
Abstract
Background
Primary aldosteronism is a common and underdiagnosed form of secondary hypertension. However, preclinical investigations of adrenal ablation as a potential therapeutic approach for primary aldosteronism treatment are limited.
Methods
A deoxycorticosterone acetate–salt hypertensive rat model was established, and the animals were treated with either unilateral adrenal ablation or oral spironolactone for 12 weeks. Blood pressure was continuously monitored throughout the study period. The key endpoints included blood pressure regulation, circulating hormone levels, and target organ damage.
Results
Adrenal ablation markedly reduced blood pressure in deoxycorticosterone acetate–salt hypertensive rats. During the first 8 weeks of treatment, the antihypertensive effect exerted by adrenal ablation was significantly greater than that achieved using oral spironolactone. After 8 weeks, the blood pressure–lowering effects of both interventions were comparable, although each effect remained significantly lower than that in the untreated controls. Moreover, adrenal ablation was more effective than spironolactone in attenuating the target organ damage associated with deoxycorticosterone acetate–salt hypertension.
Conclusions
Compared with oral spironolactone, adrenal ablation significantly lowered blood pressure and more effectively attenuated target organ damage in deoxycorticosterone acetate–salt hypertensive rats.
Keywords
Introduction
Primary aldosteronism (PA) is the most prevalent form of secondary hypertension, affecting approximately 5%–10% of patients in primary care and up to 20% of those with resistant hypertension. 1 It is characterized by autonomous aldosterone overproduction and suppressed plasma renin activity, which results in sodium retention, hypokalemia, and extracellular volume expansion. These pathophysiological changes lead to sustained elevation in blood pressure and progressive multiorgan damage. 2 Importantly, emerging evidence supports the classification of PA as a distinct clinical syndrome rather than a mere subtype of hypertension. 3 Even at similar blood pressure levels, patients with PA exhibit a substantially higher risk of cardiovascular, renal, and metabolic complications than those with essential hypertension. 4 Excess aldosterone exerts deleterious effects on multiple target organs. At the vascular level, it promotes endothelial dysfunction and inflammatory cell infiltration, facilitating atherosclerotic plaque formation, instability, arterial stiffness, and vascular calcification. 5 In the heart, aldosterone induces inflammation, fibrosis, and myocardial hypertrophy.6,7 Clinically, elevated aldosterone levels are strongly associated with increased risks of left ventricular hypertrophy, atrial fibrillation, myocardial infarction, stroke, chronic kidney disease, and all-cause mortality. 8 These adverse outcomes are largely attributable to the profibrotic, proinflammatory, and pro-oxidative effects of aldosterone on cardiovascular and renal tissues, independent of its hemodynamic effects. 9 Early diagnosis and targeted treatment of PA using mineralocorticoid receptor antagonists (MRAs) or surgical/interventional approaches can reverse organ damage and significantly improve long-term outcomes. 10
Clinical studies have consistently demonstrated that lowering aldosterone levels can effectively reduce blood pressure and mitigate target organ damage. 11 Current pharmacological therapies for PA primarily rely on MRAs. 12 MRAs such as spironolactone structurally resemble aldosterone and competitively bind to cytoplasmic mineralocorticoid receptors, thereby blocking the nuclear translocation of the aldosterone–receptor complex and antagonizing its downstream effects. 13 However, MRAs do not suppress aldosterone synthesis or secretion. As a result, elevated aldosterone levels persist and continue to exert deleterious effects on cardiovascular and renal tissues. 14 Moreover, MRAs are frequently associated with adverse effects, including hyperkalemia, gynecomastia, and menstrual irregularities, which limit long-term adherence and tolerability. 15 These limitations underscore the urgent need for minimally invasive and better tolerated therapeutic alternatives. Recent advances in interventional strategies for hypertension have drawn attention to adrenal ablation, particularly because of its dual potential to reduce both blood pressure and aldosterone levels. 16 Clinically, adrenal ablation is primarily used to manage PA. This catheter-based procedure involves selective embolization of the adrenal arteries supplying the hyperfunctioning gland, resulting in partial necrosis of the adrenal tissue and suppression of aldosterone production, thereby lowering blood pressure.17,18 Despite its promise as a minimally invasive therapeutic option, evidence regarding its efficacy in reversing aldosterone-mediated cardiac and renal injuries remains limited and warrants further investigation. 19
The deoxycorticosterone acetate (DOCA)–salt hypertensive rat model is widely recognized as a robust preclinical model for studying human PA because it recapitulates key pathological features, including sustained hypertension and severe target organ damage, which closely mirror the clinical phenotype of PA.20,21 In this study, DOCA–salt hypertensive rats were treated with either adrenal ablation or oral spironolactone. The two interventions were compared in terms of blood pressure regulation and protection against end-organ damage. This study aimed to provide a preliminary assessment of adrenal ablation as an alternative therapeutic strategy for PA management.
Methods
Animals
