
Abstract
Objective
This study compared the efficacy of ilioinguinal/iliohypogastric, transversus abdominis plane, and quadratus lumborum blocks as adjuncts to spinal anesthesia for postoperative pain management in unilateral inguinal hernia repair.
Methods
This study was a prospective, randomized, controlled, single-blind study. Eighty patients were randomized into four groups: (a) ilioinguinal/iliohypogastric block group; (b) transversus abdominis plane block group; (c) quadratus lumborum block; and (d) control group. Postoperative pain was assessed using the visual analog scale at rest and during movement over 24 h. Total tramadol consumption via patient-controlled analgesia, supplemental paracetamol use, and opioid-related adverse effects were recorded.
Results
No statistically significant differences were found in visual analog scale scores among the groups at any time point (p > 0.05). Opioid consumption ranged from 60 to 300 mg, with a mean value of 226.79 ± 49.94 mg. There was no statistically significant difference in opioid use among the groups (p = 0.930; p > 0.05). The requirement for additional analgesics did not differ significantly among the groups (p = 0.389; p > 0.05). The overall incidence of adverse effects (postoperative nausea and vomiting, and respiratory depression) was 11.2% (n = 9). No statistically significant differences were observed in the rate of adverse effects between the groups (p = 0.069; p > 0.05).
Conclusion
No statistically significant differences were observed in pain scores, opioid consumption, or adverse effects between the three block groups and the control group. There was a nonsignificant trend toward lower visual analog scale scores in the ilioinguinal/iliohypogastric group compared with the transversus abdominis plane and quadratus lumborum groups during the postoperative period. Although the total number of patients requiring additional analgesics was lower in all three block groups compared with the control group, these findings were not statistically significant.
Clinical Trial Number
This trial was retrospectively registered at clinicaltrials.gov with trial number NCT06997536.
Keywords
Introduction
Inguinal hernias are the most common type of abdominal wall hernias, accounting for approximately 75% of all hernia cases. 1 Inguinal hernia is one of the most frequent conditions requiring surgical intervention. The lifetime incidence of groin hernia is 27% in men and 3% in women. 2 Globally, approximately 20 million inguinal hernia repair surgeries are performed each year.
Globally, millions of groin hernia repairs are conducted annually, and 8%–16% of these patients experience chronic pain to a degree that impairs their daily lives 6 months postoperatively. A small proportion of these patients experience disabling pain, and due to the large number of groin hernia repairs, the number of patients with disabling pain and discomfort is an important clinical problem. 3 The goal of postoperative pain management in inguinal hernia surgery is to reduce or eliminate pain and discomfort with minimal adverse effects at the lowest possible cost. 4 Effective postoperative analgesia modifies the physiological stress response and reduces postoperative complications, thereby shortening hospital stays and lowering healthcare costs. 5
Opioid use is associated with nausea, vomiting, respiratory depression, and immune suppression; therefore, minimizing opioid consumption has become a major objective in postoperative pain management. Consequently, the concept of multimodal analgesia, which incorporates regional anesthesia techniques, has emerged. 5
Both systemic and regional analgesia methods are used for postoperative pain management in inguinal hernia repair. Although the efficacy of epidural anesthesia is well established, peripheral nerve blocks—such as the ilioinguinal/iliohypogastric (IL/IH) block, transversus abdominis plane (TAP) block, and quadratus lumborum (QLB) block—have recently gained popularity in postoperative analgesia. 6 These peripheral techniques offer advantages such as hemodynamic stability and early mobilization while reducing opioid consumption and the need for additional analgesics. 7
Several studies have demonstrated that abdominal wall blocks significantly reduce postoperative pain and opioid consumption during the first 24 h after surgery and are associated with fewer adverse effects. 8 Although individual studies have shown the benefits of TAP, IL/IH, and QLB blocks, there are few comparative studies investigating the efficacy of all three techniques in inguinal hernia surgery.
Therefore, in this study, we aimed to compare postoperative pain control and analgesic requirements among patients undergoing inguinal hernia repair under spinal anesthesia who received IL/IH, TAP, or QLB blocks and a control group without any additional regional block. Pain was assessed using the visual analog scale (VAS) at 30 min, 2, 6, 12, and 24 h postoperatively. Opioid-related adverse effects such as nausea, vomiting, and respiratory depression; total tramadol consumption via patient-controlled analgesia (PCA); and the amount of paracetamol administered as supplemental analgesia were also recorded and compared between the groups.
Materials and methods
Ethical approval and informed consent
This study was conducted in accordance with the ethical principles of the 1975 Declaration of Helsinki and its 2024 revision. The study was reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) 2025 statement. 9 Ethical approval was obtained from the Clinical Research Ethics Committee of Tekirdağ Namık Kemal University Faculty of Medicine on 28 June 2022 (Protocol Number: 2022.113.06.03), and the study was retrospectively registered at the Clinical Trials Protocol Registration and Results System (NCT06997536). All participants were fully informed about the study procedures and provided written informed consent. The study was conducted over a period of 12 months.
Artificial intelligence–based language model (ChatGPT, OpenAI) was used during the preparation of the manuscript for language editing and proofreading purposes, and all content was reviewed and verified by the authors.
Sample size and randomization
After obtaining written and verbal informed consent, this prospective, randomized, single-blind study was conducted between June 2022 and June 2023 in the general surgery operating room of Tekirdağ Namık Kemal University in patients aged 18–75 years who were scheduled for elective unilateral inguinal hernia repair.
Patients were randomly assigned into four groups: (a) those receiving IL/IH block after spinal anesthesia (Group IL/IH, n = 20); (b) those receiving TAP block after spinal anesthesia (Group TAP, n = 20); (c) those receiving QLB block after spinal anesthesia (Group QLB, n = 20); and (d) those receiving spinal anesthesia only (control group, n = 20). Randomization was performed using a computer-generated random number table and sealed envelope method.
To ensure quality and standardization of the blocks, all IL/IH, TAP, and QLB procedures were performed by an experienced anesthesiologist. The anesthesiologist performing the block was informed of the specific block assignment via a sealed envelope by an independent assistant who was not involved in the study. Postoperative follow-up and assessments were conducted by a blinded specialist who was unaware of the patients’ group assignments.
In the study titled “Ultrasound Guided Ilioinguinal, Iliohypogastric Nerve Block, Transversus Abdominis Plane Block and Quadratus Lumborum Block for Scheduled Cesarean Delivery: A Randomized Clinical Trial” conducted by Mogahed et al., the effect size for the comparison of 24-h pain scores between the groups was reported as 0.519. Based on this reference study, it was calculated that a total of 68 patients would be required to achieve the adequate sample size with 95% power, a 5% margin of error, and an effect size of 0.519. Considering possible dropouts, an additional 20% was added, and a total sample size of 80 patients was targeted. 10
Inclusion criteria
Patients aged 18–75 years who were scheduled for elective unilateral inguinal hernia repair under spinal anesthesia, classified as American Society of Anesthesiologists (ASA) physical status I or II and who voluntarily provided written informed consent to participate in the study, were included.
