
Abstract
Objective
To compare outcomes between immediate intraoperative dexamethasone implantation and scheduled 1-month postoperative dexamethasone implantation in pseudophakic eyes undergoing vitrectomy for diabetic macular edema with secondary epiretinal membrane.
Methods
This retrospective comparative study included 80 pseudophakic eyes with diabetic macular edema and secondary epiretinal membrane. All eyes underwent 25-gauge vitrectomy with epiretinal membrane and internal limiting membrane peeling. The Immediate Group
Results
Both groups showed improvement in best-corrected visual acuity and reduction in central macular thickness, but early recovery was faster in the Immediate Group. At 1 month, best-corrected visual acuity was 0.55 ± 0.08 versus 0.78 ± 0.11 logarithm of the minimum angle of resolution, and central macular thickness was 315.5 ± 28.6 versus 520.2 ± 35.4 μm, respectively (both P < 0.001). Mixed-effects models showed significant time effects and significant group × time interactions at earlier visits, supporting greater early improvement in the Immediate Group. At 12 months, best-corrected visual acuity remained better in the Immediate Group (0.36 ± 0.08 vs. 0.43 ± 0.10 logarithm of the minimum angle of resolution, P = 0.001). Although central macular thickness remained lower in the Immediate Group, the group × time interaction for central macular thickness was no longer significant, indicating that the anatomical advantage became less pronounced over time. The Immediate Group showed numerically fewer dexamethasone injections, but without statistical significance. Intraocular pressure elevation was controlled medically, and no serious ocular or systemic adverse events were documented.
Conclusion
Immediate intraoperative dexamethasone implantation was associated with faster early anatomical recovery and earlier visual improvement. The anatomical advantage became less pronounced over time, and the potential effect on retreatment burden requires confirmation in prospective randomized studies.
Keywords
Introduction
Diabetic macular edema (DME) remains a leading cause of vision loss in patients with diabetic retinopathy (DR) and is driven by a complex interaction between vascular endothelial growth factor (VEGF) upregulation and chronic inflammation. 1 In a subset of patients, DME is complicated by secondary epiretinal membrane (ERM). ERM can exert tangential and anteroposterior traction on the macula, aggravate vascular leakage, and provide a scaffold for cellular proliferation and local inflammatory activity, thereby making macular edema less responsive to conventional intravitreal anti-VEGF or corticosteroid monotherapy. 2 For DME with a tractional component caused by ERM, pars plana vitrectomy (PPV) combined with membrane peeling is commonly considered when visual symptoms and persistent macular edema are present. Although surgery can relieve the mechanical component, vitrectomy and membrane peeling may also induce transient postoperative inflammation and further disturb the blood–retinal barrier. As a result, some patients may experience persistent or aggravated macular edema during the early postoperative period, which may limit functional recovery. 3 The dexamethasone (DEX) intravitreal implant (Ozurdex®) has been used as an adjunctive treatment in this setting. As a biodegradable sustained-release device, it provides anti-inflammatory effects by stabilizing the blood–retinal barrier and suppressing multiple inflammatory mediators for up to 3–4 months. 4 However, the optimal timing of DEX implantation during the perioperative management of DME with secondary ERM remains unclear. Some surgeons advocate immediate intraoperative implantation to suppress early postoperative inflammation and promote rapid anatomical recovery. In contrast, a scheduled delayed postoperative strategy allows initial assessment after mechanical traction has been relieved and postpones corticosteroid exposure until the early postoperative visit. In the present study, the Delayed Group received the first DEX implant uniformly at 1 month after surgery, rather than following a purely observational or untreated control design. Furthermore, previous studies may have been influenced by lens status, differences in surgical procedures, or ERM recurrence. Therefore, in this retrospective comparative study, we evaluated the 12-month outcomes of immediate intraoperative versus scheduled 1-month postoperative DEX implantation in a standardized cohort of pseudophakic eyes, all of which underwent the same PPV procedure combined with ERM and internal limiting membrane (ILM) peeling. By comparing these two timing strategies, we aimed to assess whether immediate intraoperative DEX implantation was associated with faster anatomical recovery, earlier visual improvement, and a potential difference in retreatment burden.
Methods
Study design and ethical approval
This retrospective, comparative, single-center study was conducted at the Department of Ophthalmology, People’s Hospital of Leshan. The study protocol adhered to the tenets of the Declaration of Helsinki (1975, revised 2024). The study was approved by the Institutional Ethics Committee of People’s Hospital of Leshan (Approval No. LYLL[2024]KY-006, approved on 25 January 2024). Written informed consent for surgical procedures and the use of anonymized clinical data was obtained from all patients prior to surgery. All patient data were fully de-identified prior to analysis to ensure confidentiality. This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 5
Participants
This retrospective comparative study included 80 eyes from 80 consecutive patients with DME and concurrent secondary ERM who were treated between 2020 and 2024. Patient selection was based on predefined eligibility criteria during the study period, without randomization. All patients were pseudophakic before surgery to eliminate the confounding effect of cataract progression on visual outcomes. Stable systemic control was required for inclusion, defined as glycated hemoglobin (HbA1c) < 7.5% maintained for at least 3 months prior to the index surgery. Patients were divided into two groups according to the timing of intravitreal DEX implantation. In the Immediate Group (n = 40), the implant was placed intraoperatively during vitrectomy. In the Delayed Group (n = 40), the implant was administered uniformly at 1 month after surgery. Baseline demographic and clinical characteristics are summarized in Table 1. There were no significant differences between the two groups in age, sex, duration of diabetes, or duration of DR (all P > 0.05). Baseline ocular parameters, including best-corrected visual acuity (BCVA), central macular thickness (CMT), and intraocular pressure (IOP), were comparable between groups.
Baseline characteristics of the Immediate and Delayed Groups.

Data are presented as mean ± standard deviation or number (%). Between-group comparisons were performed using the independent-samples t-test or chi-squared test, as appropriate.
BCVA: best-corrected visual acuity; CMT: central macular thickness; DR: diabetic retinopathy; HbA1c: glycated hemoglobin; IOP: intraocular pressure; N/A: not applicable.
