
Abstract
Lumbar burst fractures are common high-energy spinal injuries often accompanied by neurological deficits. Although endoscopic percutaneous pedicle screw fixation has been applied in thoracolumbar fractures, it cannot be used for lumbar interbody grafting and anterior–middle column reconstruction. This case report introduces the use of arthroscopic-assisted uni-portal spinal surgery combined with transforaminal lumbar interbody fusion for an L3 burst fracture, enabling endoscopic reduction of spinal canal fracture fragments and concurrent interbody fusion. A male patient in his early 30s with severe back pain after a fall was diagnosed with an L3 burst fracture (AO: A3; Denis: IIB; Thoracolumbar Injury Classification and Severity Score: 2; Lumbar Spine Instability Classification: 6). He received percutaneous pedicle screw fixation at L2–L4 and arthroscopic-assisted uni-portal spinal surgery combined with transforaminal lumbar interbody fusion for decompression, fusion, and anterior–middle column stability reconstruction. At the 6-month follow-up, sagittal alignment and intervertebral disc height were well preserved, and solid spinal fusion with Bridwell grade 1 was achieved.
Keywords
Introduction
Thoracolumbar burst fractures are common high-energy spinal injuries, with approximately 30% of patients presenting with neurological deficits. 1 Early surgical intervention is recommended to restore spinal stability and relieve neural compression. 2 Although conventional open surgeries achieve effective decompression and stabilization, they are associated with considerable surgical trauma and tissue damage. 3 Minimally invasive spine surgery (MIS) has therefore emerged as a preferred alternative, with percutaneous pedicle screw fixation (PPSF) being widely used due to its minimal disruption of paraspinal muscles. However, PPSF alone is often insufficient for severe anterior spinal canal compromise, requiring additional targeted decompression. 4 Techniques such as unilateral biportal endoscopy (UBE) have been adopted for minimally invasive decompression5,6; however, their use in complex fracture reduction remains technically challenging due to instrument interference and limited visualization. To overcome these limitations, Professor Song developed arthroscopy-assisted uni-portal spinal surgery (AUSS),7,8 and preliminary evidence indicates that AUSS combined with transforaminal lumbar interbody fusion (AUSS-TLIF) may enable effective decompression and spinal column reconstruction. 9 This case report describes the application of AUSS-TLIF plus PPSF in an L3 burst fracture, with the aim of achieving reliable spinal canal decompression and anterior–middle column stability reconstruction.
Case presentation
This study was approved by the Ethics Committee of Guangyuan Central Hospital (Approval No. 2026014) and conducted in accordance with the Declaration of Helsinki. The study was reported in accordance with the Case Report (CARE) guidelines. 10 Written informed consent was obtained from the patient for publication of this case report and accompanying images. We have de-identified all patient details. The patient was admitted to Guangyuan Central Hospital, Guangyuan, China, in mid-2024. The patient was a male in his early 30s and presented to our emergency department 4 h after sustaining a 5-m high fall. The patient reported severe lower back pain with limited lumbar mobility and no neurological deficits (American Spinal Injury Association (ASIA) Impairment Scale grade E). Preoperative pain intensity measured via the visual analog scale (VAS) was 8/10, localized to the L3 level without radiation to the lower extremities. Preoperative evaluation included thin-slice computed tomography (CT, 1-mm slice thickness) and 3.0-T magnetic resonance imaging (MRI) to assess bony and soft tissue injuries, with assessment conducted using the Thoracolumbar Injury Classification and Severity Score (TLICS) and Lumbar Spine Instability Classification (LSC) score. X-ray and CT revealed an AO type A3 burst fracture of L3, with anterior–middle column comminution and retropulsed fragments protruding into the spinal canal. The maximum sagittal diameter of the fragment was 5.7 mm, leading to 53% spinal canal stenosis (anteroposterior diameter decreased from 12.0 to 5.6 mm). A complete cortical fracture of the left L3 pedicle was also identified. The TLICS score was 2 points (2 points for fracture type, 0 points for intact neurological function), and the LSC score was 6 points (3 points for comminution + 2 points for pedicle fracture + 1 point for ≥50% stenosis), indicating moderate lumbar instability (Figure 1(a) to (f)). MRI revealed fractures for both the superior and inferior endplates of L3 with adjacent vertebral marrow edema. A focal intervertebral disc herniation (5.7 × 4.3 × 3.2 mm) herniated through the fractured inferior endplate into the vertebral body, forming a Schmorl's node-like lesion. The L2–L3 disc was classified as Pfirrmann grade IV with 50% loss of height (Figure 1(g) and (h)). Based on the Sander Traumatic Intervertebral Disk Lesion (TIDL) classification, the injury was graded as TIDL 3: (a) full-thickness vertebral endplate fracture; (b) marked disc herniation into the vertebral body (>5 mm); and (c) subchondral bone marrow edema.11,12 No spinal cord compression, epidural hematoma, or nerve root impingement was detected on MRI. Given the moderate spinal instability, severe disc-endplate complex injury, and unsatisfactory response to conservative analgesia, surgical intervention was indicated to restore spinal stability and relieve pain.