All animal procedures were approved by the Institutional Animal Care and Use Committee of Chengdu Medical College (Approval No. CMC-IACUC-24-002, Date: 16-02-2024). This study was performed in accordance with the Helsinki Declaration of 1975 as revised in 2024. The reporting of this animal study conforms to the Animal Research: Reporting of In Vivo Experiments (ARRIVE) 2.0 guidelines. 22 The sample size was based on established study protocols.20,21,23 Thirty male Sprague–Dawley rats (8 weeks old; each weighing approximately 200–250 g) were obtained from Dashuo Experimental Animal Co., Ltd (Chengdu, Sichuan, China) and housed in a specific pathogen-free facility at Chengdu Medical College. The animals were maintained under controlled environmental conditions, at a temperature of 25°C ± 1°C and relative humidity of 45%% ± 5%, with a 12-h light/12-h dark cycle. The food and water were replenished daily, with ad libitum access to standard chow and water. All animal studies were conducted in accordance with the 8th edition of the Guidelines for the Care and Use of Laboratory Animals, ensuring that the animals were treated humanely and in compliance with the ethical guidelines for laboratory animal care. 24
Experimental protocols and experimental groups
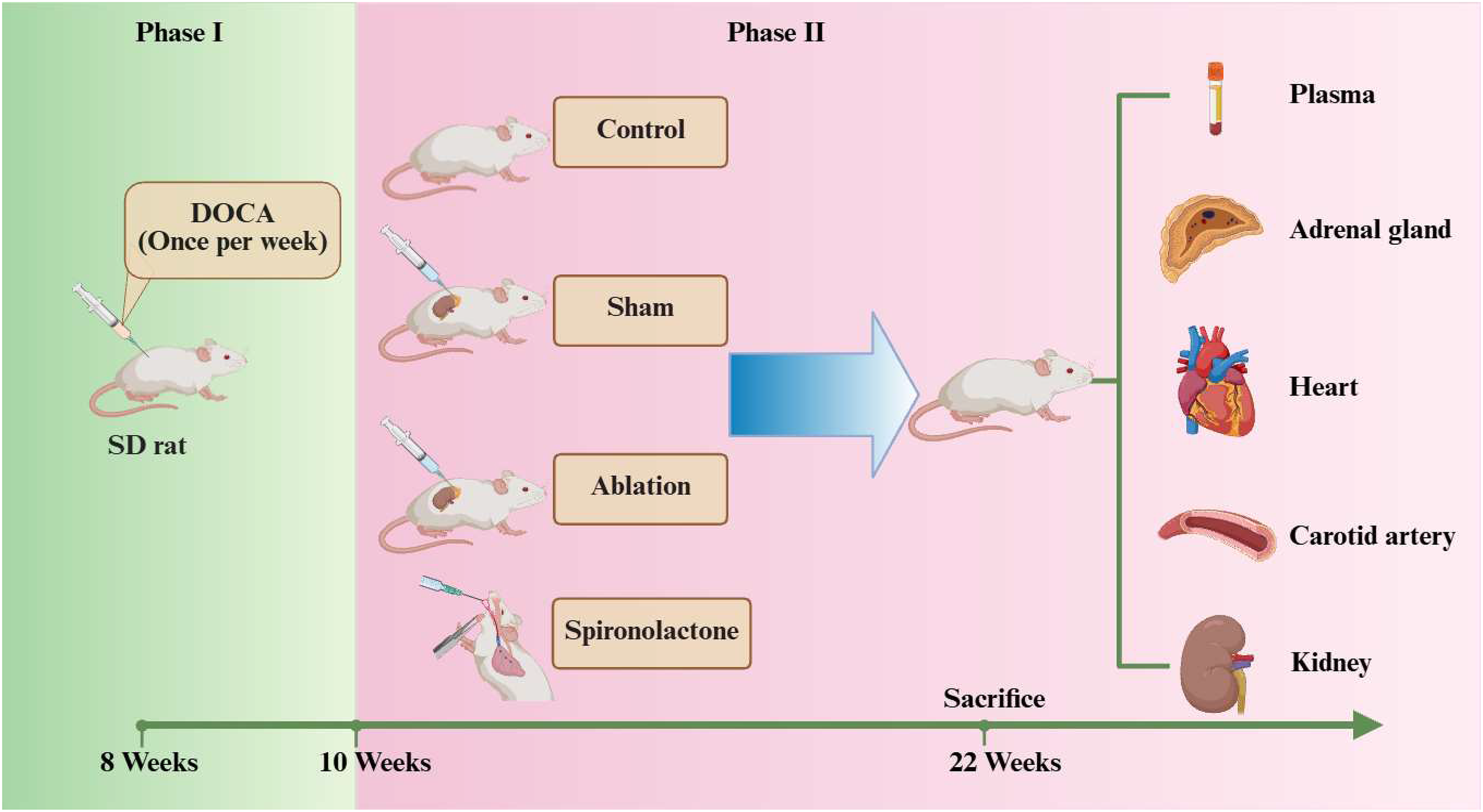
This study employed a modified DOCA–salt-induced hypertensive rat model in which both kidneys were preserved and hypertension was induced solely via subcutaneous injection of DOCA combined with high-salt drinking water.20,21 Briefly, modified DOCA–salt hypertension was established through the administration of DOCA (#56-47-3, MCE) alongside solutions containing 1% sodium chloride (NaCl) and 0.2% potassium chloride (KCl) in the drinking water for 2 weeks.20,21 DOCA was administered subcutaneously at a dosage of 50 mg/kg/week, adjusted according to body weight. The rats were briefly immobilized, and the skin over the posterior neck was disinfected using povidone–iodine solution. The DOCA oil suspension was loaded into a syringe and injected subcutaneously at an angle of 45° to a depth of 2–3 cm. Following the injection, the site was gently compressed using a sterile cotton swab to prevent leakage. After 2 weeks of DOCA–salt loading, the animals were randomly assigned to one of four groups: (a) control, DOCA–salt hypertensive rats without any additional intervention; (2) sham, DOCA–salt hypertensive rats receiving an intraglandular injection of 10 μL of sterile saline into the left adrenal gland under anesthesia; (c) ablation, DOCA–salt hypertensive rats receiving 10 μL of absolute ethanol injected into the left adrenal gland under anesthesia to induce chemical ablation 25 ; and (d) spironolactone, DOCA–salt hypertensive rats treated with spironolactone (100 mg/kg/day, oral gavage; Hangzhou Minsheng, China). 26 During the experimental period, the rats were anesthetized via intraperitoneal injection of 2% sodium pentobarbital (40 mg/kg).20,21
At the end of the experimental period, the rats were anesthetized using intraperitoneal injection of 2% sodium pentobarbital (40 mg/kg). Under deep anesthesia, blood samples (approximately 1 mL) were collected from the inferior vena cava, and the heart, kidneys, adrenal glands, and carotid arteries were rapidly excised for further analyses. The rats were placed in an induction chamber containing 4% isoflurane in 100% oxygen, with a flow rate of 1 L/min, until they exhibited a loss of righting reflex (approximately 2–3 min). Subsequently, euthanasia was performed via cervical dislocation, and death was verified by cessation of breathing and heartbeat.
Blood pressure measurement
Blood pressure was measured using a noninvasive tail-cuff system (Softron Biotechnology, Beijing, China). During noninvasive blood pressure recording, the rats remained awake. The rats were placed on a prewarmed platform, and the cuff was gently secured around the tail. The platform temperature was gradually increased to 39°C to promote vasodilation of the tail. Once a stable signal was detected, the cuff was inflated to occlude the blood flow until the pulse waveform disappeared, followed by slow deflation. Blood pressure and heart rate were automatically recorded when a regular waveform reappeared. Each rat underwent 10 measurements, and the average value was recorded as the final blood pressure value. 27 Twenty-four-hour ambulatory blood pressure monitoring was performed using a telemetry system (TA11PA-C40; Data Sciences International, St Paul, MN, USA). The rats were anesthetized via intraperitoneal injection of 2% sodium pentobarbital (3 mL/kg) and secured in the supine position. After the abdominal area was shaved and depilatory cream was applied, midline laparotomy was performed. The abdominal aorta was exposed by gently displacing the internal organs using saline-moistened gauze. A pressure-sensing catheter was inserted into the abdominal aorta, and the puncture site was sealed using Vetbond tissue adhesive. The transmitter body was placed in the abdominal cavity, and the incision was closed in layers. Systolic and diastolic arterial pressures were continuously recorded every 10 s via telemetry. 28
Biochemical measurements
Blood samples were collected in ethylenediaminetetraacetic acid (EDTA)–coated tubes and centrifuged at 3000 ×g for 15 min at 4°C. The plasma supernatants were aliquoted and stored at −80°C until analysis. All assays were performed in duplicate, and the mean values were used for statistical analyses. The plasma concentrations of aldosterone, corticosterone, renin, angiotensin II, norepinephrine, and epinephrine were measured using commercially available enzyme-linked immunosorbent assay kits (Meimian Industrial, Jiangsu, China) according to the manufacturer's protocols. The serum levels of potassium, sodium, creatinine, and blood urea nitrogen (BUN) were determined using an automated biochemical analyzer (BS-420, Mindray, Shenzhen, China).
