
Abstract
Objective
To compare the clinical outcomes and prognosis of regional citrate anticoagulation and systemic heparin anticoagulation in patients with sepsis-associated acute kidney injury undergoing continuous renal replacement therapy.
Methods
This retrospective cohort study (2020–2024) included 168 adults with sepsis-associated acute kidney injury who received continuous renal replacement therapy at the intensive care unit of Taizhou Municipal Hospital. Kaplan–Meier curves and multivariable Cox regression were used to evaluate 14- and 28-day mortality, with subgroup analyses performed to assess effect modification.
Results
Among 168 eligible patients, 1:1 propensity score matching yielded 42 well-balanced pairs (regional citrate anticoagulation, n = 42; systemic heparin anticoagulation, n = 42) with comparable baseline characteristics. Hospital mortality was lower with regional citrate anticoagulation (59.5%) than with systemic heparin anticoagulation (71.4%); however, the difference did not reach statistical significance (P = 0.251). The 14-day comparison demonstrated a higher survival probability with regional citrate anticoagulation (log-rank P = 0.043; hazard ratio, 2.10; 95% confidence interval: 1.01–4.39), and a similar benefit persisted at 28 days (log-rank P = 0.042; hazard ratio, 1.76; 95% confidence interval: 1.01–3.05). Subgroup analysis further indicated that the survival benefit of regional citrate anticoagulation on 28-day mortality was most pronounced among patients with pre-existing hypertension (hazard ratio, 2.75; 95% confidence interval: 1.32–5.71; P = 0.007; interaction P = 0.028).
Conclusions
In patients with sepsis-associated acute kidney injury requiring continuous renal replacement therapy, regional citrate anticoagulation may confer better short-term (14- and 28-day) survival than systemic heparin anticoagulation; however, no clear difference in overall hospital mortality was observed. This potential benefit may be more pronounced among patients with hypertension, meriting further evaluation of tailored anticoagulation approaches.
Keywords
Introduction
Sepsis, defined as a dysregulated host response to infection, is frequently complicated by acute kidney injury (AKI).1–3 In a contemporary intensive care unit (ICU), more than half of all AKI cases are sepsis-related, 4 and up to 60% of patients with sepsis develop AKI. 5 Mortality in this population remains unacceptably high: a recent meta-analysis reported pooled in-hospital mortality of 49.8%. 6
The 28th Acute Disease Quality Initiative (ADQI) consensus (2023) formally defined sepsis-associated AKI (SA-AKI) and emphasized continuous renal replacement therapy (CRRT) as a cornerstone for managing severe SA-AKI. 7 Adequate anticoagulation is indispensable for maintaining circuit patency during CRRT. The two most widely adopted strategies are systemic heparin anticoagulation (SHA) and regional citrate anticoagulation (RCA). Randomized trials in general AKI cohorts suggest that RCA prolongs filter life and reduces bleeding risk but may increase metabolic derangements and infection rates, without affecting overall mortality.8–10 Nevertheless, outcome data on CRRT in the specific SA-AKI population remain limited, leaving uncertainty as to whether evidence derived from broader AKI cohorts can be extrapolated to these patients. Therefore, this study was designed to compare outcomes of RCA versus SHA, particularly in patients with SA-AKI receiving CRRT, delineate their prognostic impact, and identify subgroups that might derive differential benefit, thereby informing individualized anticoagulation decisions in this high-risk population.
Materials and methods
Study population and data source
We conducted a retrospective observational cohort study of consecutive adult patients admitted to the Department of Critical Care Medicine, Taizhou Municipal Hospital (Taizhou University Affiliated Municipal Hospital), School of Medicine, Taizhou University, between 1 January 2020 and 31 December 2024.
Eligible patients met all of the following criteria: (a) age ≥18 years; (b) diagnosis of SA-AKI according to the 2023 consensus report of the 28th ADQI and AKI stage ≥2 at CRRT initiation; 7 and (c) availability of complete clinical data.
Exclusion criteria were as follows: (a) pregnancy or lactation; (b) active malignancy in a terminal stage; (c) severe immunodeficiency; (d) chronic kidney disease; (e) chronic anticoagulation therapy; and (e) use of more than one anticoagulant during CRRT.
Anticoagulation protocols were standardized: RCA used 4 mmol/L citrate in pre-filter replacement fluid, targeting post-filter ionized calcium (0.25–0.35 mmol/L); SHA used a heparin bolus of 2000–5000 IU followed by an infusion of 5–15 IU/kg/h, targeting an activated partial thromboplastin time (APTT) of 1.5–2.0× baseline.
The study protocol was approved by the Institutional Ethics Committee of Taizhou Municipal Hospital (Taizhou University Affiliated Municipal Hospital), School of Medicine, Taizhou University (Approval Number: LWSL202500277). As a retrospective analysis, the requirement for written informed consent was waived by the Institutional Review Board. All procedures were conducted in accordance with the Declaration of Helsinki (2024 revision), and all patient data were fully deidentified before analysis. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for observational studies. 11
Data collection
The following data were extracted from the electronic medical record: age, sex, body mass index (BMI), comorbidities, source of admission (emergency, internal medicine, or surgery), surgical events (yes/no), Acute Physiology and Chronic Health Evaluation II (APACHE II) 12 and Sequential Organ Failure Assessment (SOFA) 13 scores, lengths of hospital and ICU stay, site of sepsis infection, isolated pathogens, duration of mechanical ventilation, duration and total dose of vasopressor support, laboratory parameters at CRRT initiation, CRRT modality (continuous venovenous hemodiafiltration (CVVHDF), preferred for hemodynamically unstable patients; continuous venovenous hemodialysis (CVVHD) for predominant azotemia; and continuous venovenous hemofiltration (CVVH) for isolated fluid overload), total CRRT time, duration of the first filter used during CRRT, mean duration of CRRT filters, number of filters lasting >48 h, CRRT pattern, bleeding events (yes/no), bleeding site, and in-hospital mortality.
Statistical analysis
All analyses were performed using R software (version 4.3.0).
Propensity score matching (PSM). In this retrospective cohort, anticoagulation strategy was dictated by real-time clinical status rather than random allocation, introducing overt selection bias. We therefore performed 1:1 nearest-neighbor PSM without replacement as a “post-hoc randomization” to isolate the effect of the anticoagulant itself. The propensity model incorporated age, sex, BMI, chronic liver disease, APACHE II score, APTT, prothrombin time (PT), total bilirubin (TBIL), alanine transaminase (ALT), and aspartate transaminase (AST)—covariates that simultaneously influence the clinician's decision (citrate vs heparin) and independently predict survival. APACHE II score was selected as the primary severity measure given its comprehensive assessment of baseline physiological status at ICU admission; SOFA score was not included due to its high correlation with APACHE II and overlapping measurement of disease severity. Infection source was excluded because it is not associated with anticoagulation strategy selection. Post-admission variables (vasopressor use and mechanical ventilation) were excluded to avoid collider bias from potential mediators. A caliper width of 0.1 SDs of the logit of the propensity score was applied. Balance before and after matching was evaluated using standardized mean differences (SMD); variables with SMD >0.1 were considered imbalanced, and density plots together with Love plots were generated to visually corroborate covariate balance. After matching, baseline profiles were well-balanced, so any divergence in outcomes is more plausibly ascribed to the anticoagulation regimen than to residual confounding. Descriptive statistics. After PSM, normally distributed continuous variables were expressed as mean ± SD and compared using two-sample Student's t-test (unpaired); non-normally distributed variables were reported as median (interquartile range (IQR)) and compared using the Mann–Whitney U test. Categorical data were summarized as counts and percentages (n (%)) and compared using the χ2 test or Fisher's exact test, as appropriate. Two-tailed P <0.05 was considered statistically significant. Survival analysis. Kaplan–Meier survival curves were constructed for 14- and 28-day all-cause mortality and compared using the log-rank test. Hazard ratios (HRs) with 95% confidence intervals (CIs) were estimated from multivariable Cox proportional hazards models (in all Cox models, RCA was set as the reference category) adjusted for relevant variables. A P-value <0.05 was considered statistically significant. Subgroup analyses. Subgroup analyses were prespecified based on clinical relevance and pathophysiological hypotheses. Forest plots of 14- and 28-day mortality were generated from multivariable Cox regression models (in all Cox models, RCA was set as the reference category) with an interaction term between anticoagulation strategy and each predefined subgroup. Interaction tests (P < 0.05) were considered the primary assessment of subgroup effects; subgroup-specific P-values were interpreted cautiously given the exploratory nature and reduced statistical power of these analyses.
