
Abstract
Objective
To compare postoperative infection-related characteristics and risk factors for systemic inflammatory response syndrome between asymptomatic and symptomatic ureteral stone patients undergoing ureteroscopy.
Methods
This retrospective cohort study included 475 patients undergoing ureteroscopy for ureteral stones from May 2023 to August 2024. Patients were divided into asymptomatic (n = 85) and symptomatic (n = 390) groups. Clinical characteristics and inflammatory markers were compared, and multivariate logistic regression was used to identify independent risk factors for postoperative systemic inflammatory response syndrome.
Results
The asymptomatic group had higher stone impaction rates, larger stone volumes, and longer operative time but lower inflammatory markers (all p < 0.05). The incidence of systemic inflammatory response syndrome was lower in the asymptomatic group. In the symptomatic group, independent risk factors for systemic inflammatory response syndrome included sex, urine culture, operative time, C-reactive protein, and systemic immune–inflammation index. In the asymptomatic group, only positive urine culture was identified as a risk factor.
Conclusions
Asymptomatic ureteral stones are associated with a lower risk of postoperative systemic inflammatory response syndrome. However, positive urine culture remains a key predictor of postoperative infection and requires careful management.
Introduction
Ureteral stones are a common urological condition that often causes significant discomfort and complications. Based on the presence of clinical symptoms, ureteral stones can be classified as symptomatic or asymptomatic (silent stones). Both ureteral and renal pelvic stones can lead to increased pressure within the renal pelvis and affect blood flow, thereby stimulating nerve endings. Silent stones are typically defined as those that do not present any subjective symptoms directly associated with the stones, such as acute or chronic flank pain, gross hematuria, and urinary tract infections.1–3 Ureteroscopy with stone fragmentation is a commonly used surgical method for treating ureteral stones. However, patients may experience a range of postoperative complications, with systemic inflammatory response syndrome (SIRS) being one of the most common. SIRS is a systemic inflammatory response triggered by various causes. If the symptoms of SIRS persist and are not treated promptly, the condition may progress to sepsis or multiple organ dysfunction, and in severe cases, it can be life-threatening.4–6 Notably, previous studies on patients with asymptomatic renal stones have reported paradoxically lower rates of postoperative complications—including infections—compared with those involving symptomatic patients, despite similar or even more complex stone characteristics.7,8 These findings raise important questions regarding whether a similar pattern is observed in case of ureteral stones and the mechanisms that might explain such a discrepancy. Although the risk of postoperative SIRS in symptomatic ureteral stone patients has been previously investigated, the infection-related characteristics and inflammatory response in patients with asymptomatic ureteral stones remain unclear. To date, no study has specifically investigated the perioperative infectious features of asymptomatic ureteral stones. This study aimed to compare the postoperative infection-related characteristics and SIRS risk factors between patients with asymptomatic and symptomatic ureteral stones undergoing ureteroscopy and preliminarily explore the infectious profile of this unique subgroup of patients.
Materials and methods
We conducted a retrospective analysis of clinical data from 475 consecutive patients who underwent ureteroscopy at the Department of Urology, Shaoxing People's Hospital, from May 2023 to August 2024. This study was approved by the hospital's ethics committee, and all participants provided written informed consent. Patients with other potential causes of SIRS, such as chronic inflammatory diseases, kidney diseases, metabolic or endocrine disorders, and malignancies, as well as those using immunosuppressive medications were excluded. Computed tomography (CT) and postoperative stenting were performed for all patients, with stents left in place for an average of 7–10 days. However, in cases with impacted stones, the duration of ureteral stent placement was extended to 3–6 weeks to ensure adequate ureteral healing and prevent obstruction. Continuous saline irrigation was used during ureteroscopy to maintain visibility and facilitate stone removal.