Inclusion criteria
Patients were eligible for inclusion if they met all of the following criteria: (a) a confirmed diagnosis of DME with concurrent secondary ERM in pseudophakic eyes, established by multimodal ophthalmic examination including slit-lamp biomicroscopy, spectral-domain optical coherence tomography (SD-OCT; Cirrus HD-OCT 5000, Carl Zeiss Meditec, Germany), and fluorescein fundus angiography (FFA; SPECTRALIS HRA, Heidelberg Engineering, Germany); (b) presence of visual symptoms such as decreased visual acuity or metamorphopsia, with a baseline BCVA ≥ 0.52 logarithm of the minimum angle of resolution (LogMAR) and CMT > 300 μm; (c) completion of panretinal photocoagulation (PRP) at least 3 months before enrollment when clinically indicated, to ensure stabilization of DR; (d) no history of intravitreal corticosteroid therapy in the study eye, including DEX implant or triamcinolone acetonide, and a washout period of at least 3 months after the last intravitreal anti-VEGF injection; (e) and stable systemic control, defined as HbA1c < 7.5% and blood pressure controlled below 140/90 mmHg for at least 3 months prior to surgery.
Exclusion criteria
Eyes were excluded if any of the following conditions were present: (a) coexisting macular diseases other than DME, including age-related macular degeneration, myopic traction maculopathy, or retinal vein occlusion; (b) active intraocular inflammation or vitreomacular traction (VMT); (c) pre-existing glaucoma or ocular hypertension with baseline IOP > 21 mmHg requiring more than one topical IOP-lowering medication; (d) any history of intraocular surgery other than uncomplicated phacoemulsification with intraocular lens implantation performed at least 6 months before enrollment, or previous PPV; (e) significant media opacity, including corneal scarring or vitreous hemorrhage that interfered with acquisition of high-quality OCT images or FFA images; (f) monocular status; or (g) inability to complete the 12-month follow-up period.
Clinical assessments and follow-up
All patients underwent comprehensive ophthalmic examinations at baseline and at 1, 3, 6, 9, and 12 months after surgery. To ensure consistency, all examinations were performed using the same instruments by experienced technicians who were masked to treatment allocation. BCVA was measured using a standard Snellen chart at a distance of 5 m and converted to LogMAR for statistical analysis. IOP was measured using Goldmann applanation tonometry. Slit-lamp biomicroscopy and dilated fundus examinations were performed at each follow-up visit to evaluate postoperative status and monitor for potential complications. Morphological assessment was performed using SD-OCT (Cirrus HD-OCT 5000, Carl Zeiss Meditec, Germany). CMT was defined as the average retinal thickness within the central 1-mm diameter area centered on the fovea and was automatically calculated using the Macular Cube 512 × 128 scan protocol. Ultra-widefield fundus photography (Optomap, Optos PLC) was performed at each follow-up visit to document retinal status, including progression of DR and peripheral retinal changes. The need for additional DEX implantation was evaluated according to the predefined retreatment criteria described in the Treatment Protocol section. From month 3 onward, retreatment was administered on a pro re nata (PRN) basis in both groups, with a minimum interval of 3 months between consecutive injections, in accordance with approved dosing recommendations. Postoperative complications and adverse events were recorded throughout the follow-up period, including ERM recurrence, IOP elevation, endophthalmitis, vitreous hemorrhage, and other surgery- or injection-related complications. Systemic adverse events were also recorded if documented in the medical records. All 80 included eyes from 80 patients completed the scheduled 12-month follow-up. Complete BCVA, CMT, and IOP data were available at baseline and at 1, 3, 6, 9, and 12 months after surgery. No eyes were lost to follow-up, and no missing observations occurred at the prespecified intermediate visits.
Surgical procedure
Vitrectomy and membrane peeling
All surgeries were performed by the same experienced vitreoretinal surgeon. Procedures were conducted under topical and retrobulbar anesthesia using a 25-gauge transconjunctival sutureless vitrectomy system (Constellation Vision System; Alcon Laboratories, Fort Worth, TX, USA). After core vitrectomy, triamcinolone acetonide (TA) was used to visualize the vitreous and assist in the induction of posterior vitreous detachment. Residual TA was subsequently removed from the vitreous cavity. The macular area was visualized using a wide-angle viewing system. Indocyanine green (ICG; 0.25 mg/0.1 mL) was applied for approximately 30 s to stain the membranes and was then completely irrigated. The ERM was peeled using intraocular forceps, followed by ILM peeling in a circular area approximately 2–3 disc diameters centered on the fovea.
At the end of surgery, the peripheral retina was carefully examined to exclude retinal tears or other abnormalities, and the vitreous cavity was filled with balanced salt solution.
DEX implantation strategy
A 0.7-mg DEX intravitreal implant (Ozurdex; Allergan, Irvine, CA, USA) was administered according to group allocation. In the Immediate Group, the implant was administered at the end of vitrectomy. The injection site was located 4.0 mm posterior to the limbus in the inferior quadrant. The needle was inserted obliquely through the sclera and advanced into the vitreous cavity for implantation.
In the Delayed Group, no DEX implant was administered during the initial surgery. All patients in this group received their first DEX implant uniformly at the 1-month postoperative visit. The injection procedure was identical to that used in the Immediate Group.
DEX implantation schedule and retreatment protocol
During the 12-month follow-up period, DEX implantation was performed according to the predefined treatment schedule and retreatment criteria. In the Immediate Group, the first DEX implant was administered intraoperatively at the end of vitrectomy. In the Delayed Group, the first DEX implant was administered uniformly at the 1-month postoperative visit. From month 3 onward, additional DEX implants were administered in both groups on a PRN basis according to the same predefined retreatment criteria. Retreatment was considered when any of the following criteria were met: (a) a decline in BCVA compared with the previous visit; (b) an increase in CMT of more than 50 μm; or (c) the presence of persistent or recurrent intraretinal or subretinal fluid on OCT. All retreatments were performed using the same 0.7-mg DEX implant under sterile conditions. A minimum interval of 3 months was maintained between consecutive injections in the same eye, in accordance with the manufacturer's recommendations.
Statistical analysis
Statistical analyses were performed using Statistical Package for the Social Sciences software (version 26.0; IBM Corp., Armonk, NY, USA). Continuous variables are presented as mean ± standard deviation (SD), and categorical variables are presented as frequencies and percentages. The normality of continuous variables was assessed using the Shapiro–Wilk test. A two-sided P-value < 0.05 was considered statistically significant. Baseline demographic and clinical characteristics between the Immediate Group and the Delayed Group were compared using the independent-samples t-test for continuous variables and the chi-squared test or Fisher's exact test for categorical variables, as appropriate. Longitudinal changes in BCVA and CMT were analyzed using linear mixed-effects models. Time was treated as a categorical variable, with baseline used as the reference time point. The models included treatment group, time, and the group × time interaction as fixed effects and a random intercept for each patient to account for repeated measurements within the same eye. The Delayed Group at baseline served as the reference category. Bonferroni-adjusted post hoc comparisons were performed where appropriate. The number of DEX injections per eye was compared between groups using the Mann–Whitney U test. Retreatment rates and categorical safety outcomes, including the incidence of IOP elevation, were compared using the chi-squared test or Fisher's exact test, as appropriate. Postoperative complications with no events in either group were summarized descriptively.