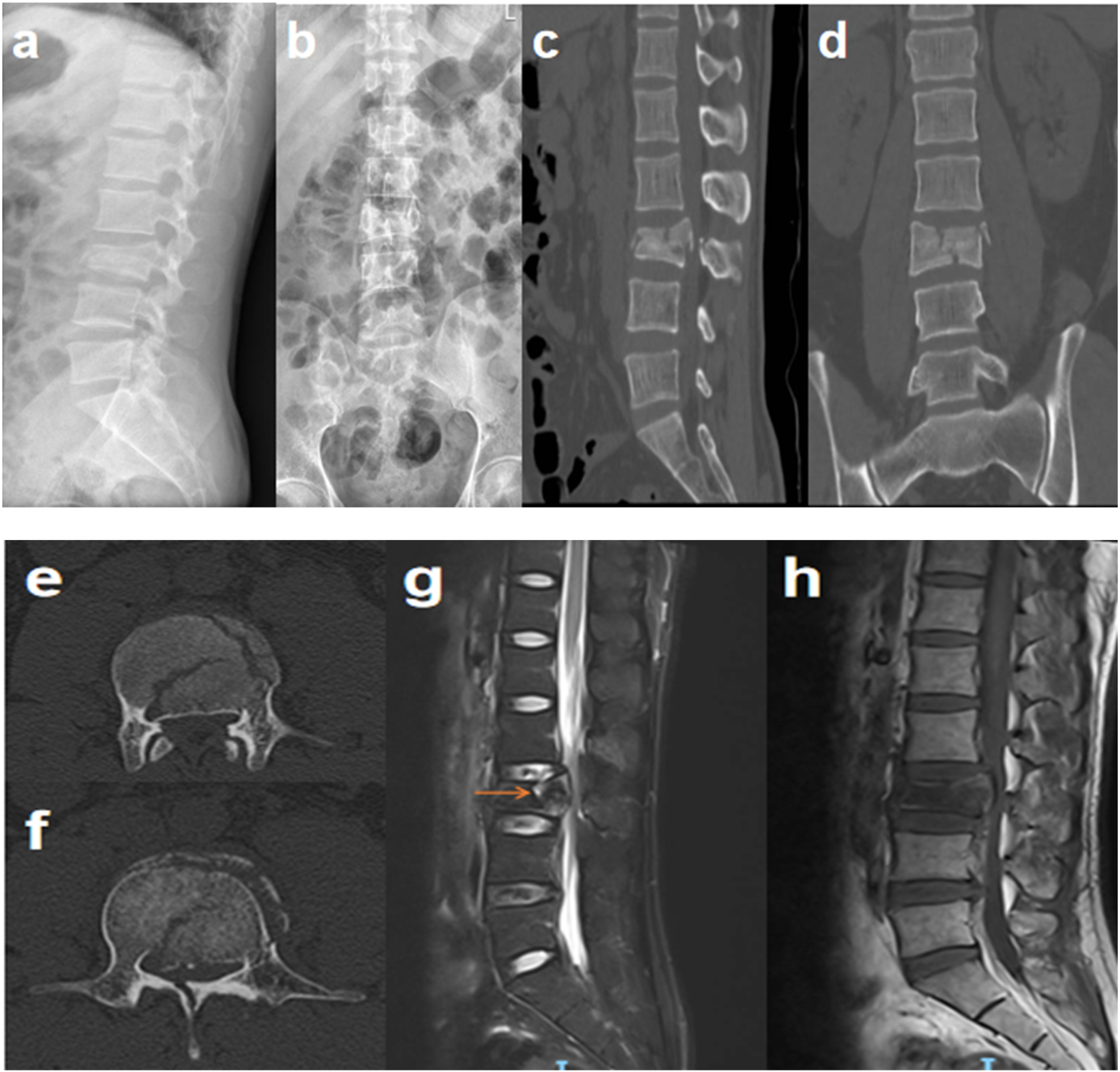
Preoperative imaging examination showed a burst fracture of the L3 vertebral body, with fracture fragments protruding into the spinal canal and a complete fracture of the left pedicle. Arrows indicate disc rupture with intradiscal hemorrhage and herniation of the disc into the vertebral body. Sagittal and axial magnetic resonance imaging at the level of the spinous process fracture clearly revealed vertebral endplate fractures with intervertebral disc herniation into the vertebral body, and the TIDL grade was assigned as 3.