In the present study, all patients were treated using semi-rigid ureteroscopy as the primary surgical approach. Flexible ureteroscopy was not used during the initial procedure. For a few patients in whom stones had migrated to the renal pelvis, staged flexible ureteroscopy was performed as the secondary treatment. Therefore, the surgical modality was consistent across all included cases, minimizing heterogeneity. During ureteroscopy, continuous saline irrigation was performed using a gravity-based irrigation system. The irrigation pressure was maintained at approximately 60–80 cmH₂O to ensure adequate visualization while minimizing intrarenal pressure and reducing the risk of infection-related complications.
All patients in this study underwent preoperative urine culture. Patients with negative urine cultures received prophylactic antibiotics, primarily second-generation cephalosporins, preoperatively. For patients with positive urine cultures, targeted antibiotic therapy was administered based on antimicrobial susceptibility testing. Antibiotics were typically administered for at least 3–5 days preoperatively, and the procedure was performed only after adequate infection control, as indicated by clinical improvement and/or negative repeat urine culture when available. Postoperatively, antibiotic regimens were adjusted based on preoperative or intraoperative urine culture results and the patient’s clinical status.
Patients were divided into two groups based on the presence or absence of subjective symptoms related to the stone as follows: (a) asymptomatic group and (b) symptomatic ureteral stone group. Patients meeting ≥2 of the following criteria were diagnosed with SIRS: (a) temperature <36°C or >38°C; (b) heart rate >90 beats/min; (c) respiratory rate >20 breaths/min; (d) partial pressure of arterial carbon dioxide (PaCO2) < 32 mmHg; (e) and white blood cell count >12 × 109/L or <4 × 109/L. The Statistical Package for Social Sciences (SPSS) software (version 21.0) was used for data analyses. Independent t-test and chi-square test were performed for numerical and categorical variables, respectively. Multivariable logistic regression was performed to assess significant variables from univariate analysis and identify independent risk factors for postoperative SIRS.
All patient data were anonymized and de-identified prior to analysis to ensure patient privacy and confidentiality. No personally identifiable information was collected or reported in this study. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 9
Results
Patient characteristics are detailed in Table 1. This study included 475 patients (85 with asymptomatic stones and 390 with symptomatic stones) who had previously undergone ureteroscopy. Among them, 99 patients (20.8%) were diagnosed with SIRS. The prevalence of SIRS was 11.8% (10/85) in the asymptomatic group, which was lower than that in the asymptomatic group (22.8%, 89/390), with a p-value <0.05. The asymptomatic group had higher stone impaction rates, stone volume, and operative time than the symptomatic group. Inflammatory markers, such as serum white blood cell count, neutrophil count, serum C-reactive protein (CRP) levels, and the systemic immune–inflammation index (SII), were significantly lower in the asymptomatic group than in the symptomatic group (all p < 0.05). Multivariate logistic regression analysis revealed five independent risk factors for postoperative SIRS in the symptomatic group: sex (odds ratio (OR): 1.980, 95% confidence interval (CI): 1.150–3.410; p = 0.014), urine culture (OR: 3.161, 95% CI: 1.530–6.529; p < 0.01), operative time (OR: 1.050, 95% CI: 1.028–1.071; p < 0.01), serum CRP levels (OR: 1.026, 95% CI: 1.009–1.043; p < 0.01), and the SII (OR: 2.400, 95% CI: 1.115–5.163; p = 0.025) (Table 2). In contrast, the only independent risk factor for postoperative SIRS in the asymptomatic group was a positive urine culture (OR: 7.086, 95% CI: 1.635–30.708; p < 0.01) (Table 3).
Patient characteristics.