Results
BCVA
Longitudinal changes in BCVA (LogMAR) are summarized in Table 2, and the results of the linear mixed-effects model analysis are presented in Table 3. At baseline, the mean BCVA was 0.88 ± 0.10 LogMAR in the Immediate Group and 0.86 ± 0.12 LogMAR in the Delayed Group, with no significant difference between groups (P = 0.420; Table 2). During follow-up, both groups demonstrated overall improvement in BCVA, although a mild fluctuation was observed around 6 months. At 1 month postoperatively, mean BCVA improved to 0.55 ± 0.08 LogMAR in the Immediate Group and 0.78 ± 0.11 LogMAR in the Delayed Group. At 3 months, mean BCVA further improved to 0.42 ± 0.07 LogMAR and 0.58 ± 0.10 LogMAR, respectively. The Immediate Group demonstrated significantly better BCVA than the Delayed Group at both time points (both P < 0.001; Table 2). At 6 months, the mean BCVA was 0.47 ± 0.07 LogMAR in the Immediate Group and 0.65 ± 0.10 LogMAR in the Delayed Group (P < 0.001). At 9 months, mean BCVA improved to 0.43 ± 0.07 LogMAR and 0.60 ± 0.10 LogMAR, respectively (P < 0.001). At the final 12-month follow-up visit, the mean BCVA further improved to 0.36 ± 0.08 LogMAR in the Immediate Group and 0.43 ± 0.10 LogMAR in the Delayed Group (P = 0.001; Table 2).
Comparative analysis of BCVA (LogMAR) over 12 months.
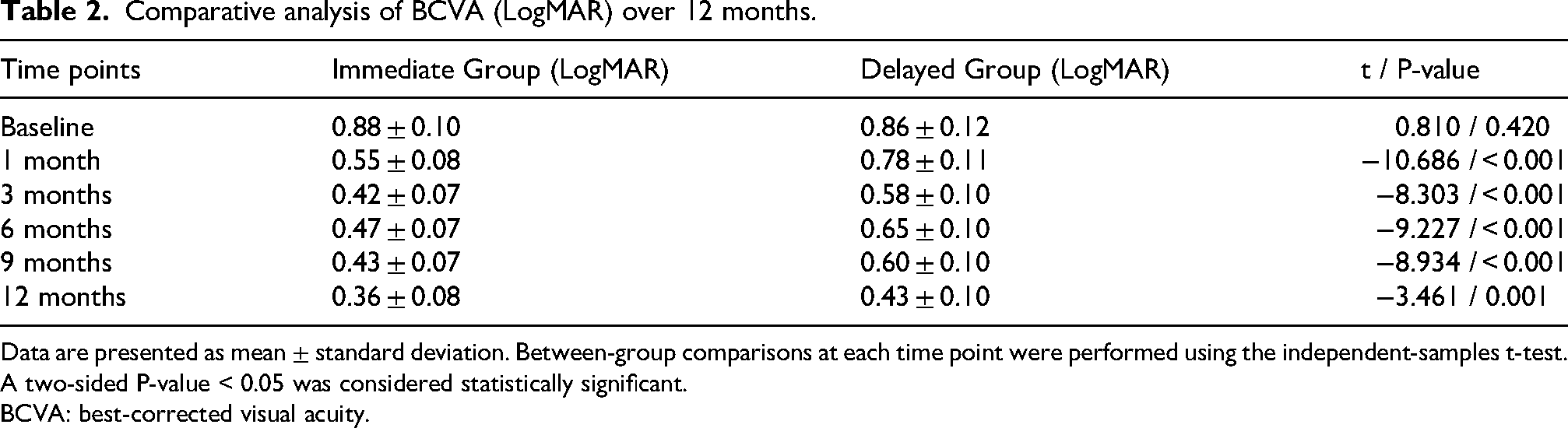
Data are presented as mean ± standard deviation. Between-group comparisons at each time point were performed using the independent-samples t-test. A two-sided P-value < 0.05 was considered statistically significant.
BCVA: best-corrected visual acuity.
Linear mixed-effects model analysis of longitudinal changes in BCVA (LogMAR) over 12 months.

Linear mixed-effects model analysis of longitudinal changes in BCVA during the 12-month follow-up period. Treatment group, follow-up time, and group × time interaction were included as fixed effects, whereas random intercepts for each patient were included to account for repeated measurements within eyes. Negative β coefficients indicate improvement in BCVA (LogMAR).
CI: confidence interval; BCVA: best-corrected visual acuity.
Linear mixed-effects model analysis demonstrated a significant longitudinal effect of time on BCVA improvement throughout follow-up (all P < 0.001 versus baseline; Table 3). No significant baseline group effect was identified (β = 0.018, P = 0.472). Significant group × time interactions were observed at 1 month (β = −0.248, P < 0.001), 3 months (β = −0.178, P < 0.001), 6 months (β = −0.198, P < 0.001), 9 months (β = −0.188, P < 0.001), and 12 months (β = −0.088, P < 0.001), indicating greater BCVA improvement over time in the Immediate Group (Table 3).
CMT
Longitudinal changes in CMT are summarized in Table 4, and the results of the linear mixed-effects model analysis are presented in Table 5.
Comparative analysis of CMT over 12 months.
