
Abstract
Objective
Thyroid disorders are among the most common endocrine conditions worldwide. However, in the Republic of North Macedonia, national level data on their prevalence and demographic distribution are lacking. This study aimed to determine the prevalence and demographic patterns of nonmalignant thyroid disorders using data from the National eHealth System.
Methods
This retrospective, population-based
Results
The overall national prevalence of nonmalignant thyroid disorders was 14.68%. Prevalence was higher in women (24.36%) than in men (4.85%) and increased with age, with the highest prevalence of 21.9% among those aged 60–79 years. Women had significantly higher odds of thyroid disorders than men (odds ratio: 6.32; 95% confidence interval: 6.25–6.38; p < 0.0001). Prevalence was higher in urban than in rural areas (17.1% vs. 10.9%). Hypothyroidism (E03) was the most common disorder, affecting 9.7% of the population.
Conclusion
This is the first national level study to examine the epidemiology of nonmalignant thyroid disorders in the Republic of North Macedonia. The findings reveal marked variations in prevalence by sex, age, and place of residence, underscoring the need for targeted public health strategies and further investigation.
Keywords
Introduction
Thyroid disorders are among the most prevalent endocrine diseases globally, affecting over 200 million people. 1 Their growing burden poses significant public health challenges.1–3 According to the World Health Organization (WHO), women are up to 10 times more likely to develop hypothyroidism than men, 2 and Hashimoto's thyroiditis (HT) affects 17.5% of women compared with 6.0% of men. 3 The prevalence of overt hypothyroidism varies geographically, ranging from 0.2% to 5.3% in Europe and from 0.3% to 3.7% in the United States. 3
Iodine deficiency and autoimmune thyroid disorders, particularly HT, are the leading global causes of hypothyroidism. 4 Approximately one-third of the world's population resides in iodine-deficient areas. Genetic predisposition accounts for approximately 70% of the risk of autoimmune thyroid disease, whereas environmental factors such as radiation exposure and iodine intake also contribute substantially. 5 Lifestyle factors such as alcohol consumption and smoking may further raise disease risk. 6 Recent evidence has suggested a link between the coronavirus disease 2019 (COVID-19) pandemic and an increased incidence of autoimmune thyroid disease. 7
The Republic of North Macedonia has historically struggled with iodine deficiency. In 1953, more than 20% of the country’s population, comprising approximately 200,000 individuals, was diagnosed with goiter. 8 In response, a national salt iodization program was initiated in 1956, using potassium iodide at a concentration of 10 mg/kg of salt; the program was modified to use potassium iodate at a concentration of 20–30 mg/kg of salt in 1999. This resulted in the achievement of iodine sufficiency in the nation’s population by 2003.8,9 The mandatory iodization of food grade salt remains a part of their national policy. 9 However, a 2024 report by the WHO and the Iodine Global Network warns of a resurgence of iodine deficiency in parts of Europe, including the Balkans. 10 This trend is attributed to changing dietary habits, including declining dairy consumption and the growing use of non–iodized salt in food preparation. 10
Despite these concerns, no national level data have been published on the prevalence or demographic patterns of nonmalignant thyroid disorders in the Republic of North Macedonia. This study aimed to address this gap by analyzing data from the National eHealth System (NeHS). 11 The objective was to examine the prevalence patterns of nonmalignant thyroid disorders stratified by age, sex, and place of residence, and thereby support early detection, improve thyroid disorder management, and inform targeted public health strategies.
Materials and methods
This retrospective, population-based, cross-sectional study analyzed the prevalence of nonmalignant thyroid disorders in the Republic of North Macedonia using data from the NeHS. 11 The NeHS is a centralized national digital health platform established in 2013 that integrates electronic health records across primary, secondary, and tertiary healthcare institutions. As the official nationwide eHealth infrastructure, it enables the collection of routinely recorded, anonymized health data and provides a comprehensive source for population-level epidemiological research.