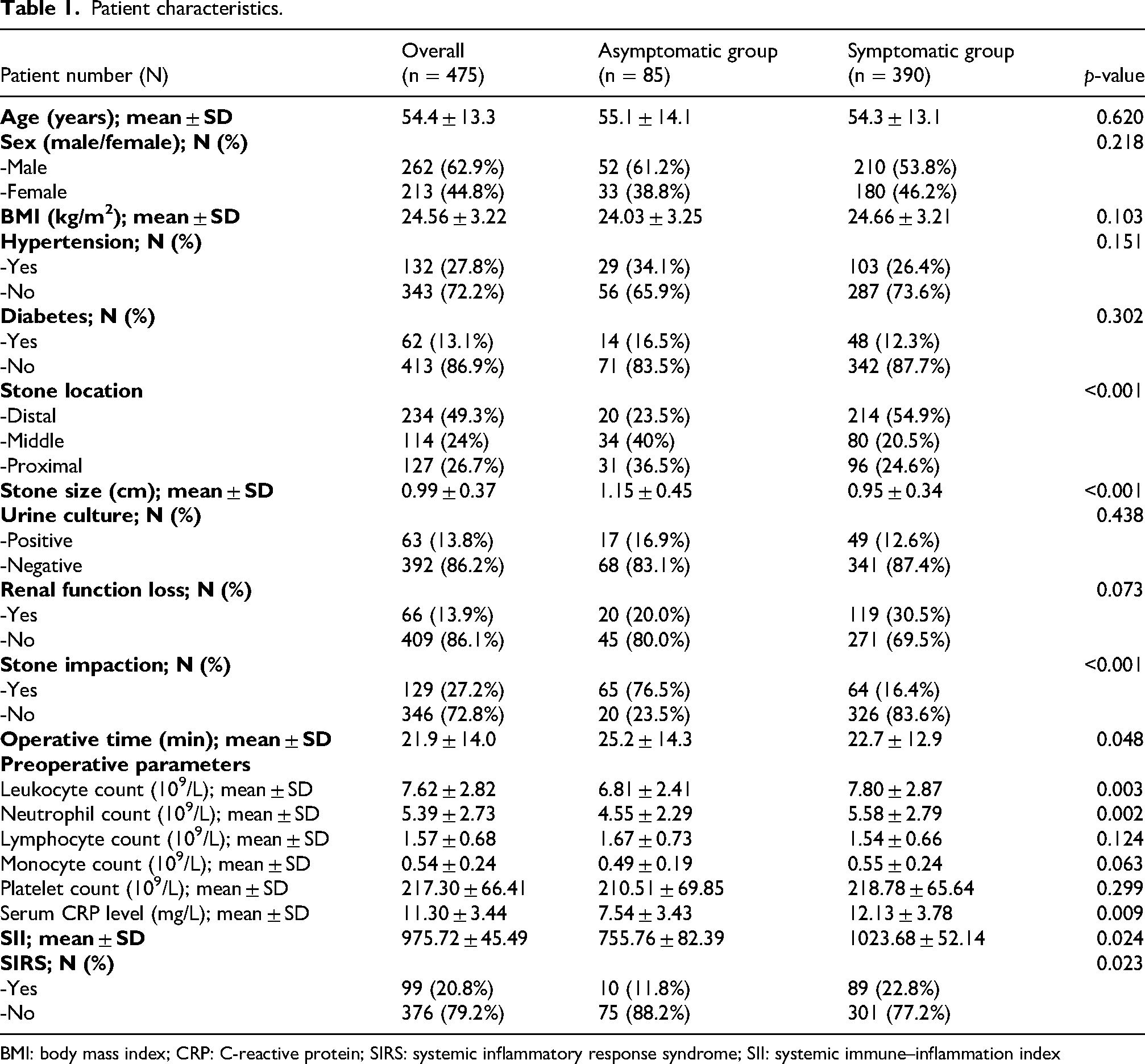
BMI: body mass index; CRP: C-reactive protein; SIRS: systemic inflammatory response syndrome; SII: systemic immune–inflammation index
Univariate and multivariate analyses for predicting SIRS after ureteroscopy in patients with symptomatic stones.