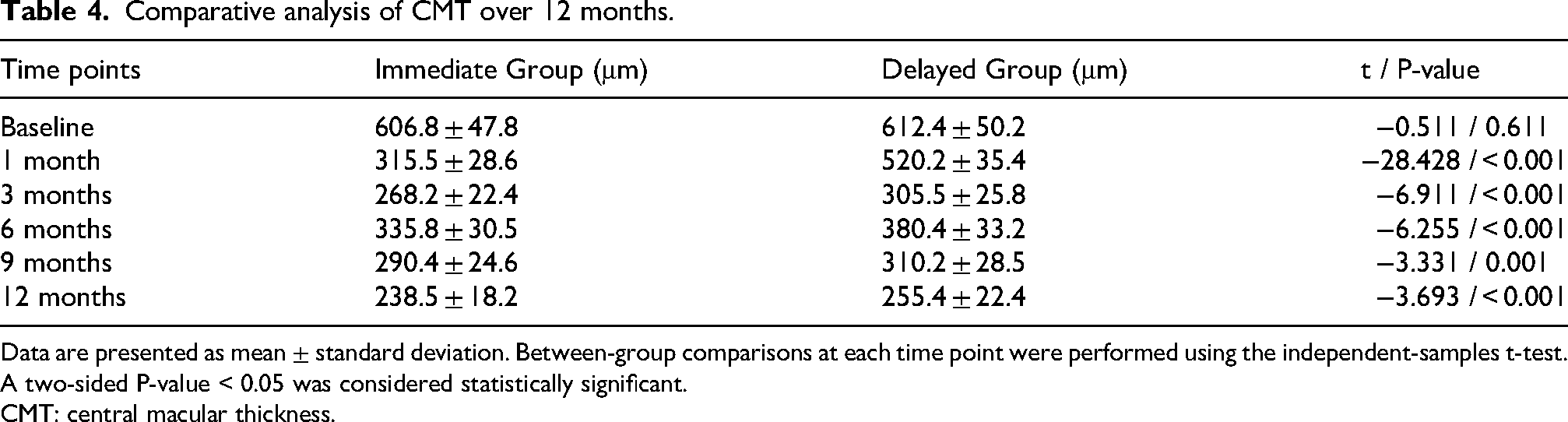
Data are presented as mean ± standard deviation. Between-group comparisons at each time point were performed using the independent-samples t-test. A two-sided P-value < 0.05 was considered statistically significant.
CMT: central macular thickness.
Linear mixed-effects model analysis of longitudinal changes in CMT over 12 months.
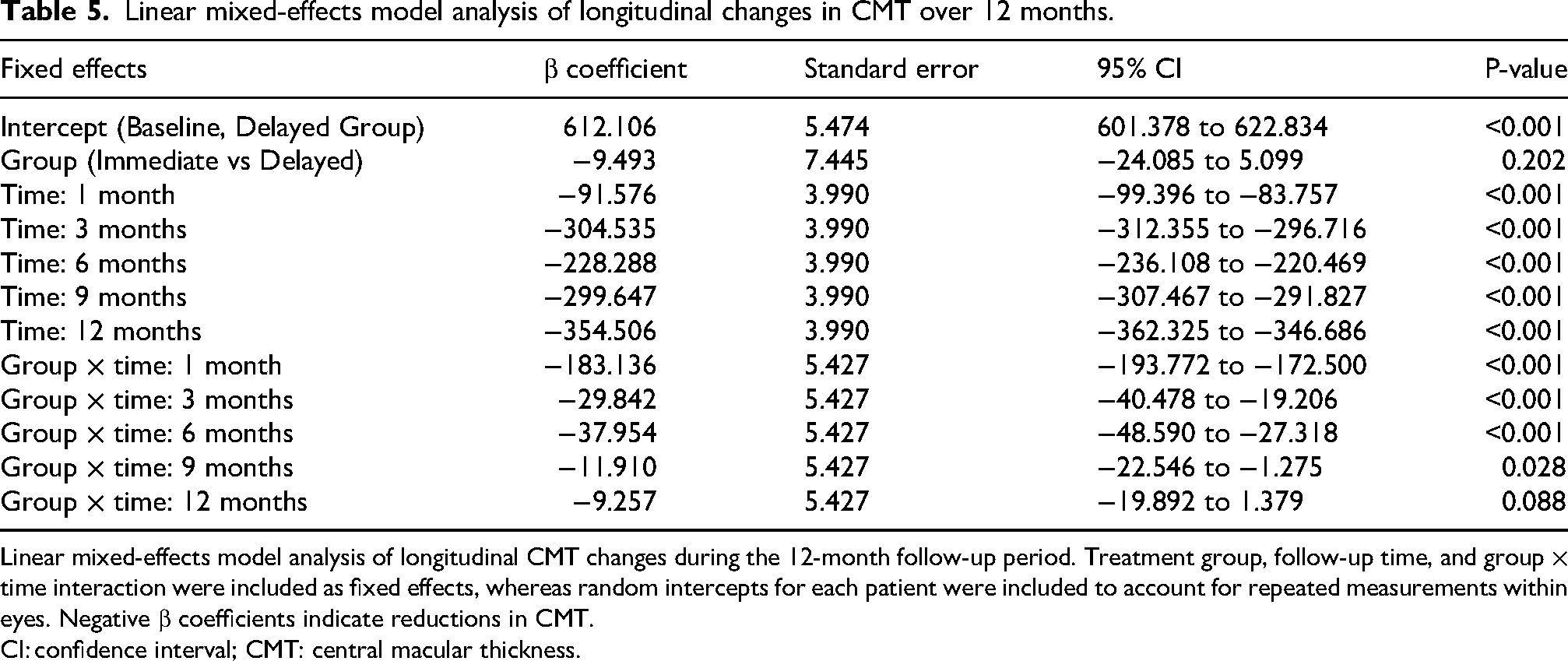
Linear mixed-effects model analysis of longitudinal CMT changes during the 12-month follow-up period. Treatment group, follow-up time, and group × time interaction were included as fixed effects, whereas random intercepts for each patient were included to account for repeated measurements within eyes. Negative β coefficients indicate reductions in CMT.
CI: confidence interval; CMT: central macular thickness.
At baseline, the mean CMT was 606.8 ± 47.8 μm in the Immediate Group and 612.4 ± 50.2 μm in the Delayed Group, with no significant difference between groups (P = 0.611; Table 4). During follow-up, both groups demonstrated overall reductions in CMT, although a transient increase was observed at 6 months compared with 3 months. At 1 month postoperatively, mean CMT decreased to 315.5 ± 28.6 μm in the Immediate Group and 520.2 ± 35.4 μm in the Delayed Group. At 3 months, mean CMT further decreased to 268.2 ± 22.4 μm and 305.5 ± 25.8 μm, respectively. The Immediate Group demonstrated significantly lower CMT values than the Delayed Group at both time points (both P < 0.001; Table 4). At 6 months, the mean CMT was 335.8 ± 30.5 μm in the Immediate Group and 380.4 ± 33.2 μm in the Delayed Group (P < 0.001). At 9 months, mean CMT decreased to 290.4 ± 24.6 μm and 310.2 ± 28.5 μm, respectively (P = 0.001). At the final 12-month follow-up visit, the mean CMT further decreased to 238.5 ± 18.2 μm in the Immediate Group and 255.4 ± 22.4 μm in the Delayed Group (P < 0.001; Table 4).
