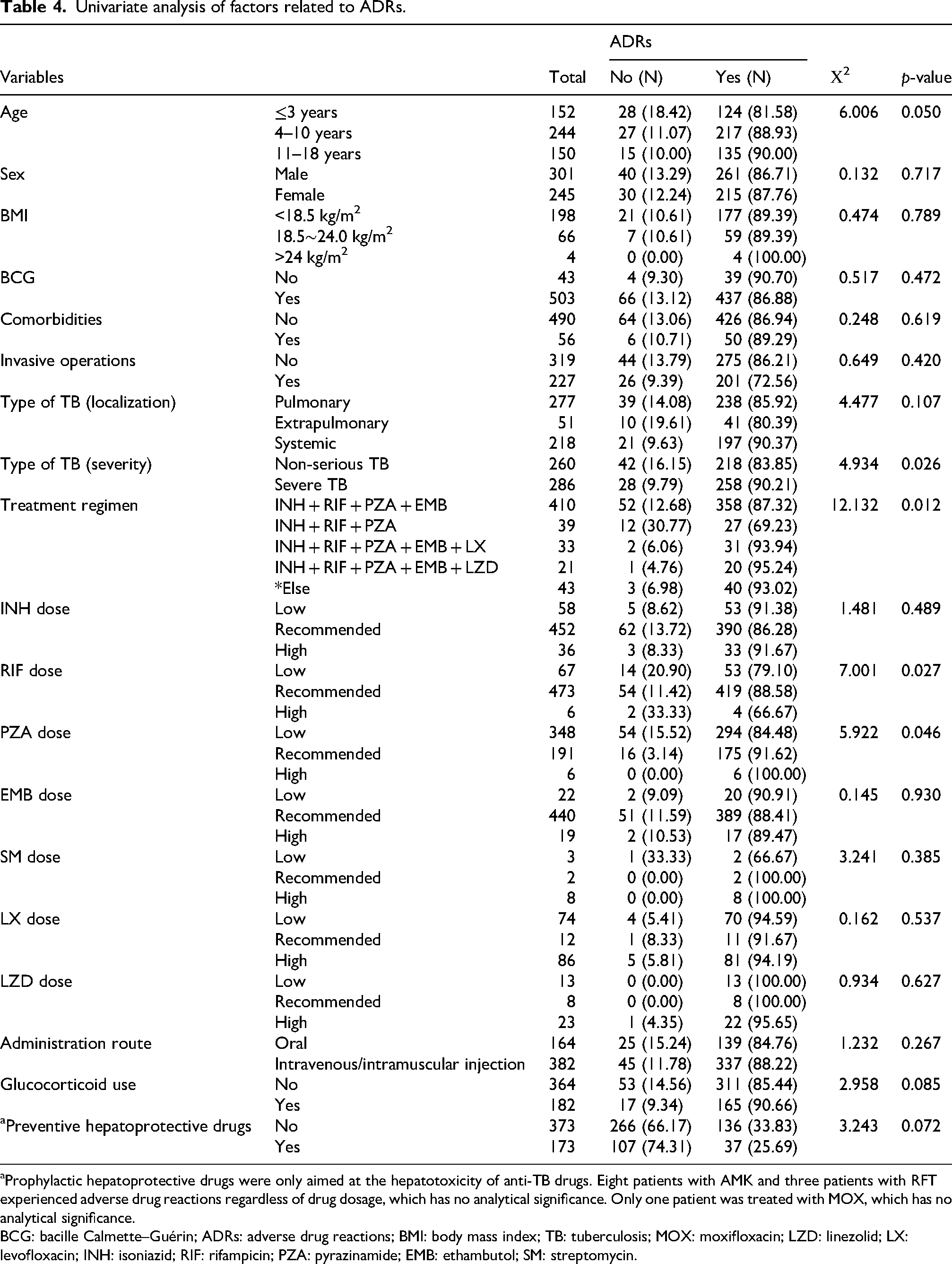
Prophylactic hepatoprotective drugs were only aimed at the hepatotoxicity of anti-TB drugs. Eight patients with AMK and three patients with RFT experienced adverse drug reactions regardless of drug dosage, which has no analytical significance. Only one patient was treated with MOX, which has no analytical significance.