Exclusion criteria
Patients were excluded if they had preoperative neurological deficits, known hypersensitivity to local anesthetics, active infection at the planned block site, scheduled bilateral inguinal hernia surgery, a history of coagulopathy, a body mass index (BMI) greater than 30 kg/m2, age <18 or >75 years, or declined to participate in the study.
Intervention
All patients were brought to the operating room, and routine monitoring was performed for all four groups, including electrocardiography (ECG), peripheral oxygen saturation (SpO2), and non-invasive blood pressure measurement. After establishing intravenous (IV) access, fluid replacement was initiated using isotonic 0.9% sodium chloride, with the infusion rate adjusted according to the patients’ preoperative fasting duration, body weight, and intraoperative fluid losses.
The patient was placed in the sitting position, and the L4–L5 interspace was identified by palpation. After ensuring sterile conditions, a 26G spinal needle (Spinocan® Braun, Melsungen, Germany) was inserted into the subarachnoid space. Clear cerebrospinal fluid (CSF) flow was confirmed, and 3 mL (15 mg) of 0.5% hyperbaric bupivacaine (Buvasin®) was administered. Motor and sensory block levels were subsequently assessed using the pin-prick test. Once a sensory block below the T10 level was achieved, the patient's head was elevated by 30°. The blocks were performed after spinal anesthesia and at least 20 min before the start of surgery. The control group proceeded directly to surgery without receiving any additional block.
For Group IL/IH (n = 20), an ultrasound-guided IL/IH block was performed in the supine position. A linear probe (Esaote MyLabX7, UK) with a depth setting of 4–6 cm was used. Conductive gel was applied to the probe, which was then covered with a sterile sheath. The procedural area was disinfected with 10% povidone–iodine solution and covered with a sterile drape. The ultrasound probe was placed along an imaginary line connecting the anterior superior iliac spine (ASIS) to the umbilicus. The ilioinguinal and iliohypogastric nerves, located between the internal oblique and transversus abdominis muscles, were visualized (Figure 1).
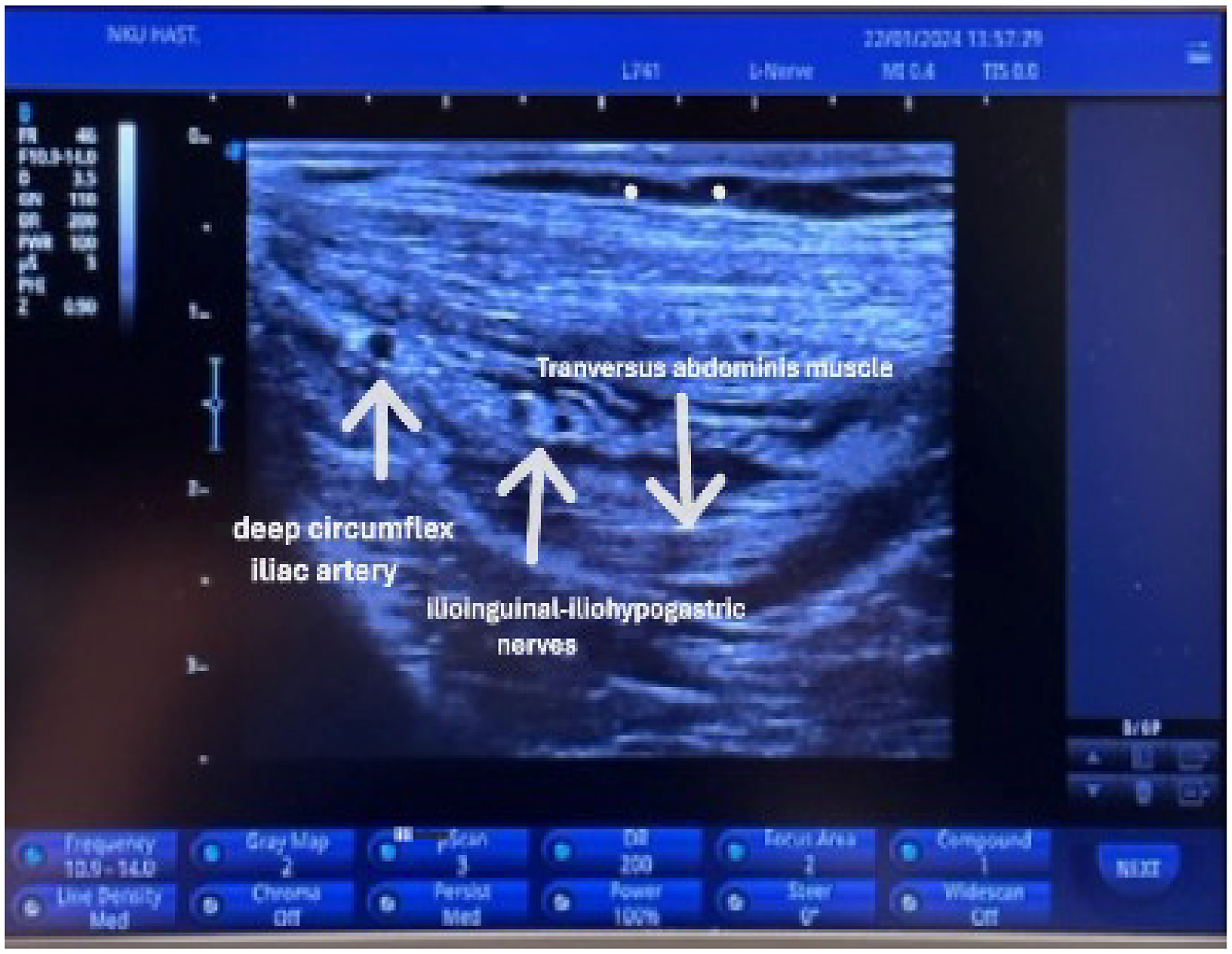
Ultrasound image of the ilioinguinal/iliohypogastric (IL/IH) block.
A 50-mm, 22G peripheral nerve needle (Stimuplex® Ultra, Braun, Melsungen, Germany) was advanced using an in-plane technique to reach the target area. In total, 20 mL of 0.25% bupivacaine, prepared in advance, was injected around the nerves. During injection, the spread of the local anesthetic was observed under ultrasound as the fascial planes of the internal oblique and transversus abdominis muscles separated. Aspiration was performed before injection and after every 5 mL to prevent intravascular injection.
For Group TAP (n = 20), an ultrasound-guided TAP block was performed in the supine position. A linear ultrasound probe (Esaote MyLabX7, UK) was used, with the depth set to 4–6 cm. Conductive gel was applied to the probe, which was then covered with a sterile sheath. The procedural area was disinfected using 10% povidone–iodine and draped with a sterile cover.