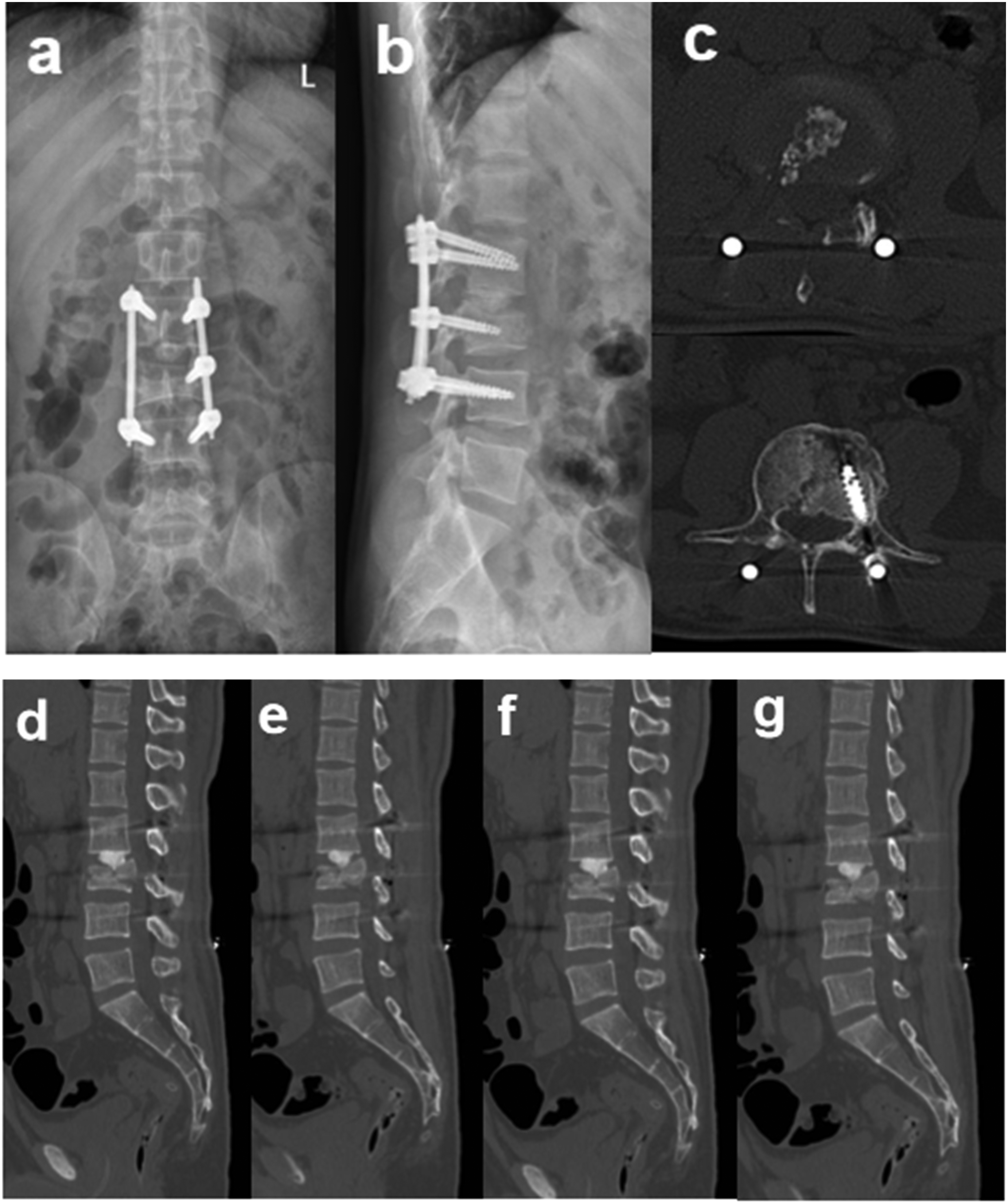
Postoperative intravenous antibiotics (cefazolin, 2.0 g) were administered for 24 h to prevent infection, and oral analgesics (acetaminophen, 500 mg every 6 h for 3 days) were prescribed to relieve pain. The patient was encouraged to perform bed exercises (e.g. ankle pumps, deep breathing) within 24 h after surgery, with early oral feeding and out-of-bed mobilization as tolerated, while avoiding lumbar flexion and rotation. A lumbar brace was required for 3 months when ambulating. Follow-up lumbar radiographs and CT were obtained at 3 days, 3 months, and 6 months postoperatively (Figure 2).
(
Surgical intervention
After induction of general anesthesia, intraoperative neurophysiological monitoring was initiated. The patient was placed in the prone position on a radiolucent operating table with chest and pelvic supports to minimize intra-abdominal pressure and preserve lumbar lordosis. The surgical site was prepared and draped using the standard aseptic technique. Under C-arm fluoroscopic guidance, pedicle screws were inserted bilaterally at L2 and L4 and unilaterally (left side) at L3. A 1.5-cm skin incision was centered at the intersection of the transverse plane of the L2–L3 intervertebral disc and the line connecting the lateral margins of the right L2 and L3 pedicles. The skin, subcutaneous tissue, and lumbodorsal fascia were incised sequentially. A tubular retractor system was gradually dilated under fluoroscopic guidance, and a 30° spinal endoscope was introduced. Soft tissue dissection was performed using a 90° radiofrequency probe (Chengdu Meicuang Medical, 4.0-mm diameter) to expose the inferior margin of the L2 lamina, superior margin of the L3 lamina, bases of the L2 and L3 spinous processes, L2 inferior articular process, and L3 superior