
Abstract
Objective
To assess the prevalence of post-traumatic stress disorder and its associated risk factors among survivors of the 2023 earthquake in Syria and Turkey.
Methods
A cross-sectional study was conducted between February and May 2024, 1 year after the earthquake, in both countries. A total of 1568 participants were included. Data were collected through an online questionnaire and face-to-face interviews. Post-traumatic stress disorder prevalence was assessed using the PTSD Checklist–Civilian Version, and social support was evaluated using the Oslo Social Support Scale.
Results
Among participants, 388 (24.7%) were classified as having probable post-traumatic stress disorder. Significant risk factors included female sex (odds ratio: 1.670, p < 0.001), poor social support (odds ratio: 2.051, p < 0.001), and pre-earthquake displacement (odds ratio: 1.726, p < 0.001). Post-trauma factors associated with post-traumatic stress disorder included experiencing a nervous breakdown (odds ratio: 3.185, p < 0.001), sustaining an injury (odds ratio: 2.075, p = 0.001), changing residence because of earthquake (odds ratio: 1.628, p = 0.004), and experiencing suicidal thoughts (odds ratio: 2.159, p < 0.001). Higher education and receiving support after the earthquake were associated with lower post-traumatic stress disorder prevalence (p = 0.004 and p = 0.002, respectively).
Conclusion
The present study found a post-traumatic stress disorder prevalence of 24.7%, 1 year after the earthquake. Female sex, poor social support, pre-earthquake displacement, and post-trauma factors including nervous breakdown, injury, residence change, and suicidal thoughts were significantly associated with post-traumatic stress disorder.
Introduction
On 6 February 2023, southeastern Turkey and northern Syria were struck by two powerful earthquakes registering magnitudes of 7.8 and 7.6 on the Richter scale, making them the most significant earthquakes in the region since 1939. 1 The disaster resulted in more than 56,683 deaths and 118,404 injuries, with approximately 18 million people requiring urgent humanitarian assistance, including food, clean water, and shelter. 1
In Syria, the earthquakes exacerbated the ongoing effects of 12 years of civil conflict, causing extensive damage to residential buildings and already fragile public infrastructure. The disaster affected 38 districts and 174 sub-districts across 6 of the country's 14 governorates, including Aleppo, Hama, Idlib, Latakia, Raqqah, and Tartous. 2 In Turkey, significant damage and disruption occurred in the provinces of Kahramanmaraş (including Pazarcık and Elbistan), Hatay, Gaziantep, Malatya, Diyarbakır, Kilis, Şanlıurfa, Adıyaman, Osmaniye, Adana, and Elâziğ. 3 Consequently, a state of emergency was declared in these regions to address the crisis.
Natural disasters, such as earthquakes, can result in significant human and economic losses as well as severe mental health challenges. Survivors may develop psychological disorders, including post-traumatic stress disorder (PTSD), anxiety, and depression. 4 These mental health impacts can be both short-term and long-term, potentially contributing to substantial morbidity and mortality. 5 PTSD is recognized as the most prevalent psychological response among earthquake survivors. 6
PTSD is a complex psychiatric disorder that develops following exposure to a traumatic event. 7 According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), criteria, a PTSD diagnosis requires exposure to life-threatening traumatic event that markedly differs from normal daily life. 7 Symptoms are categorized into four clusters: (a) intrusive symptoms (e.g. flashbacks); (b) avoidance of trauma-related stimuli; (c) negative alterations in cognition and mood; and (d) marked changes in arousal and reactivity. These symptoms must persist for at least 1 month and significantly impair daily functioning. 8
One in four earthquake survivors are diagnosed with PTSD. 9 Even a decade after the event, survivors can still suffer from severe PTSD. 10 A meta-analysis reported that the prevalence of PTSD following an earthquake ranged from 4.10% to 67.7% among adults. 6 Following the Turkey–Syria earthquakes, the prevalence of probable PTSD in Turkey was reported to be 51.4%, 11 with another study indicating a similar prevalence of 47.7%. 12 In Syria, the prevalence of PTSD was higher, with 57.9% in severely affected regions and 55.4% in moderately affected regions. 13 Another study in Turkey reported a prevalence of probable PTSD of 54.1%. 14 The risk factors for developing PTSD can be grouped into three categories: pre-trauma, trauma-related, and post-trauma factors. 15 Common risk factors include female sex, single marital status, low income, low educational level, and high levels of exposure to the earthquake (e.g. injury, bereavement, witnessing injury or death, or severe housing damage). Poor social support is also a significant contributor to PTSD development.6,9–13,16
Additional potential risk factors such as pre-existing mental illness, family history of mental illness, loss of income due to the earthquake, suicidal thoughts after the event, and limited access to mental health services in affected areas warrant further investigation. These factors may also play a role in PTSD development and require evaluation, particularly in areas where mental health services are limited. 17
In this study, PTSD is investigated in relation to three groups of variables: pre-trauma factors (such as sex, education, and prior mental health history), trauma-related exposures (such as injury, bereavement, and witnessing traumatic events), and post-trauma factors (including social support, economic impact, and displacement after the earthquake). These variables are interconnected, as pre-existing vulnerabilities may influence the degree of trauma exposure and the availability of post-trauma resources, ultimately affecting the risk of developing PTSD.
Despite the growing body of research, there is limited evidence assessing PTSD 1 year after the 2023 Turkey–Syria earthquake using a combined sample from both countries with a comprehensive evaluation of these factors. Addressing this gap is important, as understanding how these variables interact may help identify individuals at higher risk and inform targeted mental health responses in disaster-affected and conflict-affected populations.