The dataset includes information of all eligible unique individuals with an active thyroid disorder diagnosis recorded in the NeHS as of 31 October 2024. Following data extraction, the analytical dataset was restricted to individuals recorded as alive at the time of analysis. All eligible individuals were included without sampling. De-identified and anonymized data were provided by the Directorate for eHealth within the Ministry of Health. The study protocol was reviewed and approved by the Ethics Committee of the Faculty of Medical Sciences, Goce Delčev University, Štip, North Macedonia (Approval No. 2005–172/5, dated 25 June 2025). No personal identifiers were accessible to the researchers; each individual was represented by a unique anonymized identifier. The study was conducted in accordance with the Declaration of Helsinki of 1975, as revised in 2024. 12 The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies. 13
Thyroid disorders were identified using the International Classification of Diseases, 10th Revision (ICD-10) codes, specifically E00–E07, which encompass congenital iodine deficiency disorders, hypothyroidism, thyrotoxicosis, thyroiditis, and other nonmalignant thyroid disorders (excluding thyroid malignancies). 14 Individuals with multiple diagnoses were classified under more than one ICD-10 category.
The population was stratified by sex (female or male), place of residence (urban or rural), and age group (<20, 20–39, 40–59, 60–79, and ≥80 years). Corresponding population denominators for each stratum were obtained from the State Statistical Office (SSO) of the Republic of North Macedonia, based on the official Census of Population, Households and Dwellings in the Republic of North Macedonia, 2021, conducted from 5 to 30 September 2021. 15