BCG: bacille Calmette–Guérin; ADRs: adverse drug reactions; BMI: body mass index; TB: tuberculosis; MOX: moxifloxacin; LZD: linezolid; LX: levofloxacin; INH: isoniazid; RIF: rifampicin; PZA: pyrazinamide; EMB: ethambutol; SM: streptomycin.
Sex, body mass index (BMI), BCG vaccination status, comorbidities, invasive procedures, type of TB (localization), drug doses (INH, RIF, PZA, EMB, SM, LX, and LZD), route of administration, or hormone use were not significantly associated with the occurrence of ADRs (p > 0.05). In addition, there was no statistically significant difference (p > 0.05) in the use of prophylactic hepatoprotective drugs between patients with and without hepatotoxicity.
Logistic regression analysis of factors related to ADRs
In univariate logistic regression, only age significantly increased the odds of developing ADRs (OR = 1.640, 95% CI: 1.127–2.388, p = 0.010). A multivariable logistic regression model that controlled for all possible confounders revealed that therapeutic regimens were significantly associated with the odds of developing ADRs (p < 0.05). Among these, the INH + RIF + PZA + EMB + LX regimen was significantly associated with lower odds of developing ADRs (OR = 0.210, 95% CI: 0.048–0.932, p = 0.040) (Table 5).
Logistic regression analysis of factors related to ADRs.
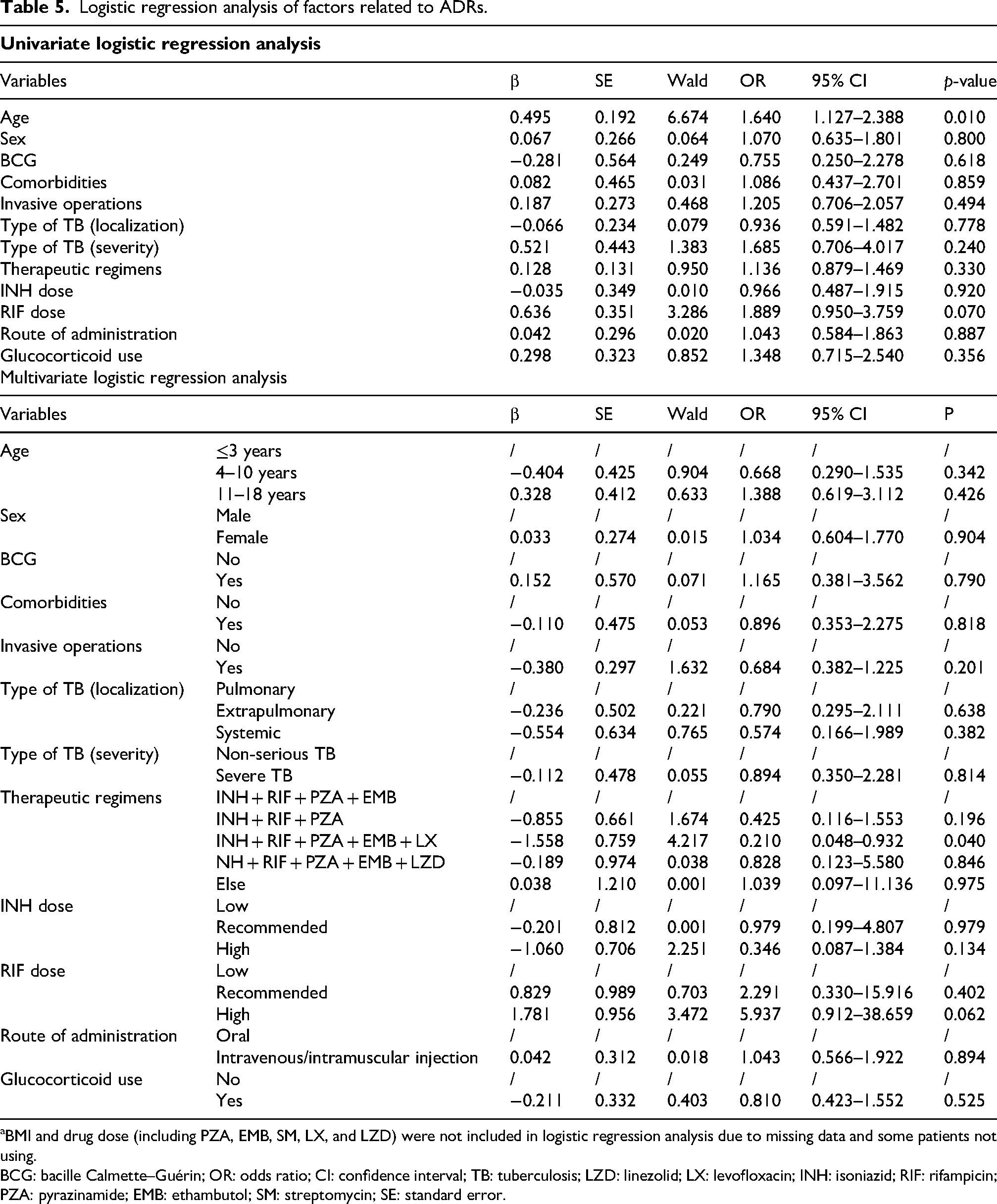
BMI and drug dose (including PZA, EMB, SM, LX, and LZD) were not included in logistic regression analysis due to missing data and some patients not using.
BCG: bacille Calmette–Guérin; OR: odds ratio; CI: confidence interval; TB: tuberculosis; LZD: linezolid; LX: levofloxacin; INH: isoniazid; RIF: rifampicin; PZA: pyrazinamide; EMB: ethambutol; SM: streptomycin; SE: standard error.
Discussion