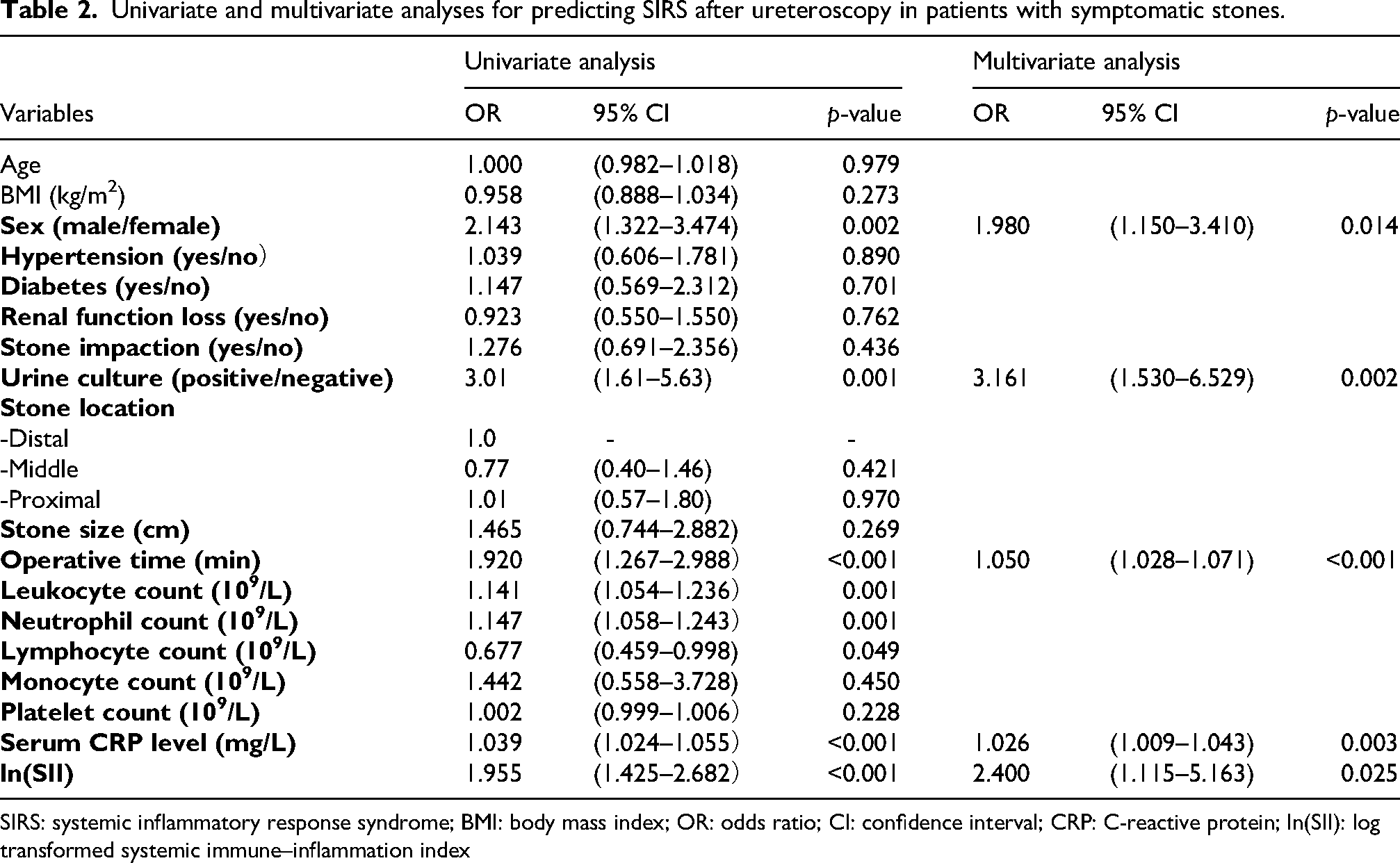
SIRS: systemic inflammatory response syndrome; BMI: body mass index; OR: odds ratio; CI: confidence interval; CRP: C-reactive protein; ln(SII): log transformed systemic immune–inflammation index
Univariate and multivariate analyses for predicting SIRS after ureteroscopy in patients with asymptomatic stones.