Data analyses were performed using the Statistical Package for Social Sciences (SPSS) software, IBM SPSS Statistics for Windows (version 25.0, IBM Corp., Armonk, NY, USA). 16 Descriptive statistics were used to summarize the demographic characteristics of individuals diagnosed with nonmalignant thyroid disorders. Frequencies and cross-tabulations were used to examine the distribution of diagnosed cases across sex, age group, and place of residence. Prevalence was calculated as the number of diagnosed individuals divided by the corresponding total population in each subgroup. Differences in the prevalence rates between women and men within each subgroup were assessed using the chi-square test. Univariable binary logistic regression was performed to estimate odds ratios (ORs), 95% confidence intervals (CIs), and p-values. Thyroid disorder diagnosis status was defined as the dependent variable. Models were fitted using grouped binomial data, with non-cases calculated as the total population minus the number of diagnosed cases. Frequency weights were applied to represent the number of individuals in each outcome category. Separate univariable models were fitted for sex, place of residence, and age group, with male sex, rural residence, and the <20-years age group used as reference categories. A two-sided p-value <0.05 was considered statistically significant.
Results
In total, 269,690 individuals were diagnosed with nonmalignant thyroid disorders. Based on the most recent data from the SSO, the national population was 1,836,713; therefore, the overall national prevalence of thyroid disorders was 14.68% (Table 1).
Prevalence of nonmalignant thyroid disorders, stratified by age group, sex, and place of residence.
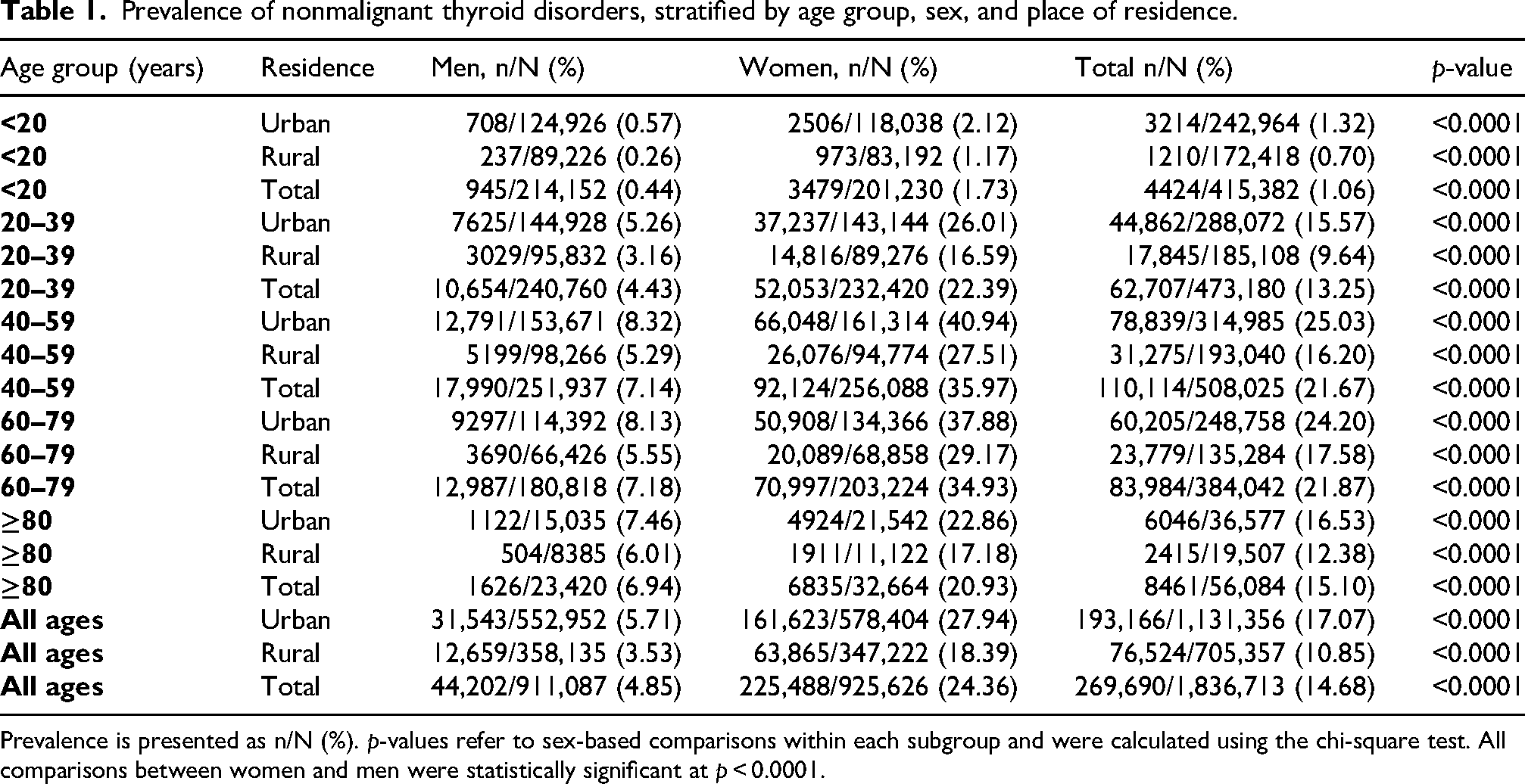
Prevalence is presented as n/N (%). p-values refer to sex-based comparisons within each subgroup and were calculated using the chi-square test. All comparisons between women and men were statistically significant at p < 0.0001.