China is one of the top 20 countries in the world in terms of TB burden. Recently, although the mortality rate among TB patients in China has declined significantly, the number of patients has increased annually. Considering the lengthy duration of anti-TB combination regimens, it is crucial to monitor adverse reaction events occurring during anti-TB treatment. This is the first hospital-based study conducted in western China to report ADRs and assess their prevalence and impact among children with TB receiving first-line anti-TB therapy.
Most of the existing research on ADRs is centered on adults, with limited cohort studies having been conducted on children. The overall prevalence of ADRs induced by anti-TB therapy ranges from 1.00% to 77.00% worldwide among adults4–10 and from 10.91% to 44.70% among children.11–14 Anti-TB drugs-induced ADRs are less common among children than among adults. Among the 546 patients included in this study, 476 (87.18%) experienced at least one ADR, with a total of 916 ADR events detected, a rate that was significantly higher than previously reported. Notably, demographic characteristics and methods of data registry were different in these other study regions. In addition, ethnicities, study designs, and various definitions of ADRs were other factors responsible for these heterogeneities. 8
Hyperuricemia was the most frequently observed ADR, accounting for 50% of all documented ADRs (405 cases, 44.26%). Notably, this ADR was less commonly reported in other pediatric studies; however, it was frequently observed in adult populations. Other studies on adults, which were conducted in different regions of China corroborate our findings but differ in terms of incidence rates. Hyperuricemia was the most frequently observed ADR in Chongqing (430/772 cases, 55.70%); 5 the incidence was slightly higher than that reported in Wuhan (177/634 cases, 29.72%). 8 Hyperuricemia was mostly mild in our study and did not impact treatment changes in most cases (379 cases, 93.58%). Gouty arthralgia was observed in only seven patients. PZA and LX were discontinued due to persistent arthralgia with hyperuricemia in two patients in our study.