The linear probe was positioned on the lateral abdominal wall between the costal margin and iliac crest, visualizing the external oblique, internal oblique, and transversus abdominis muscles. Using a 21G, 100-mm short-beveled needle (Stimuplex Ultra 360®, Braun, Germany), the plane between the internal oblique and transversus abdominis muscles was reached using an in-plane technique (Figure 2). In total, 20 mL of 0.25% bupivacaine was injected. The spread of the local anesthetic between the fascial planes of the internal oblique and transversus abdominis muscles was confirmed under ultrasound. Aspiration was performed before injection and after every 5 mL to prevent intravascular injection.
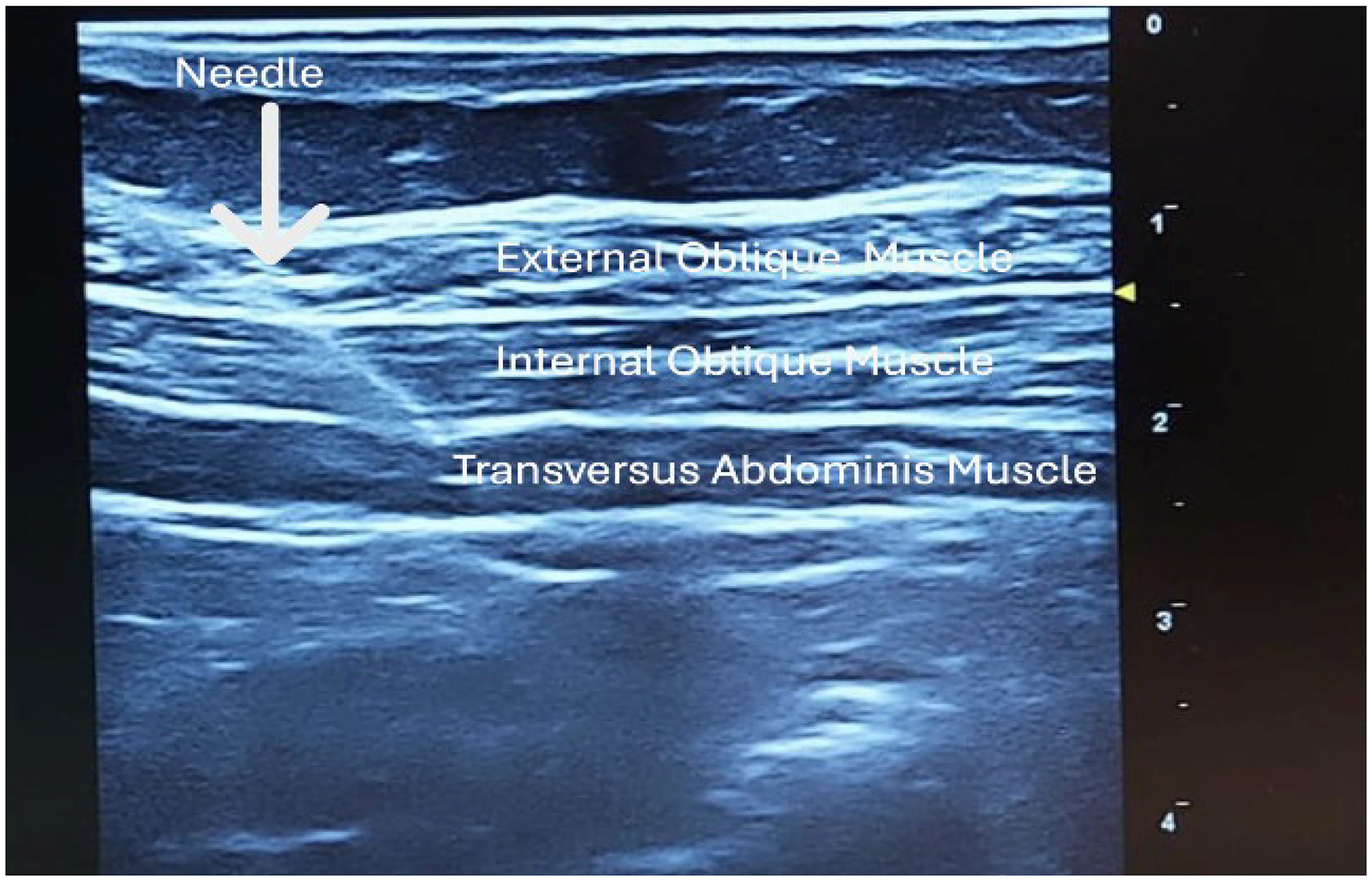
Ultrasound image of the transversus abdominis plane (TAP) block.
For Group QLB (n = 20), a QLB3 block was performed with the patient in the lateral decubitus position. The side to be blocked was positioned on top. The upper part of the iliac crest and the mid-axillary area were disinfected thrice with 10% povidone–iodine and then covered with a sterile drape.
A convex ultrasound probe (Esaote MyLabX7, UK) was used, with a depth setting of 5–10 cm. Conductive gel was applied to the probe, which was then covered with a sterile sheath. The probe was placed slightly above the iliac crest along the mid-axillary line. By advancing posterolaterally, the aponeurosis of the external oblique, internal oblique, and transversus abdominis muscles overlying the QLB muscle was visualized, with the transverse process of the vertebra positioned beneath the QLB muscle.
Using an in-plane technique, a 21G, 100-mm short-beveled needle (Stimuplex Ultra 360®, Braun, Germany) was advanced through the anterior aspect of the QLB muscle. In total, 20 mL of 0.25% bupivacaine was injected, with aspiration performed every 5 mL to prevent intravascular injection. The spread of the local anesthetic between the QLB and psoas major muscles was confirmed under ultrasound (Figure 3). After the procedure, the patient was returned to the supine position.