The most prominent finding was the marked sex-based difference in prevalence. Women had a substantially higher prevalence of diagnosed nonmalignant thyroid disorders than men at the national level, and this pattern was consistent across all age groups and in both urban and rural settings. Figure 1 illustrates the sex-specific prevalence pattern across age groups.
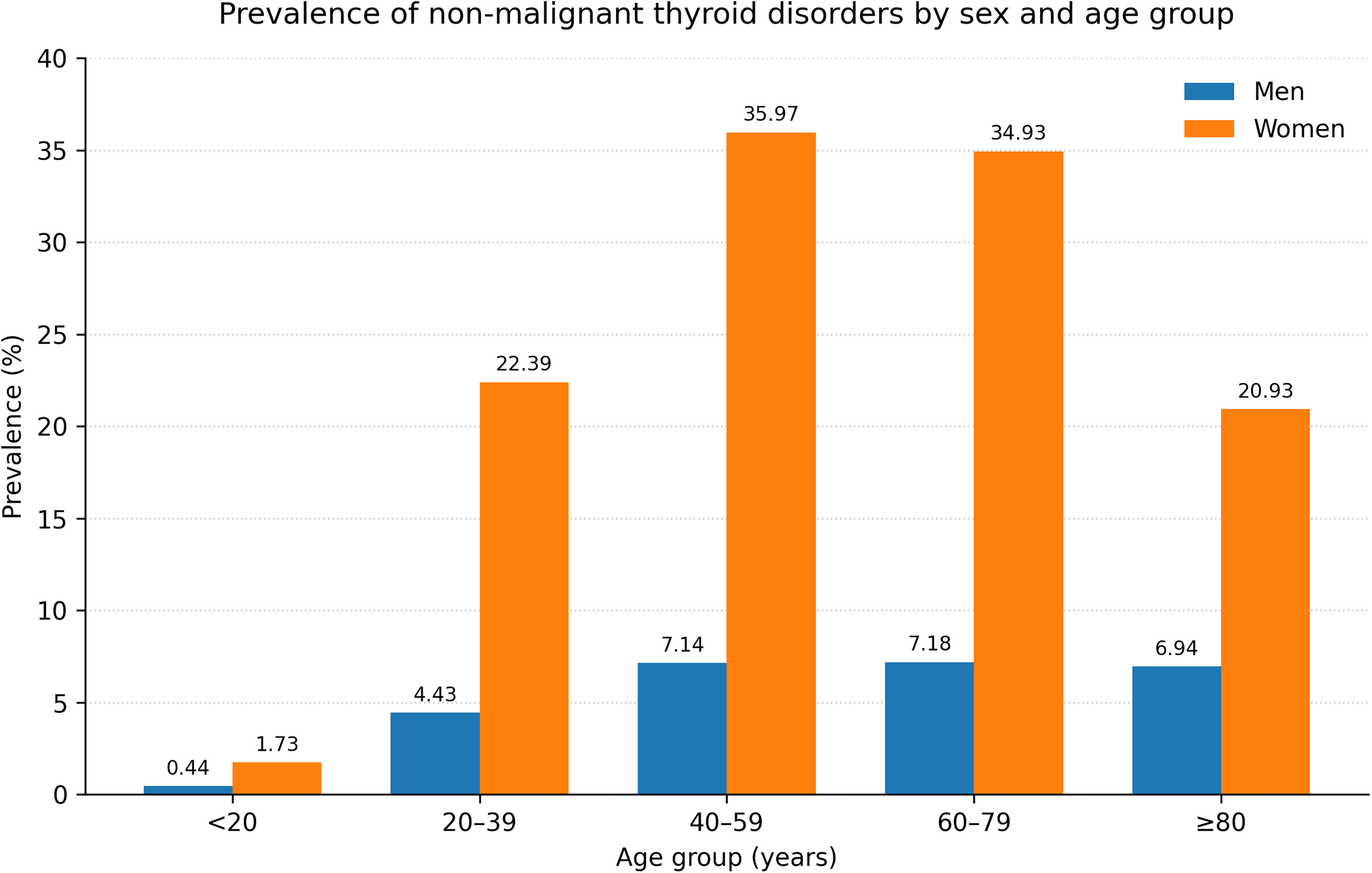
Prevalence of nonmalignant thyroid disorders, stratified by sex and age group.
Table 1 presents the number of diagnosed cases, corresponding population denominators, and prevalence estimates stratified by age group, sex, and place of residence. Overall, women accounted for most diagnosed cases and had a substantially higher prevalence than men (24.36% vs. 4.85%). A sex-based difference was observed in every age group and in both urban and rural populations. Prevalence increased with age, reaching the highest levels among individuals aged 60–79 years, followed closely by those aged 40–59 years.
Univariable binary logistic regression was performed to estimate the magnitude of the sex-based differences in the prevalence of diagnosed nonmalignant thyroid disorders. At the national level, women had more than sixfold higher odds of diagnosis than men (OR: 6.32; 95% CI: 6.25–6.38; p < 0.0001). This association remained statistically significant across all age groups and both urban and rural settings. The highest female-to-male difference was observed in the 40–59 years age group, followed by that in the 60–79 and 20–39 years age groups. The ORs for thyroid disorder prevalence in women compared with those in men, stratified by age group and place of residence, are presented in Table 2.
Univariable logistic regression analysis of thyroid disorder prevalence in women compared with men, stratified by age group and place of residence.