Histological and protein expression analyses
Tissue samples from the adrenal gland, heart, kidneys, and carotid artery were fixed in 4% paraformaldehyde, embedded in paraffin, and sectioned at a thickness of 4 μm. Hematoxylin and eosin (H&E) staining was performed to evaluate the general histological morphology, whereas Masson's trichrome staining was used to assess collagen deposition and fibrosis. Stained sections were imaged using a digital slide scanner (Pannoramic MIDI, 3DHISTECH), and quantitative image analysis was conducted using ImageJ software (Media Cybernetics, Rockville, MD, USA). The severity of renal injury was evaluated using a glomerulosclerosis (GS) scoring system as previously described. 29
For protein analysis, tissue samples were lysed in radioimmunoprecipitation assay (RIPA) buffer supplemented with protease and phosphatase inhibitors. Protein concentrations were determined, and equal amounts of protein (30–50 μg) were separated using sodium dodecyl-sulfate (SDS)–polyacrylamide gel electrophoresis (SDS‒PAGE) and transferred onto polyvinylidene fluoride (PVDF) membranes. After blocking with 5% non-fat milk, the membranes were incubated overnight at 4°C using the following primary antibodies: (a) β-myosin heavy chain (1:1000, β-MHC, ab170867, Abcam); (b) tumor necrosis factor-α (1:1000, TNF-α, ab215188, Abcam); (c) transforming growth factor-β1 (1:1000, TGF-β1, ab215715, Abcam); (d) collagen I (1:1000, COL-1, ab270994, Abcam); α-smooth muscle actin (1:1000, α-SMA, #14395-1-AP, Proteintech); (e) matrix metalloproteinase 2 (1:1000, MMP2, ab92536, Abcam); (f) proliferating cell nuclear antigen (1:1000, PCNA, ab92552, Abcam); and (g) smooth muscle protein 22α (1:1000, Sm22α, ab14106, Abcam). After washing, the membranes were incubated with horseradish peroxidase (HRP)-conjugated secondary antibody. Immunoreactive bands were visualized using an enhanced chemiluminescence (ECL) detection system and quantified using Image Lab software (Bio-Rad, USA). β-actin was used as the internal loading control.
Echocardiographic and vascular ultrasound assessments
Transthoracic echocardiography was performed using a high-resolution ultrasound system for small animals (EPIQ 7, Philips, The Netherlands) equipped with a 30–40-MHz linear-array transducer. Rats were anesthetized with 1.5%–2% isoflurane and positioned supine on a temperature-controlled heating pad to maintain normothermia. In the parasternal long-axis B-mode view, the left ventricular internal diameter at end-diastole (LVIDd) and interventricular septal thickness at end-diastole (IVSd) were measured. Left ventricular ejection fraction (LVEF) and left ventricular fractional shortening (LVFS) were automatically calculated using system-integrated algorithms based on standard formulas. For vascular assessment, the carotid arteries were imaged in two-dimensional real-time mode. Doppler-based techniques were used to measure the resistance index (RI) and pulse wave velocity (PWV). All echocardiographic and vascular parameters were averaged over at least three consecutive cardiac cycles to ensure measurement consistency.
Statistical analyses
The results are reported as the mean ± SD values. Each experiment was independently conducted at least thrice. The Shapiro‒Wilk test was used to check for normality, whereas the Brown‒Forsythe test confirmed the homogeneity of variances. For datasets that satisfied these criteria, comparisons between two distinct groups were conducted using an unpaired, two-tailed Student's t-test. For evaluating multiple groups, either one-way analysis of variance (ANOVA) or two-way ANOVA with repeated measures was utilized, followed by Tukey's post hoc test for assessing multiple comparisons. In cases where the assumptions for normality were not fulfilled, the non-parametric Mann–Whitney U test (for two groups) or the Kruskal‒Wallis test with Dunn's post hoc correction (for multiple groups) was applied. All statistical assessments were executed using Prism 8.0 (GraphPad Inc., San Diego, USA). A p-value <0.05 was considered statistically significant.
Results
Effects of adrenal ablation on blood pressure and heart rate in DOCA–salt hypertensive rats
After 2 weeks of subcutaneous DOCA administration combined with a high-salt diet, the tail-cuff blood pressure of the rats was significantly elevated compared with the baseline level. After 2 weeks, the blood pressure remained persistently high in both control and sham groups, with no significant difference between them (Figure 1(a) to (c)). In contrast, the blood pressure in both ablation and spironolactone groups was significantly lower than that in the control group (Figure 1(a) to (c)). Notably, throughout the 12-week intervention period, the blood pressure in the ablation group remained consistently lower than that in the spironolactone group, with the difference being particularly pronounced at 8 weeks after chemical adrenal ablation (Figure 1(a) to (c)). No significant changes in heart rate were observed between the groups either before or after modeling or intervention (Figure 1(d)). Similarly, after 12 weeks of intervention, both adrenal ablation and oral spironolactone significantly reduced the 24-h mean blood pressure, with the ablation group showing a more pronounced reduction (Figure 1(e) and (f)).