Results
PSM of patients with SA-AKI receiving CRRT
Figure 1 presents the patient selection procedure in the current study. We initially screened 188 consecutive patients; after excluding 20 cases with missing key variables, 168 patients were retained for analysis. Among them, 107 (63.69%) received RCA and 61 (36.31%) received SHA. Using 1:1 PSM, we generated 42 well-matched pairs (RCA, n = 42; SHA, n = 42). After matching, baseline covariates included in the propensity score model—age, sex, BMI, chronic liver disease, APACHE II score, APTT, PT, TBIL, ALT, and AST—achieved adequate balance (SMD < 0.10 for all covariates; Figure 2). We assessed balance using SMDs rather than statistical significance testing, as recommended for propensity score-matched studies. Notably, several variables not included in the propensity score model (hospitalization duration, ICU stay duration, arterial partial pressure of carbon dioxide (PCO2), lymphocyte count, hemoglobin, source of admission, and abdominal infection focus) showed statistically significant differences between groups; these represent post-admission parameters potentially influenced by early disease trajectory rather than baseline confounders. Detailed comparisons before and after matching are presented in Table 1; the corresponding SMD diagrams and density plots are shown in Figures 2 and 3, respectively.
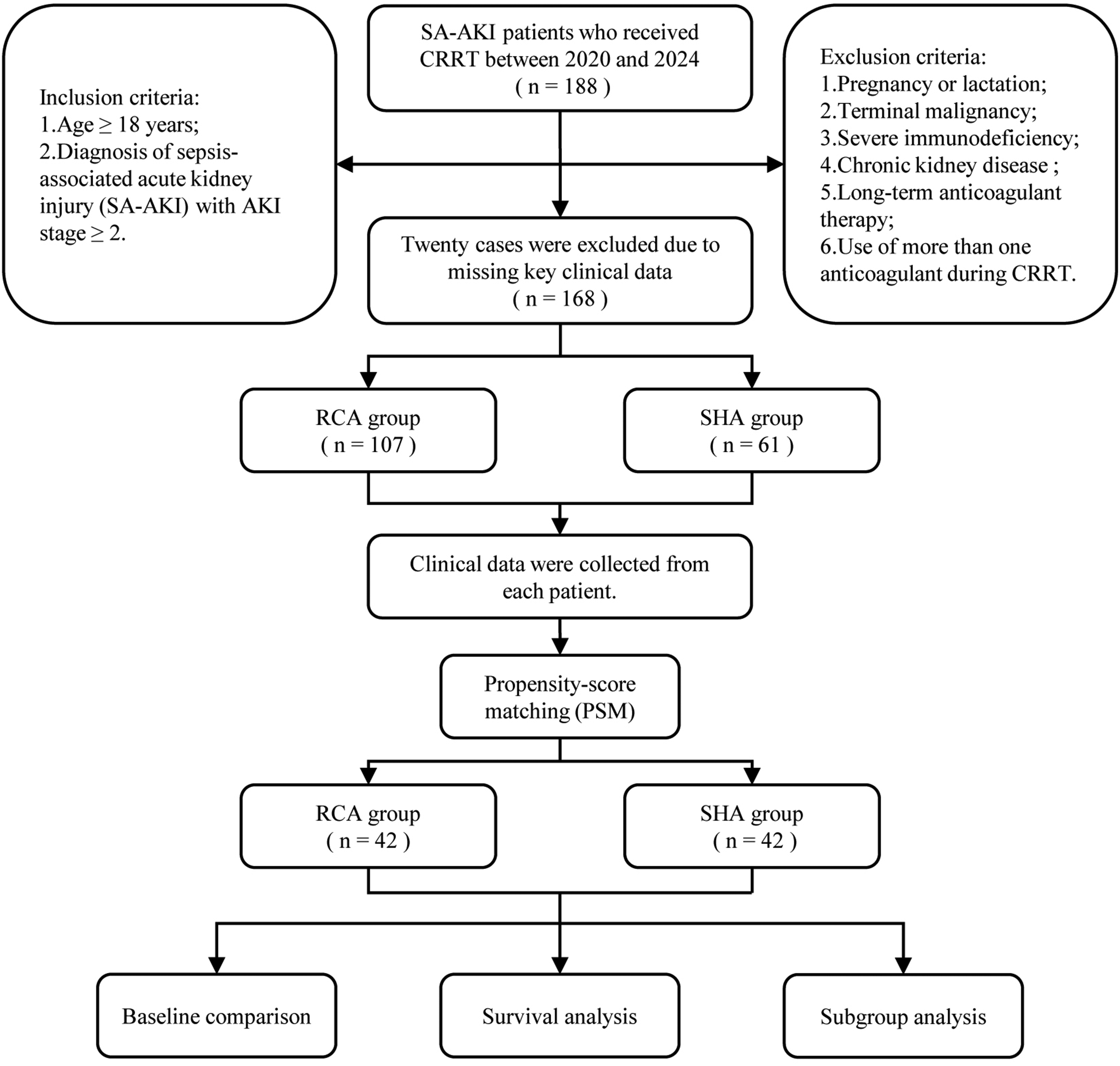
Flow diagram of the research.