To the best of our knowledge, this is the first study to examine the prevalence of probable PTSD following the 2023 earthquakes in Syria and Turkey using a representative sample from both countries. Additionally, we have identified the associated risk factors for developing PTSD among survivors of the 2023 Turkey–Syria earthquake.
Methods
Participants and sampling
A multinational cross-sectional study design was used to assess the prevalence of PTSD and its associated risk factors among earthquake survivors in Syria and Turkey, based on retrospective self-reported data collected 1 year after the event. The study was conducted between 1 February 2024 and 7 May 2024, using a convenience sampling approach. The questionnaire was developed after a comprehensive literature review using keywords as “Syria,” “Turkey,” “earthquake,” “2023 Turkey–Syria earthquakes,” and “post-traumatic distress disorder.” The questionnaire was piloted with 20 volunteers to evaluate clarity, accessibility, and relevance; these volunteers were not included in the final sample to prevent bias.
The questionnaire was administered via Google Forms and disseminated by the data collection team through social media platforms, including Facebook, Telegram, WhatsApp, and Instagram. Face-to-face interviews were also conducted in hospitals and public places. Online interactions allowed participants to comment on the questionnaire link, increasing its visibility. The data collection team operated across the earthquake-affected regions in both Syria and Turkey.
Eligibility criteria included the following: (a) residing in the earthquake-affected areas of Syria and Turkey at the time of the event; (b) age ≥18 years; (c) agreeing to participate; (d) completing the questionnaire; and (d) providing written informed consent. Those who did not meet these criteria were excluded. Incomplete or contradictory responses were removed during data validation. The questionnaire took approximately 5 min to complete. Participants were provided with a brief study description before obtaining written informed consent. All responses were kept confidential and used solely for scientific purposes. Of the 1577 initial responses, 1568 participants met the inclusion criteria and were included in the final analysis.
At the end of the questionnaire, participants were provided with a brief definition of PTSD and its symptoms. They were advised to seek medical assistance if they, their family, or friends experienced these symptoms. Additionally, information on hotlines for urgent medical advice in cases of suicidal thoughts or other urgent mental health issues was provided. Participants were assured that these services are confidential and free of charge.
Study tool. The questionnaire consisted of five sections. The first section captured the sociodemographic information, including the provinces and regions where participants were located during the earthquakes in Syria (Aleppo, Lattakia, Hama, Tartus, and Idlib) and Turkey (Adana, Diyarbakir, Gaziantep, Kahramanmaraş, Malatya, Şanliurfa, Adiyaman, Elâziğ, Hatay, Kilis, and Osmaniye). These regions were selected because they were the most severely affected by the earthquakes.18,19 Additional details included sex, age, marital status, education level, employment status, refugee or internally displaced status prior to the earthquakes, smoking history, presence of chronic diseases, medical history of mental illness, family history of mental illness, and living arrangements (whether participants lived alone or with someone else during the event).
The second section of the questionnaire assessed social support using the Oslo Social Support Scale (OSS-3). Scores range from 3 to 14, with higher scores indicating stronger social support. 20 The scores are categorized as follows: 3–8 (poor support), 9–11 (moderate support), and 12–14 (strong support). 21 The Arabic version of the subscale has been validated in a previous study and demonstrated good internal reliability, with a Cronbach's alpha coefficient of 0.925. 22 The Turkish version was translated and reviewed independently by a professional translator and a native speaker researcher, with discrepancies resolved through discussion.
The third section of the questionnaire assessed earthquake exposure through nine questions about experiences such as being trapped under rubble, sustaining injuries, witnessing fatalities, losing family members or friends, having family members or friends injured, suffering house damage, or having a nervous breakdown immediately following the earthquake. Earthquake exposure was classified as “Exposed” if participants responded “Yes” to any of these questions.
The fourth section assessed the prevalence of PTSD using the PTSD Checklist–Civilian Version (PCL-C). This checklist includes 17 items that align with DSM-IV diagnostic criteria: re-experiencing, avoidance/numbing, and hyperarousal. To ensure that the questions reflected earthquake-related symptoms, the phrase “stressful experience” was modified to “earthquake” in all relevant items. Participants rated their symptoms on a scale from 1 (not at all) to 5 (extremely) as related to the earthquake. Both the Arabic and Turkish versions of the PCL-C have been validated, with Cronbach's alpha coefficients of 0.89 and 0.922, respectively.23,24 In this study, Cronbach's alpha for the PCL-C was 0.95. A cutoff score of 50 was used to determine probable earthquake-related PTSD.25,26
The fifth part of the questionnaire assessed the earthquake's impact on various life aspects, including job loss, property damage, economic or living condition changes, having to flee one's home or place of residence due to the earthquake, and temporary living arrangements. It also covered health impacts such as permanent injuries, mental health issues (including suicidal thoughts), and consultations with mental health professionals. The questionnaire, available in English, Turkish, and Arabic, can be found in the supplementary files.
Statistical analysis
Data were collected via Google Forms and analyzed using the Statistical Package for the Social Sciences (SPSS), version 25. Descriptive statistics were used to summarize the sociodemographic characteristics of the study participants. Chi-squared and Fisher's exact tests were used to examine associations between categorical variables and probable PTSD. Pre-trauma and post-trauma factors that were statistically significant with probable PTSD in the chi-squared test were further analyzed using multivariable logistic regression to assess their impact on the likelihood of developing PTSD. All relevant factors were entered into the model simultaneously. PTSD prevalence was determined using a cutoff score of 50. P-values ≤0.05 were considered statistically significant.