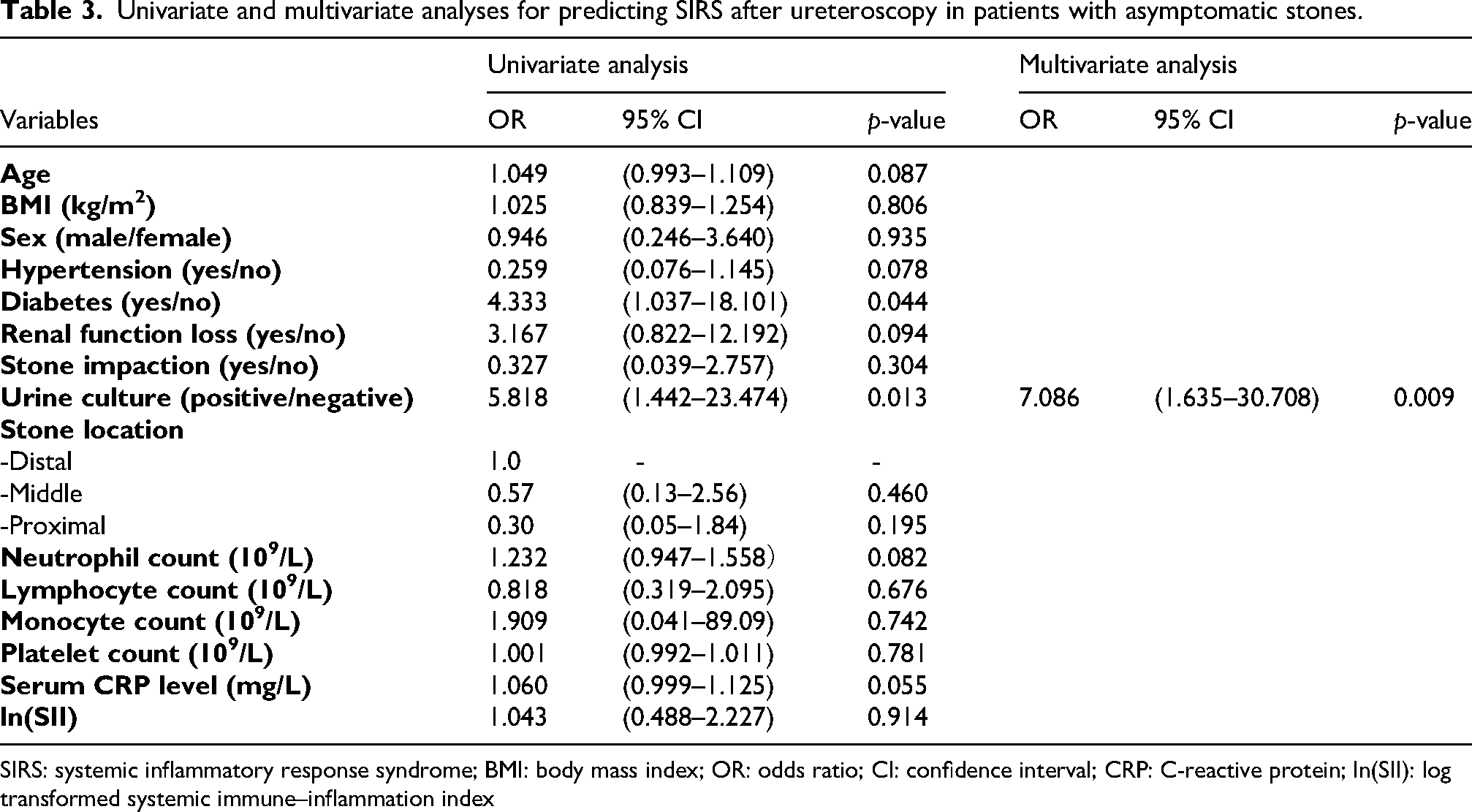
SIRS: systemic inflammatory response syndrome; BMI: body mass index; OR: odds ratio; CI: confidence interval; CRP: C-reactive protein; ln(SII): log transformed systemic immune–inflammation index
Discussion
Asymptomatic ureteral stones are a relatively unique clinical phenomenon, with limited research available. However, recent studies have gradually explored and focused on their clinical characteristics, potential impact on renal function, and management strategies. According to the study by Wimpissinger et al., asymptomatic stones are often associated with the location, size, and whether they cause urinary tract obstruction. 2 Most patients with asymptomatic stones do not experience significant pain or discomfort, leading to their frequent neglect. Although patients with asymptomatic stones do not exhibit renal colic, these stones may still cause insidious renal damage, especially when the stones are larger or located in narrow areas, potentially resulting in hydronephrosis and gradual decline in renal function. 10 Currently, there is no consensus on the management strategies for asymptomatic ureteral stones. One study investigated the characteristics of asymptomatic ureteral stones and their impact on renal function recovery, comparing them with symptomatic stones. This study has emphasized the potential harm caused by asymptomatic ureteral stones to renal function and recommended early intervention to protect renal health. 11 However, some studies have suggested that asymptomatic stones, when small and stable, can be managed using an observational approach without immediate intervention. 12
Studies on infections related to asymptomatic stones primarily focus on renal stones. For instance, Park et al. have reported that asymptomatic renal stone patients undergoing surgical management exhibit lower postoperative infection rates and fewer complications compared with symptomatic patients. 7 Similarly, Mitsuzuka et al. have highlighted that although the postoperative infection risk for asymptomatic renal stones is generally low, factors such as surgical manipulation, stone size, and number may still elevate the likelihood of infection. 8 Moreover, additional studies have analyzed risk factors for postoperative urosepsis following ureteroscopy, identifying stone quantity, location, and surgical techniques as significant determinants of infection risk. 13 Although it is generally believed that asymptomatic renal stones are associated with a lower risk of postoperative infection, the structural differences between ureteral and renal stones may lead to different outcomes. Asymptomatic ureteral stones are often impacted, which can result in positive bacterial cultures in renal pelvis urine, thereby increasing the risk of postoperative infections. These findings highlight the need for tailored management strategies for patients with asymptomatic ureteral stones to reduce the infection risk.