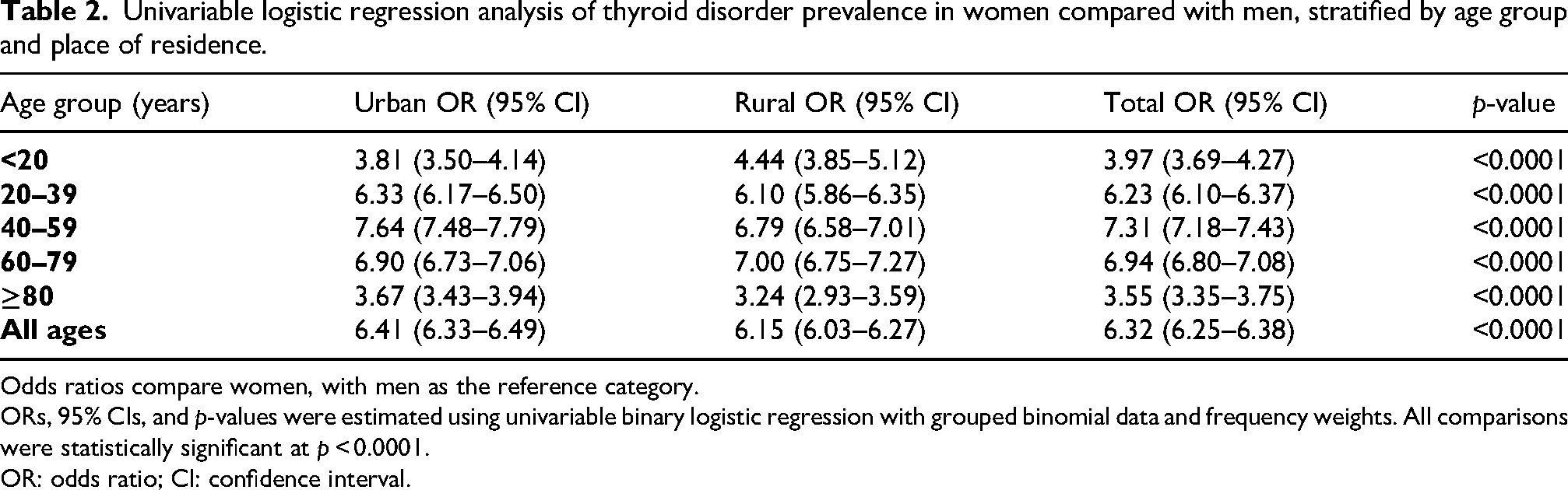
Odds ratios compare women, with men as the reference category.
ORs, 95% CIs, and p-values were estimated using univariable binary logistic regression with grouped binomial data and frequency weights. All comparisons were statistically significant at p < 0.0001.
OR: odds ratio; CI: confidence interval.
To further explore age-related patterns, univariable binary logistic regression was performed to compare each age group, with individuals aged <20 years serving as the reference category, stratified by sex. Among women, the odds increased sharply with age, peaking in the 60–79 years group (rural OR: 34.81; 95% CI: 32.61–37.16; urban: OR 28.12; 95% CI: 26.99–29.30). A similar trend was observed among men, with the highest odds in the 60–79 and ≥80 years groups compared with that in the <20 years age group (OR up to 24.01; 95% CI: 20.54–28.07). These findings underscore a strong, age-related increase in the prevalence of nonmalignant thyroid disorders among both sexes.
Table 3 presents the diagnosis-based distribution of nonmalignant thyroid disorders by ICD-10 category. Some individuals had more than one thyroid diagnosis; therefore, the total number of diagnoses may exceed the number of unique individuals.
Diagnosis-based distribution of nonmalignant thyroid disorders, according to ICD-10 category.
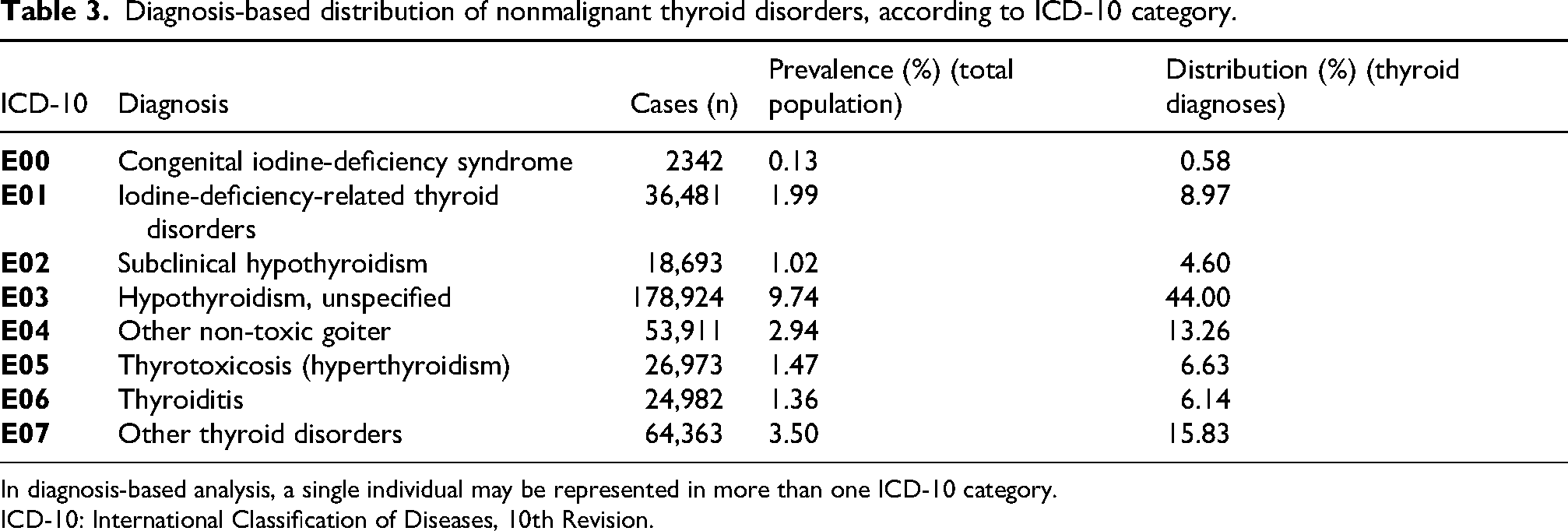
In diagnosis-based analysis, a single individual may be represented in more than one ICD-10 category.