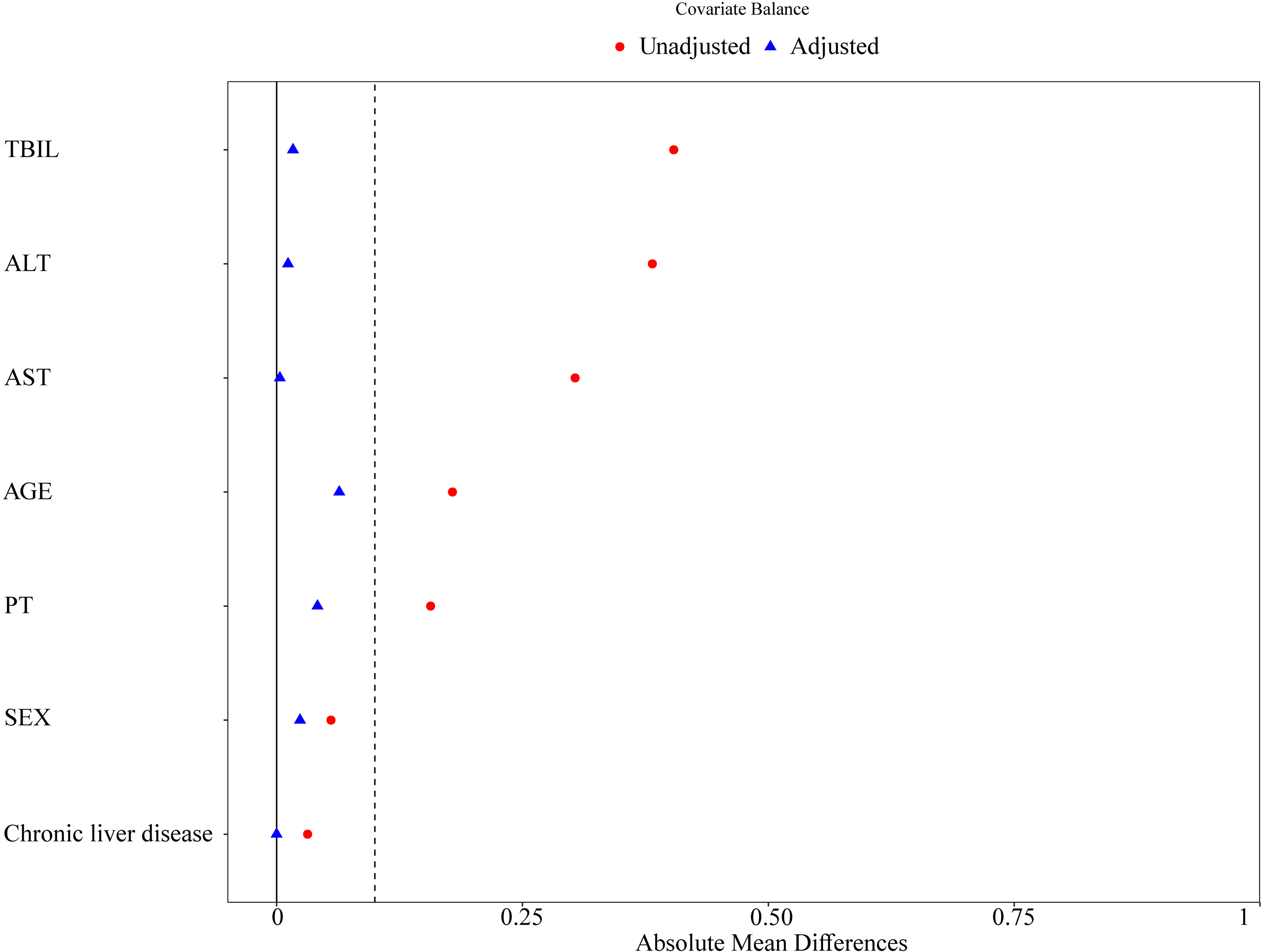
SMD diagrams before and after PSM. The SMD of seven baseline covariates after PSM.
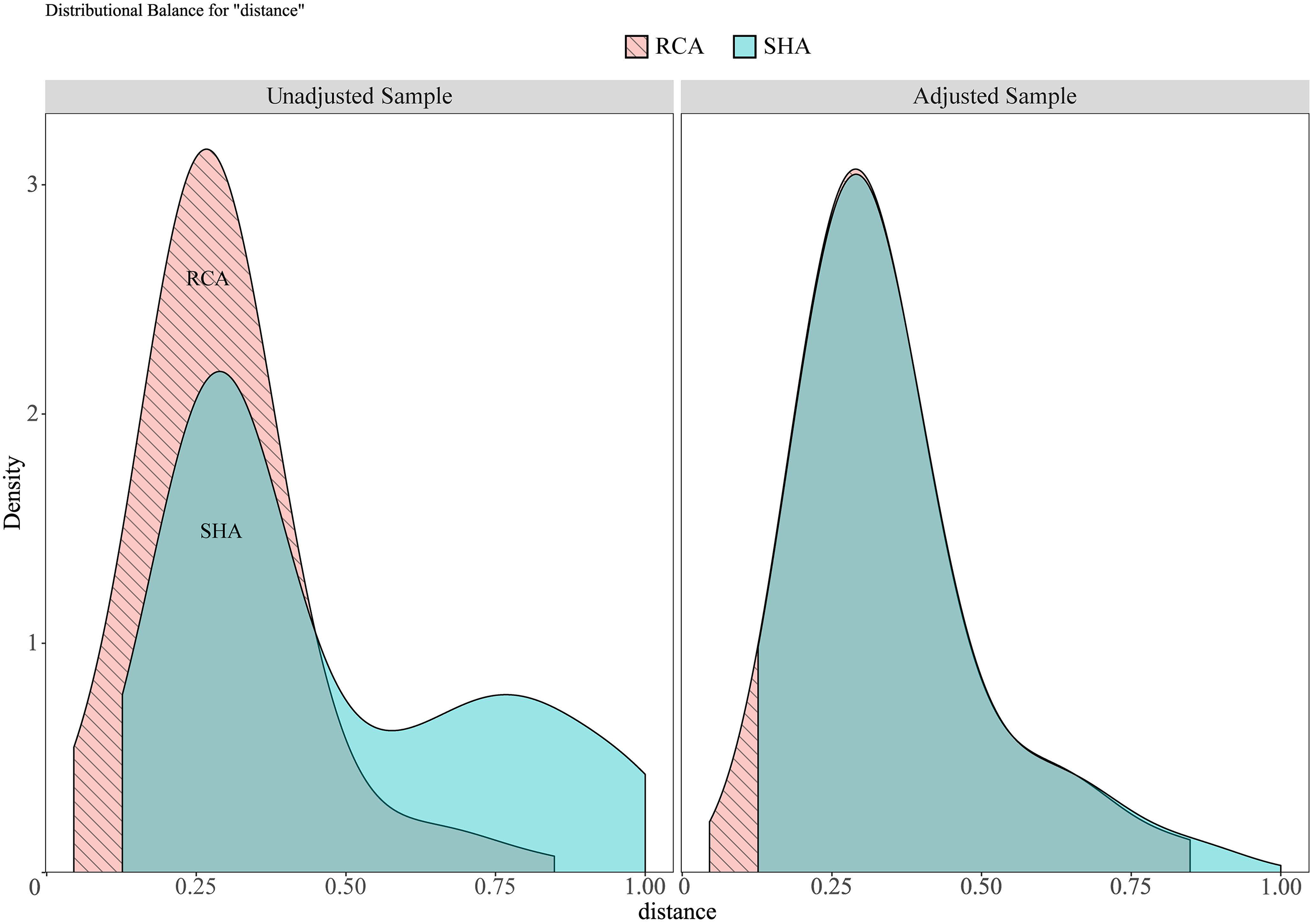
The corresponding density plots before and after PSM.
Comparison of baseline characteristics between RCA and SHA groups before and after PSM in patients with SA-AKI undergoing CRRT.