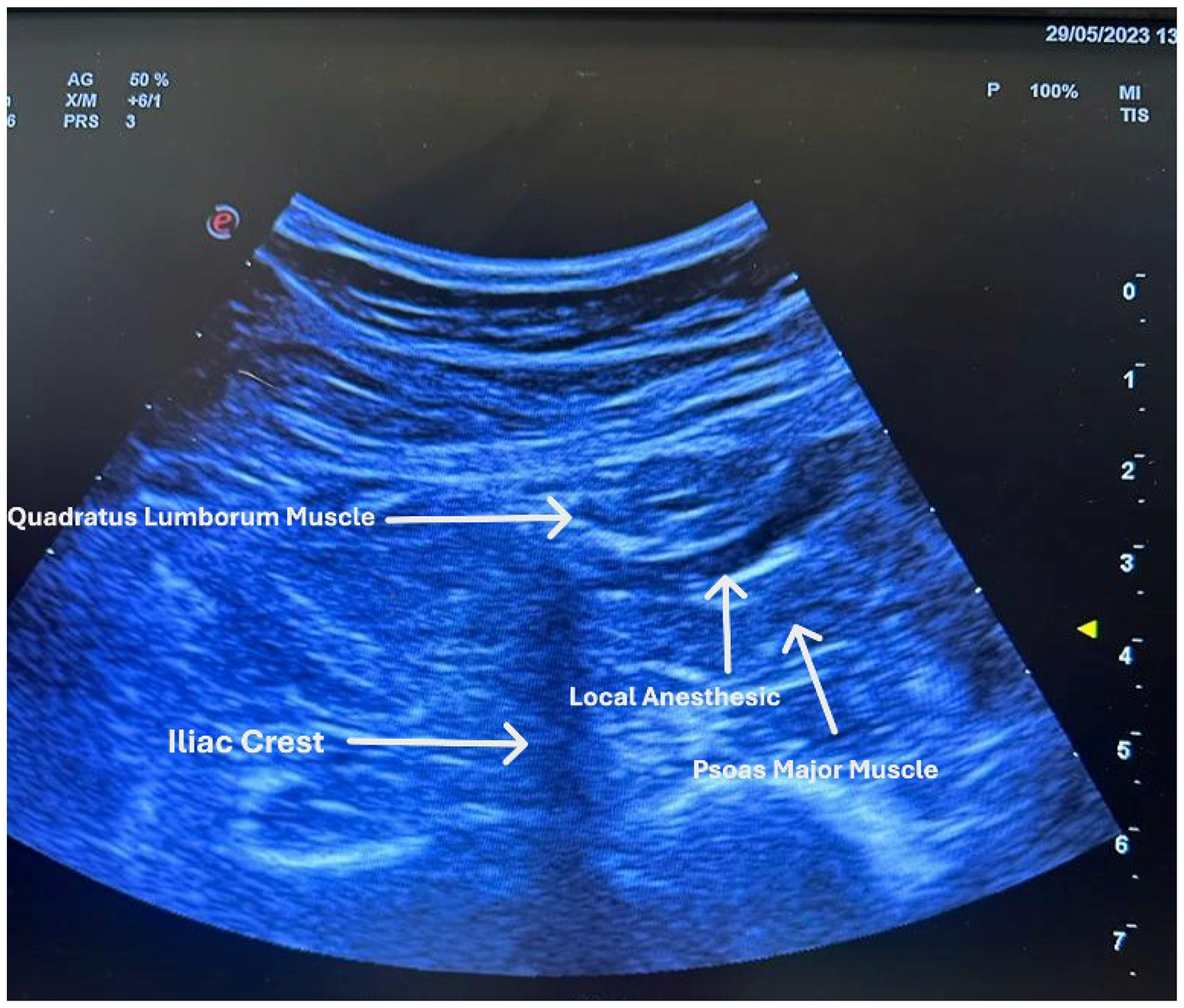
Ultrasound image of the quadratus lumborum block (QLB).
Surgery was initiated 20 min after the blocks were performed in the respective groups. No intraoperative analgesic agents were administered. During the operation, SpO2, heart rate, and non-invasive blood pressure were continuously monitored. Postoperatively, patients were transferred to the post-anesthesia care unit (PACU). Heart rate and SpO2 were continuously monitored, while non-invasive blood pressure was measured every 5 min.
PCA was set up, and IV access was established in the PACU. Tramadol was prepared at a concentration of 3 mg/mL in 100 mL of isotonic saline (total 300 mg). The PCA device was programmed with an infusion rate of 3 mL/h, a 5 mL bolus dose, a 20-min lockout interval, a maximum limit of 216 mg over 4 h and continuous use for 24 h. If patients requested additional opioids via the PCA device but reported a VAS score ≥4, 1 g of IV paracetamol was administered as a supplemental analgesic, and the ward nurses were informed. Patients were monitored in the PACU for 30 min. For patients with a modified Aldrete score ≥9, the PCA device was reviewed, pain assessment procedures were re-explained, and the general surgery team was notified before transferring the patient to the ward.
Demographic data (age, weight, height, BMI), comorbidities, ASA physical status, surgical duration, preoperative heart rate, mean arterial pressure, and SpO2 were recorded for all patients. Heart rate, SpO2, and mean arterial pressure were recorded before and after spinal anesthesia, intraoperatively at 1, 2, and 4 h, and postoperatively. Pain intensity was assessed using the VAS, a 10-cm horizontal line anchored by “0 = no pain” and “10 = worst imaginable pain.” Patients were asked to indicate their current pain level on the scale, and the distance (in centimeter) from the “0” point to the marked point was recorded as the VAS score. 11 Postoperative pain assessment was performed at PACU 30 min, 2, 6, 12, and 24 h using the VAS. Opioid-related adverse effects such as nausea, vomiting, respiratory depression; total tramadol consumption (bolus and infusion); and additional paracetamol usage were recorded by a blinded observer.
Statistical analyses
Statistical analyses were conducted using Number Cruncher Statistical System (NCSS) 2007 software (Kaysville, Utah, USA). Continuous variables were summarized using descriptive statistics, including mean, SD, median, minimum, and maximum values, while categorical variables were presented as frequencies and percentages. The distribution of quantitative data was evaluated using the Shapiro–Wilk test in combination with graphical assessments.
Considering the limited sample size of the study, quantitative variables were evaluated as non-normally distributed based on the results of normality analyses and graphical assessments; therefore, non-parametric statistical methods were preferred where appropriate. For comparisons between two groups, non-normally distributed variables were assessed using the Mann–Whitney U test. For comparisons involving three or more groups, non-normally distributed variables were analyzed with the Kruskal–Wallis test followed by Bonferroni–Dunn post-hoc tests. In the evaluation of VAS scores, considering the multiple comparisons performed across nine time points and two conditions (rest/movement), Bonferroni correction was applied to control the risk of type I error, and the significance threshold was adjusted to 0.05/18. Although this conservative approach may increase the risk of type II error, statistical significance was evaluated according to the corrected p-value threshold. Categorical data were examined using the Fisher–Freeman–Halton test or Fisher's exact test, as appropriate. A two-tailed p-value <0.05 was considered statistically significant. No subgroup or adjusted analyses were performed.
The study was retrospectively registered at clinicaltrials.gov under the identifier NCT06997536.
Results
Participant characteristics
The study was performed at Tekirdağ Namık Kemal University Hospital. Following the exclusion of 38 patients who did not meet the eligibility criteria, a total of 80 patients, aged 18–75 years, scheduled for unilateral inguinal hernia repair, were included in the study. Patients were randomly assigned into four groups: (a) those receiving IL/IH block after spinal anesthesia (Group IL/IH, n = 20); (b) those receiving TAP block after spinal anesthesia (Group TAP, n = 20); (c) those receiving QLB block after spinal anesthesia (Group QLB, n = 20); and (d) those receiving spinal anesthesia only (Group Control, n = 20). No statistically significant differences were observed in the demographic characteristics between the groups (Table 1).