articular process. A high-speed drill was used to partially resect the inferior L2 lamina down to the ligamentum flavum insertion. The right L2 inferior and L3 superior articular processes were then removed using an oscillating saw and Kerrison rongeur to achieve unilateral access to the spinal canal. Endoscopic exploration revealed a retropulsed osseous fragment at the L2–L3 level compressing the dural sac.
Under direct endoscopic visualization, an L-shaped bone reduction instrument was employed to gently mobilize and reduce the fragment, which had originated from the superior endplate of L3, back into the vertebral body. Subsequently, blunt dissection was performed to separate the fragment from the dural sac, ensuring that no neural irritation occurred. Intraoperative endoscopy confirmed adequate reduction of the fragment, restoration of dural sac pulsatility, complete neural decompression, and clear delineation of the fracture line. Special precautions were taken during subsequent disc space manipulation to prevent re-displacement of the bone fragment. The L2–L3 intervertebral disc, including the nucleus pulposus and annulus fibrosus, was completely excised, and cartilaginous endplate tissue was curetted to the bleeding bone. Interbody fusion was performed using a composite graft of autologous local bone and allogeneic cancellous bone to restore anterior–middle column stability. Post-graft endoscopic assessment verified correct placement of the posterior graft, absence of residual compression, normal segmental alignment, and robust dural sac pulsation. Following endoscope removal, final C-arm fluoroscopy confirmed accurate pedicle screw placement and construct integrity. Hemostasis was achieved, a closed-suction drain was inserted, and the wound was closed in layers (Figure 3).