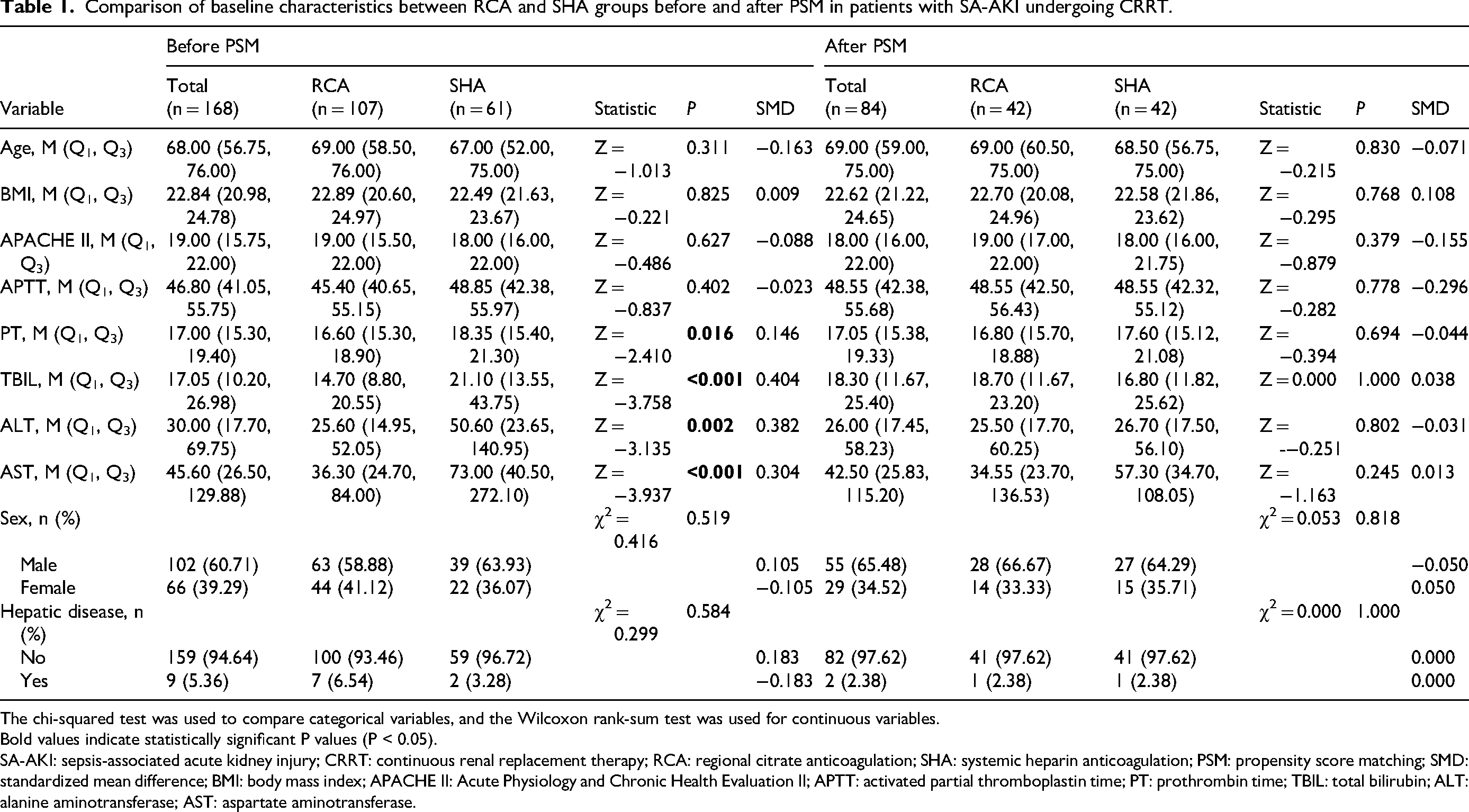
The chi-squared test was used to compare categorical variables, and the Wilcoxon rank-sum test was used for continuous variables.
Bold values indicate statistically significant P values (P < 0.05).
SA-AKI: sepsis-associated acute kidney injury; CRRT: continuous renal replacement therapy; RCA: regional citrate anticoagulation; SHA: systemic heparin anticoagulation; PSM: propensity score matching; SMD: standardized mean difference; BMI: body mass index; APACHE II: Acute Physiology and Chronic Health Evaluation II; APTT: activated partial thromboplastin time; PT: prothrombin time; TBIL: total bilirubin; ALT: alanine aminotransferase; AST: aspartate aminotransferase.
Baseline characteristics of RCA and SHA groups in patients with SA-AKI undergoing CRRT
Among the 84 propensity-matched patients, 29 (34.52%) survived and 55 (65.48%) died. Between-group comparisons revealed statistically significant differences in hospitalization duration (P = 0.038), ICU stay duration (P = 0.025), time of the first filter used in CRRT (median 54 vs 24.5 h, P = 0.006), number of filters lasting >48 h (median 1.0 vs 0.5, P = 0.007), arterial PCO2 before CRRT (P = 0.010), lymphocyte count (P = 0.042), hemoglobin concentration (P = 0.041), source of admission (emergency, internal medicine, or surgery; P = 0.039), and abdominal focus of sepsis (P = 0.035). All remaining variables were comparable between the two groups (P > 0.05). Full baseline characteristics are provided in Table 2.
Comparison of baseline characteristics between RCA and SHA anticoagulation methods in patients with SA-AKI undergoing CRRT treatment.
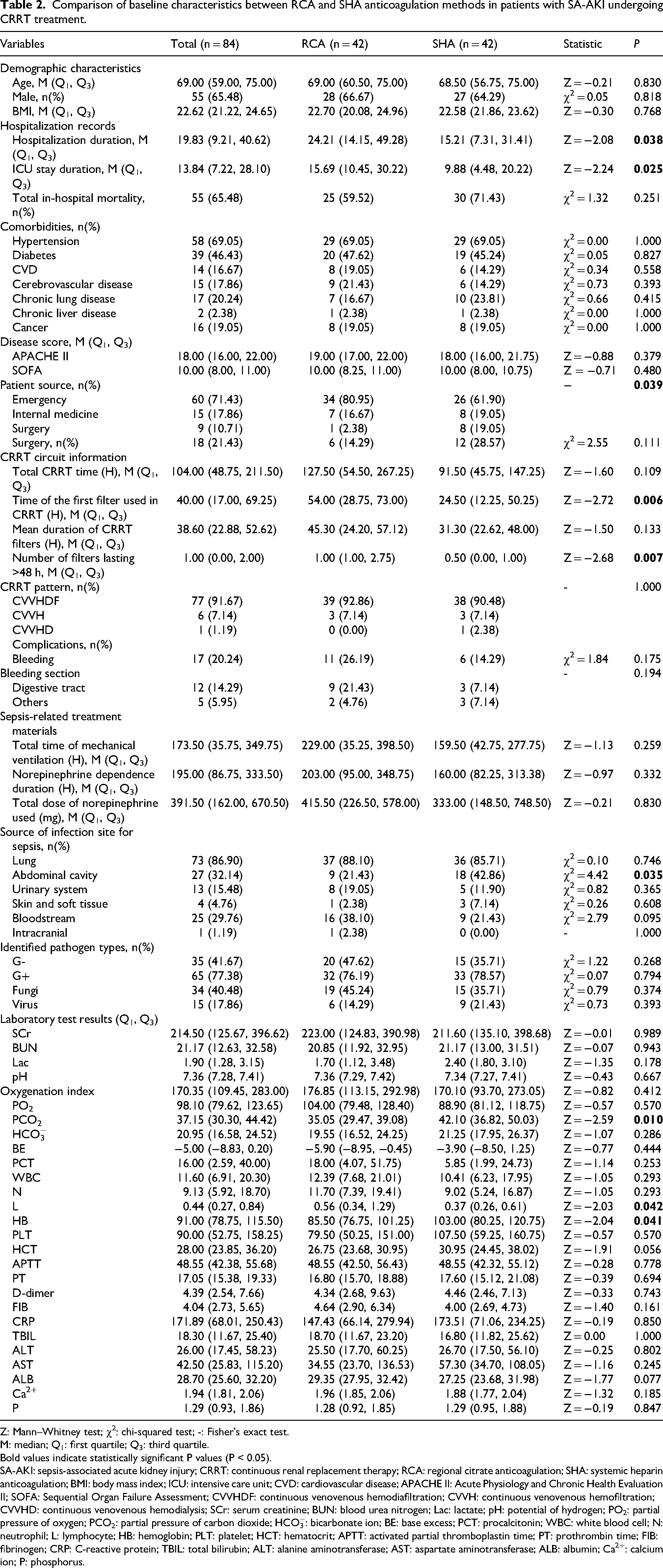
Z: Mann–Whitney test; χ2: chi-squared test; -: Fisher’s exact test.