Comparison of demographic characteristics between the groups.
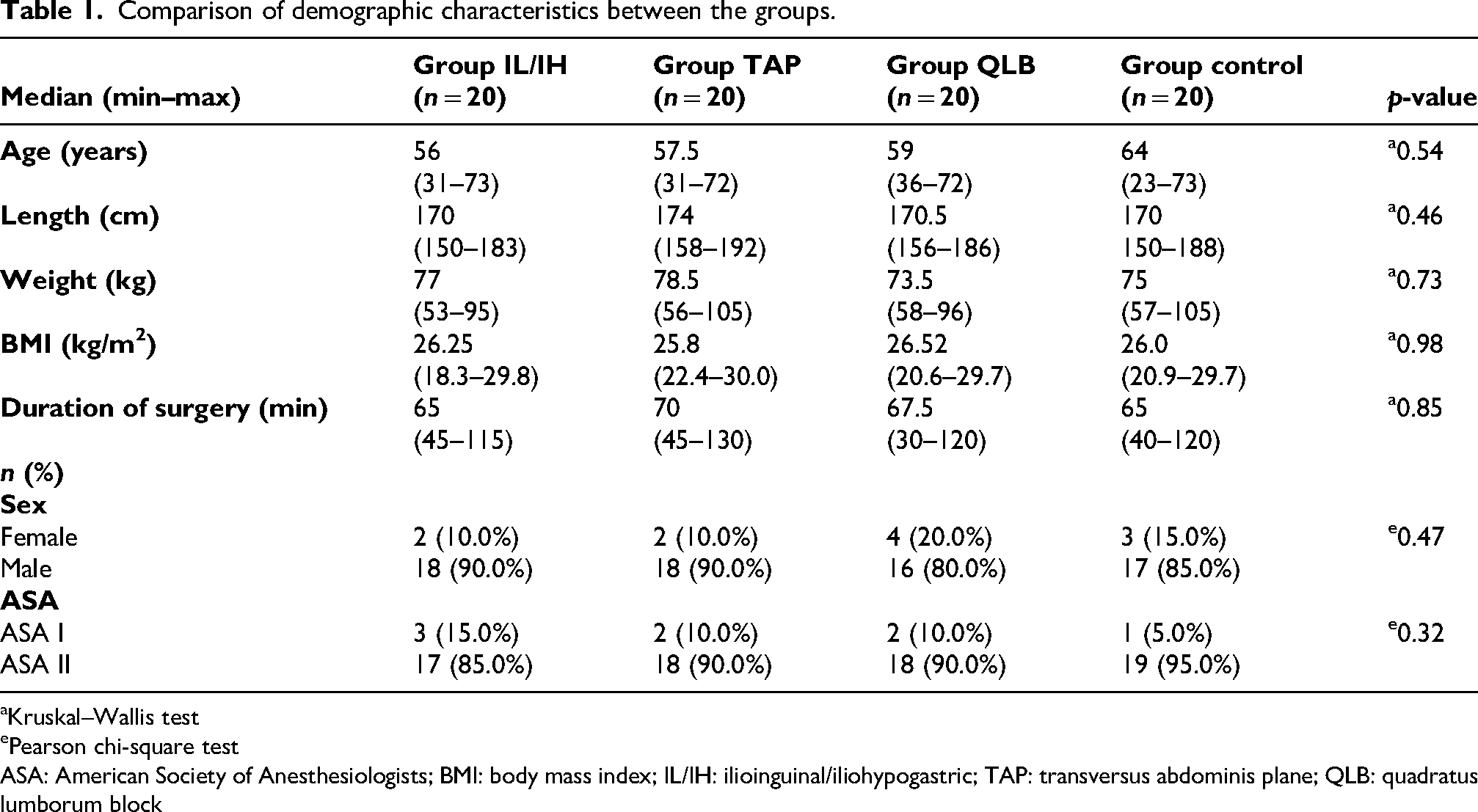
Kruskal–Wallis test
Pearson chi-square test
ASA: American Society of Anesthesiologists; BMI: body mass index; IL/IH: ilioinguinal/iliohypogastric; TAP: transversus abdominis plane; QLB: quadratus lumborum block
Postoperative pain scores
The mean VAS scores were 1.46 ± 2.10 at PACU 30 min, 3.30 ± 2.40 at 2 h at rest, 4.14 ± 2.75 at 2 h during movement, 3.41 ± 2.17 at 6 h at rest, 4.53 ± 2.43 at 6 h during movement, 2.81 ± 2.14 at 12 h at rest, 3.73 ± 2.35 at 12 h during movement, 1.55 ± 1.72 at 24 h at rest, and 2.41 ± 1.94 at 24 h during movement (Table 2).