ICD-10: International Classification of Diseases, 10th Revision.
Hypothyroidism (E03) was the most frequently recorded diagnosis, followed by other thyroid disorders (E07) and non-toxic goiter (E04). Together, these categories accounted for the largest share of the diagnosis-based burden of nonmalignant thyroid disorders in the national registry. Less commonly reported categories included iodine-deficiency-related disorders, thyrotoxicosis, thyroiditis, subclinical hypothyroidism, and congenital iodine-deficiency syndrome.
Discussion
This study presents the first national level analysis of nonmalignant thyroid disorders in the Republic of North Macedonia using data from the NeHS, demonstrating a substantial burden on public health with an overall prevalence of 14.68%. As an official centralized national platform, the NeHS provides a nationwide real-world representation of diagnosed thyroid disorders in routine clinical practice. 11 These findings likely reflect a complex interaction of historical iodine deficiency, genetic susceptibility, and environmental influences.
Hypothyroidism (ICD-10 E03) was the most prevalent thyroid condition, affecting 9.74% of the population. This is consistent with global patterns, where hypothyroidism is commonly associated with iodine imbalance and autoimmune mechanisms. A global meta-analysis estimated a 7.5% prevalence of HT, with higher rates observed in low- and middle-income countries. 3 Regional studies from Balkan countries have reported prevalence rates ranging from approximately 3%–9% for hypothyroidism and a notable presence of thyroid autoimmunity and subclinical dysfunction.17–21 However, directly comparable national level data from neighboring countries remain limited. These observations are also consistent with broader European data demonstrating substantial variation in thyroid disorder prevalence across populations. 22 In contrast, lower prevalence has been reported in the United States (5.05% between 2015 and 2018), highlighting geographic variability and potential differences in screening, iodine status, and population structure. 23
The relatively high proportion of diagnoses classified as other thyroid disorders (ICD-10 code E07) should be interpreted cautiously. This category encompasses a heterogeneous group of thyroid conditions not classified elsewhere and may include less specific, mixed, or evolving thyroid diagnoses recorded in routine clinical practice. Therefore, in the context of a large national registry, the frequency of E07 diagnoses is more indicative of real-world clinical coding than a single distinct pathological entity.
Despite achieving iodine sufficiency by 2003 according to the WHO criteria, 8 regional disparities in thyroid-related indicators persist. Variations in neonatal screening outcomes suggest heterogeneity in thyroid-related outcomes across different areas. 24 These findings indicate that the historical burden of iodine deficiency continues to influence current epidemiological patterns. In addition, inconsistent use of iodized salt and changing dietary habits may contribute to mild iodine deficiency in some populations, which remains an important determinant of thyroid disorder prevalence regionally and globally.4,9,25 The persistence of iodine-deficiency-related codes may also reflect residual coding practices or subclinical variations despite current iodine sufficiency.
Pronounced age- and sex-related differences were observed. Prevalence increased significantly with age, peaking in the 40–59 and 60–79 age groups, consistent with established epidemiological trends. 26 The low prevalence among individuals aged <20 years may reflect the long-term impact of iodine supplementation and newborn screening programs. Women accounted for most of the diagnosed cases, supporting well-established evidence of increased susceptibility related to hormonal and autoimmune mechanisms. 27 The peak prevalence among women in the 40–59 age group corresponds to the typical age of onset for autoimmune thyroid disorders.