Results
Distribution of study population between Syria and Turkey
Of the total 1568 study participants, 908 (58.0%) were in Turkey during the earthquake, whereas 660 (42.0%) resided in Syria. In Turkey, the largest group was in Hatay, with 243 participants (27.0%), followed by Adiyaman with 156 (17.0%), Gaziantep with 109 (12.0%), and Kahramanmaraş with 105 (12.0%) (Figure 1). In Syria, Aleppo accounted for 220 participants (33.0%), Lattakia for 207 (32.0%), and Tartus for 127 (19.0%) (Figure 1).
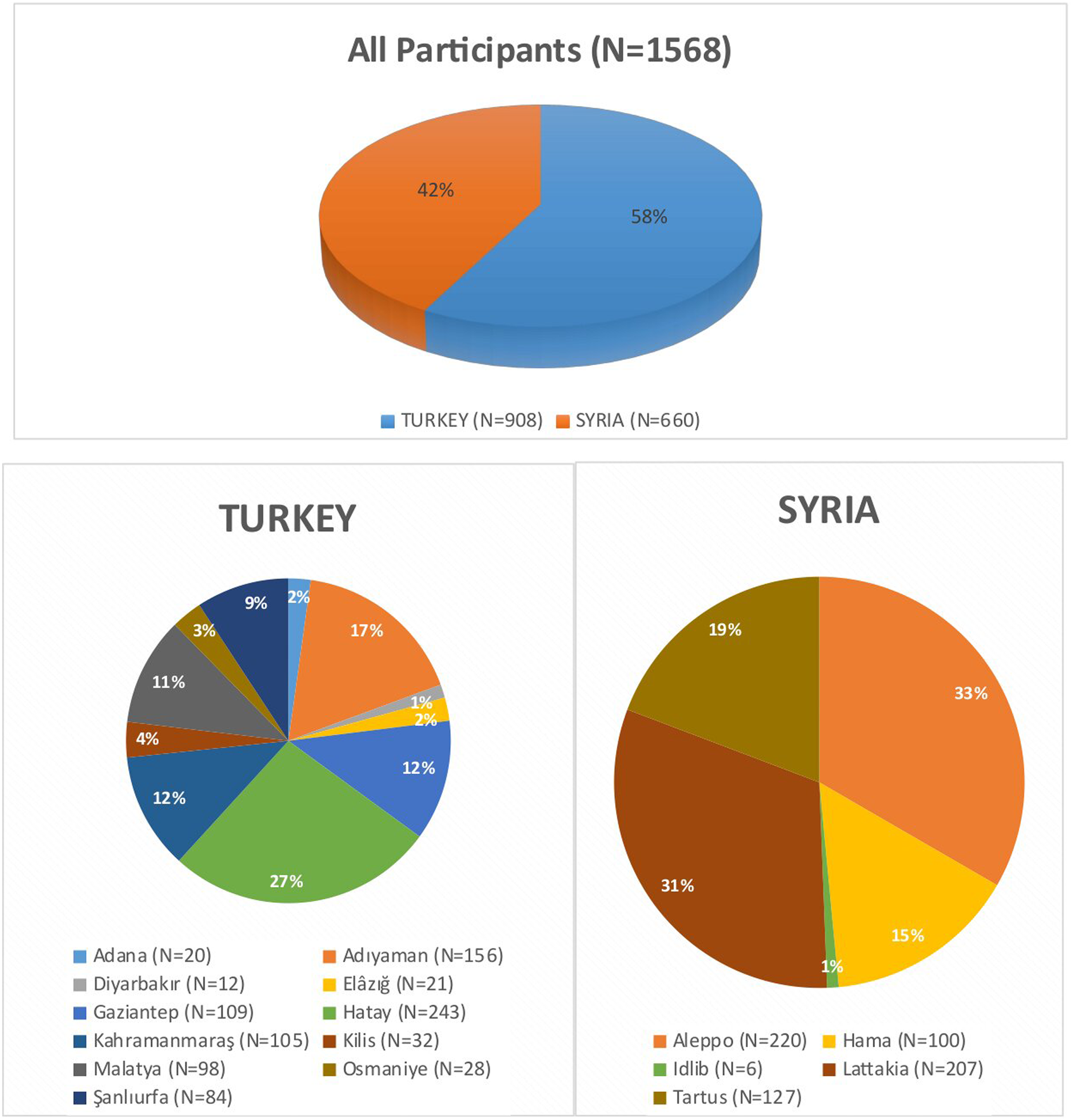
Distribution of study population between Syria and Turkey.
Sociodemographic features and degree of social support by PTSD status
Of the 1577 participants who initially responded to the questionnaire, 5 who refused to provide written informed consent and 4 who provided incomplete or contradictory responses were excluded, resulting in a completion rate of 99.4%. Of the 1568 participants included in this study, 388 (24.7%) were classified as having probable PTSD according to PCL-C checklist (Figure 2(a)), whereas 1180 (75.3%) did not have probable PTSD (Figure 2(b)).