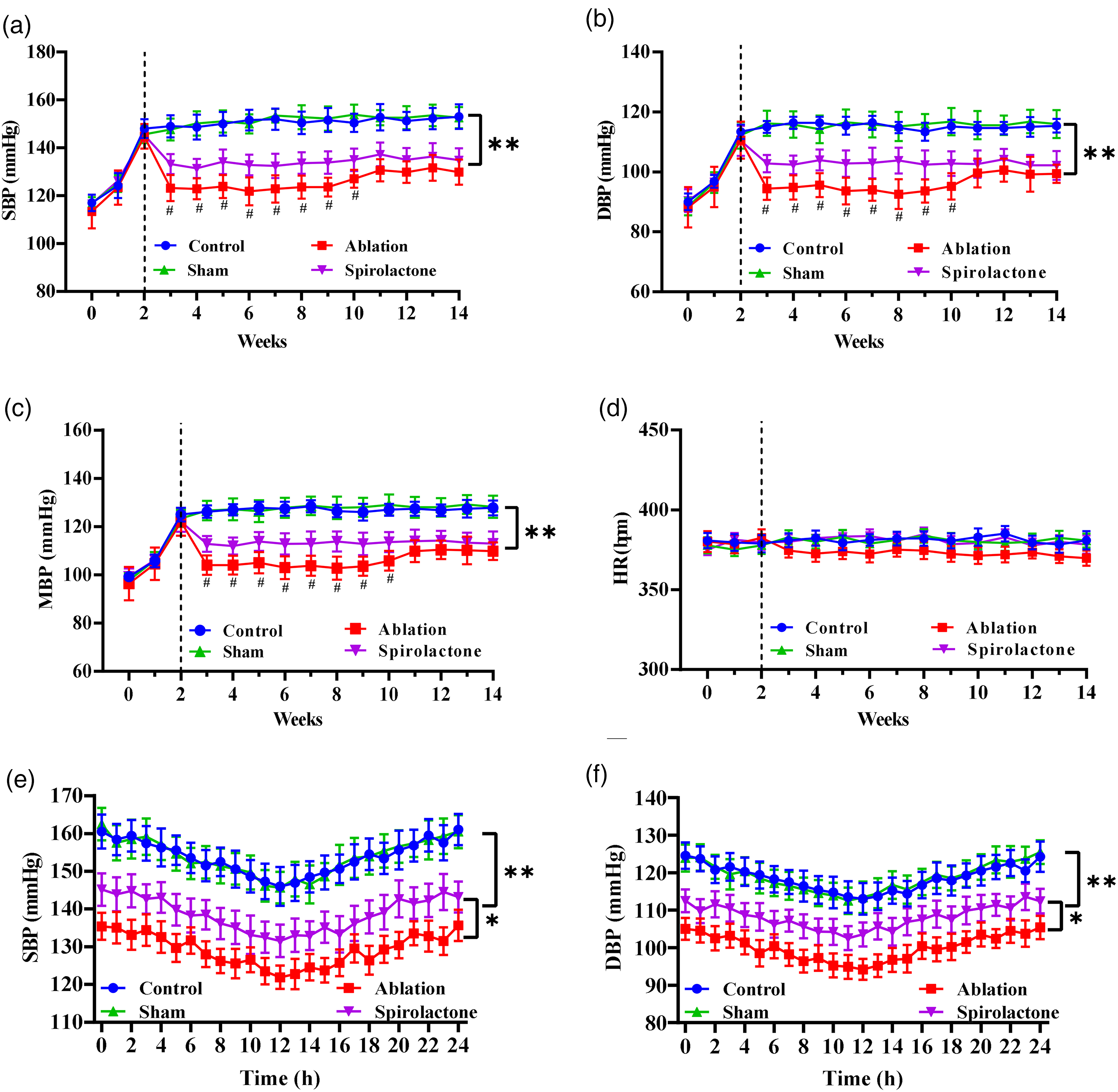
Adrenal ablation lowers blood pressure more effectively than spironolactone in DOCA–salt hypertensive rats. Tail-cuff measurements of (a) systolic blood pressure (SBP) (b) diastolic blood pressure (DBP), (c) mean arterial pressure (MAP), and (d) heart rate (HR) following intervention in DOCA–salt hypertensive rats. At 12 weeks after the intervention, (e) dynamic systolic and (f) diastolic blood pressures were assessed via telemetry. The data are presented as mean ± SEM values (n = 5 per group).
Effects of adrenal ablation on hormone levels in DOCA–salt hypertensive rats
Hormone levels were assessed in all the groups at the end of the experiment. The levels of aldosterone, corticosterone, angiotensin II, renin, norepinephrine, and epinephrine in the sham group were not significantly different from those in the control group (Figure 2(a) to (f)). In DOCA–salt hypertensive rats treated using spironolactone, renin levels significantly increased, whereas other hormone levels remained unaffected (Figure 2(a) to (f)). In contrast, the levels of aldosterone, corticosterone, norepinephrine, and epinephrine were significantly reduced in the adrenal ablation group compared with those in the control group, with no significant changes observed in the angiotensin II or renin levels between the groups (Figure 2(a) to (f)).
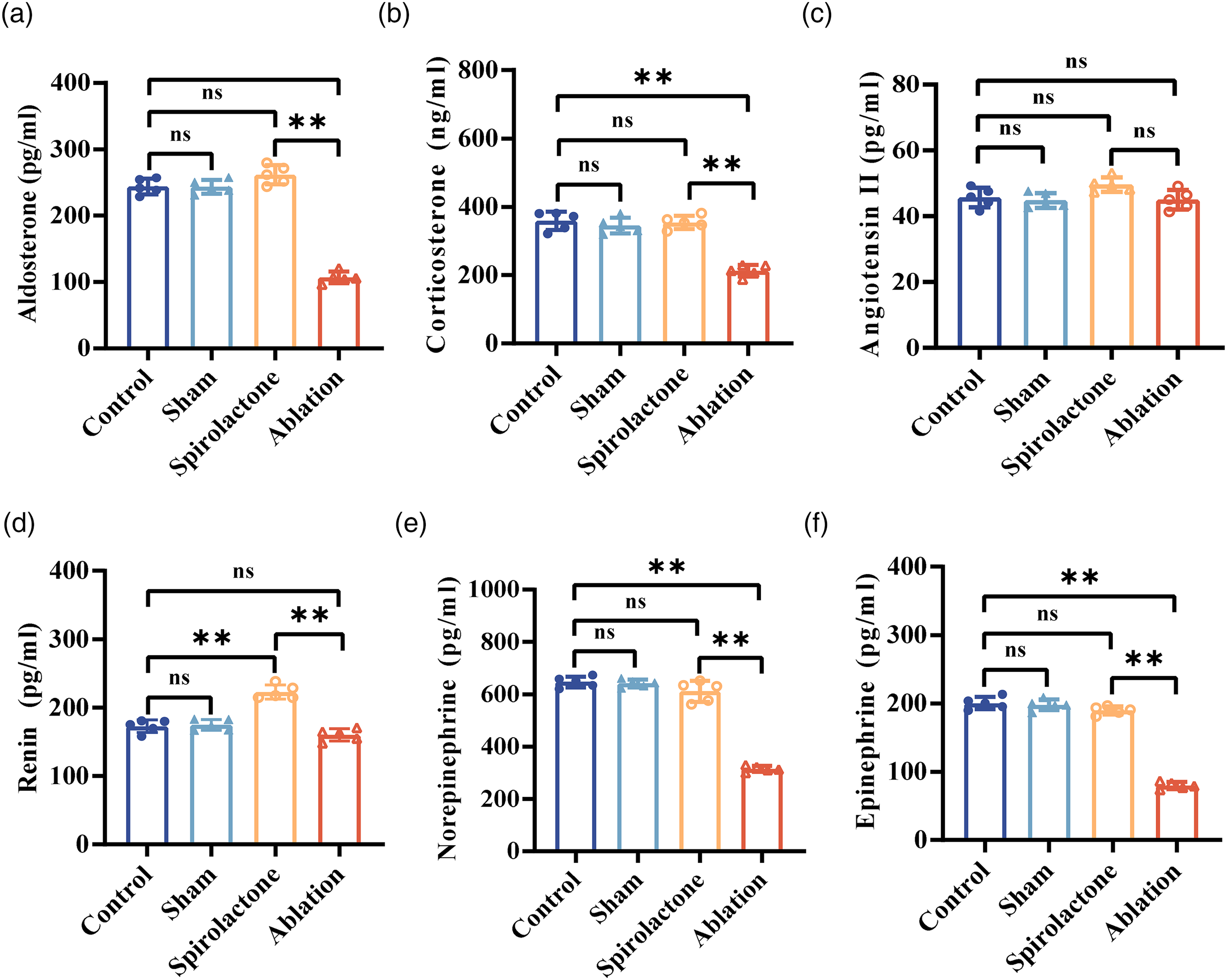
Adrenal ablation reduces adrenal cortical and medullary hormone levels in DOCA–salt hypertensive rats. Plasma levels of (a) aldosterone, (b) corticosterone, (c) angiotensin II, (d) renin, (e) norepinephrine, and (f) epinephrine were measured across groups of DOCA–salt hypertensive rats. The data are presented as mean ± SEM values (n = 5 per group).