Liver function injury (144 cases, 15.74%) was the second most common ADR in our study, with an incidence similar to that reported in another study on adolescents aged 13–18 years with TB in China (1/55 cases, 16.67%). 11 However, it was much higher than those reported by other two similar studies in children conducted in Ukraine (27/302 cases, 8.9%) 12 and Ireland (4/105 cases, 3.8%). 13 Unfortunately, neither of these studies focused on drugs that were discontinued due to liver function injury, and evidence regarding hepatotoxicity-related drugs was primarily derived from studies on adults. Imam et al. 10 from India and domestic scholars 15 have also studied anti-TB drug–induced hepatobiliary adverse events, with RIF being the primary suspected drug. PZA was most the frequently terminated drug for hepatotoxicity in our study, which is in line with reports from four adult series.16–19 Some patients were administered chemo preventive agents for TB-drug-induced liver injury (DILI) in this study. However, there was no statistically significant difference in the preventive use of hepatoprotective drugs between patients with and without hepatotoxicity, indicating that the prophylactic utilization of hepatoprotective agents was not associated with a reduction in TB-DILI risk. Our findings regarding prophylactic hepatoprotective drugs are consistent with those reported by Chen et al.; 20 however, other studies in China have reported that their preventive use significantly reduces the incidence of liver injury.21,22
In fact, some studies have shown that gastrointestinal symptoms were the most common ADR detected in their setting.9,12,13,23 Nausea and vomiting caused by anti-TB drugs are usually dose-dependent, and symptoms can be alleviated by reducing the dosage of the suspected drug. Other rare ADRs detected in our study such as thyroid dysfunction, psychiatric symptom, and abnormal electrocardiogram have been discussed in previous studies and case reports;24–27 however, most of these occurred in drug-resistant TB patients.
In the present study, most ADRs occurred during the intensive treatment phase, especially within 1 week (299 cases, 32.68%%). This finding is in agreement with the results reported by Yanrong et al. 23 (within 4–10 days, 100/156 cases, 64.1%) and Na et al. 7 (within 7 days, 216/376 cases, 57%). In addition, liver function injury, hyperuricemia, hyperuricemia, and skin reactions were most likely to occur within 1 week.
In our study, univariate analysis showed that the frequency of ADRs was significantly higher among children aged 11–18 years, those with severe TB, those administered the INH + RIF + PZA + EMB + LZD regimen, those administered the recommended dose of RIF, and those administered a high dose of PZA. The multivariate logistic regression model showed that therapeutic regimens influenced the occurrence of ADRs significant; the INH + RIF + PZA + EMB + LX regimen significantly decreased the odds of developing ADRs. Our results with respect to age and treatment regimens are in line with those reported by other studies on adult patients, which conclude that age and treatment regimens are risk factors for ADRs.8,23,28 Only three studies conducted for estimating the risk factors of occurrence of ADRs in children have concluded that newborns 29 and children aged 6–10 years, 13 and 11–18 years 30 are at high risk of ADRs. Two studies on adults in China conducted by Yanrong et al. 23 and Shi et al. 28 considered standard quadruple therapy (INH + RIF + PZA + EMB) as an independent risk factor of ADRs. However, in our study, the INH + RIF + PZA + EMB + LX treatment regimen was associated with a reduced risk of ADR; this result should be interpreted with caution. LX, as a fluoroquinolone drug, can cause ADRs in multiple systems such as the gastrointestinal tract, nervous system, skin, and joints. Its “protective effect” does not conform to biological rationality. The most likely reasons are clinical medication indication bias and the small sample size of subgroups. Therefore, in the future, it is necessary to control confounding factors through propensity score matching or employment of a prospective design to clarify the risk spectrum of ADRs for different regimens.