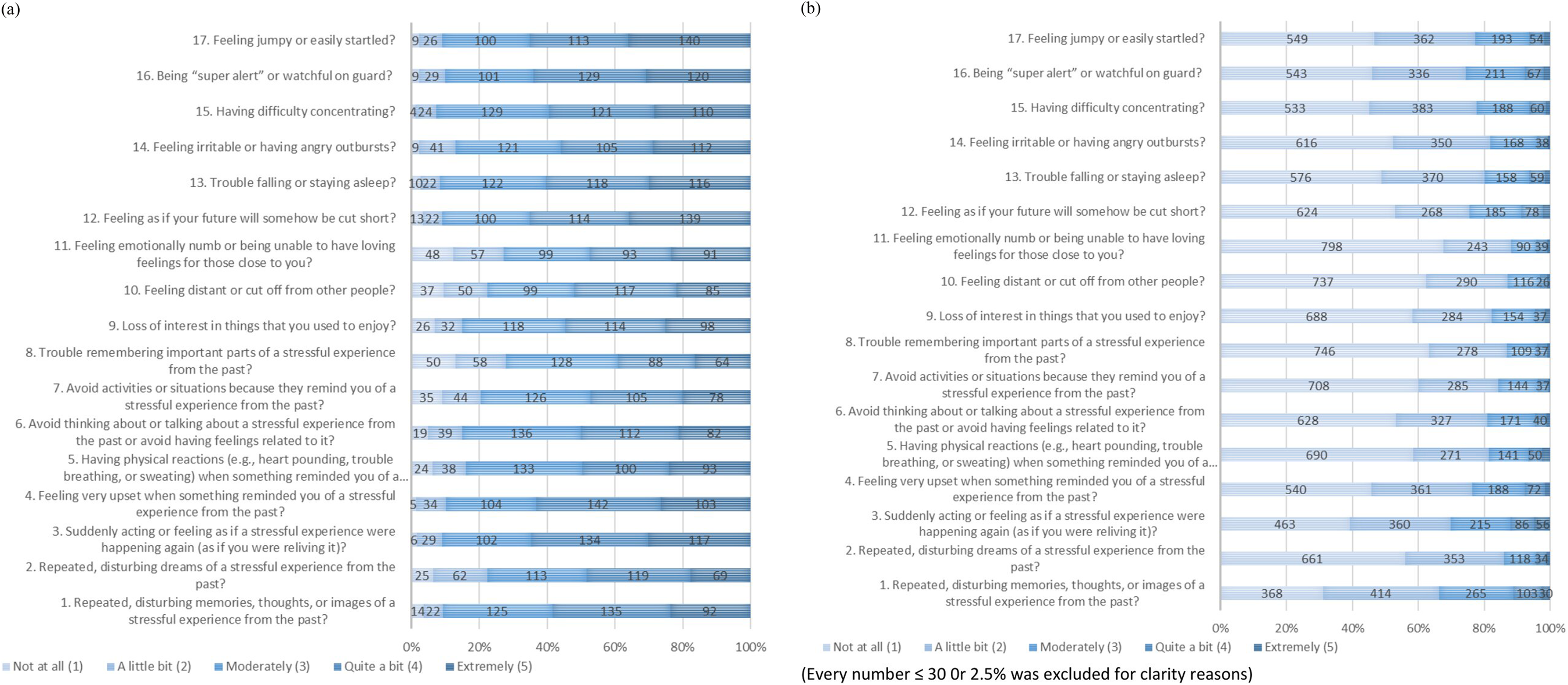
(a) Frequency of PTSD symptoms within the PTSD group according to the PCL-C; (b) frequency of PTSD symptoms within the non-PTSD group according to the PCL-C.
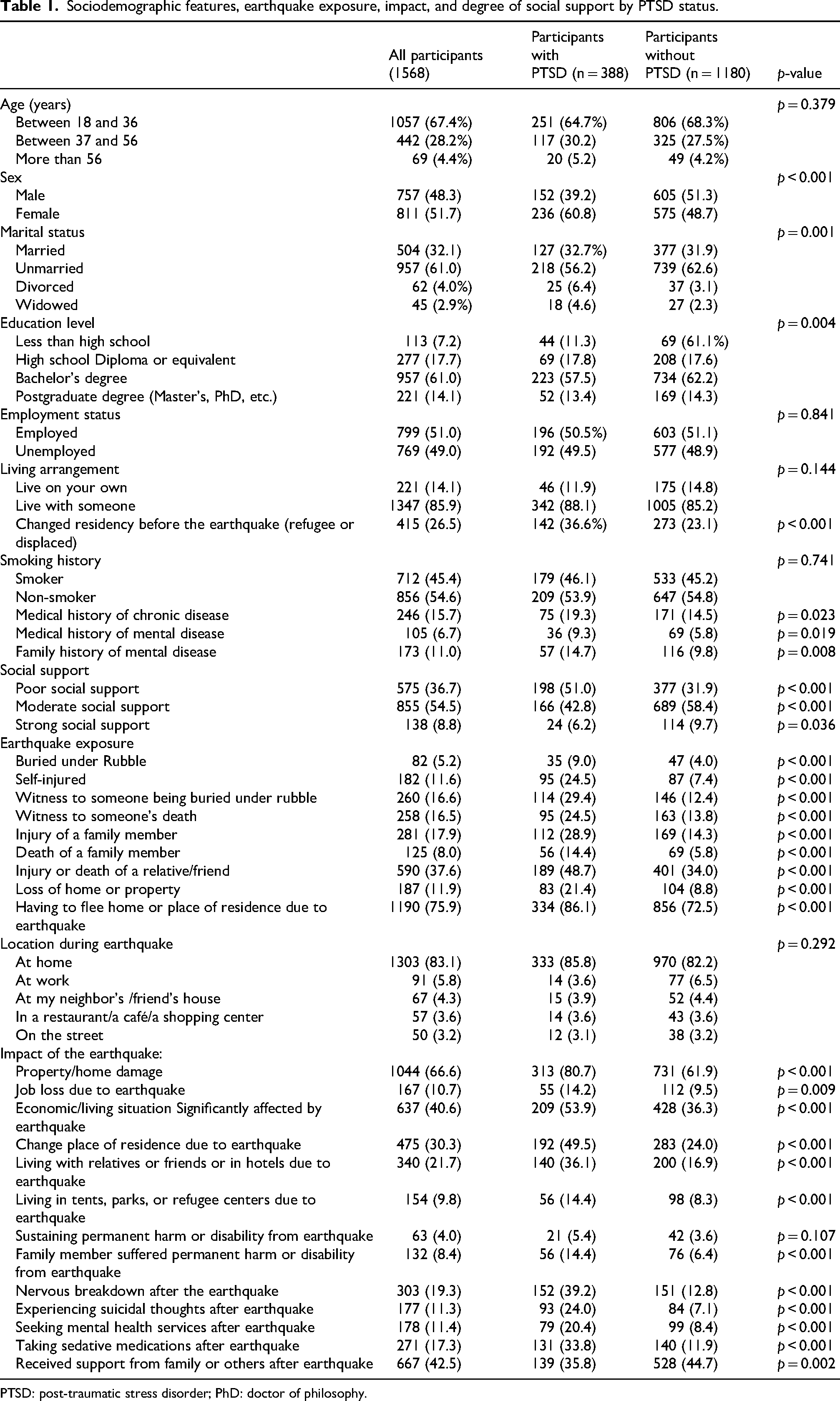
The age group between 18 and 36 was the most common among participants, accounting for 1057 (67.4%). Female sex, lower education level, refugee or internally displaced status, personal and family history of mental illness, and poor social support were significantly more common among participants with PTSD compared with those without (p < 0.05). Unemployment showed no statistically significant difference between groups (p = 0.841). Strong social support was more common in the non-PTSD group (p = 0.036) (Table 1).
Sociodemographic features, earthquake exposure, impact, and degree of social support by PTSD status.
PTSD: post-traumatic stress disorder; PhD: doctor of philosophy.
Earthquake exposure
Being buried under rubble, sustaining a self-injury, witnessing burial under rubble or death, and experiencing injury or death of family members or friends were all