Linear mixed-effects model analysis demonstrated a significant longitudinal effect of time on CMT reduction throughout follow-up (all P < 0.001 versus baseline; Table 5). No significant baseline group effect was identified (β = −9.493, P = 0.202). Significant group × time interactions were observed at 1 month (β = −183.136, P < 0.001), 3 months (β = −29.842, P < 0.001), 6 months (β = −37.954, P < 0.001), and 9 months (β = −11.910, P = 0.028), indicating greater CMT reduction over time in the Immediate Group. However, the group × time interaction at 12 months was not statistically significant (β = −9.257, P = 0.088; Table 5). These findings indicate that the anatomical advantage associated with immediate implantation was most evident during the early postoperative period and became less pronounced by 12 months.
The longitudinal trends of BCVA and CMT in both groups are shown in Figure 1. The Immediate Group showed faster early improvement in BCVA and a more rapid reduction in CMT, particularly during the first 3 months after surgery.
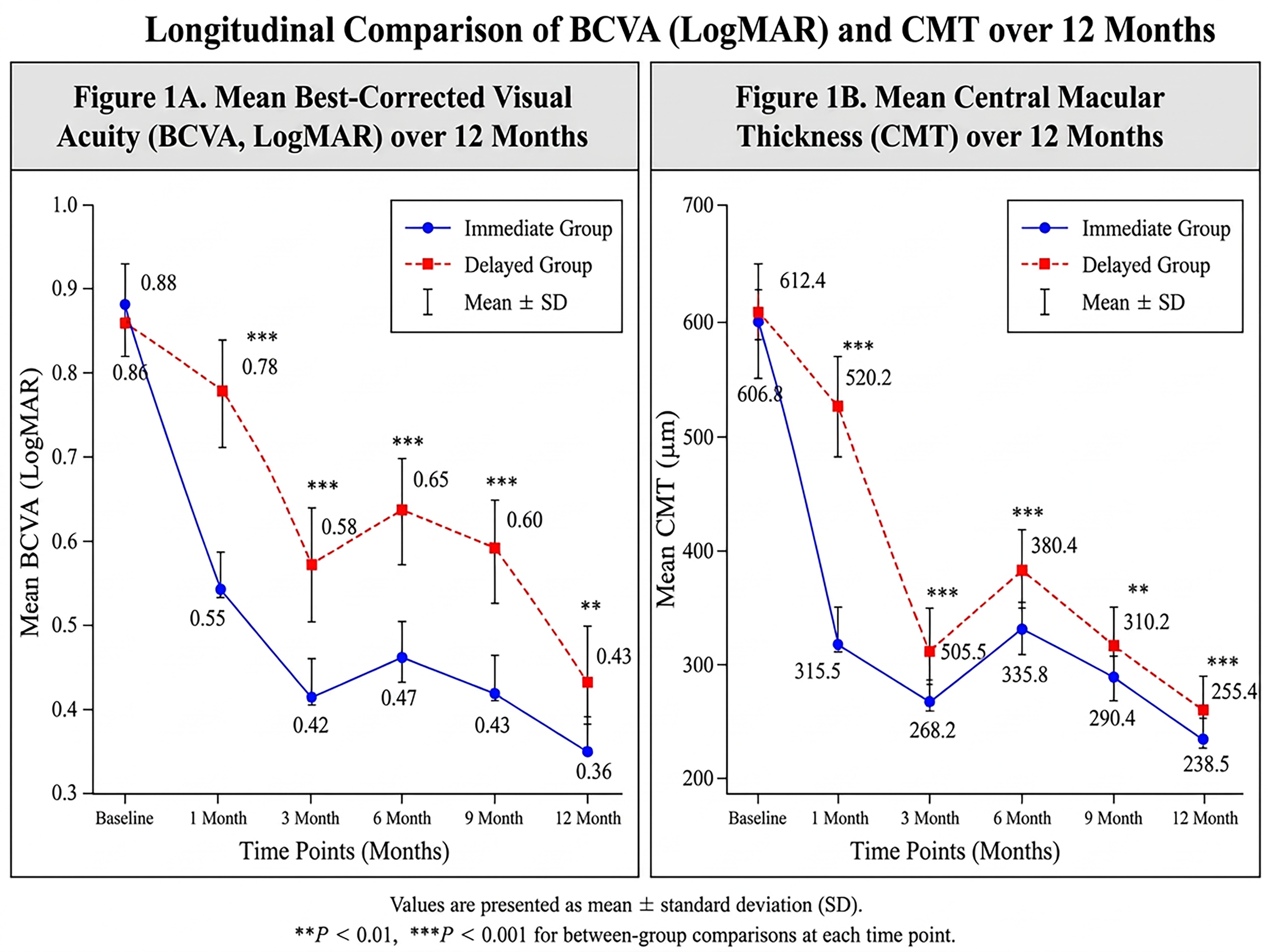
Longitudinal comparison of BCVA and CMT between the Immediate Group and the Delayed Group during the 12-month follow-up period.
Treatment burden and retreatment rates
According to the study protocol, all eyes in the Delayed Group received the first DEX implant at the 1-month postoperative visit. From month 3 onward, additional DEX implants were administered on a PRN basis in both groups according to the same retreatment criteria. DEX injection frequency and retreatment outcomes during the 12-month follow-up period are summarized in Table 6. The total number of DEX injections, including the initial scheduled DEX implant administered intraoperatively in the Immediate Group or at 1 month postoperatively in the Delayed Group, was 58 in the Immediate Group and 65 in the Delayed Group. The mean number of injections per eye was 1.45 ± 0.50 in the Immediate Group and 1.63 ± 0.62 in the Delayed Group, with no significant difference between groups (P = 0.157). A second DEX injection was required in 18 eyes (45.0%) in the Immediate Group and 22 eyes (55.0%) in the Delayed Group (P = 0.371). No eye in the Immediate Group required a third injection, whereas three eyes (7.5%) in the Delayed Group required a third injection during follow-up; however, the difference was not statistically significant (P = 0.241).
Comparison of retreatment rates and treatment burden over 12 months.