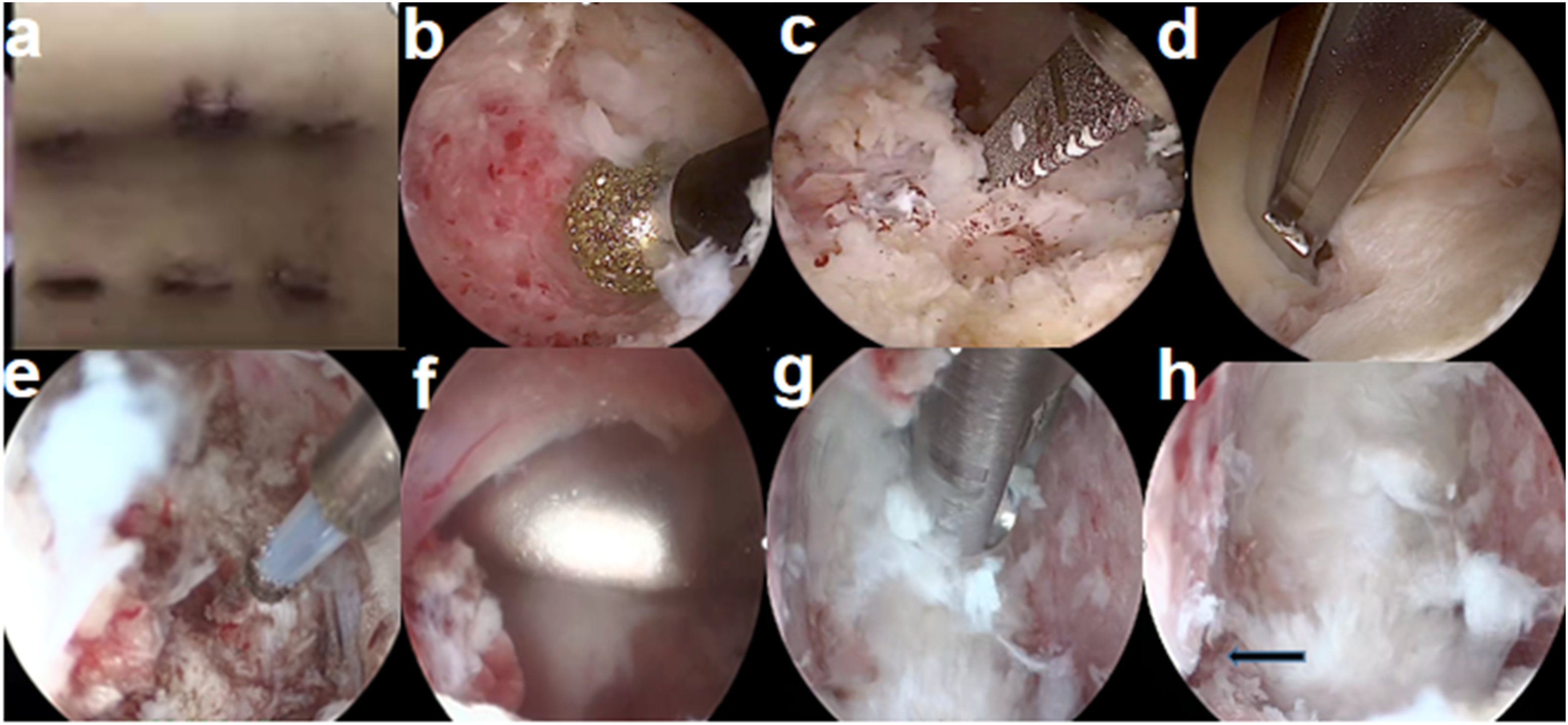
Intraoperative images of arthroscopic-assisted uni-portal spinal surgery combined with transforaminal lumbar interbody fusion and percutaneous pedicle screw fixation are presented. (
Results
Imaging outcomes
The spinal canal stenosis rate improved from 53% preoperatively to 0% at 6 months postoperatively, with the sagittal diameter recovering to 12.0 mm. Interbody fusion reached Bridwell grade 1 at the 6-month follow-up.
Clinical outcomes. The preoperative VAS score of 8/10 decreased to 2/10 at 3 months and 1/10 at 6 months postoperatively. Neurological function remained ASIA grade E throughout the follow-up period.
Surgical parameters. The operative time was 180 min, and intraoperative blood loss was 80 mL. No perioperative complications (e.g. dural tear, nerve injury, or infection) occurred.