M: median; Q1: first quartile; Q3: third quartile.
Bold values indicate statistically significant P values (P < 0.05).
SA-AKI: sepsis-associated acute kidney injury; CRRT: continuous renal replacement therapy; RCA: regional citrate anticoagulation; SHA: systemic heparin anticoagulation; BMI: body mass index; ICU: intensive care unit; CVD: cardiovascular disease; APACHE II: Acute Physiology and Chronic Health Evaluation II; SOFA: Sequential Organ Failure Assessment; CVVHDF: continuous venovenous hemodiafiltration; CVVH: continuous venovenous hemofiltration; CVVHD: continuous venovenous hemodialysis; SCr: serum creatinine; BUN: blood urea nitrogen; Lac: lactate; pH: potential of hydrogen; PO2: partial pressure of oxygen; PCO2: partial pressure of carbon dioxide; HCO3−: bicarbonate ion; BE: base excess; PCT: procalcitonin; WBC: white blood cell; N: neutrophil; L: lymphocyte; HB: hemoglobin; PLT: platelet; HCT: hematocrit; APTT: activated partial thromboplastin time; PT: prothrombin time; FIB: fibrinogen; CRP: C-reactive protein; TBIL: total bilirubin; ALT: alanine aminotransferase; AST: aspartate aminotransferase; ALB: albumin; Ca2+: calcium ion; P: phosphorus.
Survival analysis of patients with SA-AKI receiving CRRT with RCA or SHA
In-hospital mortality was 59.5% in the RCA group versus 71.4% in the SHA group, a difference that did not reach statistical significance (P = 0.25). To quantify the impact of RCA on 14-day and 28-day mortality, we refitted a multivariable Cox model—using RCA as the reference—and adjusted for age, sex, BMI, length of stay, admission route, admission source, abdominal infection focus, arterial PCO2, lymphocyte count, and hemoglobin. All covariates were measured prior to CRRT initiation and anticoagulation strategy selection. RCA remained independently associated with lower mortality at both 14 days (HR 1.97; 95% CI: 1.08–3.19; P = 0.046) and 28 days (HR 1.59; 95% CI: 1.05–2.73; P = 0.043). Schoenfeld residuals confirmed that the proportional hazards assumption was satisfied (global P = 0.18 and 0.21, respectively). To further address potential residual confounding from covariate imbalance, we conducted sensitivity analysis using inverse probability weighting (IPW) as an alternative to PSM. Results were consistent with the primary analysis (14-day mortality: HR 2.08, 95% CI: 1.03–4.21, P = 0.042; 28-day mortality: HR 1.74, 95% CI: 1.02–2.96, P = 0.041), confirming robustness of our findings. Kaplan–Meier curves diverged early and consistently favored RCA. Sensitivity analysis restricted to pre-treatment variables (age, sex, BMI, comorbidities, APACHE II score, and baseline coagulation parameters) yielded consistent results: RCA remained associated with lower 14-day mortality (HR 2.05; 95% CI: 1.02–4.12; P = 0.044) and 28-day mortality (HR 1.72; 95% CI: 1.03–2.87, P = 0.038), confirming the robustness of our findings. The 14-day comparison showed a higher survival probability with RCA (log-rank P = 0.043; HR 2.10; 95% CI: 1.01–4.39) (Figure 4), and a similar benefit persisted at 28 days (log-rank P = 0.042; HR 1.76; 95% CI: 1.01–3.05) (Figure 5).
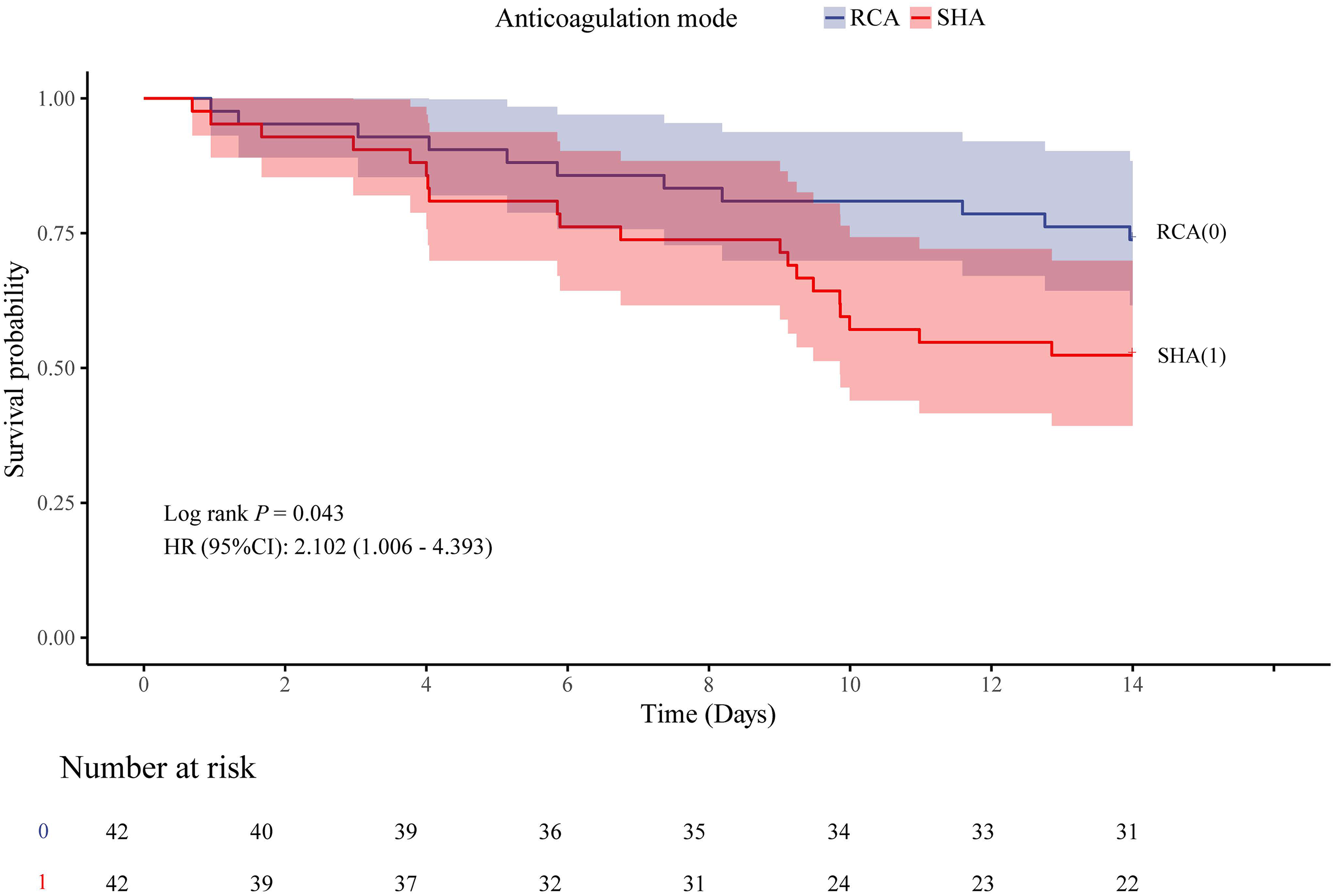
Kaplan–Meier survival curves comparing 14-day mortality risk between the RCA and SHA groups in patients with SA-AKI. RCA was set as the reference group (=0) and SHA as the exposure group (=1).