Urban–rural disparities further highlight potential inequalities in healthcare access. Higher prevalence in urban populations likely reflects greater availability of diagnostic services and screening, whereas underdiagnosis in rural areas may be driven by structural barriers, including healthcare accessibility and resource distribution.28,29 Thus, this pattern may reflect differences in detection and healthcare access rather than true differences in the underlying occurrence of thyroid disorders.
Congenital hypothyroidism (CH) remains an important component of thyroid disorder surveillance in North Macedonia. National newborn screening data indicate an incidence of approximately 1 in 1976 live births. 30 Continued evaluation of screening performance, early diagnosis, treatment initiation, and long-term follow-up remain important for reducing the occurrence of preventable neurodevelopmental consequences and improving thyroid-related outcomes.30,31
Although this study focused on nonmalignant thyroid disorders, National Cancer Registry data demonstrate overlapping demographic patterns with thyroid carcinoma, particularly among women and older individuals. 32 This observation suggests shared population-level risk profiles and supports the need for further investigation of common etiological pathways.
These findings have important public health implications. Strengthening neonatal screening programs through continued evaluation and alignment with best practices remains essential.30,31 The implementation of evidence-based clinical guidelines may improve diagnostic accuracy and long-term management.33,34 In parallel, public health strategies focused on maintaining adequate iodine intake and increasing awareness are critical, particularly in the context of changing dietary behaviors and the potential re-emergence of iodine deficiency.10,25,35 Given the historical burden of iodine deficiency and the possibility of changing dietary iodine intake, updated national screening of iodine status should be considered for more accurate determination of the contribution of current iodine nutrition to thyroid disorder prevalence. Taken together, these findings position thyroid disorders as a significant and potentially under-recognized public health concern in North Macedonia, warranting sustained surveillance and targeted intervention strategies.
Limitations
This study is based on diagnosed cases recorded in the NeHS and may have underestimated the true prevalence of thyroid disorders by excluding undiagnosed or subclinical conditions. Conversely, the overall prevalence of 14.68% may be an overestimation to some extent because 3.50% of the population was classified under ICD-10 code E07, a heterogeneous category that includes other and unspecified thyroid disorders. This category may include mixed, evolving, or less specific clinical diagnoses recorded in routine practice and should therefore be interpreted cautiously. The absence of biochemical and immunological data limited the assessment of disease severity and etiology. The cross-sectional study design precludes causal inference. In addition, regional differences in healthcare access may have influenced diagnosis rates, particularly in rural areas. The use of administrative coding data may also introduce misclassification bias inherent to routine clinical practice. Despite these limitations, the use of comprehensive nationwide data provides robust and representative estimates of diagnosed thyroid disorder prevalence.
Conclusion
This study underscores the significant public health burden of nonmalignant thyroid disorders in the Republic of North Macedonia, offering the first epidemiological insight into their prevalence, with data derived from the NeHS. The findings may inform future public health strategies, including targeted interventions and improved screening, particularly among middle-aged women, to support improved clinical management of thyroid disorders and overall health outcomes in the country.
Footnotes
Acknowledgments
The authors thank the Directorate for eHealth for providing anonymized data and administrative support.
ORCID iDs
Ethical approval
The study was reviewed and approved by the Ethics Committee of the Faculty of Medical Sciences, Goce Delčev University, Štip, North Macedonia (Approval No. 2005–172/5). All data were anonymized prior to analysis.
Consent to participate
This retrospective study used secondary anonymized registry data; therefore, individual informed consent was not required.
Consent for publication
No identifiable individual data are included; therefore, consent for publication was not necessary.
Author contributions
Ana Talevska led the study conception and design, performed data acquisition and statistical analysis, interpreted the findings, and drafted the manuscript. Ivica Smokovski performed clinical supervision, provided endocrinology expertise, and reviewed the manuscript. Zhaklina Chagoroska supported data acquisition and contributed their expertise on National eHealth System (NeHS). Emilija Antova contributed to result interpretation and manuscript review. Lisa Zottarelli provided intellectual input and critically reviewed the manuscript. Colton Daniels and Larisa Ozeryansky contributed to results interpretation and manuscript refinement. Thankam Sunil contributed to the study design, results interpretation, and substantial revision of the manuscript. All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data that support the findings of this study are available from the Directorate for eHealth within the Ministry of Health of the Republic of North Macedonia but are not publicly available due to privacy regulations. Data may be available from the authors upon reasonable request and with permission of the relevant authorities.