Effects of adrenal ablation on the adrenal glands of DOCA–salt hypertensive rats
Compared with the control group, no significant changes in adrenal morphology were observed in the sham or spironolactone groups (Figure 3(a) to (d)). Histopathological analyses revealed a disorganized architecture and irregular cell alignment in HE-stained sections from the ablation group (Figure 3(a)), whereas Masson's trichrome staining revealed a significant increase in collagen deposition within the ablated area (Figure 3(b) and (d)). These histological findings confirmed the successful induction of adrenal ablation in DOCA–salt hypertensive rats.
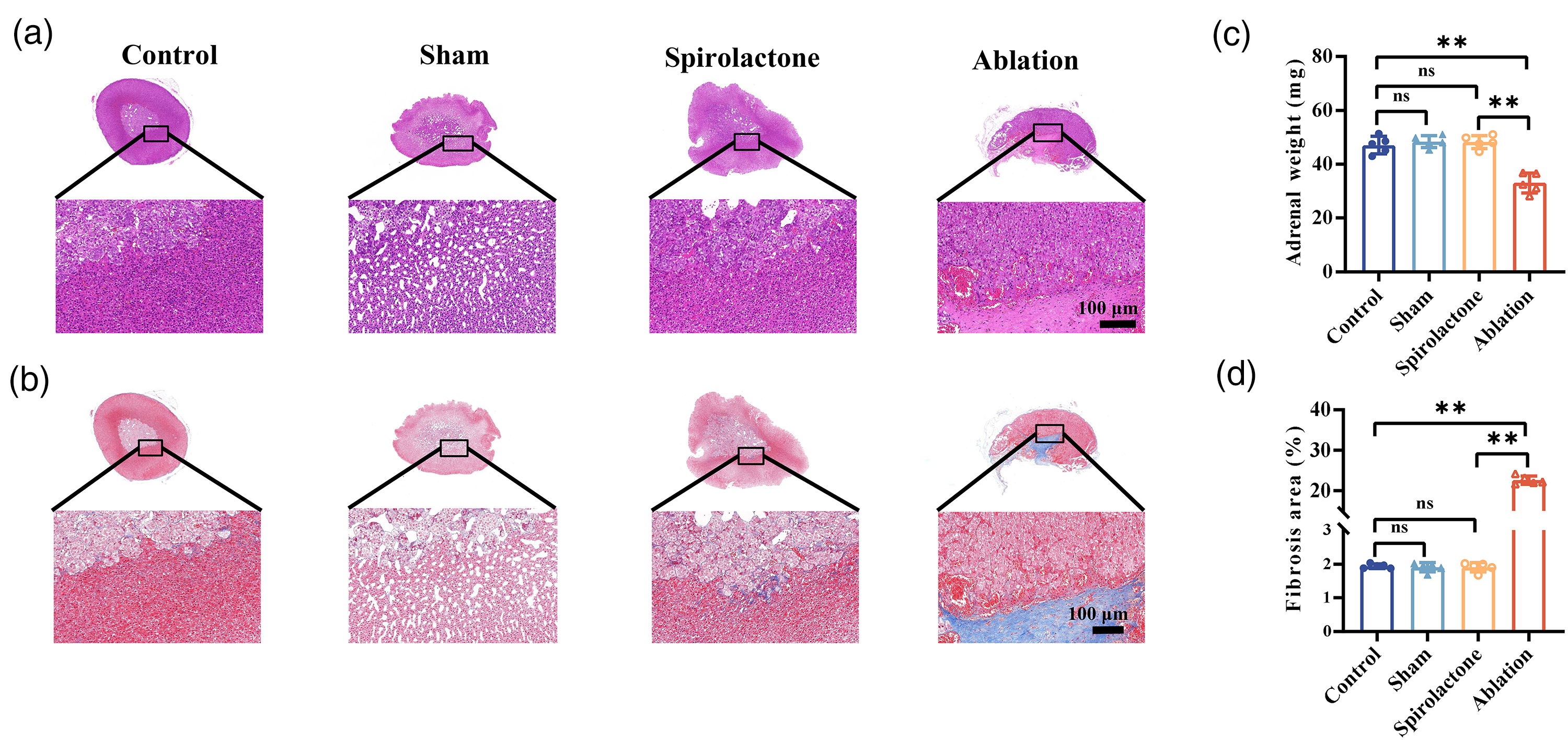
Adrenal ablation induces adrenal atrophy and fibrosis in DOCA–salt hypertensive rats. Representative images of (a) gross adrenal morphology, (b) hematoxylin and eosin (H&E) staining, and (c) Masson's trichrome staining for each group. (d) Bilateral adrenal weights and (e) quantification of the adrenal fibrotic area are shown. The data are presented as mean ± SEM values (n = 5 per group).
Effects of adrenal ablation on the cardiac health of DOCA–salt hypertensive rats
Cardiac function and morphology in the sham group were not significantly different from those in the control group (Figure 4(a) to (m)). Echocardiographic analysis revealed that the LVIDd and IVSd were significantly reduced in both adrenal ablation and spironolactone groups compared with those in the control group (Figure 4(e) and (f)), whereas FS and the LVEF remained unaffected (Figure 4(g) and (h)). Histological evaluation demonstrated that adrenal ablation and spironolactone administration alleviated cardiomyocyte hypertrophy and reduced myocardial fibrosis (Figure 4(b) to (d)). In addition, the heart-to-body weight ratio was significantly lower in the ablation and spironolactone groups than in the control group (Figure 4(i)). Western blot analysis further revealed that both interventions markedly downregulated the expression of fibrosis-related proteins, including β-MHC, TNF-α, and TGF-β1 (Figure 4(j) to (m)). Moreover, the cardioprotective effects of adrenal ablation were significantly greater than those of spironolactone (Figure 4(a) to (m)).