Distribution of VAS scores across the groups.
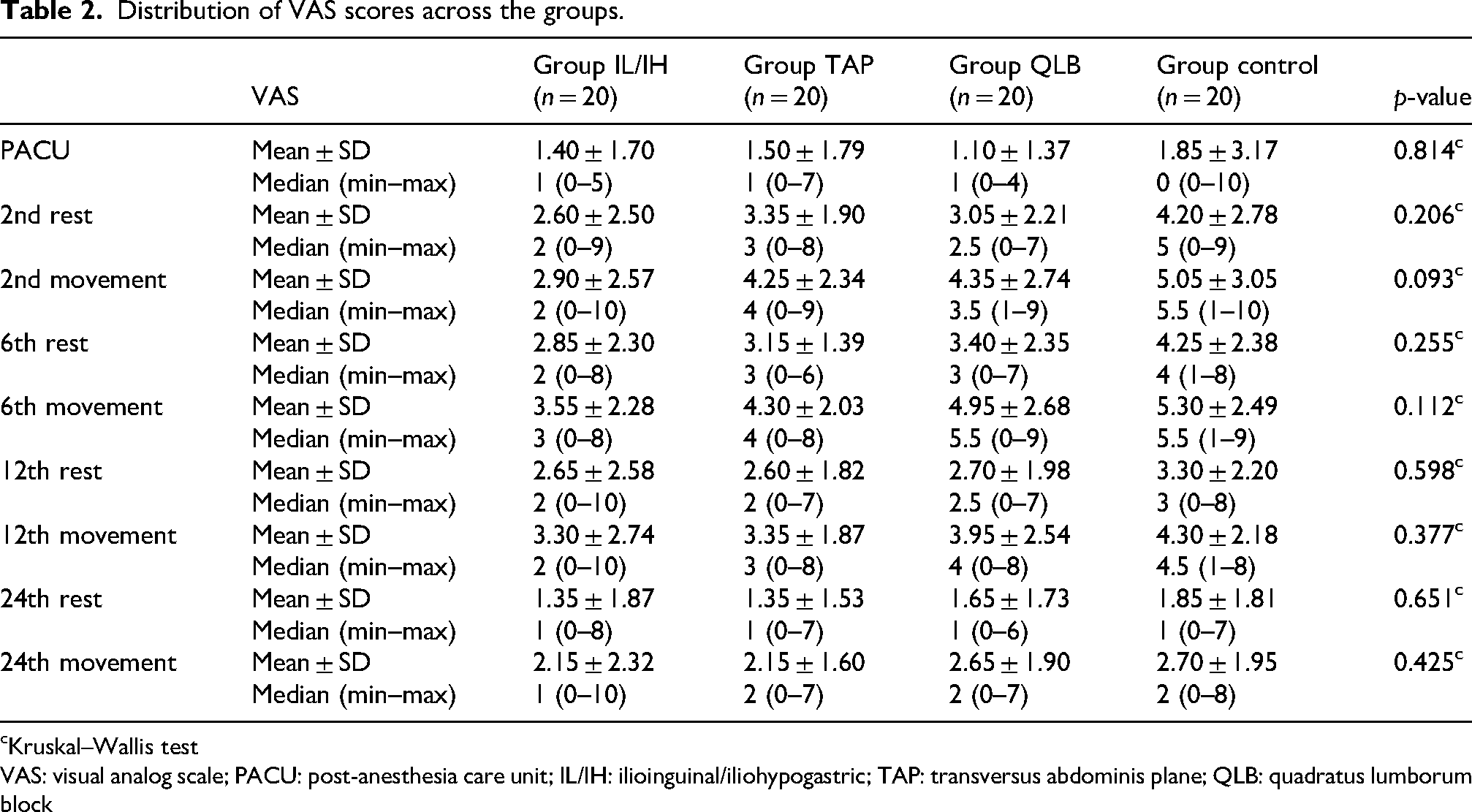
Kruskal–Wallis test
VAS: visual analog scale; PACU: post-anesthesia care unit; IL/IH: ilioinguinal/iliohypogastric; TAP: transversus abdominis plane; QLB: quadratus lumborum block
No significant differences were observed in the VAS scores of the groups at 30 min in the PACU, at 2, 6, 12, and 24 h postoperatively both at rest and during movement (all p > 0.05). Additionally, the changes in VAS scores over time were comparable across all groups (p = 0.601; p > 0.05). (Figures 4 and 5) (Table 2).
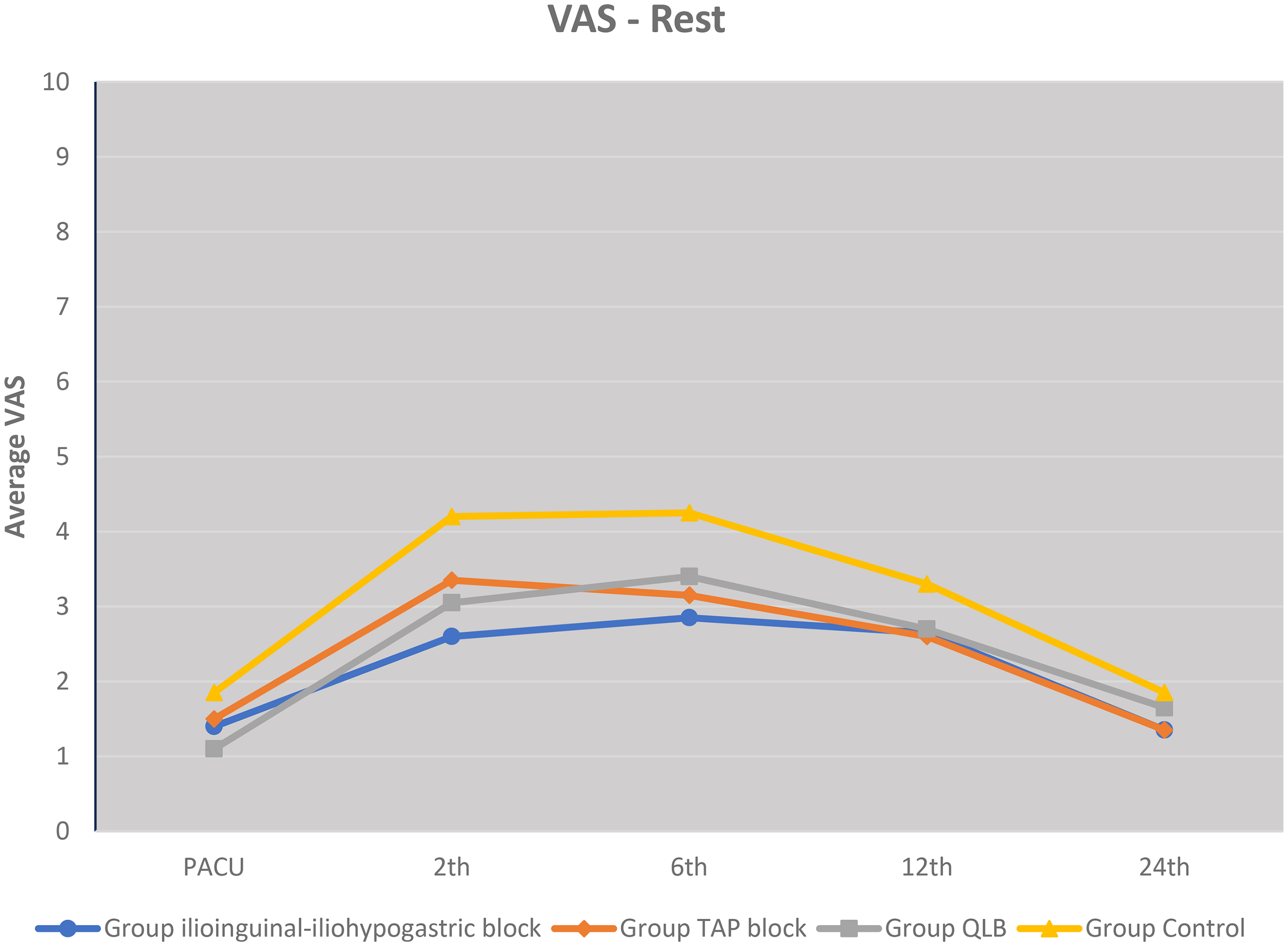
Distribution of VAS scores at rest across the groups.