significantly more common in the PTSD group compared with the non-PTSD group (p < 0.001).Having to flee home or place of residence due to the earthquake was also more frequent in the PTSD group (p < 0.001) (Table 1).
Impact of the earthquake on survivors
Loss of property, negative economic or living impacts, and changes in residence or living arrangements were significantly more common in the PTSD group (p < 0.001), whereas job loss was also higher in the PTSD group (p = 0.009). Family-related impacts, including permanent harm or disability among family members as well as suicidal thoughts, seeking mental health services, use of sedative medication, and experiencing a nervous breakdown were all significantly higher in the PTSD group (p < 0.001). Receiving social support after the earthquake was higher in the non-PTSD group (p < 0.001) (Table 1).
Multivariate logistic regression analysis
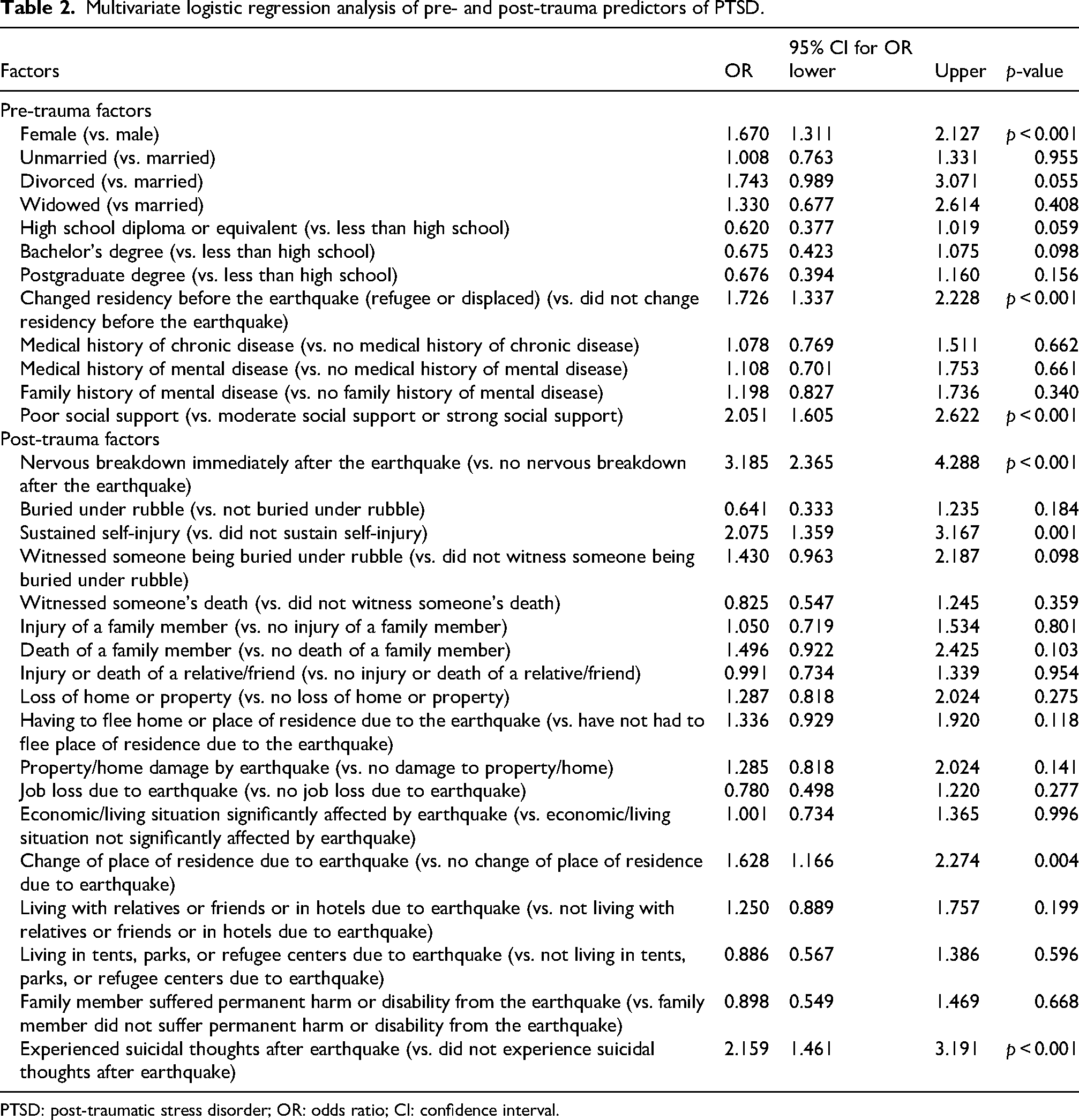
A multivariate logistic regression analysis was performed to identify the associations between pre-trauma and post-trauma variables with the development of PTSD versus no PTSD.