Discussion and conclusions
Thoracolumbar fractures can be treated surgically via anterior, posterior, or combined approaches.13,14 Posterior fixation is widely favored because of its minimal invasiveness and technical simplicity and is classified as single-segment, short-segment, or long-segment fixation. 15 Short-segment fixation is reliable and minimally invasive16–18; however, in unstable burst fractures with severe anterior column damage, it may cause stress concentration, leading to loss of reduction and implant failure. Disruption of vertebral endplates and adjacent discs is a major risk factor for correction loss after short-segment posterior fixation. 19 Thus, long-segment posterior fixation (LSPF) or anterior reconstruction is often adopted. Given the greater trauma and longer operation time of LSPF, we used short-segment fixation combined with interbody fusion to reduce the risk of failure.
UBE is widely used for lumbar degenerative diseases such as stenosis and spondylolisthesis.7,8,20 We innovatively combined AUSS with PPSF for lumbar burst fractures requiring decompression and anterior–middle column reconstruction. Both AUSS and PPSF offer the advantages of MIS, including less muscle damage, lower blood loss, less postoperative pain, and faster recovery.21,22 However, PPSF alone cannot achieve sufficient spinal canal decompression, interbody fusion, or anterior–middle column stabilization. We therefore used AUSS to overcome these limitations and expand its application to traumatic spinal fractures. After restoring spinal alignment with PPSF, we performed endoscope-guided laminectomy targeting intracanal fragments. These fragments were directly visualized, localized, and reduced under endoscopy to enlarge the spinal canal, and postoperative CT confirmed sustained improvement.
Few studies have reported minimally invasive decompression and reduction of intravertebral fragments. Huang et al. described a two-stage MIS strategy for an A3-type L1 burst fracture, achieving favorable neurological recovery with delayed transforaminal endoscopic decompression. 23 In contrast, our AUSS-TLIF technique integrates decompression, fragment reduction, and interbody fusion in a single MIS procedure, even for neurologically intact patients. The endoscopic view allows precise visualization of the ventral dura and targeted fragment reduction, with laminectomy adjusted in real time according to the lesion. Notably, AUSS uses a single portal for both the endoscope and instruments, which can move coaxially or independently to improve intraoperative flexibility. It also enables direct deep hemostasis within the paraspinal muscles, which is difficult to achieve with UBE and effectively reduces occult blood loss. Direct visualization ensures safe handling of the dural sac and preserves endplate integrity during disc preparation. Bilateral real-time reduction avoids the “pulley effect” and lowers the risk of secondary neural injury. The endoscopic working channel provides instrument maneuverability similar to open surgery while retaining the core benefits of MIS.
This study has several limitations. First, it is a single-case report, and findings require validation in larger studies. Second, the results presented herein represent short-term observations; the long-term efficacy requires further follow-up beyond 12 months. Third, no direct comparison with open TLIF or UBE-TLIF was performed, warranting future comparative trials.
Conclusions
AUSS combined with PPSF is a feasible minimally invasive option for lumbar burst fractures requiring spinal canal decompression and interbody fusion to restore anterior–middle column stability. Although AUSS is well established for degenerative spinal disorders such as low-grade spondylolisthesis, its application in traumatic burst fractures remains novel. Further prospective studies with larger samples and longer follow-up are warranted to verify the long-term efficacy and safety of this technique. These results represent short-term observations, and follow-up is planned to be extended to 12 months to evaluate long-term fusion stability.
Footnotes
Acknowledgements
We sincerely thank the patient for granting written informed consent and supporting this case report. We also gratefully acknowledge the guidance and assistance of all colleagues involved in this study.
Author contributions
Zhilin Li conceived and oversaw the study. Jing Zhang conducted the majority of the data collection and analysis. Yin He provided assistance in data collection and analysis. Jing Zhang prepared the initial draft of the manuscript. Zhilin Li reviewed and revised the manuscript. All authors contributed to the finalization of this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the results of this study are available upon request from Guangyuan Central Hospital. However, the accessibility of these data is restricted due to their use under specific permissions granted for this study, and they are not publicly accessible. With a justified and formal request to Guangyuan Central Hospital, the data may be obtained directly from the corresponding authors.