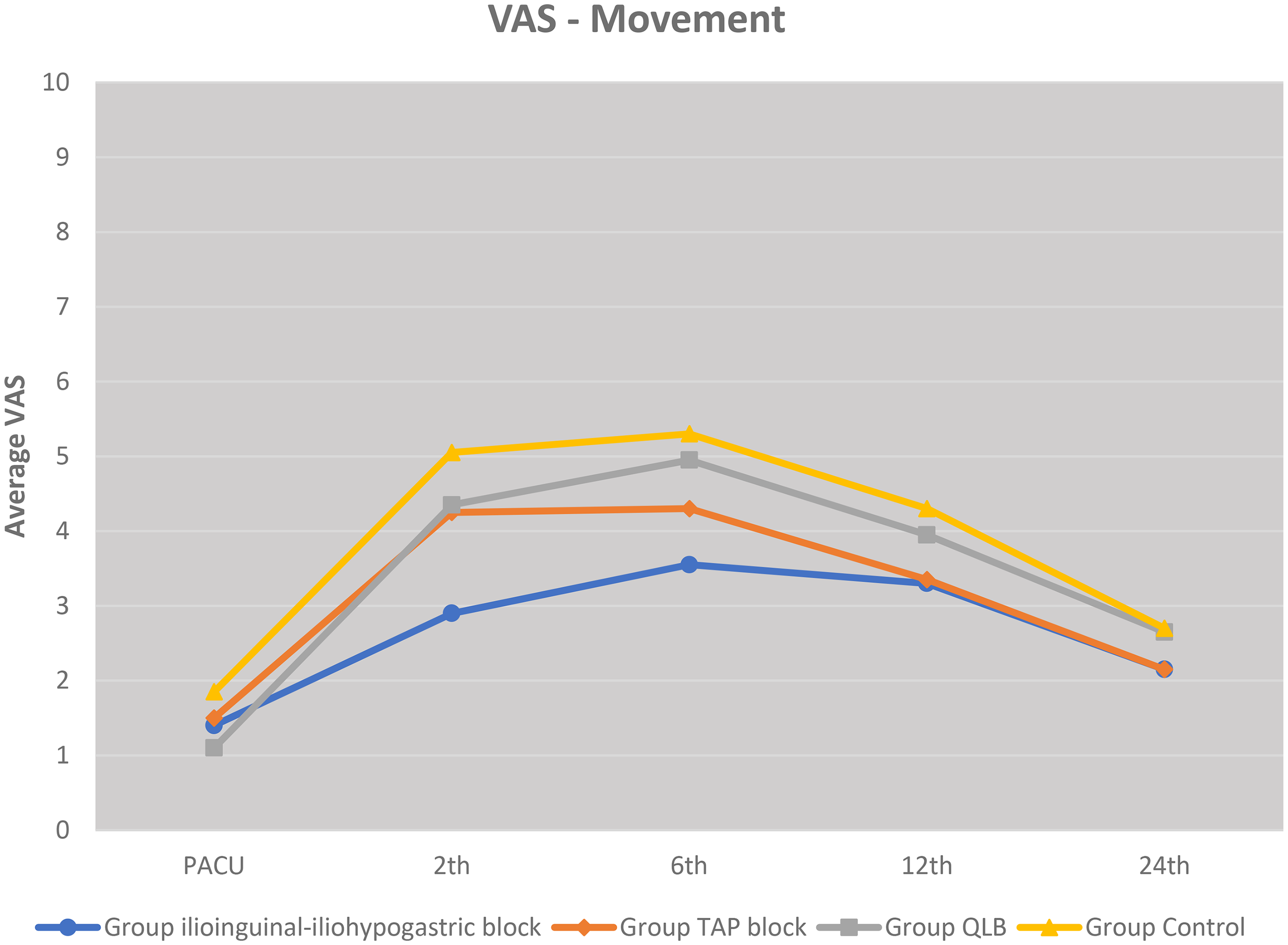
Distribution of VAS scores at movement across the groups.
Postoperative total opioid consumption, rescue analgesia, and adverse events
Opioid consumption ranged from 60 to 300 mg, with a mean value of 226.79 ± 49.94 mg. There was no statistically significant difference in opioid use between the groups (p = 0.930; p > 0.05).
The requirement for additional analgesics did not differ significantly among the groups (p = 0.389; p > 0.05) (Table 3).
Distribution of opioid consumption, additional analgesic requirement, and adverse effects across the groups.
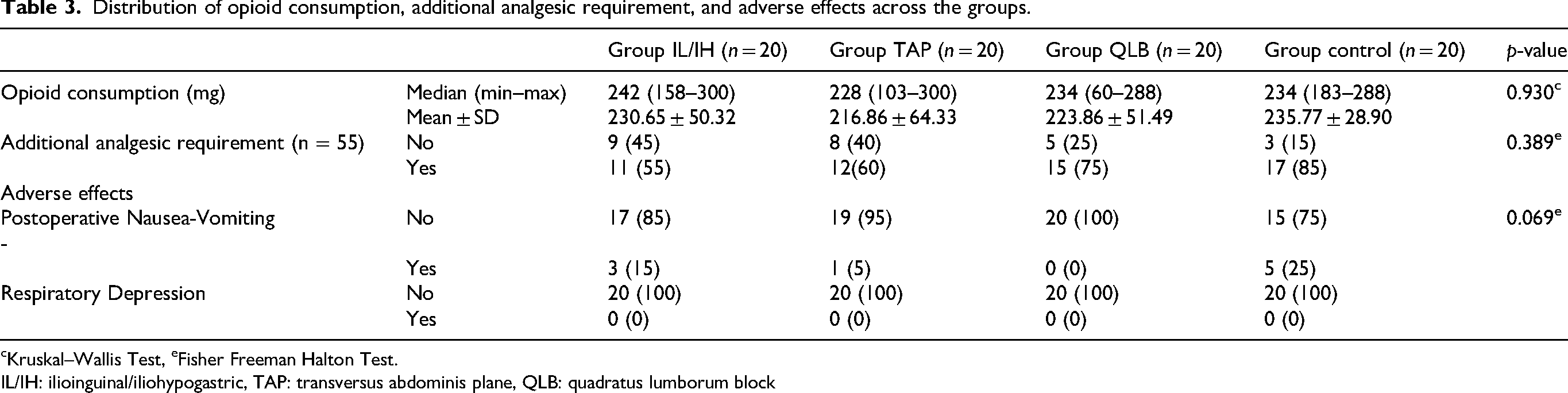
Kruskal–Wallis Test, eFisher Freeman Halton Test.
IL/IH: ilioinguinal/iliohypogastric, TAP: transversus abdominis plane, QLB: quadratus lumborum block
The overall incidence of adverse effects (postoperative nausea-vomiting and respiratory depression) was 11.2% (n = 9) (Table 3). There were no statistically significant differences in the rate of adverse effects between the groups (p = 0.069; p > 0.05).
Discussion
The primary goal of postoperative pain management in inguinal hernia surgery is to reduce or eliminate pain and discomfort with minimal adverse effects at low cost. The use of multimodal analgesia in postoperative pain management has become increasingly popular as it reduces opioid consumption and opioid-related adverse effects, shortens hospital stay and costs, and achieves better pain scores. 5 Effective control of acute postoperative pain with multimodal analgesic methods is crucial to prevent the development of chronic pain. 12
To the best of our knowledge, no studies in the literature have compared the three regional techniques used in our study together with a control group as four separate groups in patients undergoing unilateral inguinal hernia surgery. Although the sample size of our study was limited, we believe that our study contributes to the literature regarding the comparison of the postoperative analgesic efficacy of these three regional anesthesia techniques in inguinal hernia surgery.