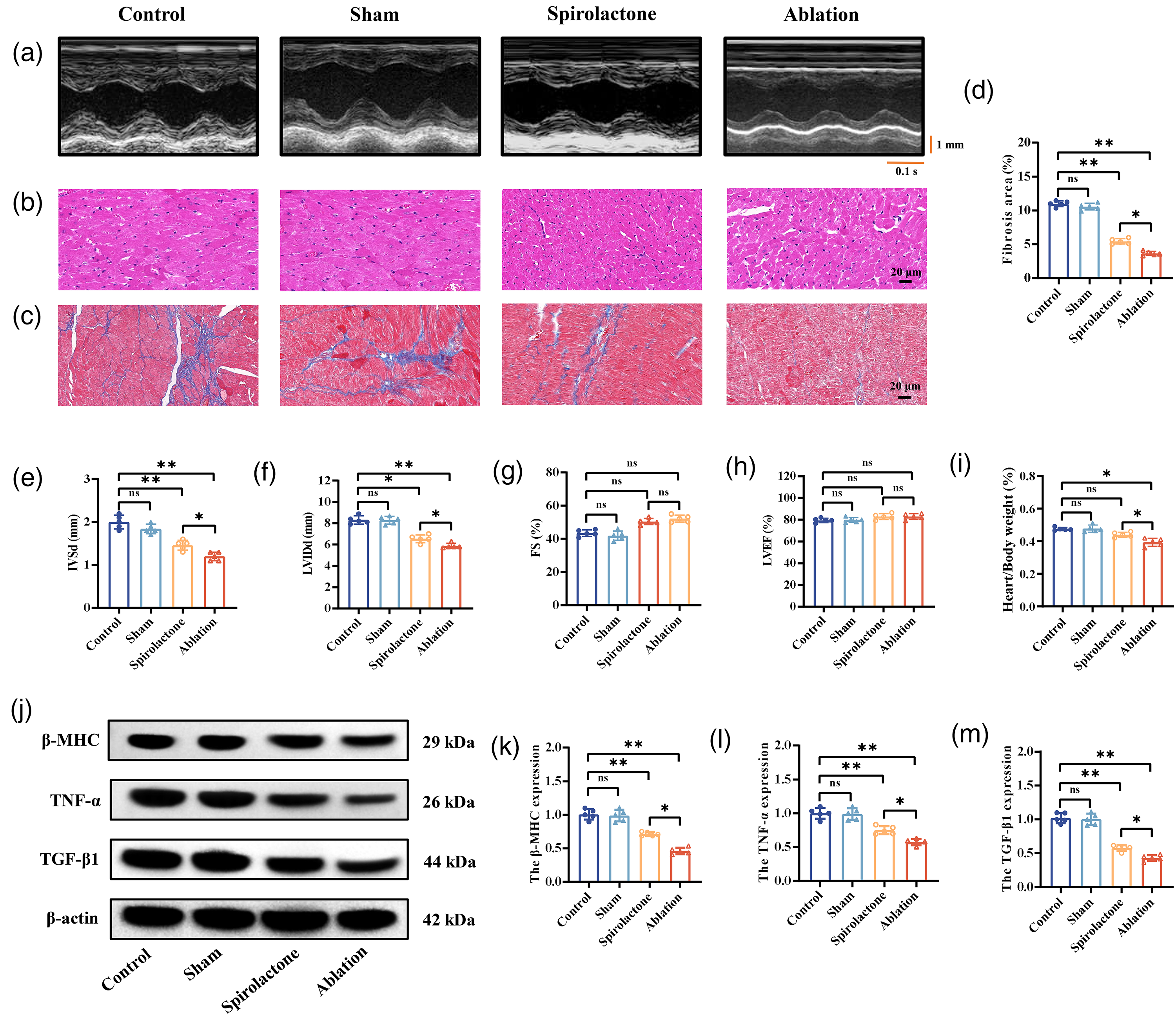
Adrenal ablation improves cardiac function and morphology more effectively than spironolactone in DOCA–salt hypertensive rats. Representative (a) echocardiographic images, (b) hematoxylin and eosin (H&E) staining, and (c) Masson's trichrome staining of cardiac tissue from each treatment group. (d) Quantification of the myocardial fibrotic area. (e–h) Echocardiographic assessment of IVSd, LVIDd, LVFS, and LVEF performed to evaluate cardiac function. (i) Heart-to-body weight ratio. (j) Representative immunoblot bands and quantification of (k) β-MHC, (l) TNF-α, and (m) TGF-β1 protein levels in cardiac tissues. The data are presented as mean ± SEM values (n = 5 per group).
Effects of adrenal ablation on the kidneys of DOCA–salt hypertensive rats
Renal function and morphology in the sham group were not significantly different from those in the control group (Figure 5(a) to (l)). Histological analyses revealed that both adrenal ablation and spironolactone effectively ameliorated segmental GS, reduced GS scores, and attenuated renal fibrosis (Figure 5(a) to (d)). Furthermore, both interventions significantly increased serum potassium levels, reduced serum sodium levels, and improved serum creatinine and BUN levels in DOCA–salt hypertensive rats (Figure 5(e) to (h)). Similar trends were observed for the renal protein expression levels of COL-I, TGF-β1, and α-SMA (Figure 5(i) to (l)). Notably, the renoprotective effects of adrenal ablation were more pronounced than those of spironolactone (Figure 5(a) to (l)).
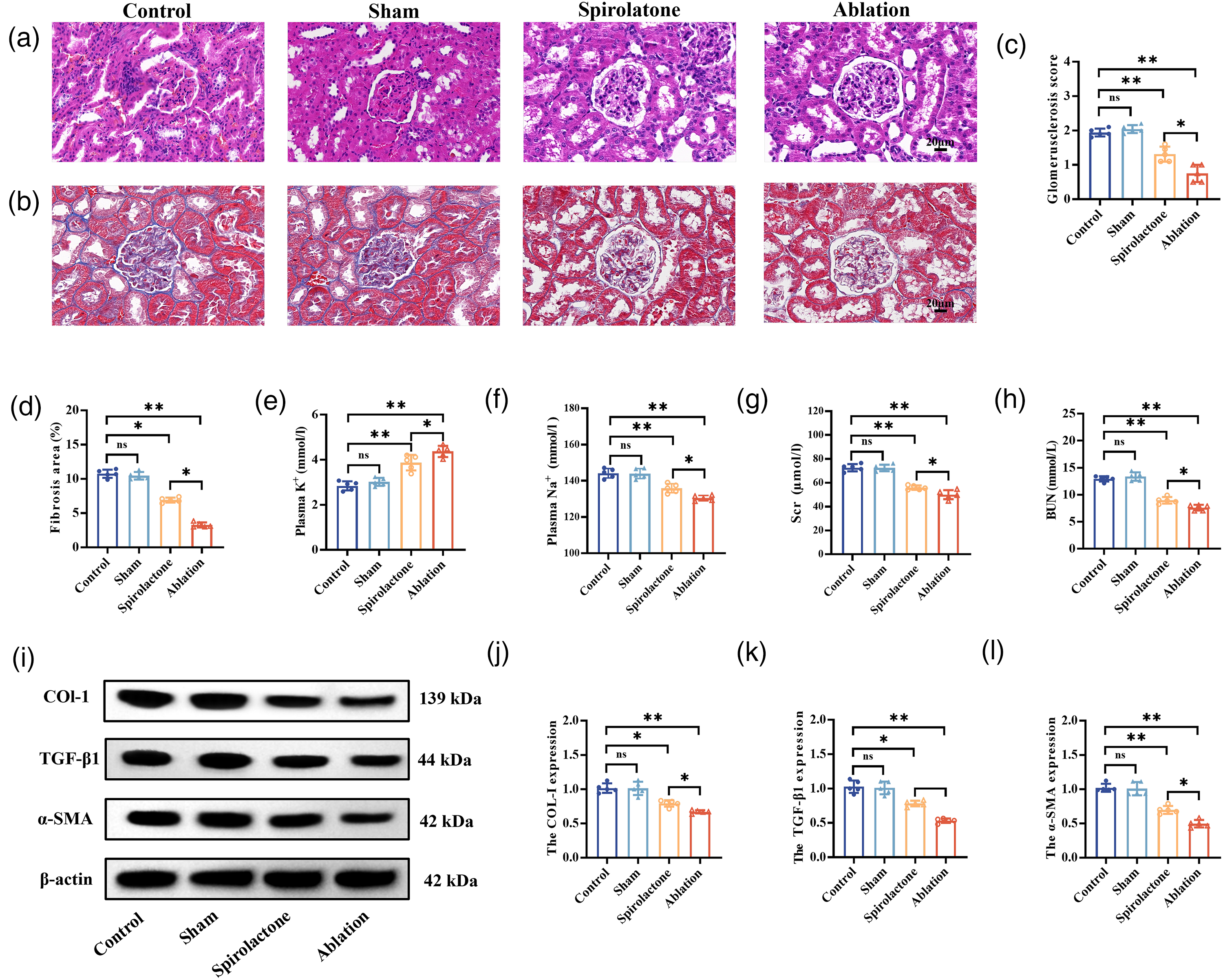
Adrenal ablation improves renal function and morphology more effectively than spironolactone in DOCA–salt hypertensive rats. Representative (a) H&E staining and (c) glomerulosclerosis scores in the indicated groups are shown. Representative (b) Masson's trichrome staining and (d) quantification of the fibrotic area across treatment groups. Serum levels of (e) potassium, (f) sodium, (g) creatinine, and (h) and blood urea nitrogen (BUN). Representative (i) immunoblot bands and quantification of (j) COL-I, (k) TGF-β1, and (l) α-SMA (L) protein levels in kidney tissues. The data are presented as mean ± SEM values (n = 5 per group).
Effects of adrenal ablation on the carotid artery in DOCA–salt hypertensive rats