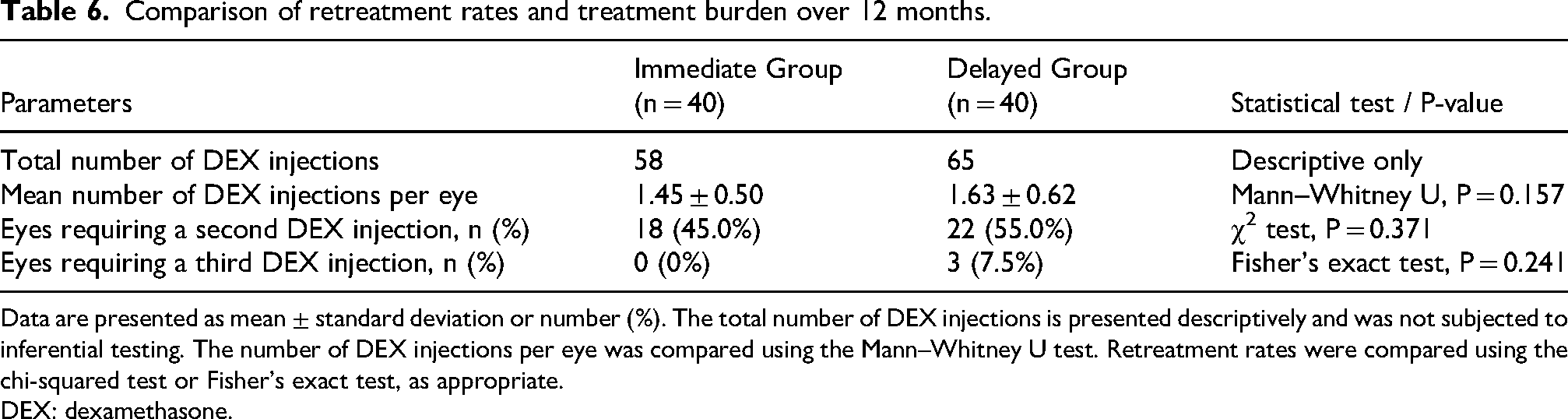
Data are presented as mean ± standard deviation or number (%). The total number of DEX injections is presented descriptively and was not subjected to inferential testing. The number of DEX injections per eye was compared using the Mann–Whitney U test. Retreatment rates were compared using the chi-squared test or Fisher's exact test, as appropriate.
DEX: dexamethasone.
Safety and IOP
IOP and safety outcomes are summarized in Table 7.
Intraocular pressure and safety outcomes during the 12-month follow-up.
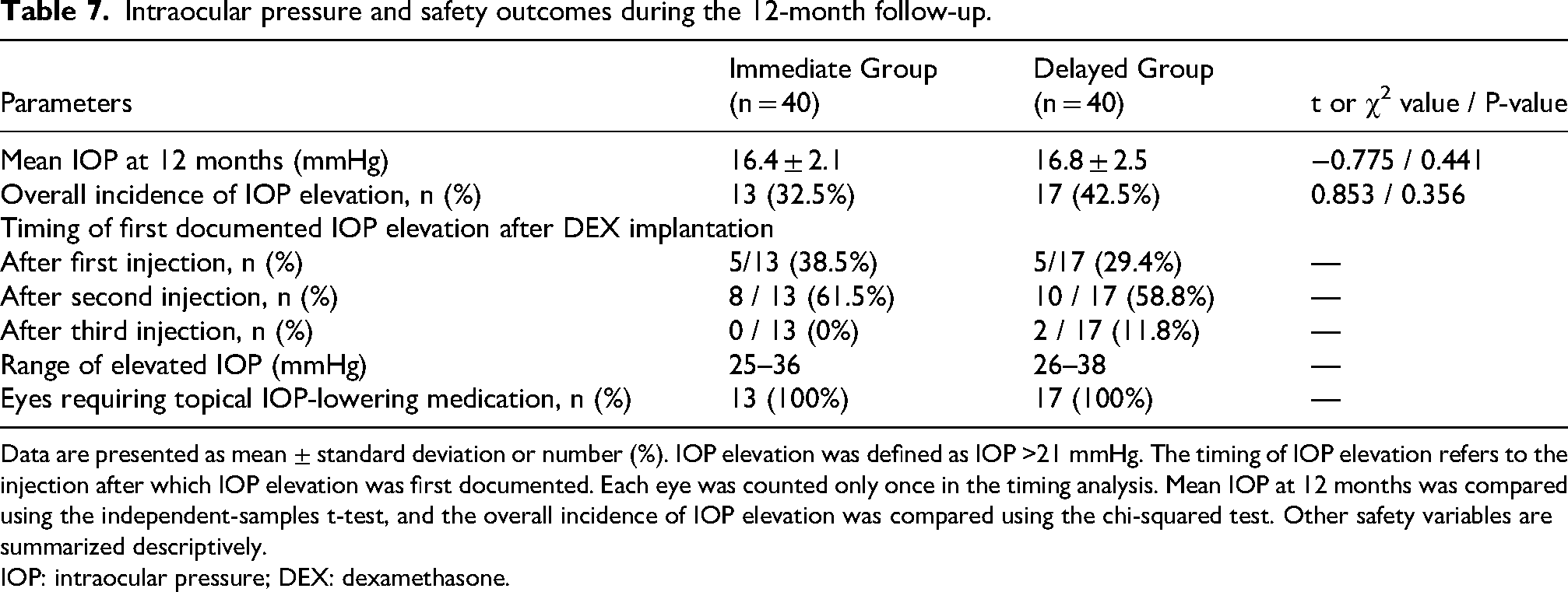
Data are presented as mean ± standard deviation or number (%). IOP elevation was defined as IOP >21 mmHg. The timing of IOP elevation refers to the injection after which IOP elevation was first documented. Each eye was counted only once in the timing analysis. Mean IOP at 12 months was compared using the independent-samples t-test, and the overall incidence of IOP elevation was compared using the chi-squared test. Other safety variables are summarized descriptively.
IOP: intraocular pressure; DEX: dexamethasone.
During the 12-month follow-up period, mean IOP remained within the normal range in both groups at all follow-up visits. At 12 months, mean IOP did not differ significantly between the Immediate Group and the Delayed Group (16.4 ± 2.1 vs. 16.8 ± 2.5 mmHg, P = 0.441). Transient IOP elevation (>21 mmHg) occurred in 13 eyes (32.5%) in the Immediate Group and 17 eyes (42.5%) in the Delayed Group, with no significant difference between groups (P = 0.356). In the Immediate Group, first documented IOP elevation occurred after the first injection in five eyes and after the second injection in eight eyes; no eye developed first documented IOP elevation after a third injection. In the Delayed Group, first documented IOP elevation occurred after the first injection in five eyes, after the second injection in 10 eyes, and after the third injection in two eyes. Each eye was counted only once in this timing analysis. All cases of elevated IOP were controlled with one or two topical IOP-lowering medications, and no patient required glaucoma surgery during follow-up.
Other adverse events
No cases of endophthalmitis, retinal detachment, or iatrogenic macular hole were observed during the 12-month follow-up period. No recurrence of ERM was detected after ILM peeling. In addition, no eyes progressed to severe proliferative DR requiring additional vitreoretinal surgery during follow-up. No systemic adverse events were documented in the medical records during follow-up.