With respect to the impact of drug dosage on the outcome of ADRs, this study concludes that the use of the recommended dose of RIF and a high dose of PZA significantly increased the incidence of ADRs. Several studies have been conducted both domestically and internationally on the safety and effectiveness of using high-dose anti-TB drugs for the treatment of TB patients. Research studies and clinical trial results have clearly demonstrated that the high-dose INH, RIF, and PZA treatment regimens significantly improve the sterilizing activities compared with the standard doses, without increasing the risk of ADRs.31–33 Interestingly, high-dose INH is one of the higher dose anti-TB drugs recommended during the induction phase, especially for INH-resistant TB. The WHO recommends a high-dose of INH (15–20 mg/kg). 34 Currently, the new dispersible tablet formulations of MOX and clofazimine have gained substantial pharmacokinetic and acceptability evidence.35,36 However, the unpleasant taste of the drugs remains a major obstacle in improving compliance, and the development of rifampin dispersible tablets remains the most urgent priority.37,38
In addition, although our study showed no significant association of sex with the occurrence of ADRs, some similar studies on children12,13 and adults5,6,8 have confirmed that female sex is an independent risk factor for ADRs, possibly owing to the increased androgen activity or induction of liver microsomal enzyme activity among men, which allows them to metabolize drugs more effectively. 39 A study on children from Ireland has also confirmed that the risk of developing ADRs is higher in patients who have been re-treated and have not received BCG vaccination. 13 Conclusion on the high risk in re-treated patients has also been supported by studies on adults in China. 4 However, our study only focused on newly diagnosed patients, and there was no significant correlation between BCG vaccination status and ADRs.
Our study has certain limitations. First, as a single-center retrospective analysis, we are unable to summarize the clinical characteristics of TB and the incidence of ARDs and its influencing factors across the entire region. Second, the duration of the intensive phase treatment in our study was 4–6 months, whereas the WHO recommends a duration of 2 months for non-severe TB and 6 months for tuberculous meningitis in children. Hence, we could not delve into the impact of different treatment durations on the outcome of ARDs. Third, due to the retrospective design of this study, key treatment details could not be fully ascertained. Some regimens do not conform to the WHO guidelines, and dosages are often unspecified. Moreover, the lack of syrup formulations for TB drugs raises uncertainty about how drugs were actually administered (crushing or splitting tablets). These factors may have led to the occurrence of ADRs and limit the reliability of our conclusions. The strength of the study is that we included outpatient patients and conducted follow-ups for all patients, obtaining information about various ADRs throughout their treatment courses via telephone consultations until treatment completion.
Conclusion
This study suggests a high rate of ADRs in patients undergoing anti-TB treatment, particularly pediatric patients with TB. Therefore, monitoring for possible ADRs, especially during the intensive treatment phase, should be routinely performed. The frequency of hyperuricemia monitoring and hepatic function test should be increased during anti-TB therapy. Patients with risk factors associated with ADRs, such as age 11–18 years, severe TB, and administration of INH + RIF + PZA + EMB + LZD regimen, should be closely monitored during the treatment. Finally, such surveillance for ADRs should be expanded throughout the country so that more representative data can be obtained, thereby improving treatment adherence and maximizing the TB cure rate.
Footnotes
Acknowledgments
The authors would like to express their gratitude to all the staff members of the Department of Infectious Diseases, Children’s Hospital of Chongqing Medical University.
Ethics approval
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2024) and was approved by the Ethics Committee of the Children's Hospital of Chongqing Medical University (protocol No. Ethics Review [Clinical Research] No. 14 of 2025). All data extracted from medical records were kept confidential. As this was a retrospective study with no interventions, the requirement for informed consent was waived.
Consent for publication
Not applicable.
Authors’ contributions
Xinxue Wang conceptualized the research question and conducted the analysis. Hongmei Xu provided valuable feedback and comments on successive manuscript drafts and revised these manuscript drafts.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicts of interest
The authors declare that they have no competing interests.
Clinical trial number
Not applicable.
Availability of data and materials
The data used and/or analyzed during the current study are available from the corresponding author on reasonable request.