Previous studies have suggested that the pathological mechanism of silent ureteral stones is related to the stone not completely obstructing urine flow or failing to trigger a significant inflammatory response. Therefore, the presence of the stone does not lead to typical renal colic or other notable symptoms. However, there is a lack of specific experimental data in support of this hypothesis. 2 In this study, patients in the asymptomatic group exhibited significantly lower inflammatory indices than those in the symptomatic stone group, including white blood cell count, neutrophil count, CRP, and the SII. Among these, SII holds potential clinical significance in predicting postoperative infections and systemic inflammatory responses in patients with ureteral stones. The SII is a composite biomarker calculated using platelet count and neutrophil-to-lymphocyte ratio (NLR) and is used to assess a patient's systemic inflammatory and immune responses. As a simple and easily accessible inflammatory marker, the SII has been widely used for predicting and evaluating the prognosis of various infectious diseases, such as diabetic foot infections, 14 odontogenic infections, 15 and acute pancreatitis, 16 demonstrating significant clinical value. In addition, the SII has potential application value in the field of urinary stones. Studies have suggested that patients with higher preoperative SII levels have a higher risk of developing postoperative infections or systemic inflammatory responses.17–19
Positive urine bacterial cultures are an important risk factor for postoperative infections after ureteroscopy.20,21 Although this study suggests that the incidence of impacted ureteral stones is significantly higher in the asymptomatic group, it did not lead to a significant increase in the rate of positive urine cultures. A previous multicenter retrospective study has shown that although impacted ureteral stones may cause localized urine flow obstruction and mild urinary tract inflammation, they do not significantly increase the rate of positive urine cultures. 22 Therefore, although the impacted stones were relatively large and operative times were longer, the incidence of postoperative urinary tract infections appeared to be lower in the asymptomatic group. We hypothesize that this is attributed to a lower baseline systemic inflammatory response, as reflected by significantly reduced levels of preoperative inflammatory markers (all p < 0.05) and the absence of significant bacterial colonization, evidenced by a lower rate of positive urine cultures. These findings suggest that in asymptomatic ureteral stone patients, even in the presence of seemingly high-risk stone characteristics, systemic infection risk is mitigated by a more quiescent inflammatory milieu. Similar observations have been reported in renal stone cohorts where asymptomatic patients have shown fewer postoperative complications than their symptomatic counterparts.7,8
However, positive urine cultures remain a common risk factor for the occurrence of SIRS in both groups of patients. Moreover, the results of this study show that the OR of positive urine cultures for postoperative infection in the asymptomatic stone group is twice that of the symptomatic group (7.086 vs. 3.077), indicating that for asymptomatic ureteral stones, preoperative urine culture positivity should be taken seriously. Laparoscopic ureterolithotomy (LU) offers certain advantages in terms of reduced postoperative infections, particularly for large, complex, or impacted ureteral stones. Studies have shown that compared with ureteroscopic lithotripsy (URS), LU has a higher stone clearance rate and lower postoperative infection rate. 23 Additionally, the incidence of urinary tract infections after LU is relatively low (approximately 1%), making it suitable for patients with acute infections. 