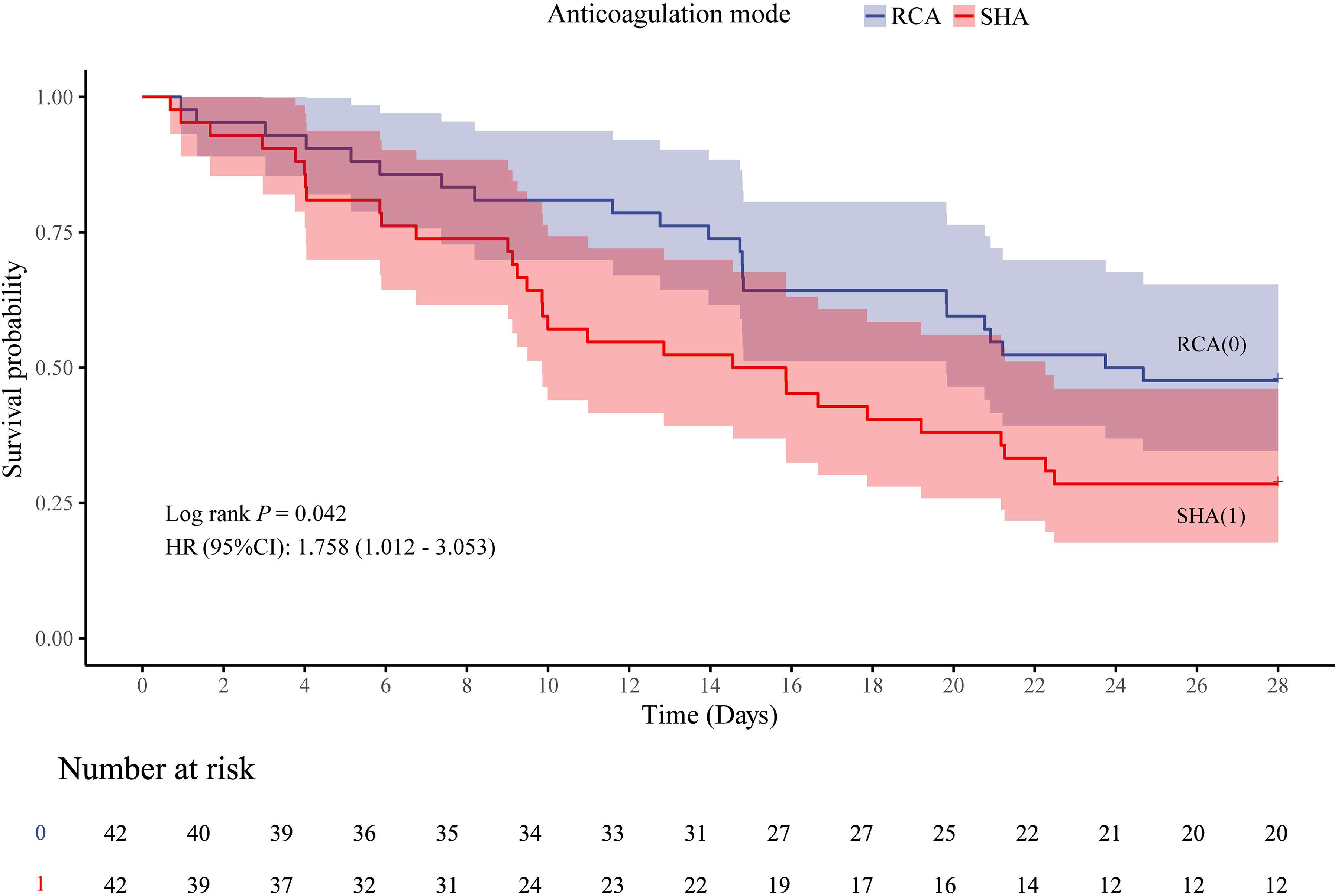
Kaplan–Meier survival curves comparing 28-day mortality risk between the RCA and SHA groups in patients with SA-AKI. RCA was set as the reference group (=0) and SHA as the exposure group (=1).
Subgroup analyses of RCA versus SHA in patients with SA-AKI receiving CRRT
Guided by clinical relevance, we examined whether baseline characteristics modified the effect of anticoagulation strategy. Eight prespecified subgroups were analyzed: age (<65 vs ≥65 years), comorbidities (hypertension, diabetes mellitus, cardiovascular disease, cerebrovascular disease, chronic pulmonary disease, chronic liver disease, andmalignancy), source of infection (pulmonary, abdominal, urinary, skin/soft tissue, bloodstream, and central nervous system), APACHE II score (3–14 vs 15–71),
14
SOFA score (0–6, 7–10, and 11–24),15,16 platelet count (<100 × 109/L vs ≥100 × 109/L), and TBIL (<20 μmol/L vs ≥20 μmol/L).
17
Multicollinearity was excluded; variance inflation factors for all subgroup variables were <5. In multivariable Cox models, we adjusted for sex and BMI.
We included 84 patients with SA-AKI who required CRRT (RCA 42, SHA 42). Within 14 days, mortality was lower with RCA than with SHA (11 vs 20 events; HR 2.10, 95% CI: 1.01–4.39, P = 0.048). At the subgroup level, RCA conferred a significant benefit in patients with hypertension (HR 3.20, 95% CI: 1.24–8.27, P = 0.016), pulmonary infection (HR 2.39, 95% CI: 1.11–5.14, P = 0.027), no enterocoelia infection (HR 2.46, 95% CI: 1.05–5.78, P = 0.038), no urinary system infection (HR 2.50, 95% CI: 1.08–5.75, P = 0.032), TBIL <20 μmol/L (HR 2.77, 95% CI: 1.18–6.49, P = 0.019), and APACHE II 15–71 (HR 2.28, 95% CI: 1.04–4.98, P = 0.039). None of the corresponding interaction tests, however, reached significance (all P > 0.05), leaving insufficient evidence to conclude that these baseline characteristics modify the relative effect of RCA. The subgroup forest plot is shown in Figure 6. Overall, 84 patients with SA-AKI receiving CRRT were included (42 per group). RCA was associated with a significantly lower 28-day mortality compared with SHA in the entire cohort (22/42 vs 30/42; HR 1.76, 95% CI: 1.01–3.05, P = 0.045). Subgroup analyses revealed that the survival benefit of RCA was predominantly confined to patients with pre-existing hypertension (interaction P = 0.028). Interaction tests were not significant for other subgroups (all P > 0.05). Given the modest sample size and exploratory nature of these analyses, these findings should be considered hypothesis-generating and require validation in larger cohorts. Among hypertensive patients (n = 58), 28-day mortality was 37.9% (11/29) in the RCA group versus 72.4% (21/29) in the SHA group (HR 2.75, 95% CI: 1.32–5.71, P = 0.007), whereas no significant difference was observed in non-hypertensive individuals (n = 26; HR 0.75, 95% CI: 0.31–1.80, P = 0.514). Consistent benefits were also detected in patients with pulmonary infection (HR 1.86, 95% CI: 1.03–3.37, P = 0.040), TBIL <20 μmol/L (HR 2.42, 95% CI: 1.25–4.69, P = 0.009), platelet count ≥100 × 109/L (HR 2.59, 95% CI: 1.11–6.06, P = 0.028), and APACHE II score 15–71 (HR 1.88, 95% CI: 1.06–3.36, P = 0.032). No significant survival advantage of RCA was found in the remaining subgroups, with all interaction P-values >0.05. The subgroup forest plot is shown in Figure 7.