The logistic regression revealed statistically significant associations between PTSD and the following pre-trauma factors: being female (odds ratio (OR): 1.670, p < 0.001), having changed residency before the earthquake (OR: 1.726, p 0.001), and poor social support (OR: 2.051, p < 0.001).
Additionally, significant post-trauma factors included experiencing a nervous breakdown (OR: 3.185, p < 0.001), sustaining a self-injury (OR: 2.075, p = 0.001), changing residence due to the earthquake (OR: 1.628, p = 0.004), and experiencing suicidal thoughts (OR: 2.159, p < 0.001) (Table 2).
Multivariate logistic regression analysis of pre- and post-trauma predictors of PTSD.
PTSD: post-traumatic stress disorder; OR: odds ratio; CI: confidence interval.
Discussion
This study is the first to examine the prevalence and risk factors of PTSD among survivors of the 2023 Syria and Turkey earthquake 1 year following the event. We identified a probable PTSD prevalence of 24.7%, which is consistent with previous findings from Turkey.27,28 In Syria, PTSD rates were higher shortly after the earthquake, with 57.9% in severely affected areas and 55.4% in moderately affected areas within 1 month after the earthquake. 13 A 3-month follow-up study in Turkey showed a prevalence of 51.4%. 11 A meta-analysis indicated that PTSD incidence averages 28.76% within 9 months of traumatic events, decreasing to 19.48% for later assessments. 9 This suggests a gradual decline in PTSD prevalence over time and spontaneous recovery.29,30 A historical comparison in Turkey showed a decrease from 42% 1 month post-event to 23% 13 months after the 1998 earthquake. 31 Globally, PTSD prevalence varies widely and is influenced by factors such as study design, cultural context, demographic characteristics of the study population, assessment tools, and timing after the disaster. Overall, previous studies suggest that PTSD prevalence is typically higher in the early post-disaster period and tends to decline over time, although it remains influenced by contextual and demographic factors. For instance, cross-sectional studies reported varying rates of PTSD prevalence: 20.3% in Peru 1 month post-earthquake, 32 18.9% in Nepal 3 years later, 26 21.71% in Italy after 20 months, 33 and 14.7% in Japan 6 months post-event. 34 These findings highlight the complex factors that influence PTSD prevalence after earthquakes.29,35
Having a medical history of mental disease and a family history of mental disorders were significantly associated with PTSD, with p-values of 0.01 and <0.001, respectively. Previous studies have shown that pre-trauma mental disorders, including mood, anxiety, and conduct disorders, increase the risk of developing PTSD.15,36,37 A study of Wenchuan earthquake survivors found that personal histories of depression and anxiety were predictive of PTSD. 38 In the US, veterans who had fathers with PTSD histories were 26% more likely to meet PTSD criteria themselves, suggesting a potential generational transmission of trauma. 39 Additionally, family histories of psychopathology and substance abuse have been identified as pre-existing vulnerability factors for developing PTSD among children. 40 Overall, previous studies consistently identify pre-trauma vulnerabilities, particularly prior mental illness and demographic factors, as important predictors of PTSD across different populations.
Exposure to several traumatic events during earthquakes was associated with PTSD. These events included being buried under rubble, witnessing someone being buried or dying, sustaining injuries to family members, experiencing the deaths of family members, dealing with injuries or deaths of relatives or friends, losing a home, and having to evacuate. All these factors were significantly associated with increased PTSD rates (p < 0.001). This was similar to findings in previous studies.26,33,41–44 An observational study in Italy found that 57% of individuals who were buried under rubble continued to experience PTSD 3 years after the earthquake. 45 Similarly, recent findings from the 2023 earthquake in Turkey indicated that individuals who witnessed death or injury had family or friends injured or killed, were buried under debris, suffered home damage, or were forced to evacuate displayed significantly higher rates of PTSD. 46 These traumatic exposures often induce intense feelings of fear and helplessness, which can lead to long-lasting mental health challenges, according to various studies. 47 These findings suggest that the severity and directness of trauma exposure are consistently associated with increased PTSD risk across different disaster settings.