Discussion
DME results from chronic hyperglycemia-induced activation of pro-inflammatory and pro-angiogenic cascades, leading to breakdown of the blood–retinal barrier and subsequent accumulation of fluid in the macula. It remains one of the leading causes of vision loss among patients with diabetes mellitus.6,7 Historically, focal or grid laser photocoagulation was recommended for clinically significant DME or lesions located within 500 μm of the foveal center. Although this approach may stabilize disease progression to some extent, it generally fails to improve visual acuity and is associated with complications such as paracentral scotomas, retinal scarring, and ERM formation.8,9 Recent evidence has established VEGF as a central mediator in the pathogenesis of DME, contributing to protease secretion, endothelial cell proliferation and migration, and neovascularization. In DR, upregulation of VEGF disrupts the blood–retinal barrier and increases vascular permeability, thereby promoting macular edema. 10 Consequently, intravitreal anti-VEGF agents, including conbercept, ranibizumab, and aflibercept, have emerged as first-line therapies for DME. However, these regimens typically require repeated injections over extended periods, imposing substantial financial burdens on patients. Moreover, frequent treatment requires good patient adherence, and a subset of individuals exhibit suboptimal responses, limiting the effectiveness of anti-VEGF therapy in refractory cases.11,12 Emerging data indicate that, beyond VEGF, inflammation driven by leukostasis and cytokine release also plays a pivotal role in DR-related vision loss. Multiple inflammatory mediators, including interleukins, chemokines, and adhesion molecules, are implicated in DME pathophysiology. 13 In eyes with coexisting ERM, mechanical traction and local inflammatory stimulation may further exacerbate macular edema through enhanced vascular leakage and microglial activation, thereby contributing to persistent preoperative macular edema. Corticosteroids exert anti-inflammatory effects by suppressing VEGF and other inflammatory cytokines, stabilizing the blood–retinal barrier, and reducing vascular permeability. 14 As such, they represent a valuable therapeutic option for DME. The DEX intravitreal implant (Ozurdex®), a biodegradable sustained-release formulation approved by the US Food and Drug Administration for DME, delivers 0.7 mg of DEX and provides therapeutic effects for up to 3–4 months. Comparative studies suggest that while Ozurdex achieves visual gains comparable to anti-VEGF therapy, it may be associated with more favorable anatomical outcomes, particularly in terms of CMT reduction. 15 A 2021 study on refractory DME reported peak improvements in BCVA and CMT at 2 months after injection, although recurrence required repeat dosing in some patients. 16 Several clinical trials have also supported the efficacy of Ozurdex in improving visual acuity and resolving macular edema.17,18
However, corticosteroid use is associated with known risks, particularly IOP elevation and cataract progression. In our cohort, transient IOP increases ranging from 25 to 38 mmHg were observed in a subset of patients in both groups. First documented IOP elevation occurred after the first or subsequent DEX injections, with most cases recorded after the second injection. Each eye was counted only once in this timing analysis. All cases of ocular hypertension were controlled with one or two topical IOP-lowering medications, and no patient required glaucoma surgery. These findings suggest that IOP elevation after DEX implantation may be more frequently observed after repeated dosing but remained clinically manageable throughout the 12-month follow-up period. In addition, all patients in this study were pseudophakic before surgery, which minimized the influence of lens opacity on visual outcomes. Therefore, we could not assess the risk of cataract formation associated with DEX implantation in phakic eyes. Further prospective studies including phakic and younger diabetic patients are needed to evaluate the long-term lens-related safety of this combined surgical approach. For patients with DME complicated by ERM, PPV combined with ERM and ILM peeling may offer anatomical benefits and help reduce the risk of recurrence. ILM removal likely contributes by eliminating residual adherent cells and the scaffold for membrane regrowth, thereby stabilizing the retinal microenvironment. 19 Surgical membrane peeling alone may relieve mechanical traction but does not fully address the underlying inflammatory milieu. Postoperative inflammatory activation and blood–retinal barrier disruption may exacerbate vascular permeability, potentially worsening macular edema. 20 Furthermore, ERM-induced distortion of the macular microstructure may persist or even progress due to gliotic remodeling after membrane removal, thereby impairing anatomical recovery. 21 Previous clinical evidence has suggested a potential role for combination therapy, with ERM peeling followed by adjunctive Ozurdex implantation showing better functional and structural outcomes compared with peeling alone. 22 For instance, Chang et al. randomized 40 patients with persistent post-ERM-peeling macular edema to receive either Ozurdex (n = 20) or observation (n = 20). The Ozurdex group demonstrated a rapid reduction in CMT at 1 month and sustained BCVA improvement through 6 months, whereas the control group showed no significant CMT change. However, CMT tended to rebound beyond 6 months, reflecting the waning effect of the implant. 23
In the present study, both treatment groups demonstrated overall improvement in BCVA and reduction in CMT during the 12-month follow-up period, although a transient rebound in CMT and mild BCVA worsening were observed around 6 months. Patients who received immediate intraoperative DEX implantation showed faster functional and anatomical recovery during the early postoperative period compared with those who underwent delayed treatment initiation. The longitudinal mixed-effects model further supported a significant interaction between treatment strategy and follow-up time for both BCVA and CMT outcomes. These findings suggest that the timing of corticosteroid administration may influence the postoperative recovery trajectory in patients with DME associated with ERM. The most pronounced difference between groups was observed during the early postoperative phase, particularly at 1 month. The Immediate Group achieved a greater reduction in CMT and greater BCVA improvement shortly after surgery. This early anatomical response may be related to prompt suppression of postoperative inflammatory cascades and rapid stabilization of the blood–retinal barrier following vitrectomy.24,25 Therefore, immediate intraoperative corticosteroid administration may help counteract postoperative inflammation and facilitate earlier retinal recovery. In addition, CMT fluctuations after 3 months appeared less pronounced in the Immediate Group, suggesting that early edema control may help maintain macular structural stability and reduce anatomical rebound after peeling of the secondary ERM.26,27
The apparent benefit of immediate intraoperative DEX implantation should be interpreted mainly as an early recovery advantage. The between-group differences in BCVA and CMT were most pronounced during the first 3 months after surgery, when postoperative inflammation and blood–retinal barrier instability are likely to be most active. Over time, particularly for CMT, the additional anatomical benefit became less pronounced. Therefore, these findings suggest that earlier corticosteroid exposure may accelerate early postoperative recovery rather than proving definitive long-term superiority of immediate implantation. Although the anatomical difference between groups gradually decreased during later follow-up, the visual advantage in the Immediate Group persisted throughout the 12-month observation period. At 12 months, CMT remained statistically lower in the Immediate Group, but the group × time interaction for CMT was no longer significant, suggesting that the magnitude of additional anatomical improvement associated with immediate treatment diminished over time. This apparent dissociation between anatomical and functional outcomes has also been reported in previous retinal studies. Several mechanisms may explain this phenomenon. Early resolution of macular edema may reduce prolonged photoreceptor disruption, Müller cell dysfunction, and outer retinal damage, thereby preserving visual function even after subsequent anatomical convergence between groups. In contrast, delayed corticosteroid exposure may allow persistent edema-related stress during the interval before DEX implantation, potentially limiting later functional recovery. Another notable finding was the overall stability of visual and anatomical improvement during long-term follow-up. Both groups maintained substantial reductions in CMT and sustained BCVA gains at 12 months, suggesting that vitrectomy combined with DEX implantation may be a useful treatment approach for DME complicated by ERM. Nevertheless, the better early outcomes observed in the Immediate Group suggest that earlier corticosteroid intervention may provide additional clinical benefit beyond eventual edema control alone. 28