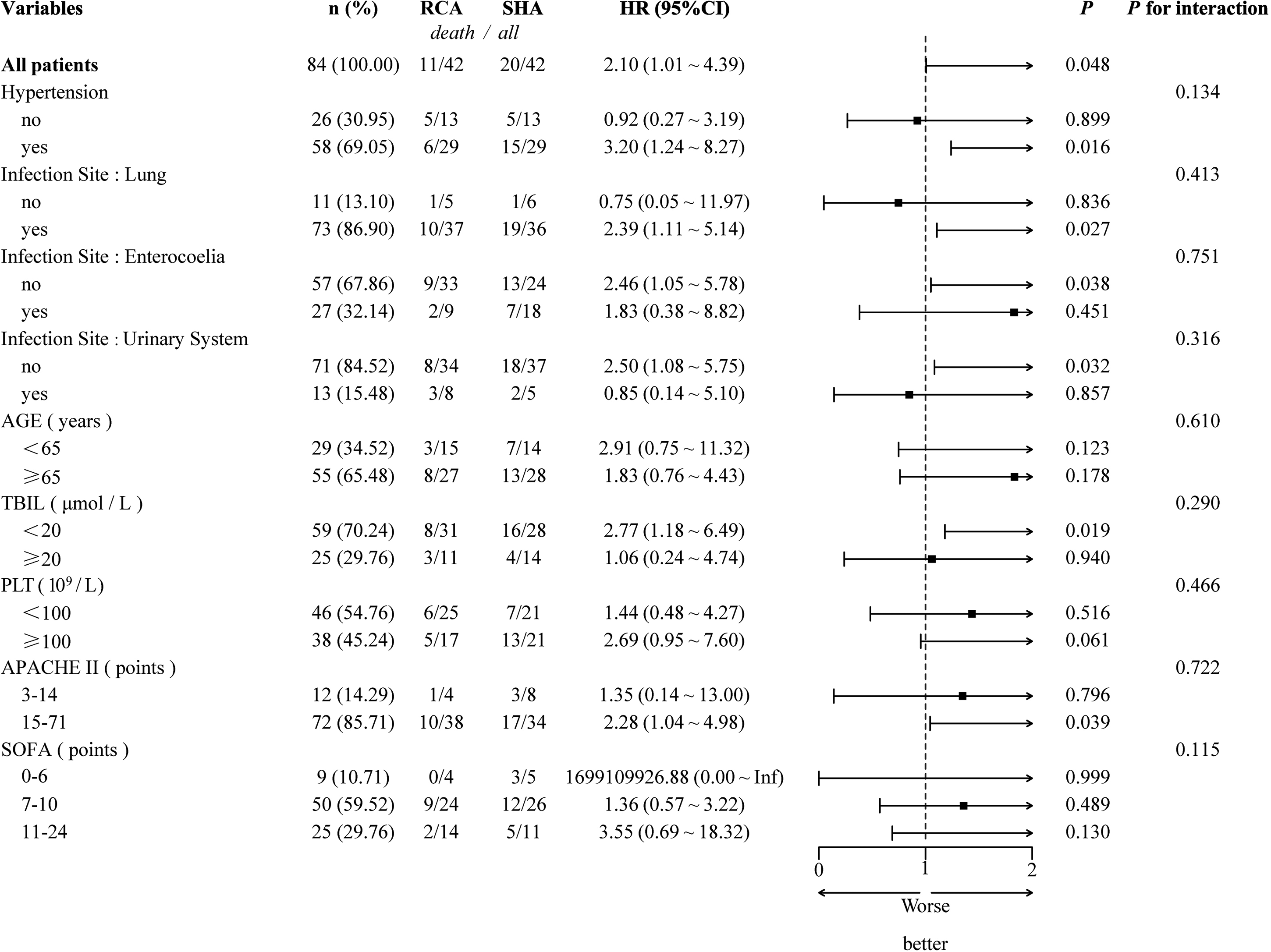
Subgroup analysis of RCA versus SHA within 14 days in patients with SA-AKI undergoing CRRT, illustrated by a forest plot. HRs were estimated with RCA as the reference; HR >1 indicates reduced mortality risk in the RCA group.
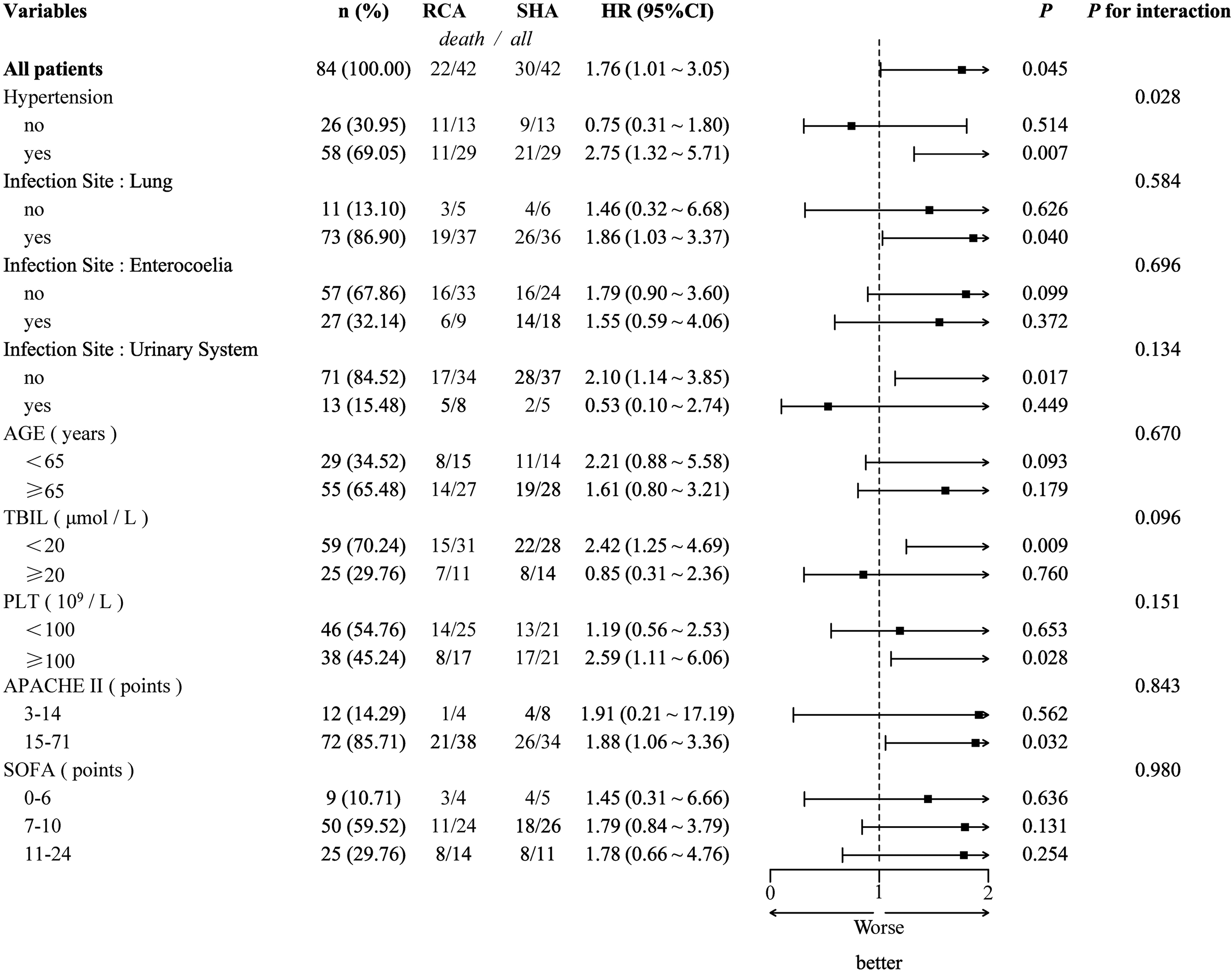
Subgroup analysis of RCA versus SHA within 28 days in patients with SA-AKI undergoing CRRT, illustrated by a forest plot. HRs were estimated with RCA as the reference; HR >1 indicates reduced mortality risk in the RCA group.