Regarding the impact of the earthquake on survivors’ lives, job loss due to the earthquake and changes in economic situation due to the earthquake (p < 0.001) were associated with PTSD. A longitudinal study among survivors of the 2011 Great East Japan Earthquake and Tsunami found that those who suffered job loss due to the earthquake still had PTSD even after 5 years. 42 Another study in Japan showed that a decline in economic situation following an earthquake increased the prevalence of PTSD. 48 Overall, post-trauma stressors, including economic hardship, displacement, and limited support, appear to play a significant role in the persistence and severity of PTSD symptoms.
Seeking mental health services after the earthquake was also significantly correlated with PTSD (p < 0.001). A longitudinal study of natural disaster survivors found that using psychological counseling was associated with PTSD. 49 Furthermore, PTSD symptoms were significant predictors of mental health service utilization post-disaster in the Netherlands. 50 The use of sedative medications after the earthquake was also associated with PTSD (p < 0.001). Following the 11 September attacks, survivors with PTSD were more likely to use psychiatric medication. 51 Conversely, receiving family support was linked to lower PTSD prevalence (p < 0.001), which was consistent with previous studies.9,12,52
In the logistic regression analysis, we explored pre-trauma factors associated with the development of PTSD. We found that being female was linked to a 1.670 times higher OR of developing PTSD compared with males (p < 0.001). This result is consistent with previous studies.10,53–55 Both psychological and biological factors contribute to this pattern. 56 During disasters, women tend to be more sensitive not only to their own situations but also deeply affected by the trauma experienced by others, which could potentially amplify their own traumatic responses. 57 Additionally, the sense of loss of control and the disruption of social support networks post-disaster significantly increase the impact of disasters on women, thereby raising their risk of PTSD.57,58 Moreover, women's brains often respond to stress with increased sensitivity, making them more susceptible to PTSD. 56 Being a refugee or internally displaced individual was associated with a 1.726 times higher odds of developing PTSD (p < 0.001), consistent with previous findings. 59 This elevated risk may be explained by experiencing multiple traumas—such as war, the refugee journey, and subsequent disasters like earthquakes—which cumulatively increase the likelihood of developing PTSD. 60 This pattern is distinctly observable among Syrian participants in our study. For instance, before the earthquake, a cross-sectional study reported a PTSD prevalence of 33.5% among Syrian refugees in Turkey. 61 Another study revealed a 36.9% prevalence rate of PTSD among the Syrian population, and both studies linked experiences of war and displacement with an increased risk of developing PTSD. 62 Another important factor identified was social support; our findings indicated that having poor social support was associated with 2.051 times higher odds of developing PTSD compared with having moderate or strong social support (p < 0.001). This result is consistent with a study in Ethiopia among landslide survivors, which reported that individuals with poor social support had a 3.64 times higher risk of developing PTSD. 63 Another review revealed the critical role of social support in the prevention and recovery of PTSD by fostering a sense of safety in affected individuals. 64 However, another systematic review suggested that the relationship between social support and PTSD is not direct and may be influenced by confounding factors such as sex, previous history of trauma, and self-efficacy. 65
For post-trauma factors, experiencing a nervous breakdown immediately after the earthquake was associated with an increased likelihood of developing PTSD, with an OR of 3.185 (p < 0.001). A cross-sectional study in Peru confirmed that survivors who experienced a nervous breakdown immediately after the earthquake showed a higher prevalence of PTSD symptoms. 32 Additionally, changing residence due to the earthquake was also linked to an increased risk of developing PTSD, with an OR of 1.628 (p = 0.004). This finding is supported by a study in Turkey, which indicated that relocation among earthquake survivors predicted PTSD. 66 Moreover, a qualitative study in China among Sichuan earthquake survivors with PTSD revealed that post-disaster relocation undermines individual's sense of meaning and community belonging, disrupts connections, and negatively impacts daily life, which might lead to prolonged and persistent PTSD. 67 Another cross-sectional study in Turkey, however, showed no significant correlation between relocation and the development of PTSD. 68
Sustaining a self-injury was associated with a 2.075 times higher odds of developing PTSD compared with those who did not sustain injuries (p = 0.001). This finding aligns with a study in China, which reported that 10 years after the Wenchuan earthquake, the prevalence of PTSD among victims with physical disabilities remained high at 42.21%, highlighting the importance of providing mental support for these victims’ well-being. 38 Previous studies revealed similar findings.6,9,69 Experiencing suicidal thoughts was associated with significantly increased odds of developing PTSD compared with participants who did not have such thoughts (OR: 2.159; p < 0.001). These results are consistent with previous research demonstrating a strong connection between PTSD and suicidal behaviors among earthquake survivors.70–72 Furthermore, a recent study in Turkey involving survivors of the 2011 earthquake supports this relationship, showing that suicidality post-earthquake predicts PTSD development. 72
This study contributes uniquely to the literature by providing 1-year post-disaster data from a large, combined sample of survivors in both Syria and Turkey and simultaneously evaluating pre-trauma, trauma-related, and post-trauma factors. This comprehensive approach allows for a more integrated understanding of PTSD risk in populations affected by both natural disasters and prolonged conflict.
Although this study focused on PTSD, other trauma-related conditions such as complex post-traumatic stress disorder (C-PTSD) and embitterment disorder may also be relevant in this population. C-PTSD, often associated with prolonged or repeated trauma such as war and displacement, includes additional symptoms related to emotional regulation, self-concept, and interpersonal relationships. 73 Embitterment disorder, characterized by persistent feelings of injustice and helplessness following negative life events, may also arise in disaster-affected populations. 74 The absence of specific assessment tools for these conditions in this study may lead to an underestimation or misclassification of trauma-related psychological outcomes. Future studies should consider incorporating these constructs to provide a more comprehensive evaluation of mental health following complex disasters.