No significant differences in carotid artery function or morphology were observed between the sham and control groups (Figure 6(a) to (k)). Histological analysis demonstrated that both adrenal ablation and spironolactone significantly reduced the medial carotid thickness and improved fibrosis (Figure 6(a), (b), (d), and (e)). Ultrasonographic assessment revealed that both treatments effectively decreased the RI and PWV in the carotid artery (Figure 6(c), (f), and (g)). Protein analysis of carotid tissues revealed downregulation of MMP-2 and PCNA and upregulation of Sm22α in both ablation and spironolactone groups compared with that in the control group (Figure 6(h) to (k)). Notably, adrenal ablation exerted more pronounced effects than spironolactone on these vascular parameters (Figure 6(a) to (k)).
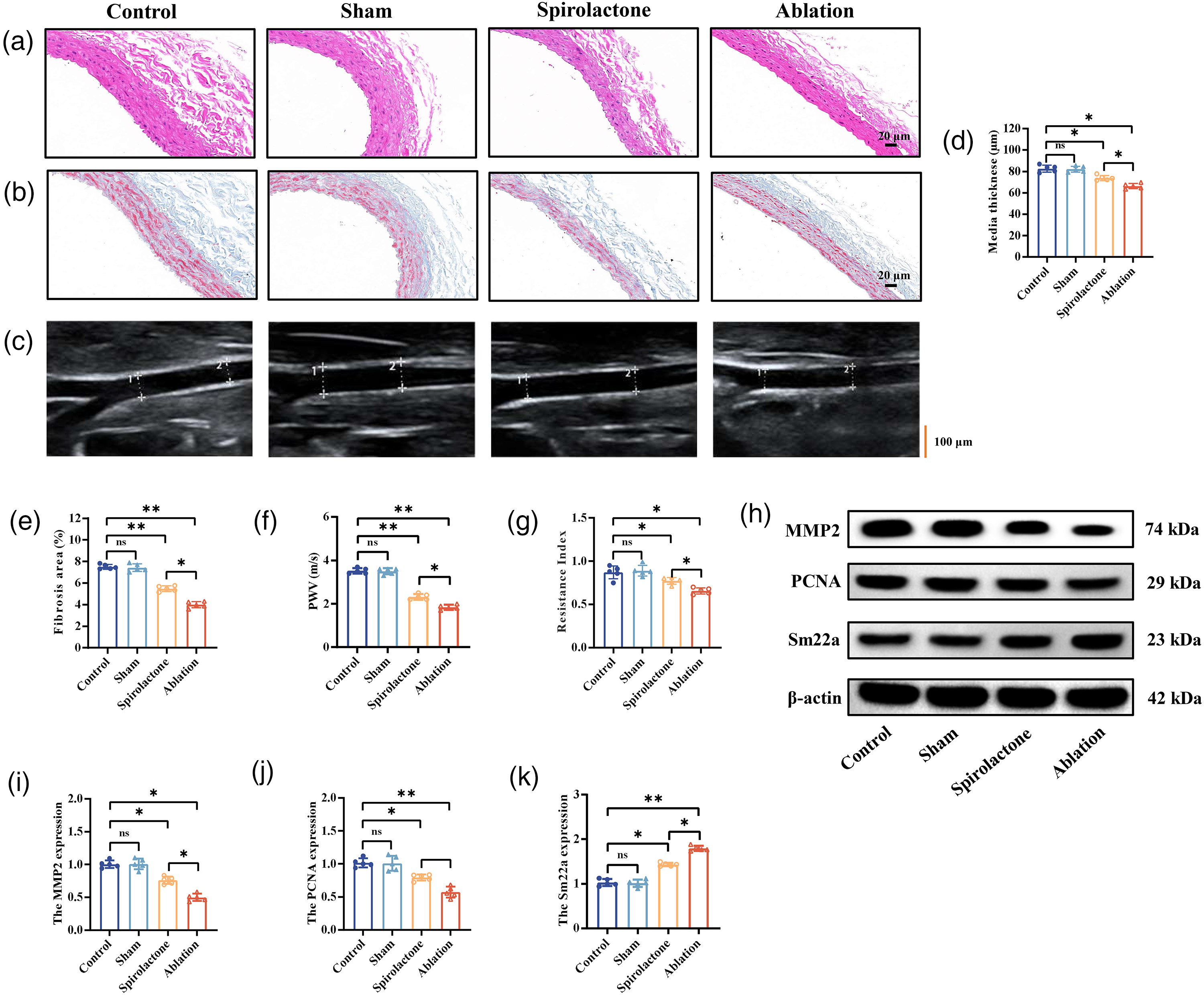
Adrenal ablation improves carotid artery function and morphology more effectively than spironolactone in DOCA–salt hypertensive rats. Representative images of (a) H&E staining, (b) Masson’s trichrome staining, and (c) carotid artery ultrasonography in the indicated groups. Quantification of (d) carotid artery medial thickness and (e) the fibrotic area. (f) Carotid artery pulse wave velocity and (g) resistance index. Representative (h) immunoblot bands and quantification of (i) MMP2, (j) PCNA, and (k) Sm22α protein levels in carotid artery tissues. The data are presented as mean ± SEM values (n = 5 per group). ap < 0.05; bp < 0.01;
Discussion
To identify effective therapeutic strategies for PA, this study utilized a DOCA–salt hypertensive rat model to comprehensively assess the impact of adrenal ablation on blood pressure regulation, hormone secretion, and target organ remodeling. These findings provide several key insights. First, adrenal ablation led to a more substantial reduction in blood pressure than spironolactone. Second, the procedure induced partial necrosis of the adrenal tissue, thereby reducing the secretion of both cortical and medullary hormones. Third, adrenal ablation provided superior protection against target organ damage compared with spironolactone. Together, these results suggest that adrenal ablation offers enhanced therapeutic efficacy over spironolactone in this mineralocorticoid-induced hypertension (Figure 7).