Discussion
This study sought to compare the clinical impact of RCA and SHA in patients with SA-AKI undergoing CRRT and to explore relevant subgroup effects. We found that RCA and SHA conferred similar in-hospital mortality; however, RCA was associated with superior short-term survival at 14 and 28 days. In addition, RCA prolonged first-filter lifespan and increased the number of filters lasting >48 h. Among predefined subgroups, patients with pre-existing hypertension appeared to derive particular benefit from RCA within 28 days. When contraindications are absent, RCA should therefore be considered the preferred anticoagulation strategy.
Overall mortality did not differ between RCA and SHA, consistent with previous studies conducted in broader AKI populations.8,10,18,19 This finding may be attributable to (a) limited statistical power in prior or the present cohorts 8 and (b) the multifactorial nature of mortality in critically ill patients receiving CRRT, where underlying disease severity, infection control, and multiorgan dysfunction often outweigh any anticoagulation-specific effect.7,8,10,18,19
Although regional citrate anticoagulation achieved a statistically longer first-filter lifespan than heparin (median 54 versus 24.5 h, P = 0.006) and a greater number of filters lasting >48 h (P = 0.007), the clinical importance of these differences is questionable. Filter longevity alone has not been convincingly linked to patient-centered outcomes. Total CRRT duration did not differ significantly between groups (median 127.5 vs 91.5 h, P = 0.109), and we did not observe differences in delivered dose or clotting rates. A 2023 systematic review demonstrated that prolonged circuit life was associated with lower short-term mortality but not 90-day or hospital mortality, with evidence certainty rated as “low to very low.” 20 Consequently, we acknowledge that the short-term survival benefit reported here is probably independent of the modest gain in circuit longevity, and mechanistic extrapolations based solely on filter patency should be viewed cautiously.
Importantly, our data demonstrate a short-term survival advantage with RCA. Several mechanisms may account for this observation.
1. Regional anticoagulation, bleeding, and infectious complications. RCA chelates ionized calcium in the extracorporeal circuit, forming a citrate–calcium complex that rapidly lowers ionized calcium within the circuit, thereby preventing clotting and preserving systemic coagulation. 8 Previous studies have reported significantly fewer bleeding events (5.1% vs 16.9%) and fewer infections (4.9% vs 20.3%) with RCA compared with SHA.10,19,21–24 RCA also avoids heparin-induced thrombocytopenia (HIT), a relevant consideration in septic patients at high bleeding risk. 25
2. Physiological metabolism and circuit longevity. The citrate–calcium complex is metabolized in the liver via the tricarboxylic acid cycle to bicarbonate, allowing rapid recirculation of calcium. This physiologic pathway maintains filter patency, reduces clotting-related interruptions, conserves coagulation factors, and extends effective treatment time, all of which may translate into improved outcomes.26,27
3. Reduced anticoagulant-related adverse effects. RCA eliminates the risk of HIT, a potentially catastrophic complication of heparin exposure.28–31
To the best of our knowledge, this is the first report to suggest that patients with pre-existing hypertension may derive particular 28-day survival benefit from RCA during CRRT for SA-AKI. This finding was supported by a statistically significant interaction test (P = 0.028), although given the modest sample size and exploratory nature of subgroup analyses, it should be considered hypothesis-generating and requires confirmation in prospective studies. Two non-mutually exclusive mechanisms could explain this observation. First, RCA's regional mode of action minimizes systemic anticoagulation, thereby reducing bleeding risk in patients whose underlying vascular pathology already predisposes them to hemorrhage. 32 Second, heparin can increase endothelial permeability and exacerbate organ injury in hypertensive individuals, whereas RCA lacks this deleterious effect, thus better preserving organ function.33,34
Limitations
This study has several limitations. First, it is a single-center retrospective analysis without external multicenter validation; our single-center design and modest sample size (n = 84 after PSM) limit generalizability, and our short-term endpoints (14- and 28-day mortality) require validation in external cohorts. These time frames were chosen because they are less likely to be confounded by withdrawal-of-care decisions; nevertheless, confirmation in larger, multicenter cohorts with longer follow-up is warranted. Second, although PSM was used to balance baseline characteristics, the selection of covariates and the matching algorithm may not have eliminated all residual confounding, and unmeasured biases could still influence the results. Third, because of its retrospective nature, selection bias related to the choice of anticoagulant cannot be fully excluded; prospective randomized trials are warranted to confirm and extend these findings. Fourth, subgroup analyses were exploratory and limited by reduced statistical power; the significant interaction for hypertension, although biologically plausible, requires validation before informing clinical practice. Fifth, we did not directly measure delivered CRRT dose or systematically record filter clotting events; therefore, the clinical significance of prolonged filter lifespan with RCA remains uncertain.
Conclusions
Among patients with SA-AKI receiving CRRT, RCA may confer short-term (14- and 28-day) survival benefits compared with SHA, although no difference in overall hospital mortality was observed. This potential advantage might be more pronounced in those with pre-existing hypertension, suggesting that anticoagulation selection should be individualized.
Footnotes
Acknowledgments
We thank the nursing and laboratory staff of Taizhou Municipal Hospital for their assistance in data collection and patient care.
Human ethics and consent to participate declarations
The study was approved by Taizhou Municipal Hospital (Taizhou University Affiliated Municipal Hospital), School of Medicine, Taizhou University, in accordance with the Declaration of Helsinki (No. LWSL202500277).
Consent for publication
The authors of this paper all consent to its publication.
Authors’ contributions
Jian Lan: Conceptualization, Methodology, Data Analysis, and Writing–Original Draft Preparation.
Yifeng Mao: Data Curation, Investigation, and Writing–Review and Editing.
Chenyang Shi: Investigation, Supervision, Data Curation, and Writing–Review and Editing.
Qingqing Chen: Data Curation, Formal Analysis, Visualization, and Funding Acquisition.
Shangwen Cai: Data Curation, Formal Analysis, and Visualization.
Xijiang Zhang: Writing–Review and Editing, Project Administration, Supervision.
Cheng Zheng: Conceptualization, Methodology, Formal Analysis, Writing–Review and Editing, Supervision, and Funding Acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by grants from the Medical Health Science and Technology Project of Zhejiang Provincial Health Commission (No. 2024KY1824, Qingqing Chen; No. 2025KY1871, Cheng Zheng; No. 2025HY1473, Jian Lan), the Science and Technology Project of Taizhou (No. 23ywb70, Qingqing Chen; No. 24ywa44, Cheng Zheng), the Zhejiang Provincial Science and Technology Program of Traditional Chinese Medicine (No. 2026ZL0149, Jian Lan), and the Zhejiang Medical Association Clinical Research Fund Project (No. 2025ZYC-A355, Cheng Zheng).
Conflicts of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Data availability
Data will be made available on request. Data can be requested from corresponding author (dr.zhengcheng@foxmail.com).