Study limitations
Our study has several important limitations that should be considered when interpreting the findings. First, the cross-sectional nature of the study limits our ability to establish causal relationships between the variables. Second, we used convenience sampling from social media and specific sites for interviews. This sampling approach might lead to underrepresentation of specific groups, such as older individuals who represented a minority in our study and those most severely affected by the earthquake, including individuals who lost their homes. These populations are less likely to be reached due to limited internet access; therefore, further research is needed to assess these groups. As such, prioritizing outreach to these vulnerable populations is essential. Third, as the survey was self-administered, there is a potential for recall bias. Moreover, although the PCL-C is widely used globally as a screening measure, it is not a diagnostic tool. Participants in our study with a score of ≥50 were classified as having probable PTSD without a clinical interview, which may affect the accuracy of PTSD diagnosis. The use of the PCL-C, based on DSM-IV criteria, rather than DSM-5–based instruments may limit comparability with more recent studies and affect alignment with current diagnostic standards. Finally, this study focused solely on PTSD and did not assess other trauma-related conditions such as C-PTSD or embitterment disorder, which may overlap with or influence PTSD symptoms, potentially leading to underestimation or misclassification of psychological outcomes.
Conclusion
This cross-sectional study of survivors of the 2023 earthquake in Syria and Turkey found a PTSD prevalence of 24.7% 1 year post-disaster. Multivariate regression analysis identified significant predictors of PTSD, including female sex, refugee or internally displaced status, and poor social support. Post-trauma factors significantly associated with PTSD included sustaining self-injury, changing residence due to the earthquake, experiencing suicidal thoughts, and having a nervous breakdown immediately after the disaster.
Supplemental Material
sj-docx-1-imr-10.1177_03000605261464268 - Supplemental material for Prevalence and risk factors of post-traumatic stress disorder among 2023 earthquake survivors in Syria and Turkey: A multinational cross-sectional study
Supplemental material, sj-docx-1-imr-10.1177_03000605261464268 for Prevalence and risk factors of post-traumatic stress disorder among 2023 earthquake survivors in Syria and Turkey: A multinational cross-sectional study by Sara Albuaini, Michel Najjar, Yahia Mustafa, Mohammad Hasan, Musab Ibrahim Yehya Tawfik and Lana Saeed in Journal of International Medical Research
Supplemental Material
sj-docx-2-imr-10.1177_03000605261464268 - Supplemental material for Prevalence and risk factors of post-traumatic stress disorder among 2023 earthquake survivors in Syria and Turkey: A multinational cross-sectional study
Supplemental material, sj-docx-2-imr-10.1177_03000605261464268 for Prevalence and risk factors of post-traumatic stress disorder among 2023 earthquake survivors in Syria and Turkey: A multinational cross-sectional study by Sara Albuaini, Michel Najjar, Yahia Mustafa, Mohammad Hasan, Musab Ibrahim Yehya Tawfik and Lana Saeed in Journal of International Medical Research
Supplemental Material
sj-docx-3-imr-10.1177_03000605261464268 - Supplemental material for Prevalence and risk factors of post-traumatic stress disorder among 2023 earthquake survivors in Syria and Turkey: A multinational cross-sectional study
Supplemental material, sj-docx-3-imr-10.1177_03000605261464268 for Prevalence and risk factors of post-traumatic stress disorder among 2023 earthquake survivors in Syria and Turkey: A multinational cross-sectional study by Sara Albuaini, Michel Najjar, Yahia Mustafa, Mohammad Hasan, Musab Ibrahim Yehya Tawfik and Lana Saeed in Journal of International Medical Research
Footnotes
Acknowledgments
We are thankful to all who participated in the study.
Ethics approval and informed consent
This study was approved by the Institutional Review Board (IRB) at the Syrian Private University (SPU) and Medstar Antalya Hospital. The IRBs at SPU and Medstar Antalya Hospital did not provide us with a number/ID. All participants’ data were deidentified by the investigators to ensure participant confidentiality and compliance with the Declaration of Helsinki. All participants confirmed their written consent by answering a yes–no question. Participation in the study was voluntary, and participants were assured that anyone who was not inclined to participate or decided to withdraw after confirming consent would not be victimized. All information collected from this study was kept strictly confidential. Given the sensitive nature of trauma-related questions, participants were informed that they could skip any question or withdraw from the study at any time without consequence. At the end of the questionnaire, participants were provided with a brief definition of Post-Traumatic Stress Disorder (PTSD) and its symptoms. They were advised to seek medical assistance if they, their family, or friends experienced these symptoms. Additionally, information on hotlines for urgent medical advice in cases of suicidal thoughts or other urgent mental health issues was provided. Participants were assured that these services are confidential and free of charge. Efforts were made to minimize psychological distress by avoiding unnecessarily triggering or graphic content in the questionnaire.
Authors’ contributions
SA and MN conceptualized the study, participated in the study design, performed the statistical analysis, interpreted the results, conducted a literature search, drafted the manuscript, and revised the final draft of the paper. YM, MH, and MT participated in the study design, assisted in data collection, and contributed to the statistical analysis. LS participated in the design of the study and revised the final draft. Data Collection Group: Georgina Najjar, Musab Alkhani, Lina Albari, Samaher Younes, Hossein Mohammad, M. Wafa Hamoud Alhussein.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The dataset(s) supporting the conclusions of this article are included within the article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.