As illustrated in Figures 4 and 5, the trends in VAS scores at rest and during movement exhibited a statistically nonsignificant decreasing trend in the IL/IH block group compared with that in the other groups. The VAS scores during movement at postoperative 2 h in the IL/IH group approached statistical significance when compared with the control group but did not reach statistical significance. We believe that this trend may become clinically significant in future studies with larger sample sizes.
In the literature, Baerentzen et al. have evaluated the efficacy of ultrasound-guided IL/IH nerve block in adult patients undergoing unilateral inguinal hernia repair under general anesthesia. Patients who received IL/IH block had significantly lower VAS scores in the PACU and at 30 min both at rest and during movement as well as lower resting VAS scores at discharge. 13
Venkatraman et al. randomly assigned 60 patients scheduled for elective inguinal hernia repair into two groups. Pain intensity was evaluated using the VAS. IV paracetamol was administered when the VAS score exceeded 3, and IV tramadol was administered when the VAS score exceeded 6. In the group receiving TAP block with ropivacaine, VAS scores and total analgesic requirements at postoperative 4, 6, and 12 h were significantly lower than those in the control group. 14
There is limited literature on the use of QLB block in adult patients undergoing inguinal hernia repair. Yadav et al. compared QLB and IL/IH block groups in patients undergoing unilateral inguinal hernia surgery and found that VAS scores during the first 24 h were significantly lower in the QLB group than in the IL/IH group. 15 In line with these studies demonstrating that TAP block, IL/IH block, and QLB provide effective postoperative analgesia in adult inguinal hernia surgery, our study, which was conducted to compare these methods, also did not reveal a statistically significant difference.
Although opioids play a key role in the management of moderate-to-severe postoperative pain, some studies recommend minimizing opioid use to avoid potential adverse effects, using opioids as a last resort, or reducing opioid doses.16,17 Increased postoperative opioid consumption can lead to adverse effects such as respiratory depression, nausea, vomiting, and pruritus. Faiz et al. conducted a prospective randomized study comparing ultrasound-guided IL/IH block and TAP block in 90 patients undergoing open inguinal hernia repair (45 patients in each group). The VAS scores at rest and during movement were lower in the IL/IH group than in the TAP block group, and analgesic satisfaction was higher. No difference was found between the two groups regarding postoperative opioid requirements. Although there was no difference in the parenteral analgesic doses, patients in the IL/IH block group requested the first analgesic dose 2.1 h later than those in the TAP block group. No nausea or vomiting was observed in either group. 18
Similarly, in our study, consistent with the findings of this study, no significant difference was found in opioid consumption among the block groups. During the 24-hour follow-up period, no patient developed respiratory depression. The highest incidence of nausea and vomiting was observed in the control group, although the difference was not statistically significant. Additional IV paracetamol was administered to patients requiring extra analgesia within the first 24 h despite PCA tramadol.
This study has certain methodological limitations. The fact that the study was conducted at a single center has been recognized as an important methodological limitation as it may have restricted the evaluation of patient population diversity and variability in clinical practice within a limited setting. The relatively small sample size may have limited the ability to detect statistical significance in subgroup analyses. Follow-up was only limited to the first 24 h postoperatively; therefore, the long-term analgesic efficacy, late complications, or development of chronic pain could not be evaluated. Additionally, potential surgeon-dependent variations that could affect block efficacy were not completely eliminated. Nonetheless, the prospective, randomized design; balanced groups; and standardized surgical–anesthetic protocol support the validity of the results.
A further limitation of this study is the relatively low statistical power observed in the post-hoc power analysis. This may be explained by the smaller-than-expected effect size observed in the study compared with the effect size used in the a priori sample size calculation. Although the planned sample size was achieved, the reduced observed effect may have limited the ability to detect statistically significant differences between groups. Therefore, the findings should be interpreted with caution, and larger studies with higher statistical power are warranted to confirm these results.
A potential limitation of this study is the use of a standardized spinal anesthesia dose (15 mg hyperbaric bupivacaine) without adjustment according to patient height. Although the relationship between anthropometric factors and spread of spinal anesthesia remains controversial, and several studies have reported no consistent correlation, the application of a uniform dosing protocol in patients with varying body heights may have acted as a potential confounding factor affecting the extent of sensory block and postoperative analgesic outcomes. However, no cases of excessively high sensory block or related complications were observed in this study.
Although the study was registered in the Clinical Trials Protocol Registration and Results System at a later stage, the study design and protocol were prospectively planned as a randomized controlled trial and conducted accordingly. Importantly, no outcome data analysis influenced by study registration was performed before registration. No retrospective changes were made to the study protocol, eligibility criteria, or outcome definitions following trial initiation. The retrospective registration resulted from an administrative delay during the registration process. This should be considered a study limitation.
We believe that regional blocks administered as part of multimodal analgesia in inguinal hernia surgery performed under spinal anesthesia may contribute to postoperative pain control; however, no statistically significant difference supporting this was found in our study. In particular, there was a nonsignificant trend toward lower VAS scores in the IL/IH group compared with that in the TAP and QLB groups during the postoperative period. Although the total number of patients requiring additional analgesics was lower in all three block groups compared with that in the control group, these findings were not statistically significant. These results suggest that regional blocks can be used as an effective and safe analgesic method in inguinal hernia surgery. However, further multicenter studies with larger sample sizes are needed to confirm these findings and support their broader clinical application. 13
Conclusion
No statistically significant differences were found in the postoperative pain, opioid consumption, or adverse effects between the IL/IH, TAP, QLB, and control groups.
Footnotes
Acknowledgements
We extend our gratitude to the patients and healthcare teams whose contributions enabled the completion of this study. Language editing support was sought from ChatGPT (OpenAI), an artificial intelligence (AI)–based language model, during the manuscript preparation process; the authors reviewed and approved the final version of the manuscript. We also express our gratitude to Emire Bor for her invaluable guidance in statistical analyses throughout the study.
Author contributions
Conceptualization: Meltem Savaş Özdemir and Cavidan Arar
Data curation: Meltem Savaş Özdemir
Formal analysis: Meltem Savaş Özdemir, Ahmet Gültekin, and Cavidan Arar
Investigation: Meltem Savaş Özdemir
Methodology: Ahmet Gültekin and Ayhan Şahin
Supervision: Ayhan Şahin and Cavidan Arar
Validation: Ahmet Gültekin and Ayhan Şahin
Writing – original draft: Meltem Savaş Özdemir, Ahmet Gültekin, and Cavidan Arar
Writing – review & editing: Meltem Savaş Özdemir, and Ahmet Gültekin
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current study are stored in written form by the researchers and are available from the corresponding author upon reasonable request. The data are not publicly available due to patient privacy and ethical restrictions.