24 In the treatment of complex stones, LU can also reduce the risk of urinary leakage and postoperative ileus. 25 Overall, LU is a preferable option for patients with preoperative infection risk or larger stones. However, due to its higher invasiveness, the choice of surgical approach should be based on individual patient conditions.
Our study has certain limitations. First, as a retrospective analysis, it is inherently subject to selection bias and the potential for missing data, which may have affected the robustness of our findings. Additionally, the relatively small number of patients with asymptomatic stones may have limited the statistical power of our analyses, particularly in the multivariate regression model, potentially reducing the reliability of the conclusions drawn. Furthermore, our study is based on data from a single center, which limits the generalizability of our results to broader patient populations with varying demographic and clinical characteristics. Additionally, surgical efficacy outcomes such as the stone-free rate (SFR) were not evaluated as the primary focus of this study was postoperative infection. Therefore, the relationship between stone clearance and infectious complications could not be assessed. Despite these limitations, our study still contributes to the field as it is the first study to preliminarily explore the risk of postoperative infection in patients with asymptomatic ureteral stones. By comparing the differences in infection characteristics between symptomatic and asymptomatic patients undergoing ureteroscopy, our findings provide potentially useful information for clinical decision-making and perioperative management strategies and offer a reference for future research on the risks associated with silent ureteral stones.
Conclusion
This study focused on comparing the infection-related characteristics of asymptomatic and symptomatic ureteral stones. Asymptomatic ureteral stones showed both differences from and similarities with symptomatic ureteral stones in terms of infection-related characteristics and postoperative infection risk. The perioperative management of asymptomatic ureteral stones should comprehensively consider the characteristics of the stones as well as the systemic inflammatory status.
Footnotes
Ethical approval
This study was conducted in accordance with the ethical principles of the Helsinki Declaration of 1975, as revised in 2024. Due to the retrospective nature of the study, the requirement for informed consent was waived, and all patient data were anonymized prior to analysis.
Author contributions
All authors participated in data collection and analysis. Chao Peng and Junlong Qu drafted the manuscript, and all authors contributed to writing, reviewing, and refining of the final version of the manuscript.
Funding
The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the Yu Ren (grant number the Zhejiang Provincial Medical and Health Science).
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available within the article and/or as supplementary material.
Supplemental material
Supplemental material for this article is available online.