The present study also supports the use of longitudinal statistical approaches when evaluating repeated postoperative measurements. Compared with conventional repeated pairwise comparisons, the linear mixed-effects model enabled simultaneous assessment of time effects, group effects, and group × time interaction effects while accounting for within-subject correlations. This approach may provide a more robust evaluation of postoperative recovery patterns and improve the reliability of longitudinal outcome interpretation. Moreover, the Immediate Group showed a numerically lower total number of DEX injections than the Delayed Group during the 12-month follow-up period. Although this difference did not reach statistical significance, this trend suggests that early intraoperative corticosteroid administration may help achieve more rapid edema control and potentially reduce the need for repeated retreatment in some patients. 29 Therefore, the potential effect of immediate DEX implantation on long-term retreatment burden requires confirmation in larger prospective studies. The anatomical data also showed a transient increase in CMT around 6 months in both groups, which may reflect the waning pharmacological effect of the DEX implant during follow-up. In vitrectomized eyes, the absence of the vitreous gel may accelerate intraocular drug clearance and shorten the effective duration of the implant, thereby contributing to temporary anatomical rebound before subsequent PRN retreatment.30,31 The Immediate Group appeared to show a less pronounced transient increase in CMT during follow-up, suggesting that early edema control may contribute to a more stable postoperative retinal microenvironment. In terms of safety, the rate of IOP elevation was numerically higher in the Delayed Group than in the Immediate Group (42.5% vs. 32.5%), although the between-group difference was not statistically significant. Because repeated corticosteroid exposure is a recognized risk factor for steroid-induced ocular hypertension, the slightly higher IOP elevation rate in the Delayed Group may be related in part to greater cumulative corticosteroid exposure. However, this interpretation remains uncertain because of the limited sample size and the lack of statistical significance. Similarly, whether the numerical reduction in retreatment frequency observed in the Immediate Group may translate into a more favorable safety profile requires further investigation in larger prospective studies.32,33 Several limitations of this study should be acknowledged. First, this was a retrospective, single-center, non-randomized comparative study. Treatment allocation was based on clinical practice rather than random assignment. Although baseline demographic and ocular characteristics were comparable between groups, residual confounding and selection bias cannot be completely excluded. Second, although 80 eyes were included, the relatively limited sample size may have reduced the ability to detect rare adverse events and may limit the generalizability of the findings. Third, variations in the timing and frequency of retreatment during follow-up may have introduced additional variability into long-term outcomes. Fourth, the 12-month follow-up period may not have been sufficient to fully evaluate the long-term effects of repeated intravitreal injections on retinal microstructure. In addition, several important imaging biomarkers, including ellipsoid zone integrity, disorganization of the retinal inner layers, and retinal capillary non-perfusion assessed by OCT angiography, were not quantitatively analyzed, which may further influence postoperative visual prognosis. 34 Future prospective multicenter studies with larger sample sizes, longer follow-up durations, and multimodal imaging assessments are warranted to further validate these findings.
Conclusion
In summary, this study suggests that immediate intraoperative DEX implantation was associated with more rapid early postoperative anatomical and visual recovery in pseudophakic patients with DME and secondary ERM undergoing PPV with ERM and ILM peeling. ERM peeling relieves macular traction, whereas ILM peeling may further reduce residual traction and the cellular scaffold for membrane recurrence, thereby contributing to a more stable postoperative retinal structure. Although CMT remained lower in the Immediate Group at 12 months, the longitudinal anatomical advantage diminished over time. In contrast, the BCVA benefit persisted at the final follow-up, suggesting that early edema control may have functional relevance beyond short-term anatomical improvement. The Immediate Group also showed a numerical tendency toward fewer DEX injections, but this difference was not statistically significant and should therefore be interpreted with caution. Given the retrospective and non-randomized design, these findings should be interpreted as associations rather than definitive evidence of causal superiority. Overall, immediate DEX implantation may be a clinically useful strategy for promoting early postoperative recovery in complex tractional DME, with a manageable safety profile throughout the 12-month follow-up period. Further prospective randomized studies with larger sample sizes and longer follow-up are needed to confirm these findings and to better define the optimal timing of corticosteroid use in vitreoretinal surgery.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605261463829 - Supplemental material for Immediate versus delayed dexamethasone implantation during vitrectomy for diabetic macular edema with secondary epiretinal membrane: A retrospective comparative study
Supplemental material, sj-pdf-1-imr-10.1177_03000605261463829 for Immediate versus delayed dexamethasone implantation during vitrectomy for diabetic macular edema with secondary epiretinal membrane: A retrospective comparative study by Jing Chen in Journal of International Medical Research
Footnotes
Acknowledgments
The author used ChatGPT only to assist with grammar correction, language polishing, and figure preparation during manuscript preparation. All scientific content, data analysis, interpretation of results, and final figure presentation were independently reviewed and verified by the author, who takes full responsibility for the accuracy and integrity of the manuscript.
Ethical considerations
Ethical approval was obtained from the Ethics Committee of People’s Hospital of Leshan (Approval No. LYLL[2024]KY-006; approved on 25 January 2024).
Consent for publication
Written informed consent for treatment and the use of anonymized clinical data for research and publication purposes was obtained from all patients prior to surgery. No identifiable patient information or images are included in this manuscript.
Author contributions
Jing Chen was responsible for the conception and design of the study, data acquisition, statistical analysis, interpretation of the results, drafting and revision of the manuscript, and final approval of the submitted version. The author agrees to be accountable for the accuracy and integrity of the work.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this retrospective comparative study are available from the corresponding author upon reasonable request. The data are not publicly available due to patient privacy and institutional regulations.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.