Simplified diagram showing the effects by which adrenal ablation alleviates blood pressure and target organ damage in DOCA–salt hypertensive rats.
Our results demonstrate that both adrenal ablation and spironolactone effectively lowered blood pressure, albeit through distinct mechanisms. Although both approaches antagonize aldosterone activity, adrenal ablation uniquely reduces aldosterone secretion and concurrently suppresses corticosterone and catecholamine levels.30,31 Previous studies have shown that excess aldosterone and sodium retention in patients with PA can further activate the sympathetic nervous system.32,33 By lowering circulating hormone levels, adrenal ablation may exert a sustained antihypertensive effect via inhibition of the renin-angiotensin-aldosterone system and attenuation of sympathetic nerve activity. Notably, adrenal ablation directly decreases secretion from both adrenal cortex and medulla, thereby circumventing the “escape phenomenon,” which is common in pharmacological therapies. 34 Furthermore, the direct suppression of aldosterone production through adrenal ablation not only alleviates aldosterone-driven sodium and water retention but also reduces the risk of related cardiovascular complications. 35
We also observed a notable “early enhancement–late compensation” dynamic following adrenal ablation. Blood pressure rapidly declined during the initial phase post intervention, followed by a gradual rebound. This phenomenon may reflect compensatory mechanisms as some adrenal tissues may undergo transient edema rather than complete necrosis. With edema resolution, there might be partial recovery of residual adrenal function. In addition, the inherent regenerative capacity of the adrenal gland may enable surviving cells to proliferate and compensate for tissue loss. Importantly, despite late-phase blood pressure rebound, the levels remained significantly lower than those observed in the spironolactone group, suggesting that adrenal ablation establishes a new steady-state set point for blood pressure regulation. As opposed to spironolactone, adrenal ablation does not involve the long-term metabolic burdens associated with chronic pharmacotherapy. Although spironolactone effectively controls blood pressure, its off-target interactions with androgen receptors can cause adverse effects such as gynecomastia in men. 36 Moreover, the efficacy of pharmacological treatments is frequently limited by poor patient adherence. 37 As a single-session interventional therapy offering sustained blood pressure control, adrenal ablation may represent a valuable alternative, especially for patients with low medication adherence or in healthcare settings with limited resources. 38 Following adrenal ablation, the heart rate of the rats decreased compared with that at baseline. This may be because ablation reduced catecholamine levels, thereby decreasing sympathetic nerve activity.
Adrenalectomy is a guideline-recommended treatment for PA. 39 However, both clinical and preclinical studies have reported a significantly increased risk of adrenal insufficiency following adrenalectomy.40,41 In contrast, multiple single-center clinical studies investigating adrenal ablation in PA patients have not reported any cases of adrenal insufficiency.42,43 Consistent with these findings, our previous work involving spontaneously hypertensive rats (SHRs) has demonstrated that following adrenal ablation, adrenal cortical and medullary hormone levels remained higher than those observed in normotensive Wistar–Kyoto controls. 25 Similarly, the present study revealed that post ablation, hormone concentrations in DOCA–salt hypertensive rats remained within normal physiological ranges, suggesting preserved adrenal function.
Limitations
This study has certain limitations. Although the DOCA–salt hypertensive rat model, characterized by sodium and water retention, along with suppressed renin levels, is widely regarded as a classic and relevant model for human PA, the pathological processes induced by exogenous hormone administration fundamentally differ from those underlying human PA. These discrepancies may limit the translational applicability of our findings and affect the predictive accuracy of the ablation efficacy. From a technical standpoint, the minute size of the rat adrenal artery precludes replication of catheter-based microablation procedures commonly employed in clinical practice. Moreover, the substantially smaller adrenal gland volume in rats than in humans introduces inherent procedural differences that may have impacted the experimental outcomes. We did not evaluate atrial function or the ratio of early (E) to late (A) mitral flow velocities. Inclusion of these parameters would provide a more holistic view of cardiac remodeling. The evidence on the long-term impact of adrenal ablation remains poor. Finally, this study assessed only a limited panel of hormones and did not examine hormonal rhythmicity or temporal fluctuations, which could provide further insights into post-intervention endocrine dynamics.
Conclusions
This study confirmed that adrenal ablation markedly reduces blood pressure and mitigates target organ damage, demonstrating superior efficacy over spironolactone. These findings highlight that interventional approaches that directly target aldosterone production may provide distinct therapeutic advantages in managing PA.
Footnotes
Acknowledgments
Ethics declaration
All animal procedures were approved by the Institutional Animal Care and Use Committee of Chengdu Medical College (Approval No. CMC-IACUC-24-002, Date: 16-02-2024).
Author contributions
J.W., T.L., and R.D. conceived the original idea and performed the experiments and data analysis. J.W., T.L., X.W., Q.Y., J.H., Y.W., Y.L., and Q.R. wrote the manuscript and prepared the figures. S.L. and P.W. prepared the final draft of the manuscript. All authors have read and approved the final version of the manuscript.
Funding
This work was supported by grants from the Central Funds Guiding the Local Science and Technology Development of Sichuan Province (No. 2024ZYD0148), the high-level talent research start-up fund of the First Affiliated Hospital of Chengdu Medical College (No. CYFY-GQ81, No. CYFY-GQ82), Innovative Team Project of Chengdu Medical College (No. 2024kjTzn05), Innovation Team Project of Sichuan Provincial Health Commission (No. 24CXTD01), and National Key Clinical Specialties Construction (No. 2024GXNKG002).
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data and material availability
The data that support the findings of this study are not publicly available because they contain information that could compromise the privacy of research participants; however, they can be made available from the corresponding author upon reasonable request.